Prevention
Lec.13 Diet and dental caries
Dr.Jihan Abdulhussein
The role diet and nutrition in the etiology and pathogenesis of caries may be viewed
as systemic and local effect In general, the term diet refers to food and drink
consumption (diaita ‘way of life’) while nutrition refers to a process by which living
organisms physiologically absorb and metabolize food to ensure growth, energy
production, repair of tissue and ultimately reproduction of the sp ecies (nutritio ‘to
nourish’).
The relationship between diet and dental caries
Dental caries is a progressive microbial disease of multifactorial nature and is
strongly affected by diet. Diet affect the integrity of teeth; quantity, pH, and
composition of the saliva; and plaque pH.
Role of carbohydrates in caries development
Dietary carbohydrates exert their cariogenic effect locally on tooth surface by
influence the quality and quantity of dental plaque. Dental caries occurs as plaque
bacteria metabolize fermentable carbohydrate, producing organic acids. These
acids diffuse through the plaque into the enamel and dissolve mineral. If mineral
diffuses out of the tooth and into the oral environment, then demineralization
occurs. If the process is reversed the damaged crystal are rebuilt (reminerilization).
Caries occurs when demineralization exceeds remineralization.
Carbohydrate is an essential nutrient and can be classified in to three main
categories:
1- Free-form monosaccharide (simple sugars) include glucose and fructose which
are found naturally in fruit, vegetables and honey while galactose occur only as a
result of the breakdown during digestion of lactose.
2-Disaccharides (two simple sugar molecules linked together): the most
common:
Sucrose (refined from sugar cane or sugar beets, it’s a major part of dietary
sugar) formed when one molecules of glucose combine with one molecules of
fructose.
Lactose is formed when a molecule of glucose combine in a molecules of
galactose (milk sugar).
Maltose is formed when two molecules of glucose combine; it is mainly derived
from hydrolysis of the starch.
Fermentable carbohydrate: any carbohydrate that can be hydrolyzed by salivary
amylase and subsequently fermented by bacteria
3-Polysaccharides: the polysaccharides not sugar.
All polysaccharides are made up of many individual sugar molecules, usually
glucose, joined together. The digestible forms include starch, which is found in rice,
potatoes, peas; about half of dietary carbohydrates are composed of starch.
Types of study providing evidence for the relationship between diet and caries
development: The evidence come from a number of type of studies, these include:
Observational (epidemiological) studies: Numerous world-wide epidemiological
studies show that caries prevalence is low in population adhering to a primitive way
of living and a diet of local products with little sugar.
Interventional studies
:
in which diets of groups of people are purposefully altered
and the effect of this intervention observed. Those that have been reported are
now decades old and were conducted on highly selected groups of people, before
the strong link between sugars and caries was established. Such studies would not
be possible to repeat today because of ethical constraints they include.
The Hopewood House was an orphanage in Australia. From its beginning sugar and
other refined carbohydrate were excluded from the children diet. Dental surveys of
these children from the ages of 5-11 years revealed a greatly reduced caries
incidence compared the state school population in that age group. When the children
became old enough to earn wages in the outside economy, they deviated from the
original diet. A steep increase of decayed missing and filled teeth (DMFT) after the
age of 11 years indicates that the teeth did not acquire any permanent resistance to
caries
The Vipeholm study was conducted shortly after the Second World War in an adult
mental institution in Sweden between 1945-1953. The study investigated the effect
of consuming sugary foods of varying stickiness (i.e different oral retention times)
and at different time throughout the day on the development of caries by measuring
caries increment in subjects.
Main conclusions of the Vipeholm study:
when consumed in large amounts, had little effect on caries
increment if it was ingested up to a maximum of four times a day at mealtimes only
f sugar in between meals was associated with a marked increase in
dental caries
- rich foods
.
Animal studies: various animal experiments were conducted to evaluate the effect
of sugar intake.
Enamel slab experiments: These observe the effects of diet on demineralization in
slabs of enamel (cut from extracted teeth) which are held in the mouth of human
volunteers in a removable plate constructed like an orthodontic appliance.
Plaque pH studies: This type of experiment investigates the effect of food, meals, or
component of foods on the pH of dental plaque. These studies are relatively easy to
do, but they measure acidogenicity of diet rather than cariogenicity (only an
indication of the possible effect of diet on the development of dental caries).
Incubation studies: these are the simplest but weakest method. Test foods are
incubated with plaque or saliva (which contains plaque organisms) and the rate of
acid production is recorded. In some experiments, whole enamel, powdered enamel,
or calcium phosphate are added to the saliva/substrate mixture and the rate of
dissolution of mineral is taken as a measure of cariogenic potential.
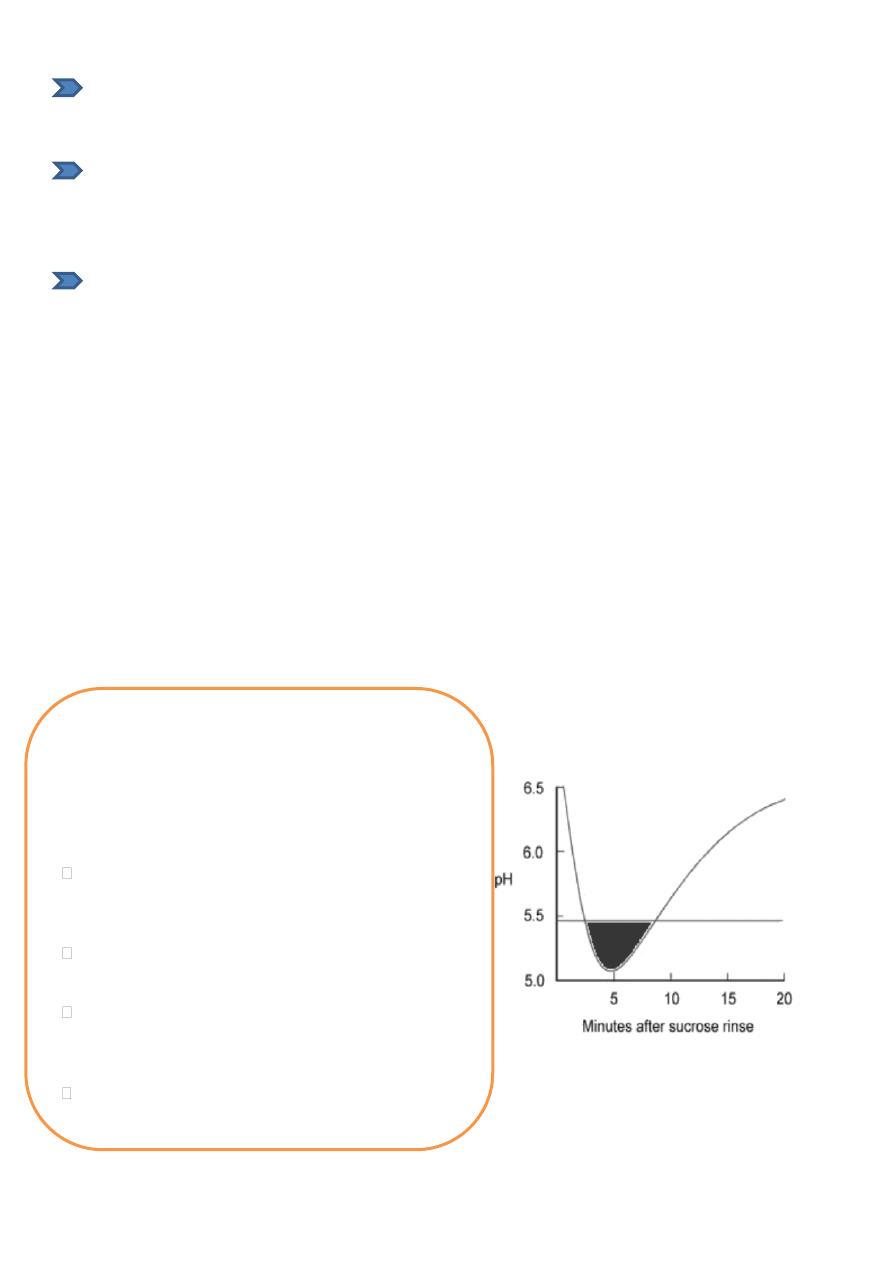
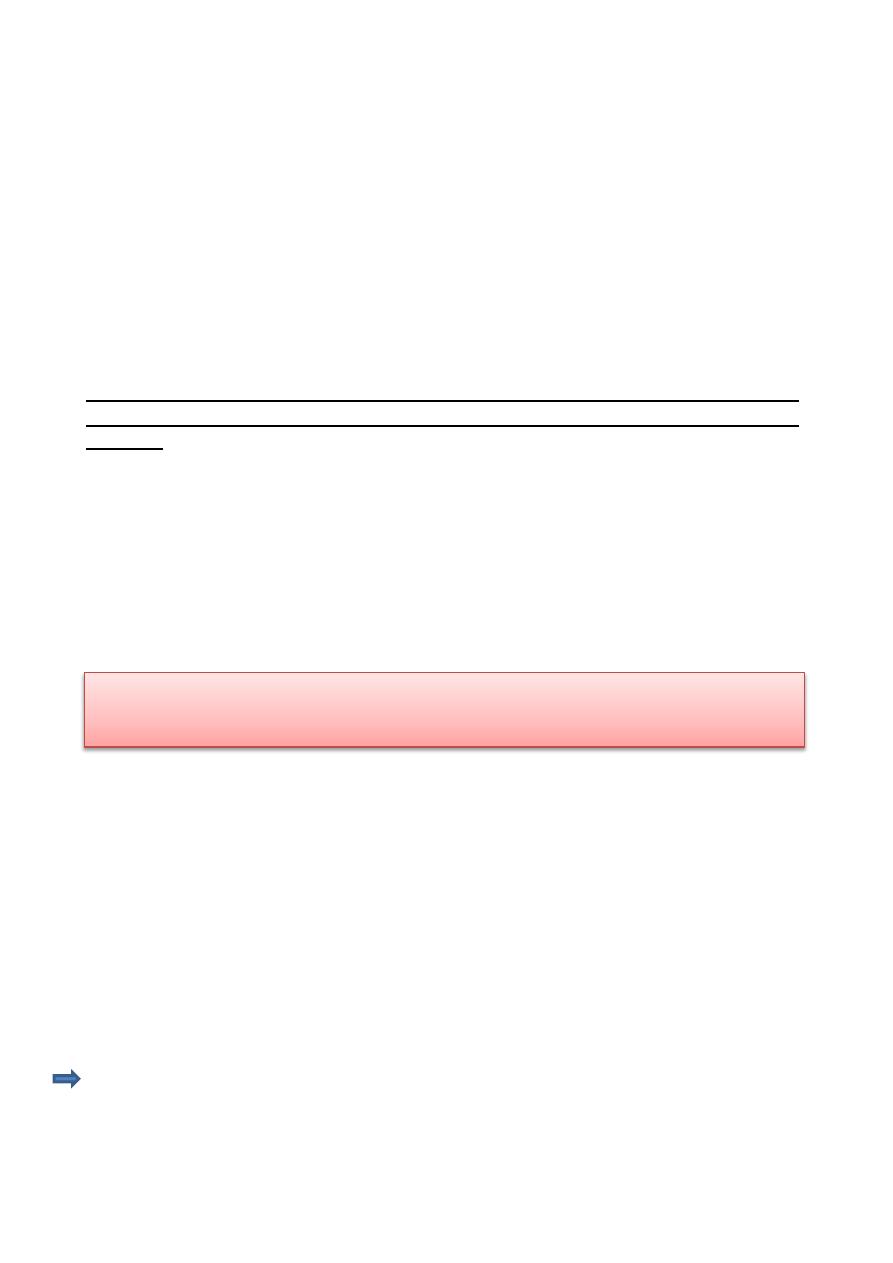
The basic Stephan curve
The resting PH of dental plaque was mostly between pH 6.5 and 7, the term resting
plaque refers to plaque 2-2.5 hours after the last intake of carbohydrate. But when
the plaque exposed to sucrose or glucose, the pH of plaque falls rapidly below the
critical value within 2-5 minutes.
(the value of pH 5.5 has become accepted as critical pH below which dental
enamel will begin to dissolve because the environment is no longer saturated with
enamel mineral), this rapid fall was then followed by slow recovery over the next
30-60minutes. The plot of plaque pH against time has become known as the
Stephan curve.
The rapidity with which the pH falls is a reflection of
speed on which sucrose come diffuse in to plaque and
the activity of the concentration of enzymes produced
by the great number of bacteria in the plaque. The slow
rate of recovery to the resting pH, critical factor in
caries production depend mainly on
Rapid production of high concentration of acids
within the plaque, temporarily overcomes local
buffering
Escape of acids in to saliva, delayed by the diffusion-
limiting properties of plaque and its thickness
Diffusion of salivary buffers in to plaque hampered
by the diffusion-limiting prope rtie s of plaque and its
thickness
Continued sugar production from bacte rial
intracellular polysaccharides
Caries free subjects tend to have a slightly higher resting plaque pH, a higher
minimum pH following consumption of fermentable carbohydrate and a faster
return to resting levels, when compared with caries susceptible subjects (as shown in
figure above).
Factors affecting food cariogenicity:
1-Types of carbohydrates
For dental health purpose , there is no evidence from epidemiological studies that
sugar located within the cellular structure of a food are harmful to teeth, and
therefore it is important to distinguish between these and sugars in free form,
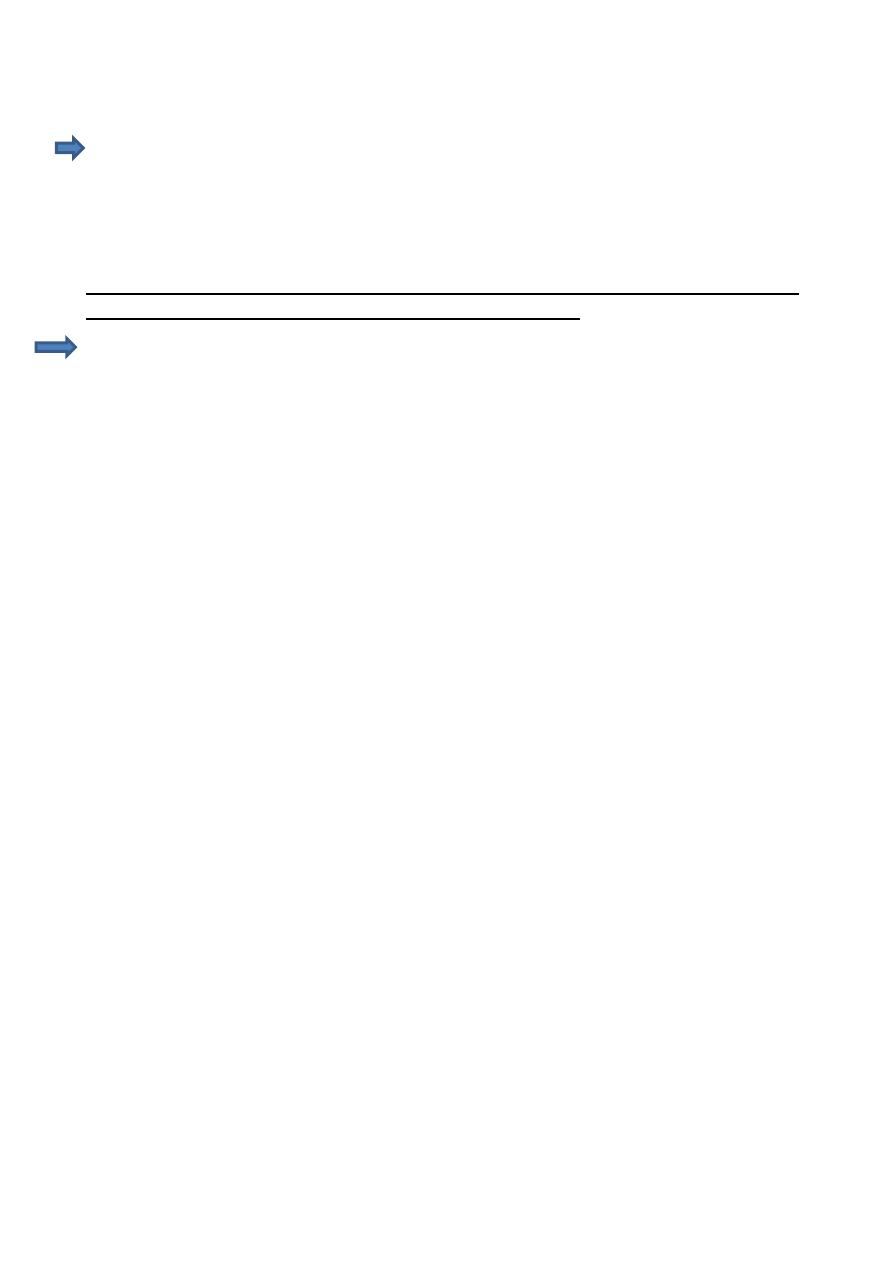
therefore they classified sugars for dental health purpose into intrinsic and extrinsic
sugars, extrinsic sugar were subdivided into milk sugars (as lactose naturally present
in milk is not thought to be harmful to the teeth) and non milk extrinsic sugar which
include all added sugars and sugars present in fruit juices, hony and syrups. In term
of dental caries, it’s the intake of non milk extrinsic sugar (or free sugars) that need
to be reduced.
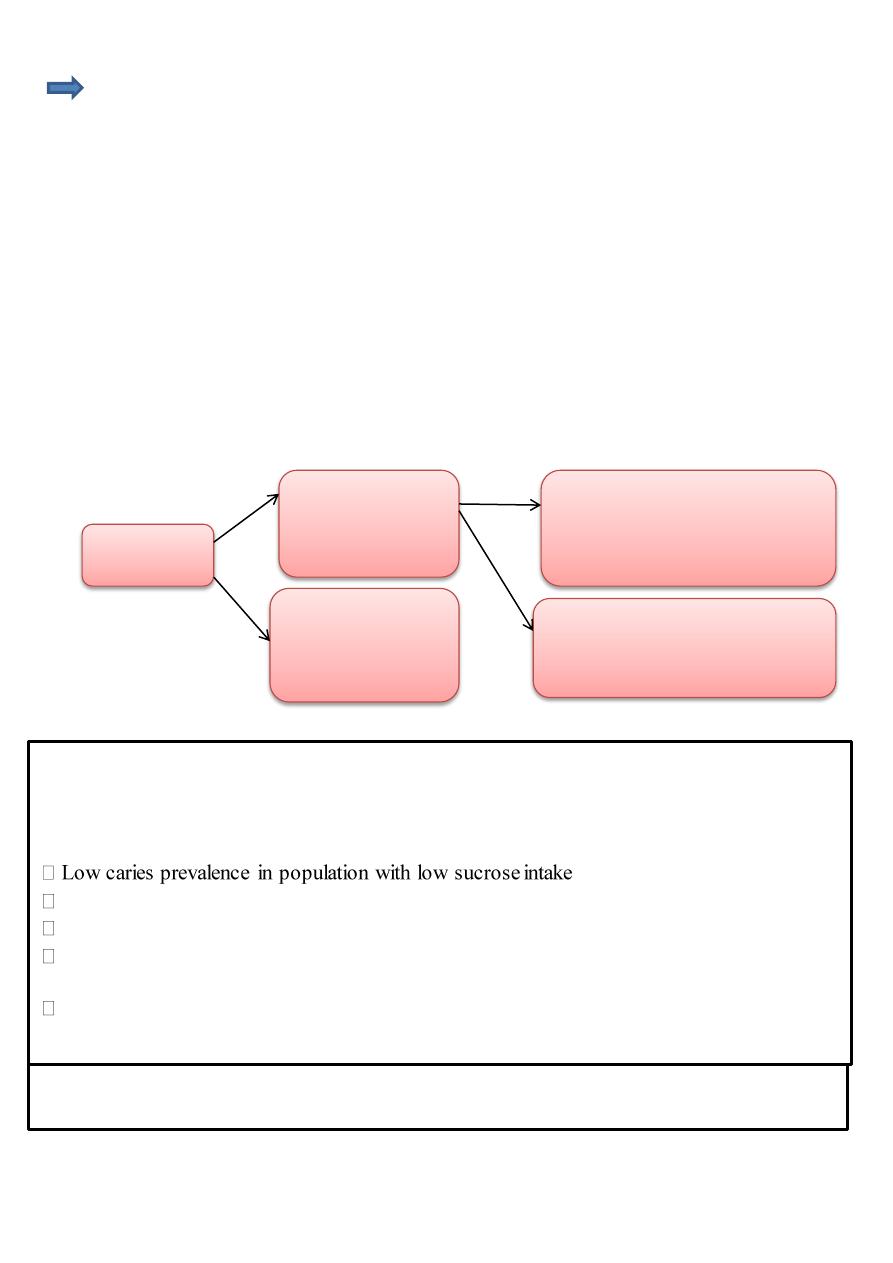
total sugar
Extrinsic sugars that
located outside the
cellular structure of
foods
Intrinsic sugars that
Located within the
cellular structure of
foods
Non – milk extrinsic sugars that
include all added sugars and sugars
present in fruit juices, honey and
syrups
Milk sugars that naturally present in
milk and milk products
Sucrose is the most abundant sugar. It is used by food manufacturers all over the world as a
food ingredient.
For several reasons sucrose has been called the arch-criminal in dental caries. The
epidemiological evidence for sucrose as the cause of dental caries:
The decline in caries prevalence during wartime sucrose shortages
The rise of caries prevalence with increasing availability of sucrose
Archaeological evidence of low caries prevalence in eras before sucrose became freely
available
Low caries prevalence in disorders of sucrose metabolism hereditary fructose
intolerance
There seems to be little difference in the cariogenicity of glucose, fructose, and maltose, but
the same source of evidence show that lactose is less cariogenic
Sucrose is unique because it is a substrate for extracellular dextrin synthesis by S.
mutans. The cariogenicity of plaque depend on its ability
to adhere to the teeth,
to resist dissolution by saliva and
its protection of bacterial acids from salivary buffering.
These properties depend on the formation of insoluble polysaccharides produced
particularly by cariogenic strains of S. mutans. In addition, colonization by S.
mutans (cariogenic bacteria) is highly dependent on the sucrose content of the diet
In the absence of sucrose, S. mutans cannot colonize the mouth, therefore its plaque
counts appear to depend on the sucrose content of the diet.
Nevertheless, no sugar has been shown to be more cariogenic than sucrose and, it
is the most widely available dietary sugar, it is has been subject of the greatest
criticism.
Starch: Starch constitutes a heterogeneous food group, it may be highly refined or
consumed in its natural state, it may be consumed raw or in cooked form- all these
factors should be considered when assessing the cariogenicity of starches. They
argue that all carbohydrate including starch cause dental caries, because although
the starch (polysaccharide) molecules are, too large to diffuse into the plaque,
however they are broken down by salivary amylase releasing maltose, maltotriose,
and glucose that may be metabolized by oral bacteria to produce acids that cause
dental caries.
The starch granules of plants are only slowly attacked by salivary amylase, because
the starch is in an insoluble form and protected by cellulose membrane, therefore the
cariogenicity of uncooked starch is very low. Heating at temperature used in
cooking cause a partial degradation to a soluble form, which can be further broken
down by salivary and bacterial amylases to maltose, maltotriose, and glucose.
2-Physical form of food and clearance time:
In addition to the chemical composition of food, physical and organoleptic
properties (particle size, solubility, adhesiveness, texture and test) are important for
cariogenicity, since they influence eating pattern and oral retention of the foods.
Diets that results in the greater retention of refined carbohydrate over the longest
period are the most cariogenic.
The carbohydrate in various drink are eliminated within 5 minutes while sweet such
as sugar containing chewing gum, toffees, lozenges generally give high oral sucrose
Plaque pH drop very little following consumption of raw starch but soluble
starch and starch containing food such as bread cause a pH fall which is
somewhat smaller than with sugar
concentration and clearance time from 40 minutes for chewing gum to 15-20
minutes for other sweets.
The texture of the diet is also important, for both salivary secretion and elimination
of fermentable carbohydrate from the oral cavity. A diet that require thorough
chewing will result in the secretion of large amount of saliva with a high pH and
strong buffering capacity, in contrast to a finely textured diet that require little
mastication tends to be retained in the oral cavity and eliminated slowly.
The caries producing potential could possibly be reduced by modifying their
physical properties (roughage, adhesiveness, solubility).
Practical way to speed up carbohydrate clearance are
tooth brushing immediately after meal, or
induction of rapid salivary flow by mechanical or gustatory stimuli through
eating tough or highly flavored foods at the end of meals
Chewing sugar free chewing gum or peanuts immediately after eating sugar also
speed up sugar clearance and neutralization of plaque acid through saliva
stimulation
Mouth rinsing with water has a very limited effect, partly because it is generally
done too late: two minutes after a sucrose challenge, the sugar concentration in
saliva is usually lower than that in plaque so rinsing with water at that time would
not be expected to reduce the diffusion of sugar into plaque, unless the sugar
clearance were excessively slow, as in xerostomic subjects.
The advantages of mouth rinsing after meal is that it also help to remove sugars in
solution and food debris.
Chewing sugar-cane yield a less pronounced pH drop and a quicker pH reco very in
dental plaque than is seen following a mouth rinse with sucrose. The difference
probably result from stimulation of salivary flow associated with the chewing
It's often advised to consume sugar- rich foods at meal times rather than alone, or in
between meals; This is because, when consumed with other foods the effect on pH
is minimized probably due to
(1) The dilution effect
(2) The increased salivary flow rate due to mastication of other foods
Frequency of intake sugar and dental caries
Frequent intake sugars will induce a prolonged and intense acid attack on the tooth
surface; moreover, the time available for reminerlization is thus decreased.

The pH of dental plaque falls rapidly when sugar are eaten, the more occasion sugar
is taken the greater the number of times plaque pH will fall below a level where
demineralization can occur (critical pH), the less time there is for reminerilization to
occur.