DR. JAMAL AL-SAIDY
M.B.CH.B…F.I.C.M.S
1
OSTEOCHONDROSIS (OSTEOCHONDRITIS)
The terms ‘osteochondrosis’ or ‘osteochondritis’ have for many years been applied to a group of
conditions in which there is demarcation, and sometimes separation and necrosis, of a small
segment of articular cartilage and bone.
The affected area shows many of the features of ischaemic necrosis, including death of bone cells
in the osteoarticular fragment and reactive vascularity and osteogenesis in the surrounding bone.
The disorder occurs mainly in adolescents and young adults, often during phases of increased
physical activity, and may be initiated by trauma or repetitive stress.
Pathogenesis
Still not completely understood.
Impact injuries can cause oedema or bleeding in the subarticular bone, resulting in capillary
compression or thrombosis and localized ischaemia.
The critical event may well be a small osteochondral fracture, too faint to show up on plain x-
ray examination but often visible on MRI.
If the crack fails to unite, the isolated fragment may lose its blood supply and become necrotic.
Traction injuries may similarly damage the blood supply to an apophysis.
However, it is thought that there must be other predisposing factors, for the condition is
sometimes multifocal and sometimes runs in families.
Types :-
Crushing
Splitting (osteochondritis dissecans )
Pulling ( tractional apophysitis )
Crushing Osteochondritis
This is usually seen in late adolescence, but adults also are sometimes affected.
It is characterized by apparently spontaneous necrosis of the ossific nucleus in a long-bone
epiphysis or one of the cuboidal bones of the wrist or foot.
Local anatomical features (e.g. a metatarsal bone that is longer than usual, or disproportion in the
lengths of radius and ulna) which could result in undue compressive stress being applied to the
bone, can sometimes be identified.
The pathological changes are the same as those in other forms of osteonecrosis: bone death,
fragmentation or distortion of the necrotic segment, and reactive new bone formation around the
ischaemic trabeculae.
Pain and limitation of joint movement are the usual complaints.
Tenderness is sharply localized to the affected bone.
X-rays show the characteristic increased density, accompanied in the later stages by distortion
and collapse of the necrotic segment.
The common examples of crushing osteochondritis have, by long tradition, acquired eponymous
labels:
Freiberg's disease of the metatarsal
Kohler's disease of the navicular
Kienbock's disease of the carpal lunate
Panner's disease of the capitulum.
Perthes disease. of femoral head.
Vertebral osteochondritis (Scheuermann's disease)
DR. JAMAL AL-SAIDY
M.B.CH.B…F.I.C.M.S
2
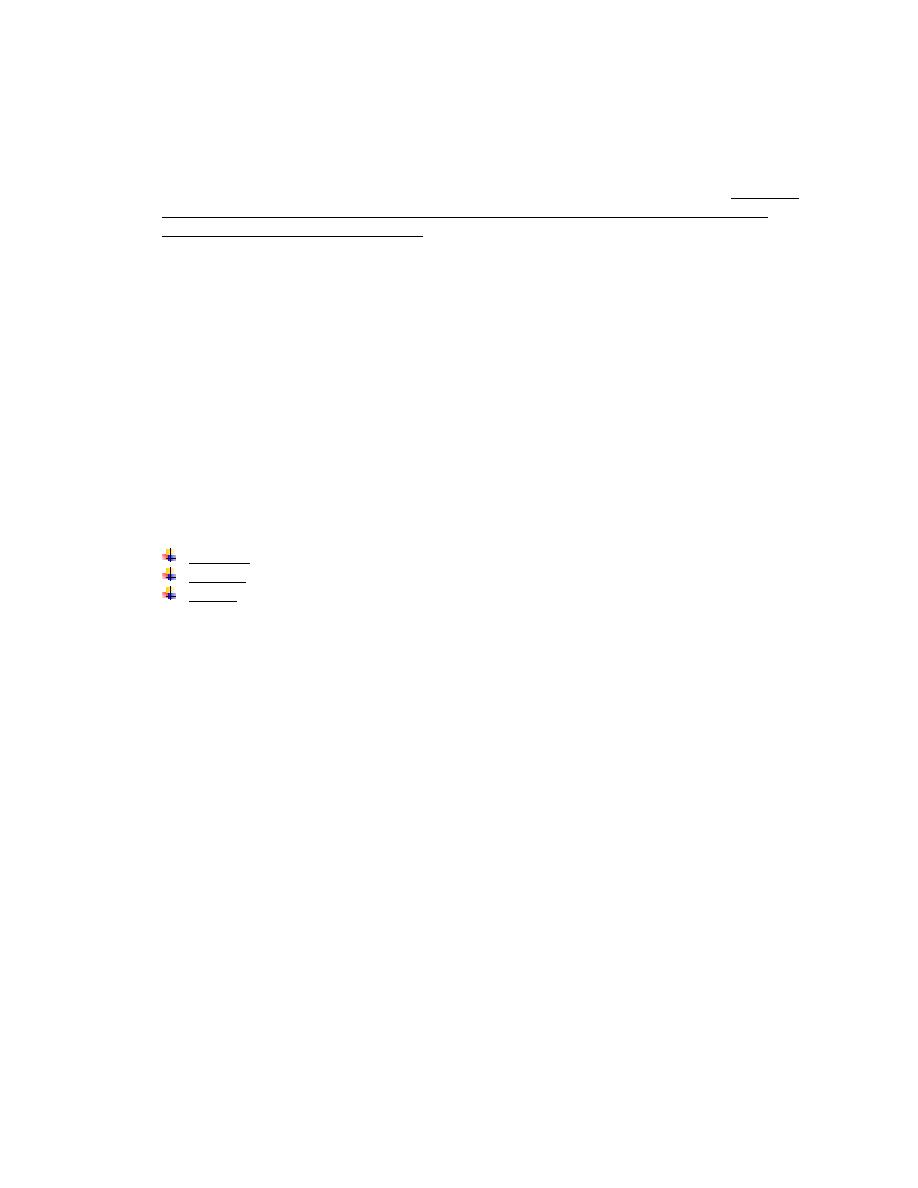
Freiberg'sdisease
Kohler's disease
Kienbock's disease
Vertebral osteochondritis (Scheuermann's disease)
is similar in kind but without clear evidence of bone death.
Compression and fragmentation of the vertebral epiphyseal plates lead to
distorted growth of the vertebral bodies.
The condition occurs during adolescence and may cause back pain and dorsal
kyphosis
X-rays show irregularity or fragmentation of the vertebral endplates; in the
thoracic spine the affected vertebrae may end up slightly wedge-shaped (hence
the kyphosis).
Scheuermann's disease
Splitting Osteochondritis (Osteochondritis Dissecans)
A small segment of articular cartilage and the subjacent bone may separate (dissect) as an
avascular fragment.
This occurs typically in young adults, usually men, and affects particular sites: the lateral surface
of the medial femoral condyle in the knee, the anteromedial corner of the talus in the ankle, the
superomedial part of the femoral head, the humeral capitulum and the first metatarsal head.
The cause is almost certainly repeated minor trauma resulting in osteochondral fracture of a
convex surface; the fragment loses its blood supply.
The knee is much the commonest joint to be affected.
The patient presents with intermittent pain, swelling and joint effusion.
If the necrotic fragment becomes completely detached, it may cause locking of the joint or
unexpected episodes of giving way.
Less frequently, similar episodes occur in the hip or ankle.
DR. JAMAL AL-SAIDY
M.B.CH.B…F.I.C.M.S
3
X-rays
must be taken with the joint in the appropriate position to show the affected part of the
articular surface in tangential projection.
The dissecting fragment is defined by a radiolucent line of demarcation. When it separates, the
resulting 'crater' may be obvious.
The early changes (i.e. before demarcation of the dissecting fragment) are better shown by
MRI
: there is decreased signal intensity in the area around the affected osteochondral segment.
Radionuclide scanning with 99mTc-HDP shows markedly increased activity in the same area.
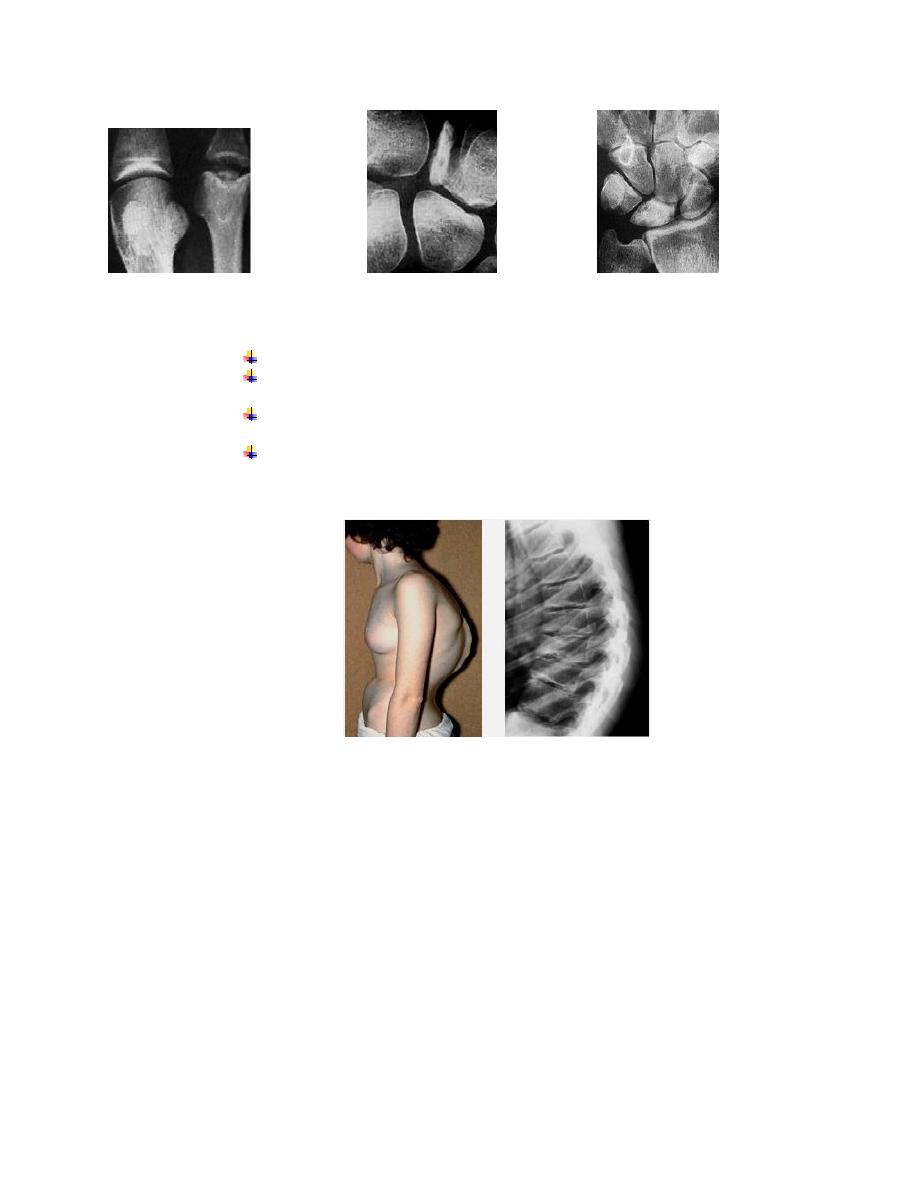
Treatment
In the early stage consists of load reduction and restriction of activity.
In children, complete healing may occur, though it takes up to 2 years.
It is generally recommended that partially detached fragments are pinned back in position after
roughening of the base, while completely detached fragments should be pinned back only if they
are fairly large and completely preserved.
In the knee, these procedures may be carried out by arthroscopy.
If the fragment becomes detached and causes symptoms, it should be fixed back in position or
else completely removed.
Osteochondritis Dissecans (knee)
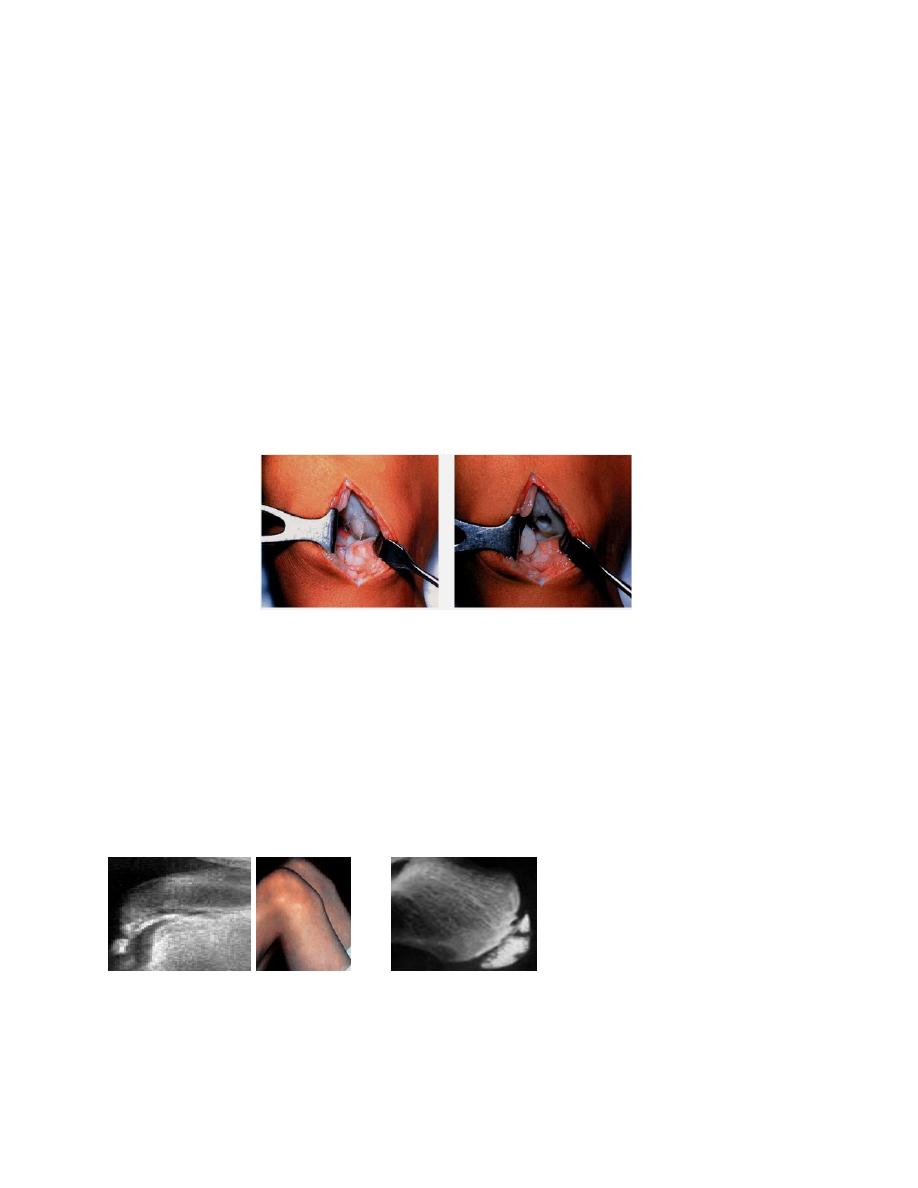
Pulling Osteochondritis (Traction Apophysitis)
Localized pain and increased radiographic density in an unfused apophysis may result from
tensile stress on the physeal junction.
This is seen at two sites:
the tibial tuberosity (Osgood-Schlatter's disease)
the calcaneal apophysis (Sever's disease)
Both are subject to unusual traction forces from powerful tendons which insert into the apophysis.
The bone changes may be a reaction to repetitive local trauma but this never leads to true
necrosis.
Osgood-Schlatter's disease Sever's disease
THANK YOU
Dr. Jamal Al-Saidy
M.B.Ch.B..F.I.C.M.S

DR. JAMAL AL-SAIDY
M.B.CH.B…F.I.C.M.S
4