Secret Lectures
(10)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
1
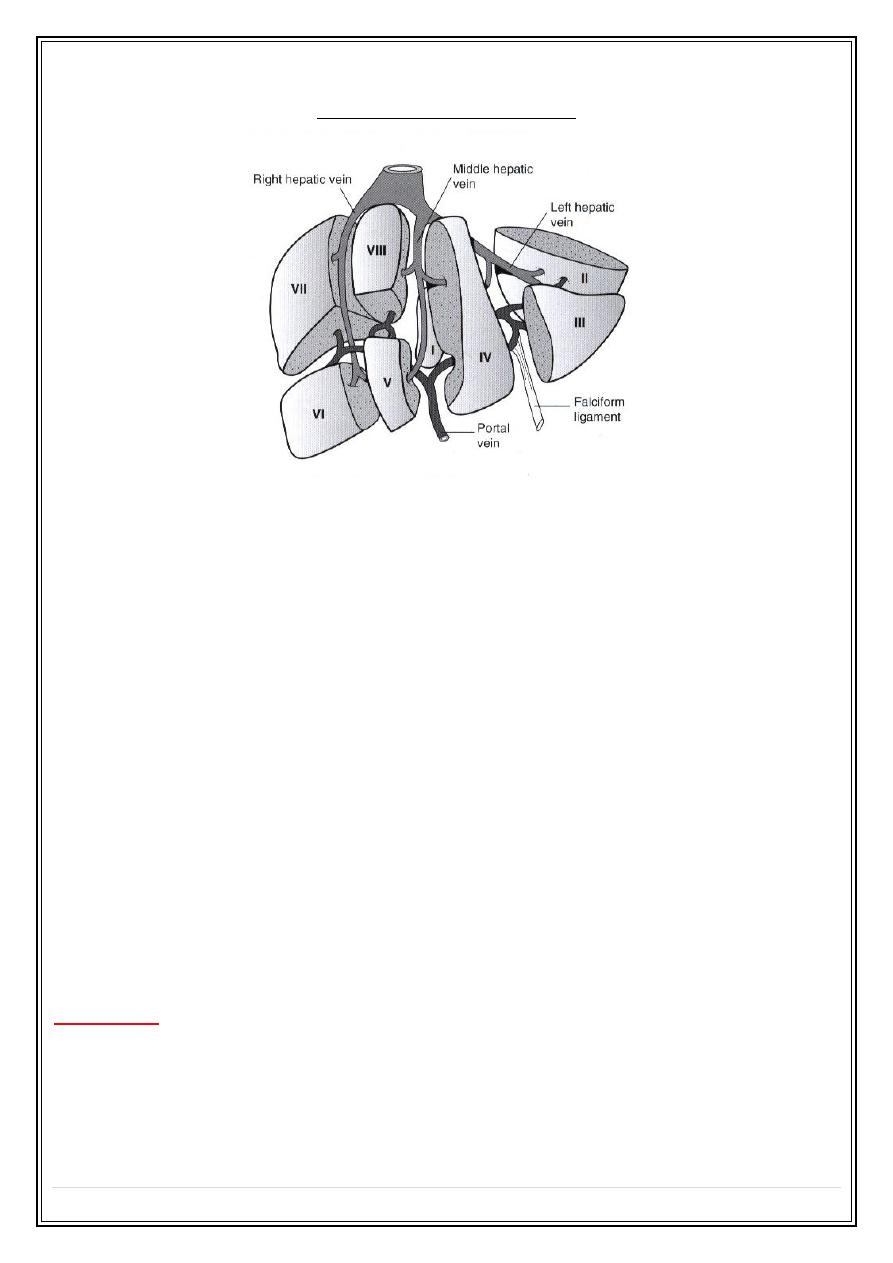
Hepatobiliary system
Imaging techniques
US
:
• Diagnosing focal & diffuse hepatic disease.
• Defining perihepatic fluid collection
• Guidance liver biopsy procedure
Plain abdomen
: Restricted uses in hepatic disease ( shows calcified foci in the liver & some time
shows hepatic enlargement )
CT
: is a superb investigation for most of liver pathology.
MRI
; provide multidisplay information in great range of liver disease and may make successful
diagnosis when other imaging modalities fail. It provides details of vessels and bile ducts with
ever-increasing resolution. MRA being particularly helpful to a surgeon contemplating liver
resection.
Radionuclide scanning
:
Angiography
: now more applicable to interventional technique and therapy ( e.g. embolization of
vascular lesion & transhepatic portosystemic anastomosis-TIPS )
Ultrasound of the liver
:
Focal masses
(
cysts , solid , mixed
"complex ") masses
• Cysts are echo free, have thin or invisible wall.
• Solid or complex masses may be benign or malignant.
• In practice its difficult to differentiate benign from malignant lesions unless the mass is
clearly simple cyst.
• When multiple solid or complex masses are seen within the liver , metastatic disease is
likely diagnosis.
Secret Lectures
(10)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
2
• The prime differential diagnosis of multiple masses are multiple abscesses,
regenerating nodules of cirrhosis of the liver and multiple haemangiomas.
Diffuse parenchymal diseases
: such as diffuse chronic inflammation and diffuse neoplastic
infiltration
CT of the liver
:
•
Native scan
( pre contrast scan )
•
Post contrast scan
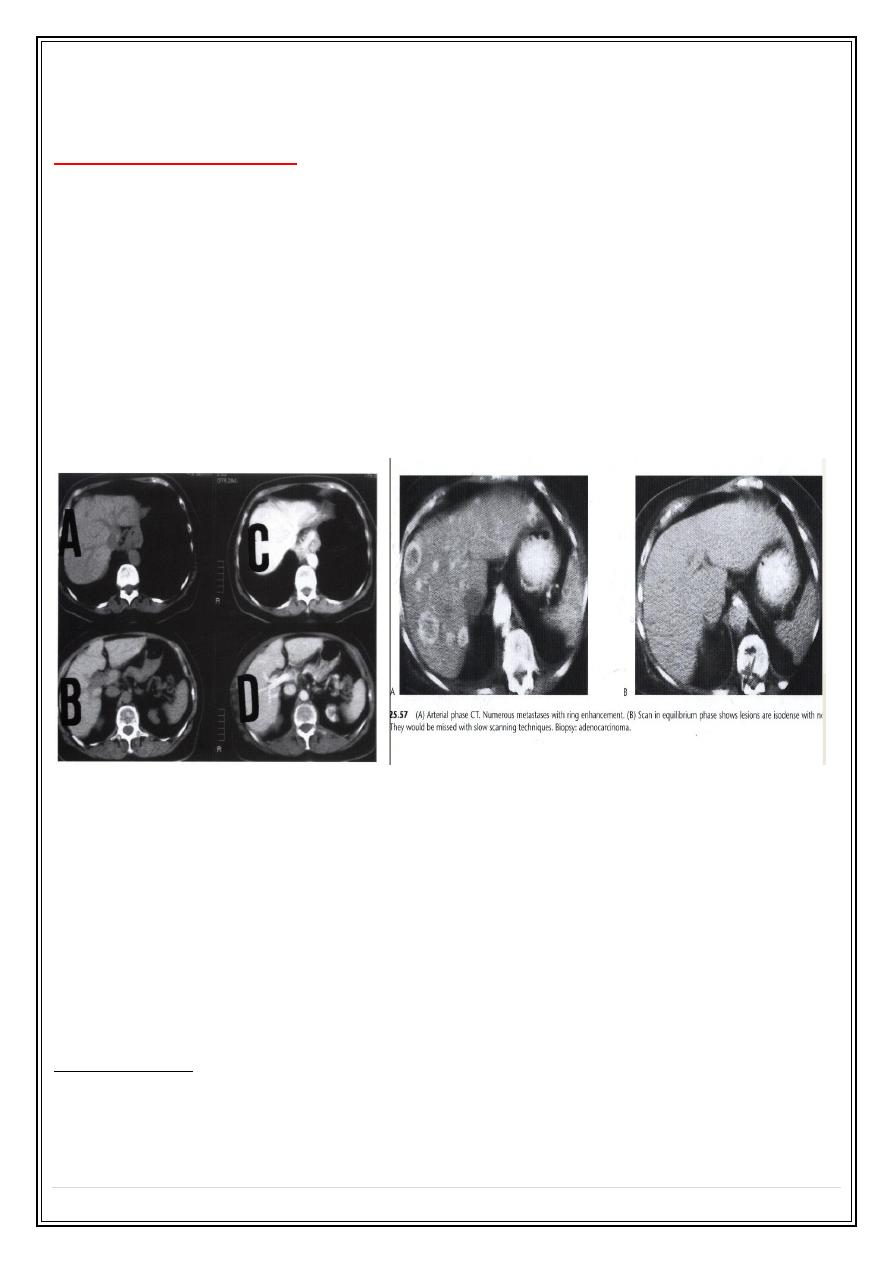
–dynamic-triphasic liver scan (arterial phase "30 sec ", portal phase
"60-70 sec " & delayed scan )
• Most metastases are best demonstrated at portal phase as areas of low
attenuation"hypodense" .
• Scanning during arterial phase will shows lesions such as haemangiomas ( has typical
enhancement pattern – discuss later ) and highly vascular metastases , as areas of
grater enhancement than surrounding parenchyma
MRI of the liver:
•
Used as problem solving to give additional information to US and CT.
•
Multiplanar imaging ( direct axial , coronal and sagittal views ).
•
IV contrast media ( gadolinium -) or new liver specific agent some are taken by
hepatocytes and some taken by reticulo-endothelial cells .
Note : malignant tumors do not normally possesses hepatocytes or reticulo-endothilial
cells , so there is heightened contrast between tumor and normal liver.
Liver masses :
1-
Malignant liver neoplasm
:
• Metastases are more common than primary tumors ( hepatoma and malignant
lymphoma , both of which can be multifocal )
Secret Lectures
(10)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
3
Metastases
:
• Often multiple , peripherally situated and variable sizes.
•
US
#
may
shows
increase
attenuation ( increase echogencity ) (echognic ) (hyperechoic ).
#
more usually
shows
decrease
echogencity ( hypoechoic ).
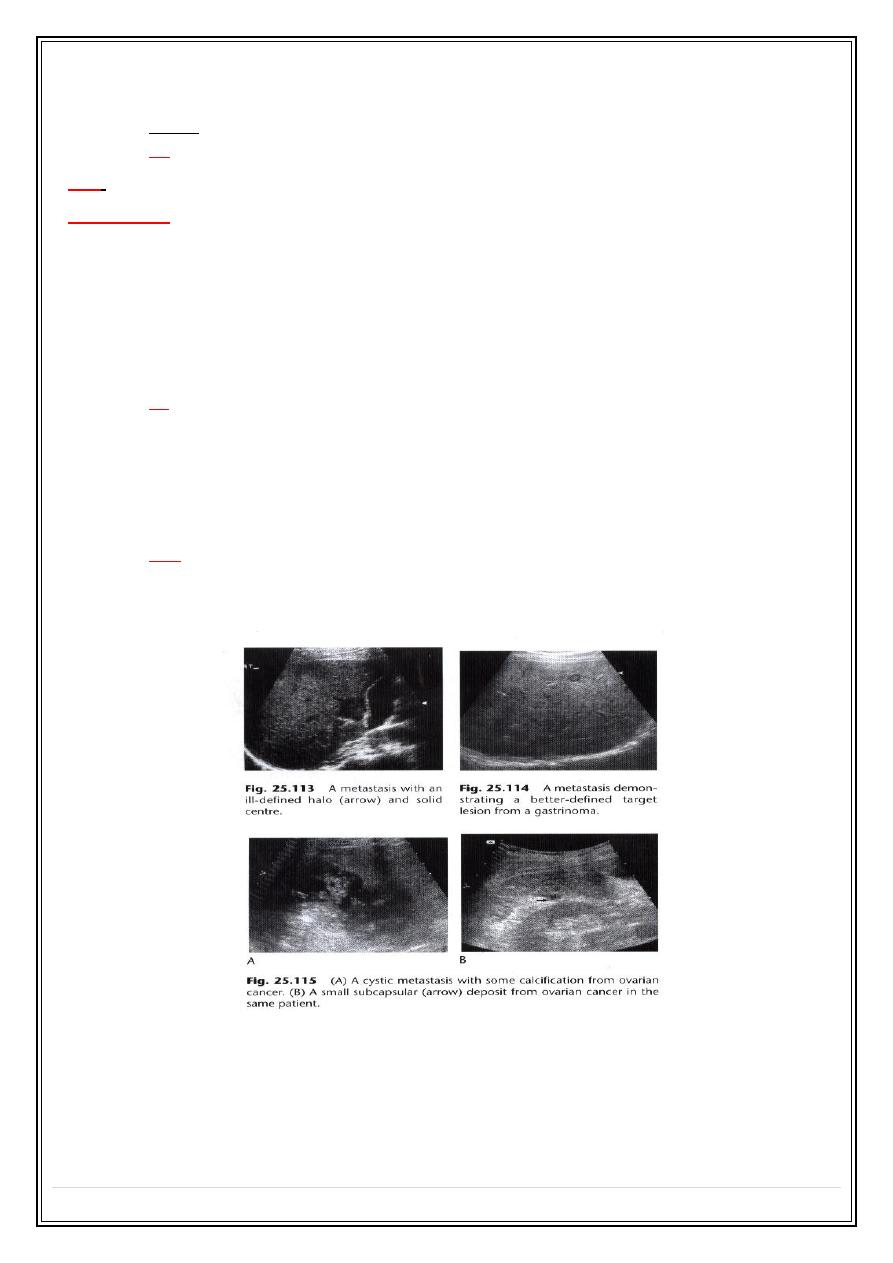
#
At time , they show a
complex echo pattern
.
#
When undergoes central necrosis they
may even resemble cysts
.
#
may
have an echogenic center giving an appearance described as a
target lesion
.
#
some
isoechoic
to surrounding liver parenchyma ( i.e cannot be visualized sonographically )
•
CT
#
usually seen as lower density than the contrast enhanced surrounding liver parenchyma.
#
intense contrast enhancement some time seen within the tumor or immediately surrounding
them- a useful differentiating feature , which is not seen with cysts.
#
some metastases ( e.g. carcinoid )are hypervascular and appear as high density areas.
•
MRI
#
most shows lower signal than surrounding liver (
hypointense) on T1-weighted
scan and a high
signal (
hyperintense ) on a T2-weighted
scan.
Primary carcinomas
of the liver, which include hepatocellular carcinoma and cholangiocarcinoma
are often large and usually solitary but they may be multifocal. CT, US and MRI features are
similar to metastatic neoplasm
Secret Lectures
(10)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
4
2-
Benign liver masses
:
- Most are cysts , some are haemangiomas . focal nodular hyperplasia are rare but can closely
resemble malignant masses.
-
Liver cysts
;
•
Simple liver cysts :
#
single or multiple , usually congenital , some due to
infection.
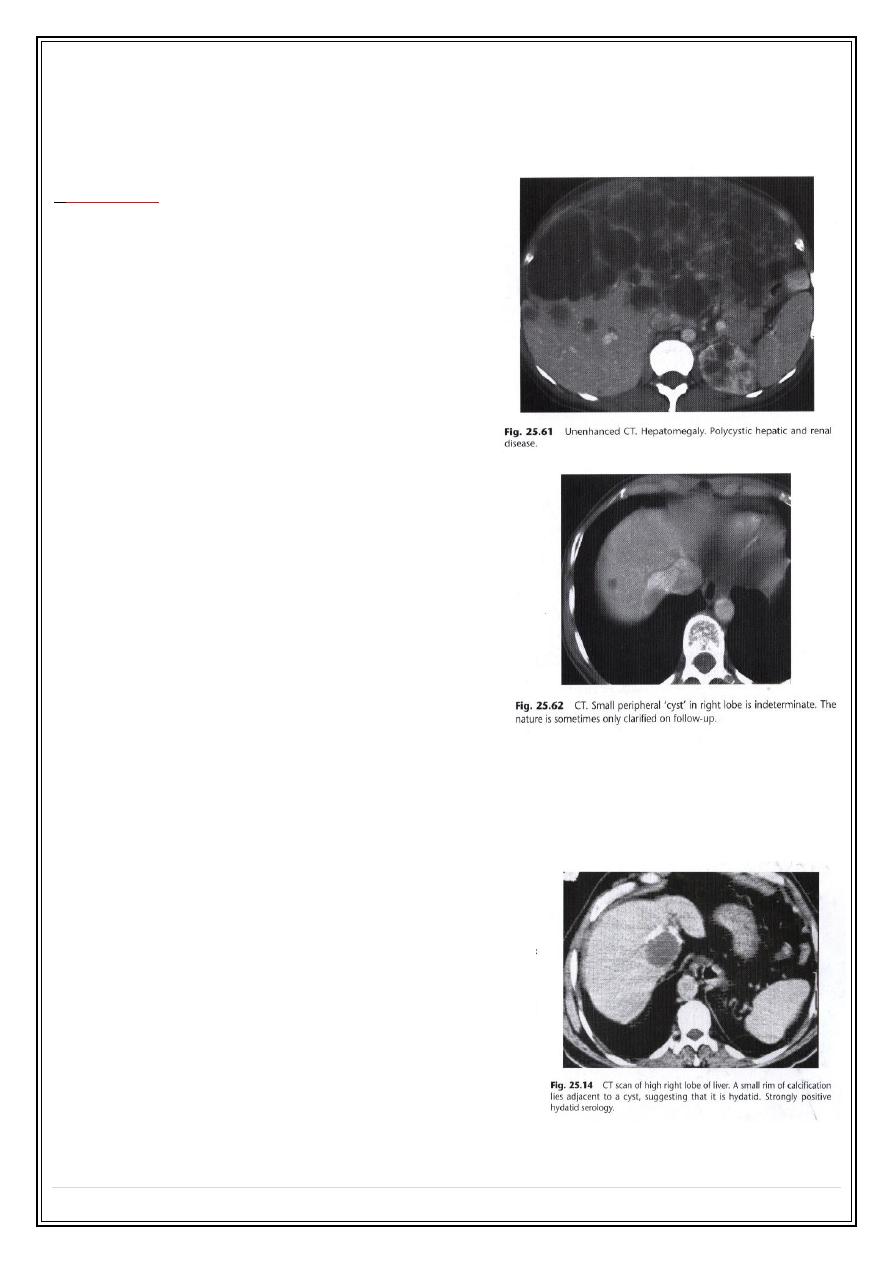
#
multiple hepatic cysts occur in polycystic disease (
not only affect the kidney but may also affect the
liver and other organs )
#
at
US
: typical features of cysts elsewhere (
sharp
margin
, no echo within the lesion "
anechoic
",
intense echo from the front and back walls with
acoustic enhancement
deep to the larger cysts.
#
at
CT
: very well defined margins , attenuation value
similar to that of water (HU=0-15 ). Its often not
possible to characterize small lesions and with
lesions below 1 cm in diameter its almost never
possible to distinguish cyst from neoplasm.
#
at
MRI
: low signals on T1-W and high signal on T2-W
•
Hydatid cysts:
# may be single or multiple
# some shows
calcific wall
, some shows
daughter cysts
and
some shows
internal undulating membrane (waterlily
sign )
# unless these features are present (
some time H.cyst
resemble simple cyst criteria
), H cysts may prove
indistinguishable from simple cysts at both US and CT
# Response to medical therapy include : reduction in size of
cyst , membrane detachment , progressive increase in
cyst reflectivity, and wall calcification.
•
Occasionally metastases can have a cystic
appearance.
Secret Lectures
(10)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
5
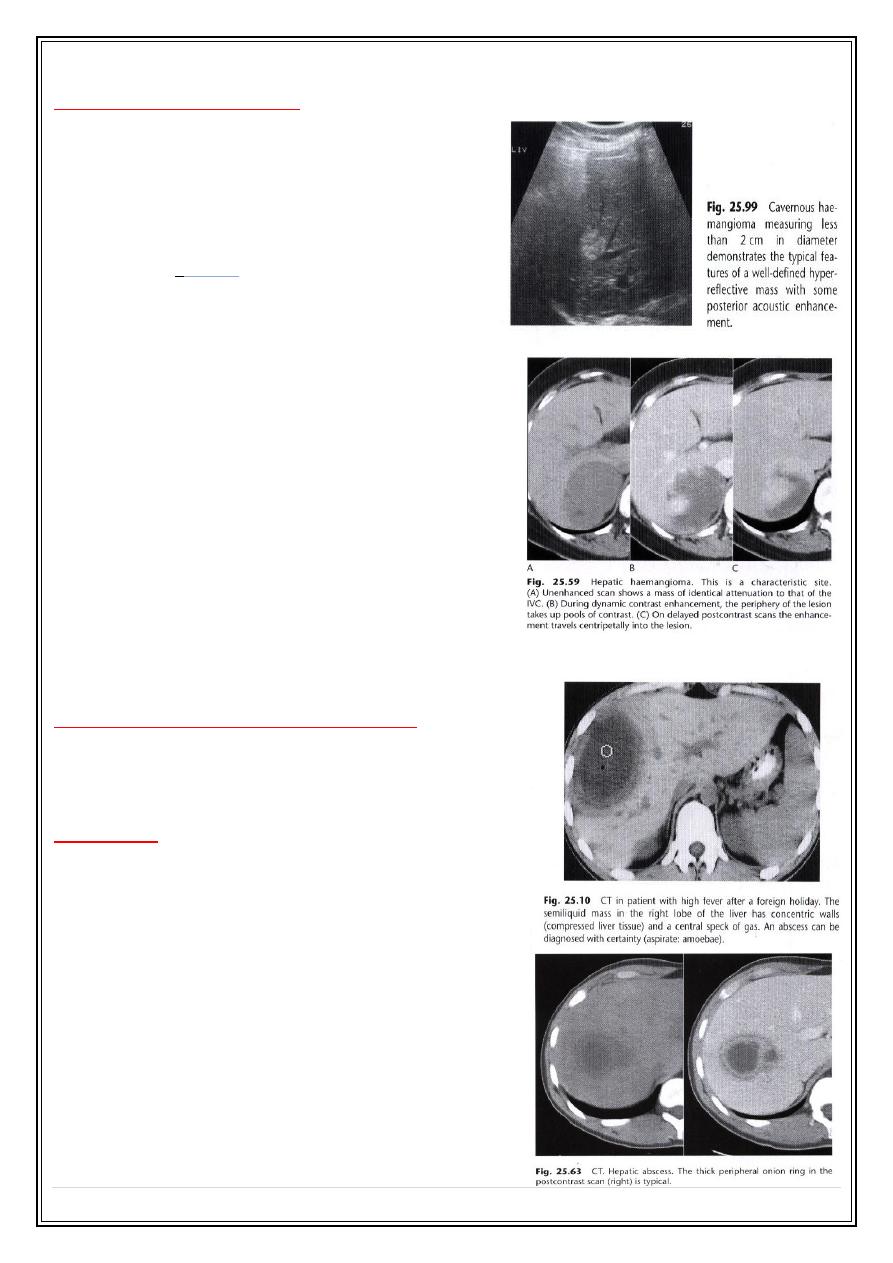
Haemangiomas of the liver
• Often incidental finding, single or multiple
, occasionally can cause significant
hemorrhage , especially following trauma
therefore percutanous biopsy should be
avoided.
•
Resemble neoplasm and other masses at
US
,
usually hyperechoic and well defined
.
• At
native CT
scan : appears rounded low
density.
• On
dynamic Post contrast CT or MRI
:
early shows nodular peripheral nodular
enhancement , slow centrepital filling on
next few min scan then became similar to
surrounding liver.
• Giant haemangiomas : >6 cm shows central
irregular necrotic non enhancing core.
• Small haemangiomas : <1 cm may give
similar post contrast features to other liver
masses and cannot be differentiated.
• On
MRI
shows uniform very high intensity on
T2-W , a characteristic that is shared with
benign cysts , but very unusual with malignant neoplastic lesions.
Adenoma and focal nodular hyperplasia
• Both of these conditions appear as enhancing
masses on CT.
Liver abscess
:
• Hepatic abscess tend to have fluid centers ,
with walls that are thicker , more irregular and
more obvious than those of simple cysts.
• At
CT
: the core fluid have attenuation values
may be same as water , usually they are
higher .
• At
US
: necrotic debris may be seen within the
abscess.
• Occasionally chronic abscess calcify.
• Abscess cannot usually be differentiated from
necrotic tumor by US,CT or MRI, clinical
situation should be aid in distinction.
Secret Lectures
(10)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
6
Cirrhosis of the liver and portal hypertension:
• In portal HT the pressure of portal venous pressure is elevated due to obstruction to
the flow of blood in the portal or hepatic venous systems.
• Cirrhosis of the liver is by far the commonest cause.
• Other causes include occlusion of hepatic veins (Budd-Chiari syndrome ) and
thrombosis of portal veins, particular following infection of the umbilical vein in
neonatal period.
• Portosystemic anastomosis collateral may follow to enter the vena cava by passing the
liver , the most important of these are varices at lower esophagus. And these can be
shown with color Doppler US.
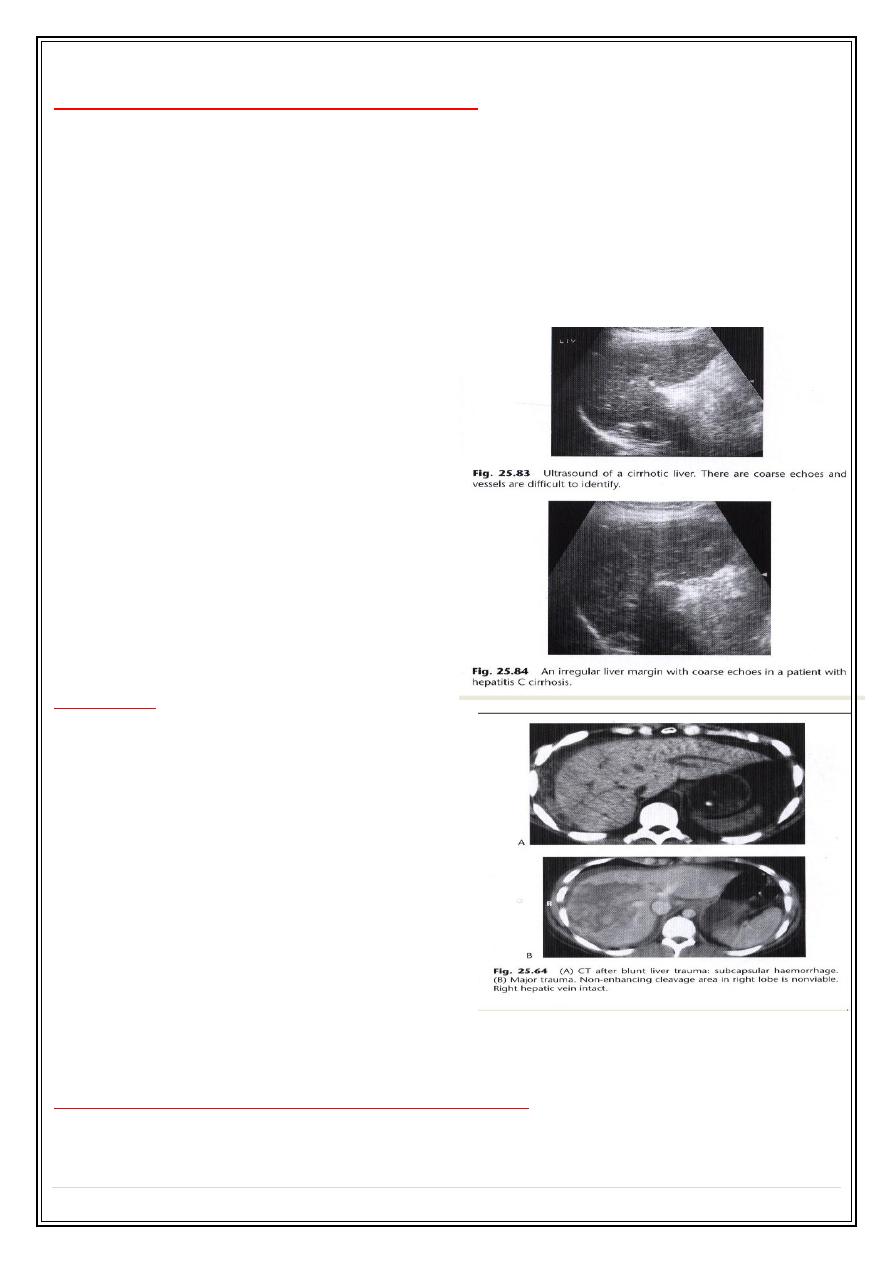
•
The signs of cirrhosis of liver at CT
and US
are
reduction in the size of Rt
lobe of the liver and irregularity
of
liver surface , together with
splenomegal
y .
•
Ascite
s may be present.
•
Liver texture at US
may be diffusely
abnormal while on CT appears
normal until late in the disease.
• Patency of splenic , portal and
hepatic veins can be assessed with
Doppler US , CT or MRI.
Liver trauma :
• Is the commonest abdominal injury
that leads to death.
•
Features are :
parenchymal lacerations ,
subcapsular and intrahepatic
haematomas.
• Lacerations and haematomas are
recognized as
low density areas
relative
to the contrast enhanced parenchyma ,
leakage of contrast indicate active
bleeding .
• Although US and MRI can demonstrate
liver injury ,
CT is the best technique
,
which can survey other organs like
spleen and kidneys. And identify any peritoneal fluid collection.
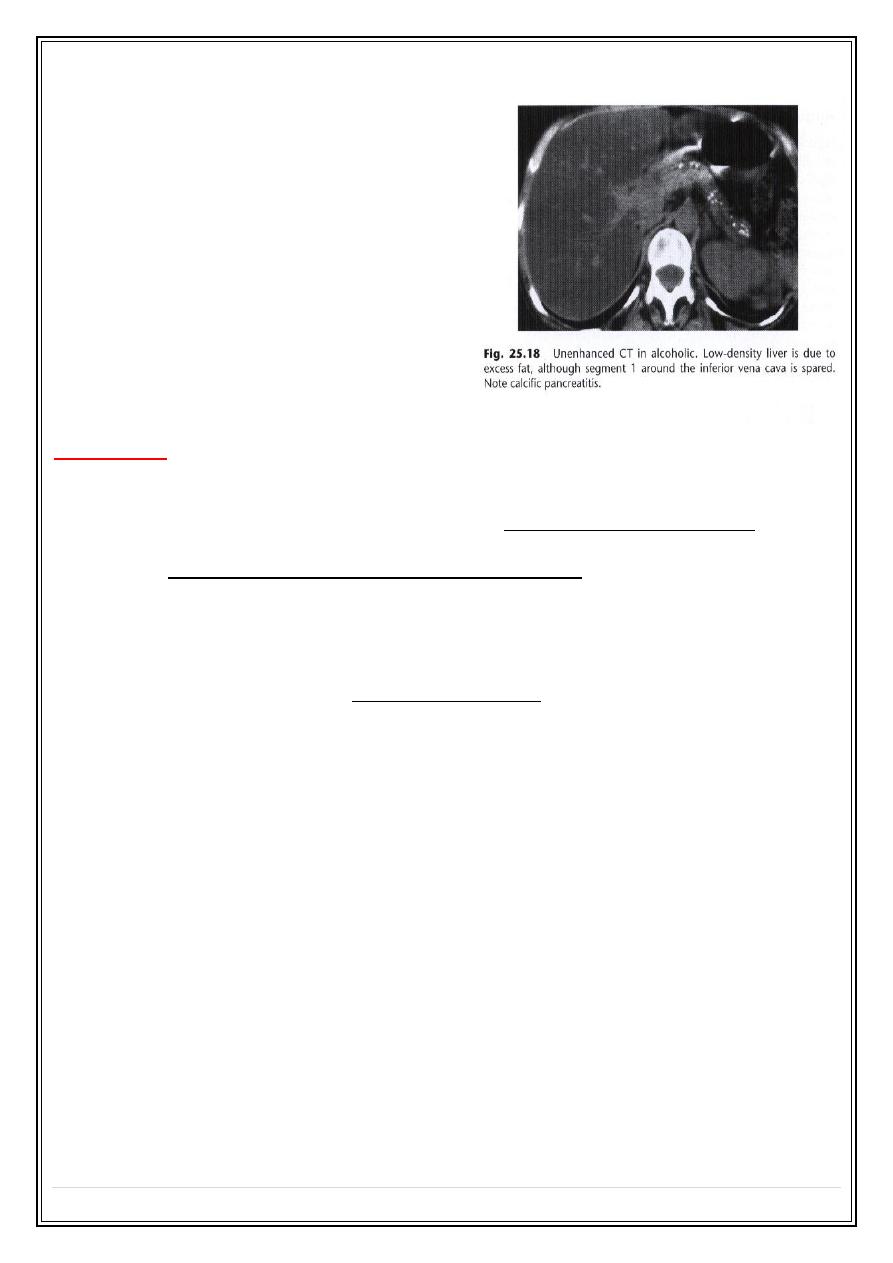
Fatty degeneration ( or infiltration ) of the liver :(steatosis )
• Commonly seen in patient with
diabetes
mellitus and
alcoholics
. other include
obesity
,
hyperlipedaemia , parentral nutrition, severe hepatitis and chemotherapy.
Secret Lectures
(10)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
7
• On
US
:causing increase liver
reflectivity (bright liver ), poor
definition of posterior liver and hepatic
veins . the liver will be enlarged in 75-
80%.
• On
CT
appear as reduction of
attenuation (low density) , and vessel
more prominent (due to reduction of
back ground of parenchymal density )
•
MRI
can be very helpful because fat
gives characteristic set of signals.
• Fatty infiltration may be diffuse , focal ,
or diffuse with focal sparing areas.
Viral hepatitis :
• In acute viral hepatitis the liver is enlarged in 70%, splenic enlargement in 20% of
cases.
• By US : liver parenchyma
usually normal
and decrease echogencity in severe cases and
portal vessels more echogenic than normal. GB wall thickened may also be observed.
•
In Sever chronic hepatitis there is increase echogencity of the liver parenchyma
undifferentiated from fatty infiltration ,
Biliary system :
Imaging investigations:
•
US
: is the best and primary method of investigation ,because simplest and excellent
method in showing gallstones and diseases of gallbladder also an excellent test for
confirming or excluding bile duct dilatation.
patient should be fasting 6—8 Hrs prior to
procedure to fully distend the GB .
•
Radionuclide
imaging using hepatobiliary agents ( e.g. 99m TC-HIDA ). Hepatic
excretion occurs despite relatively high serum bilirubin levels, and, therefore, these
agents can be used when the patient is jaundiced, even with serum bilirubin levels of
up to 250 μmol/L (15 mg%). The main use of this technique is in patients with
suspected biliary leak following biliarysurgery. The technique may also be used in acute
cholecystitis (with nonfilling of the gall bladder in cases of an impacted stone in the
cystic duct) or in children, when biliary atresia is suspected.
•
CT
: GB wall thickening , gall stones and dilatation of common duct all can be recognized
at CT , but US produced better information , because pure cholesterol stone density
may approach that of fat and difficult to appreciated with CT.
•
MRI and MRCP
: excellent in visualization of biliary radicles , equivocal US and CT
results and may be diagnostic in non dilating biliary disorders .the examination is non
invasive and
no contrast needed .
Secret Lectures
(10)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
8
•
PTC ( percutanous cholangiography ):
reduced now a day as a diagnostic method &
mostly replaced by ERCP &MRCP is generally performed if an
- ERCP is unsuccessful in treating a distal common bile duct (CBD) obstruction or
-
as the primary procedure in treating a more proximal hilar stricture.
Chiba needle under fluoroscopic or US guide. With local anesthesia
Haemorrhage is an occasional problem,as are septicaemia and biliary peritonitis.
•
ERCP
: advantage is biliary & pancreatic ducts are studies , allow direct inspection and
biopsy of papilla and duodenum & therapeutic procedure of sphencterectomy & stone
extraction , endoscopic basket or balloon extraction & stint placement.
It is still occasionally used for more detailed imaging of the intrahepatic biliary ducts as
resolution is better than with MRCP (e.g. in sclerozing cholangitis). Pancreatitis is an
occasional complication of ERCP.
•
Operative cholangiography . & post-operative T-tube cholangiography.
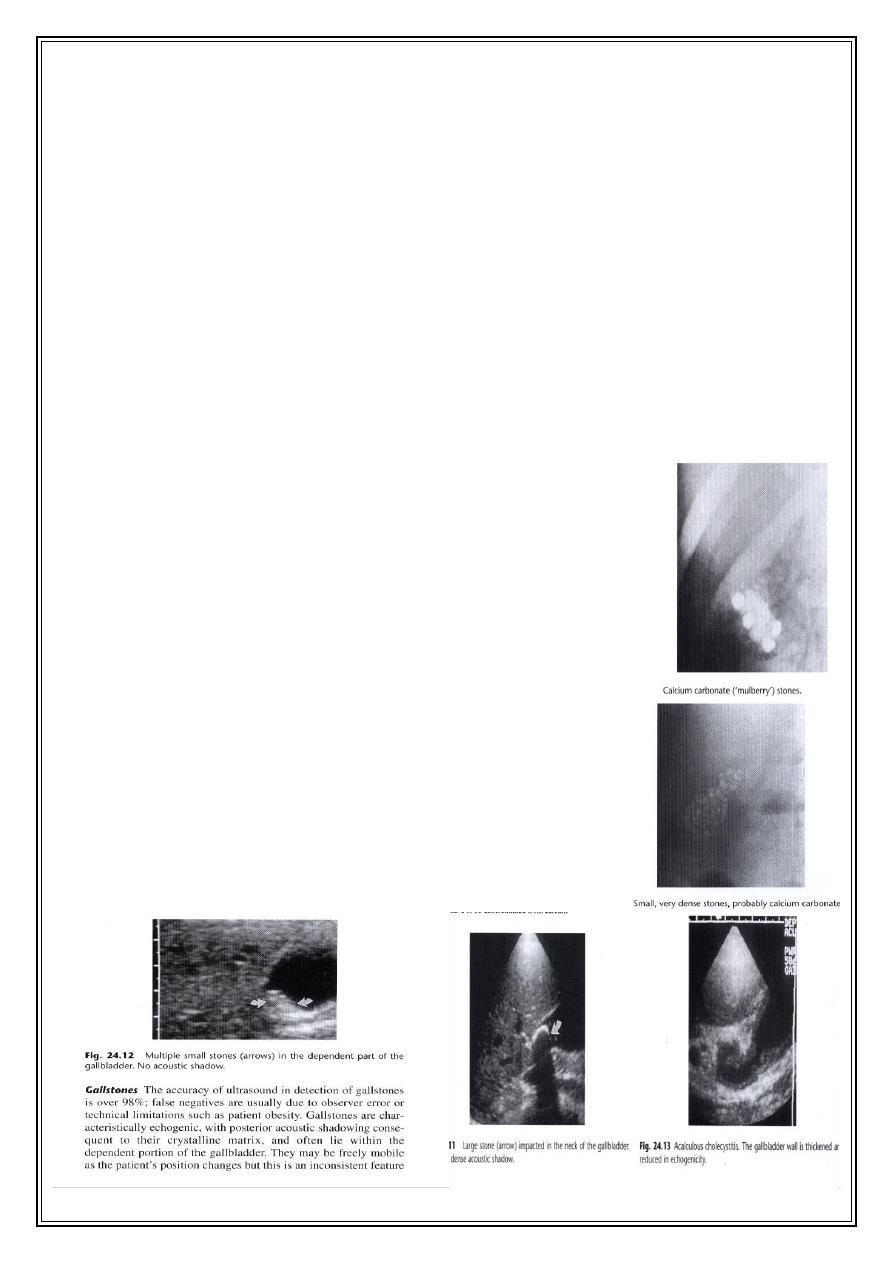
Gall stones and cholycystitis
:
• Gall stones are frequent finding in adults , particularly in
middle age female. Together with accompanying chronic
cholecystitis they are a major cause of recurrent upper
abdominal pain .
• 20% of gall stones contain sufficient calcium to be visualized
by plain film.
• At
ultrasound
, gallstones are seen as a strongly
echogenic
foci
within the dependant portion of gall bladder .
acoustic
shadow
usually
seen behind stones..
• Acoustic shadows is an important sign, not seen with polyp. Most polyps are small
measuring only few millimeters and are not neoplasms but aggregation of cholesterol.
• US very accurate in detecting gall stones but less reliable for detecting stones in the
common bile duct.
•

Secret Lectures
(10)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
9
Calculus cholecystitis :
• In acute cholecystitis , sonography will usually detect
gall ston
es , inflammatory debris
"
biliary sludge
" and
gall bladder wall thickening
.
• Unless there is
visible edema adjacent
, ultrasound cannot distinguish acute from
chronic cholecystitis. In acute cholecystitis pain is often localized to gallbladder
(ultrasonic Murphy sign). Also
in chronic cholecystitis the GB is contracted.
• No available test to be very good in diagnosing gallbladder inflammation , but since
the cystic duct is always obstructed in acute cholecystitis , a normal hepatobiliary
radionuclide scanning exclude the diagnosis.
• An empyemia or mucocoele may results if there is continuing cystic duct dilatation.
• Perforation may results give rise to localized abscess or biliary peritonitis.
• Infection with specific coliform organism or clostridium welchii may resuls in
emphysematous cholecystitis
, particularly in patient with DM and
immunocompramized with mural air seen on plain abdomen or CT.
• Fistulation may occur to small or large bowel with associated enteric obstruction
termed gallstone ileus.
Secret Lectures
(10)
/ Diagnostic Imaging / Dr.Riyadh A. Al-Kuzzay (M.B.Ch.B – FICMS-RD)
P a g e
10
Jaundice:
• Imaging test may be required when there is doubt as the nature of jaundice.
• The basis of this distinction is that dilated biliary ducts are a feature of jaundice from
biliary obstruction.
• Most often the imaging is used to determined the site and possible cause of such
obstruction.
• The causes of large duct obstruction :
- Impacted stone in the common bile duct.
- Carcinoma of the head of pancreas.
- Carcinoma of ampulla of vater
• Dilatation of the intra- and extra-hepatic biliary system can be identified at both US
and CT. US is more sensitive test and is usually the 1
st
test to be performed.
• The CBD located just infront of portal vein and is dilated when more than 7 mm in
diameter ( some books 8 mm , and range of 6—8 mm is equivocal , vey rarely normal
ducts seen up to 12 mm , especially in post cholectectomy , elderly )
• More often the cause of obstruction cannot be seen because of overlying gas in
duodenum especially in distal portions.
• CT may be helpful in such cases but MRCP is exceedingly better.
• Substantial dilatation of common hepatic and CBD may be present with only minimal
dilatation of intrahepatic biliary ducts & also the intrahepatic biliary tree may not
dilate at all within the 1
st
48 Hrs following obstruction.
• ERCP provide excellent diagnostic & interventional procedure in obstructive jaundice.
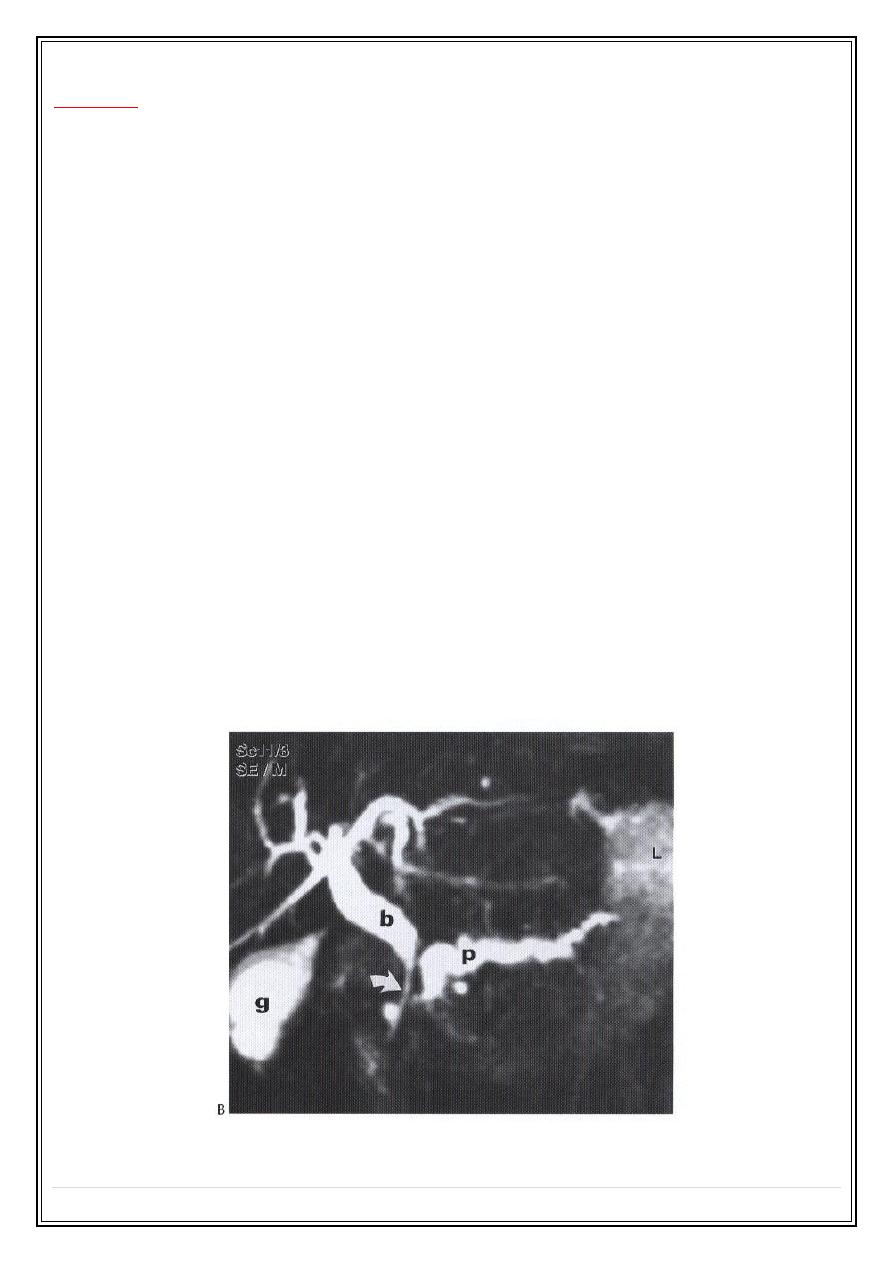
MRCP- stricture cholangiocarcinoma:
Thank you,,,