ENT Emergencies
THE EAR
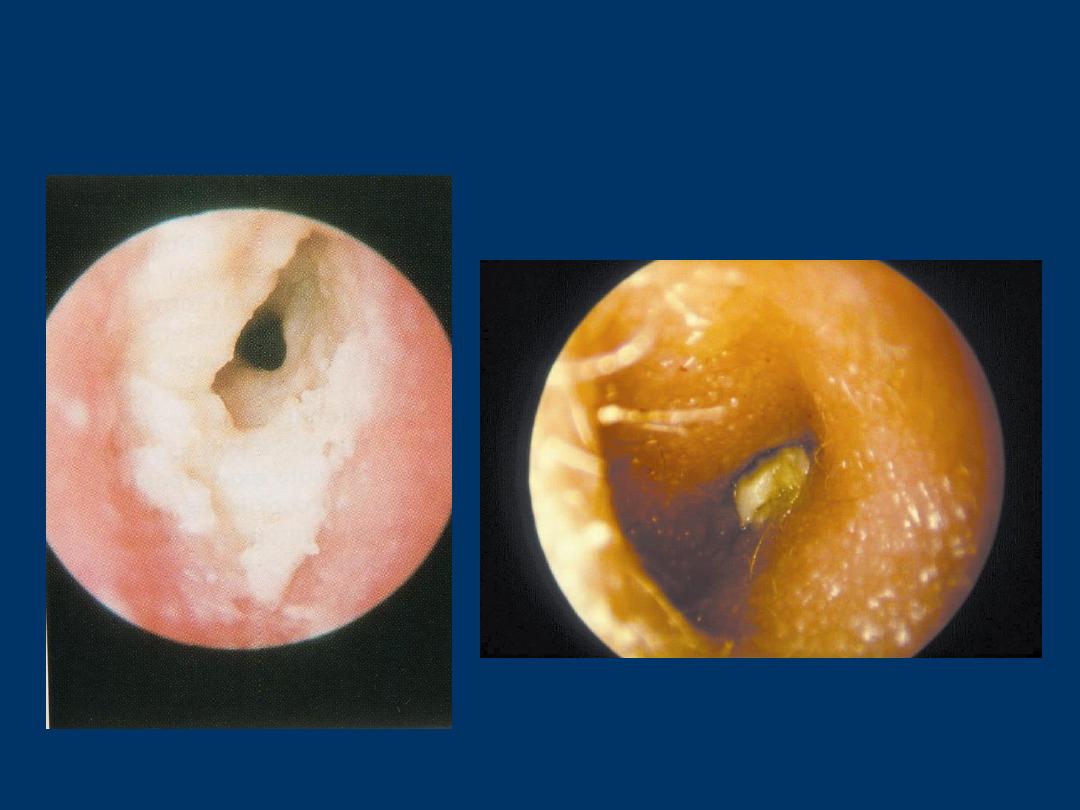
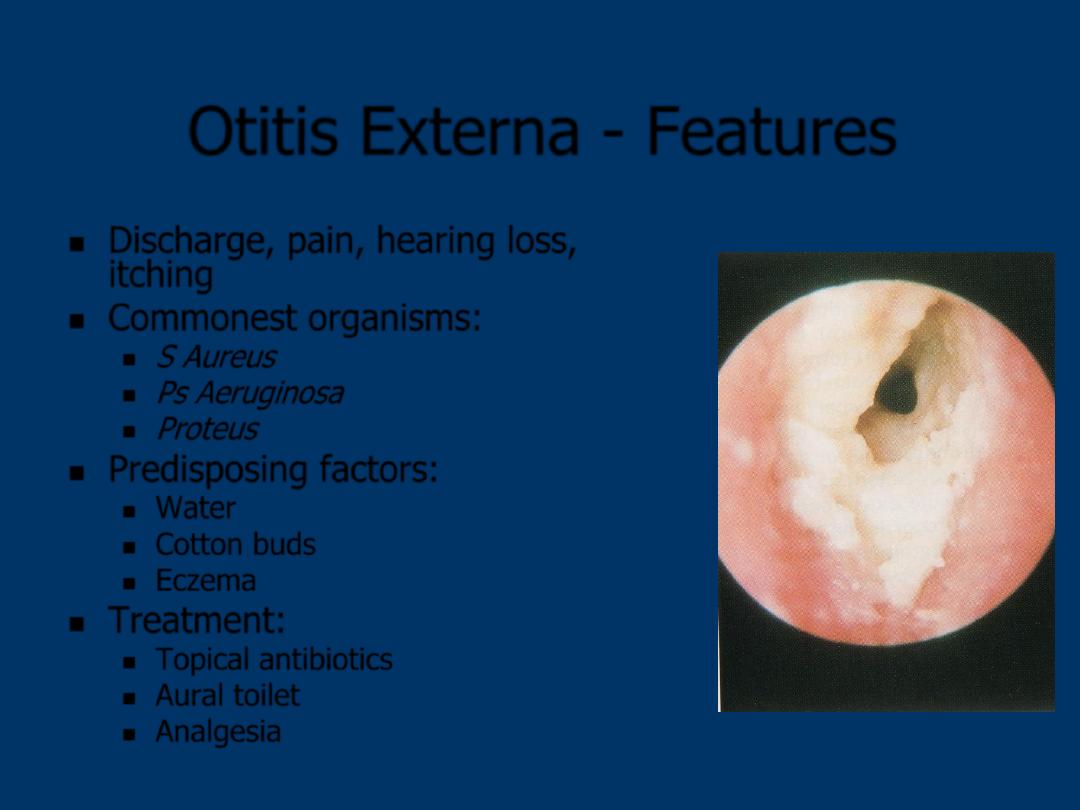
Otitis Externa - Features
Discharge, pain, hearing loss,
itching
Commonest organisms:
S Aureus
Ps Aeruginosa
Proteus
Predisposing factors:
Water
Cotton buds
Eczema
Treatment:
Topical antibiotics
Aural toilet
Analgesia
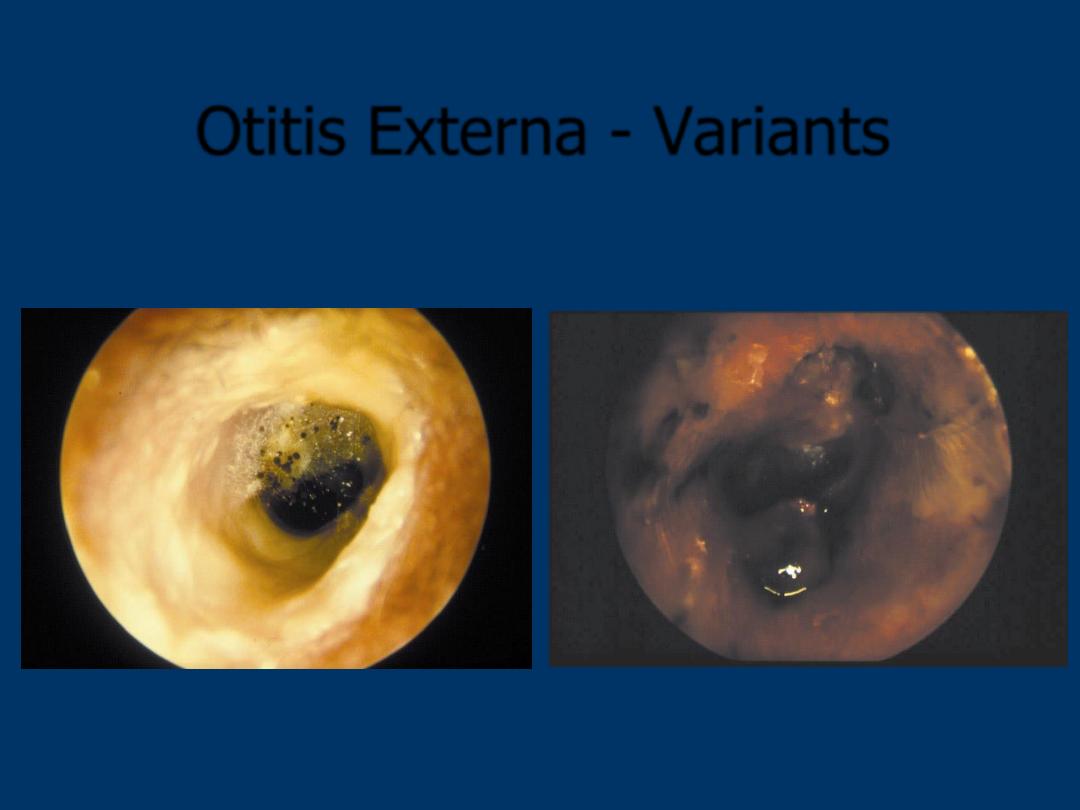
Otitis Externa - Variants
Fungal
Malignant OE
- Diabetes
- VII palsy
Malignant Otitis Externa
Risk factor – Diabetes
Granulomatous polypoid otitis externa
Disproportionately severe pain
Associated features:
Cranial nerve involvement – VII, IX, X, XI, XII
Treatment:
Topical antibiotics and aural toilet
i.v. antibiotics > 6/52
Hyperbaric oxygen
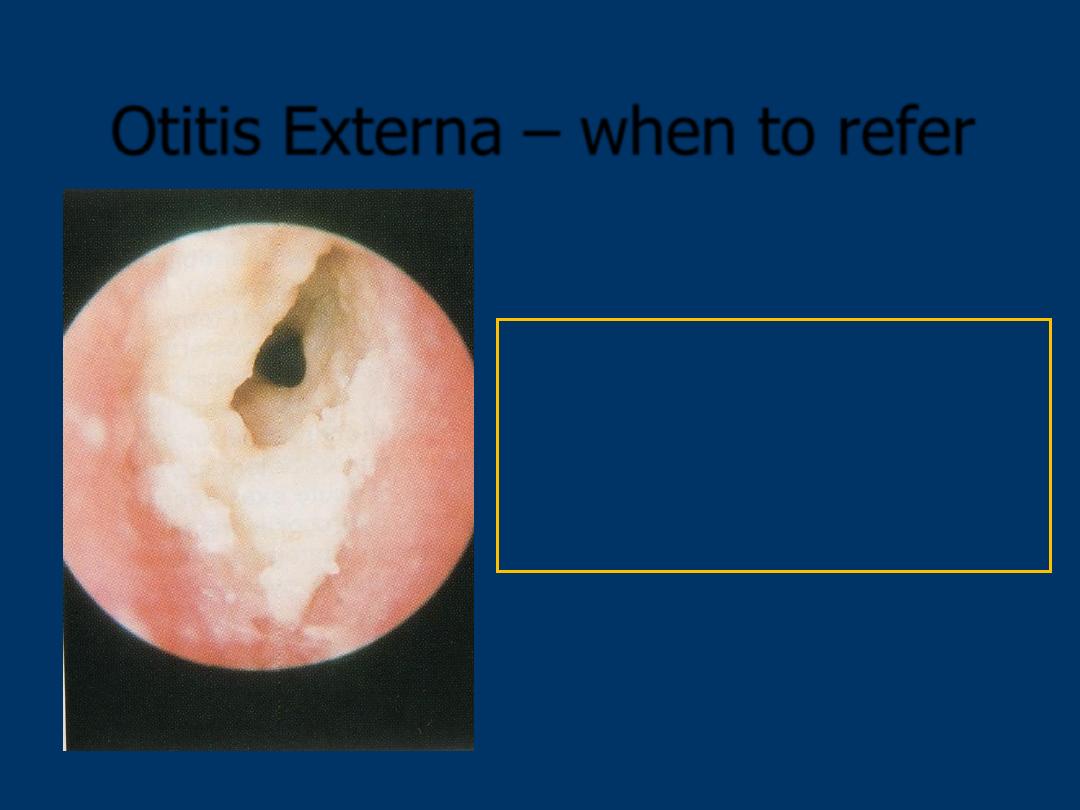
Otitis Externa – when to refer
Refer if
: Non responsive
Canal oedematous
Needs aural toilet
Suspicion of malignant OE

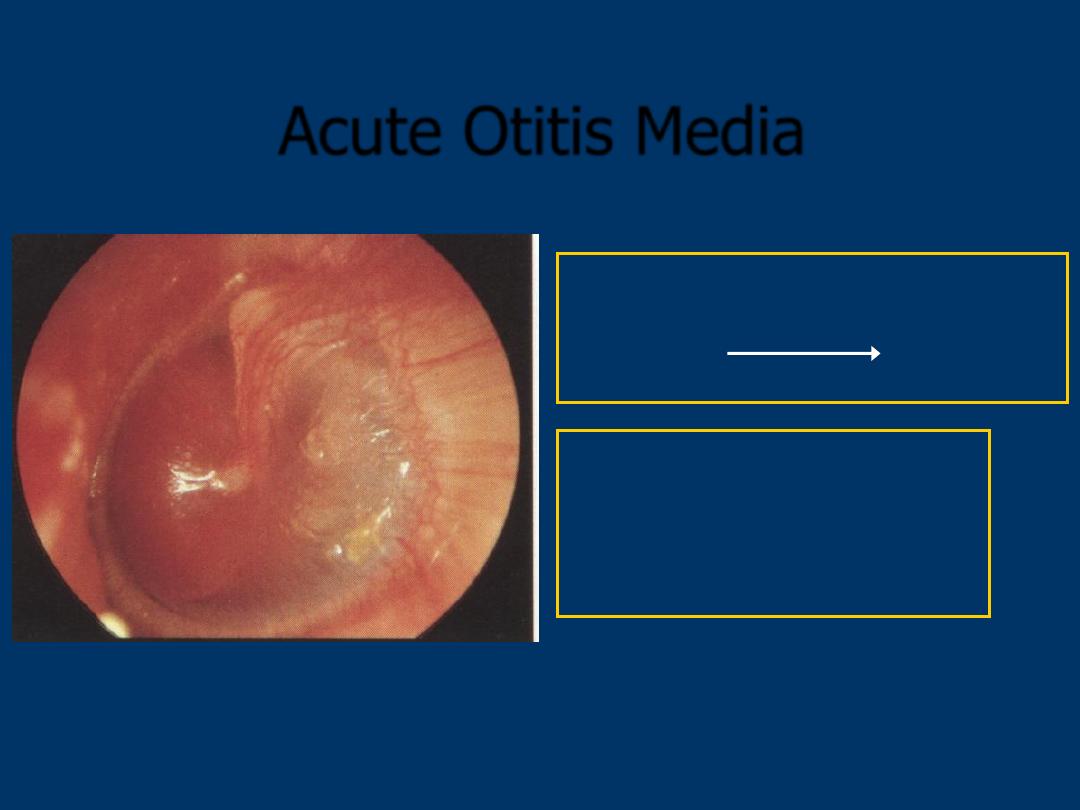
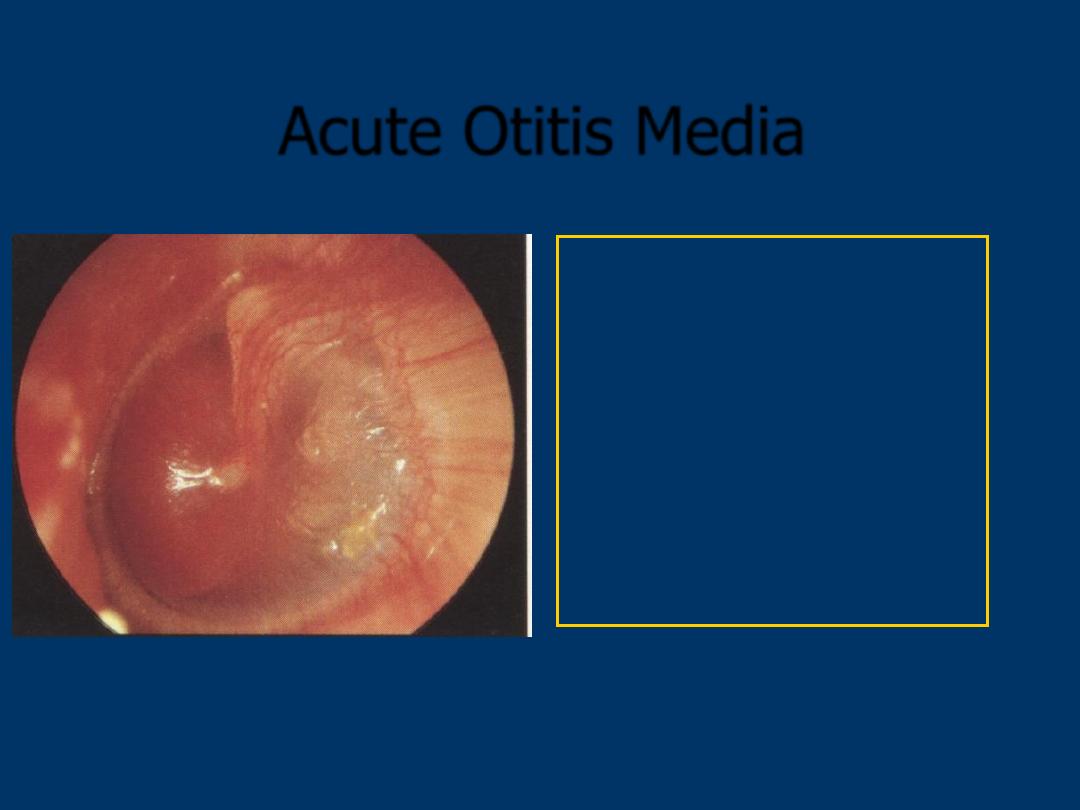
Acute Otitis Media
Rx
:
Systemic antibiotics
Analgesia
Decongestants
Symptoms:
Pain
Discharge
Hearing loss
Pain subsides
Acute Otitis Media
When to refer?:
•
Failure of resolution
• Persistent discharge
• Complications
•
VII palsy
• Mastoiditis

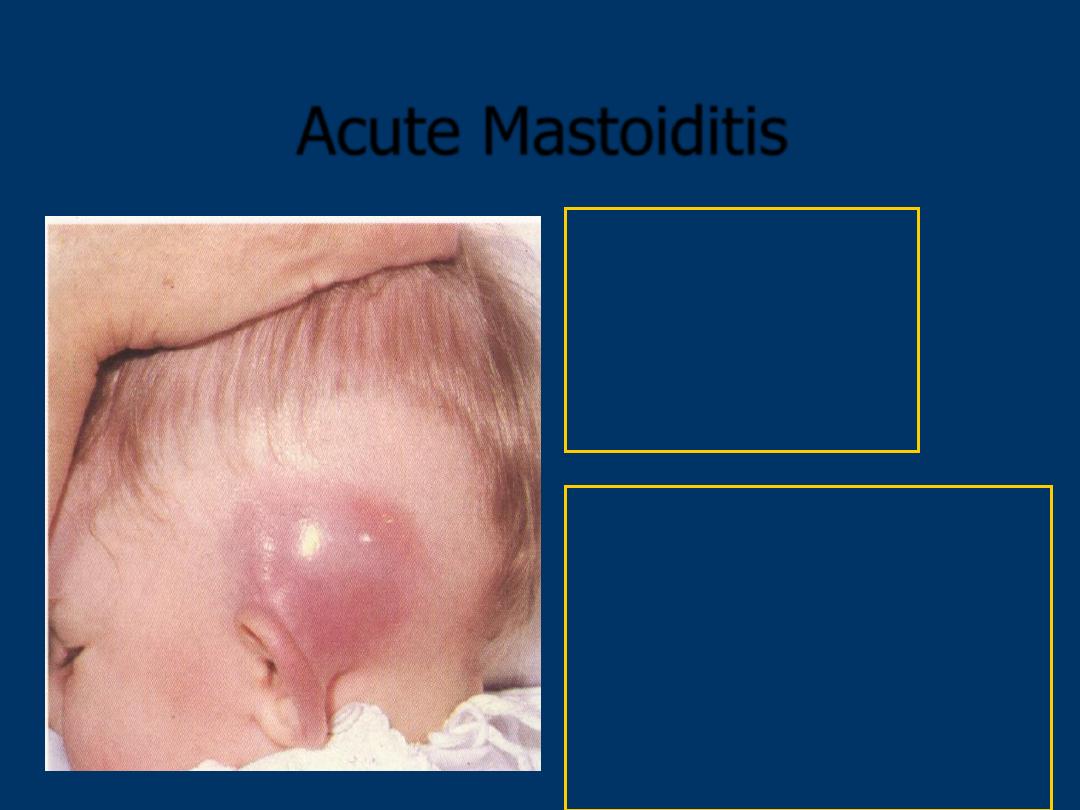
Acute Mastoiditis
Rx
: Systemic antibiotics
Analgesia
drainage
URGENT REFERRAL
Features
Recent URTI
Ear discharge
Blunting of postaural sulcus
Fluctuant tender swelling
Fever

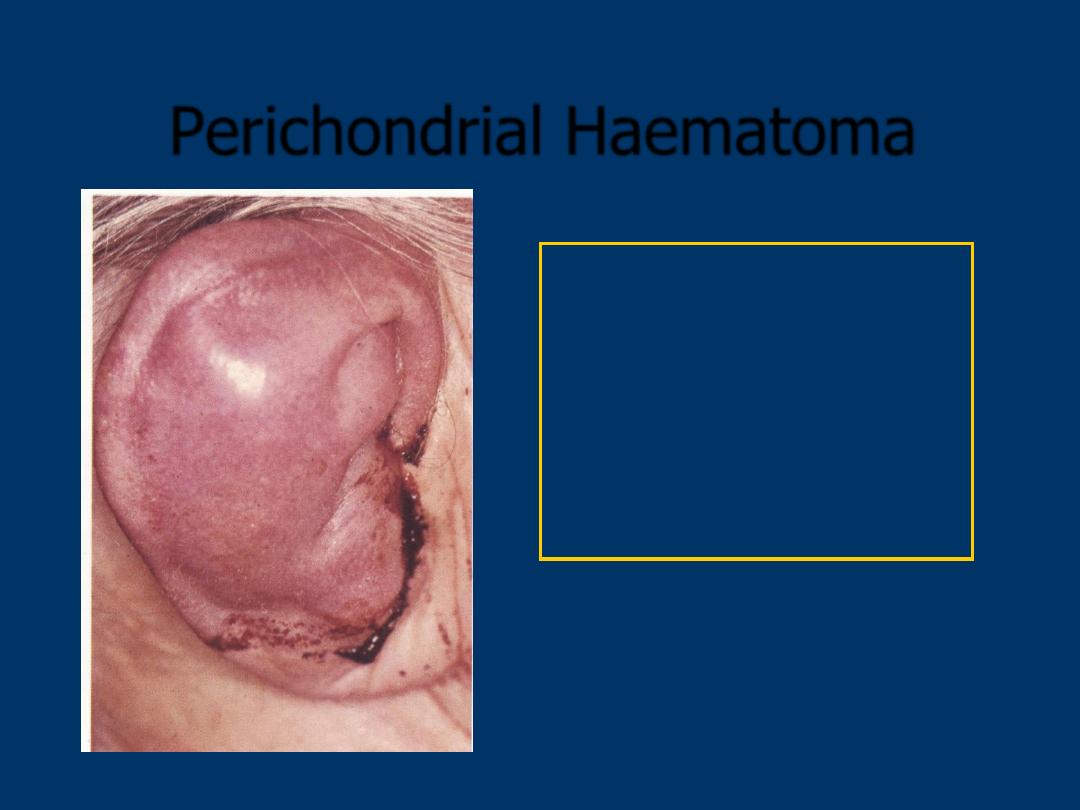
Perichondrial Haematoma
Rx
: Systemic antibiotics
Analgesia
URGENT REFERRAL
for
incision & drainage
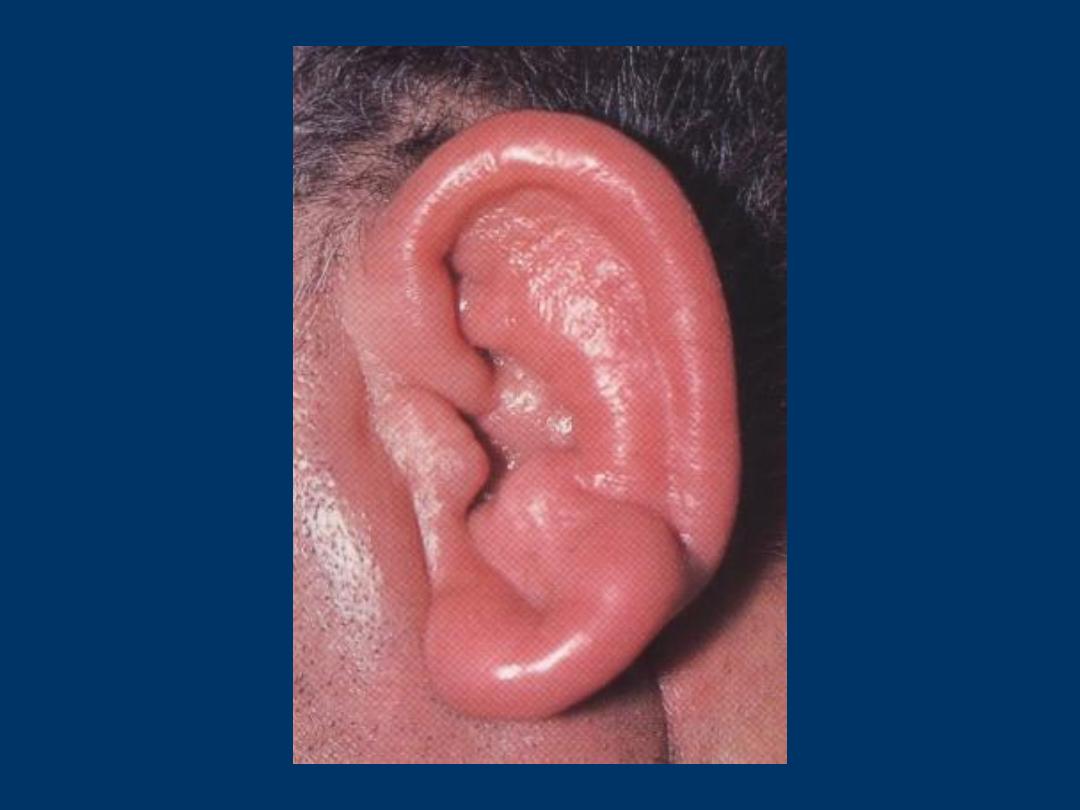
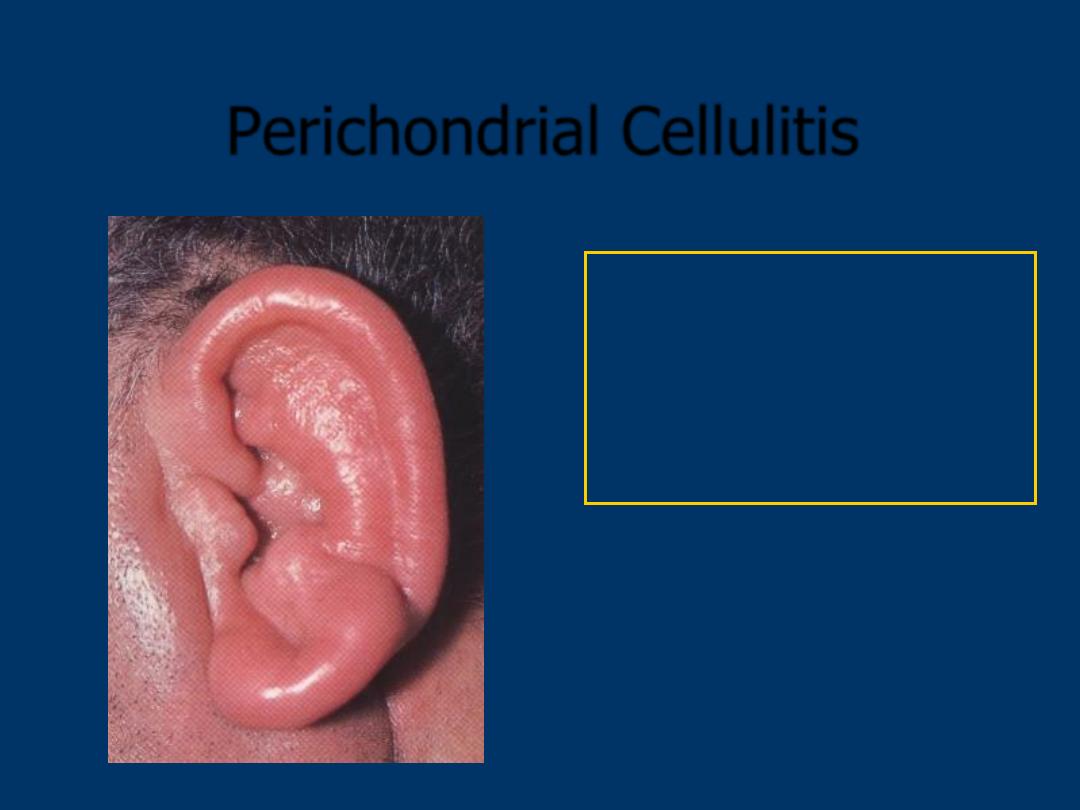
Perichondrial Cellulitis
Rx
: Systemic antibiotics
Analgesia
REFERRAL
to ENT if no
response after 24hr
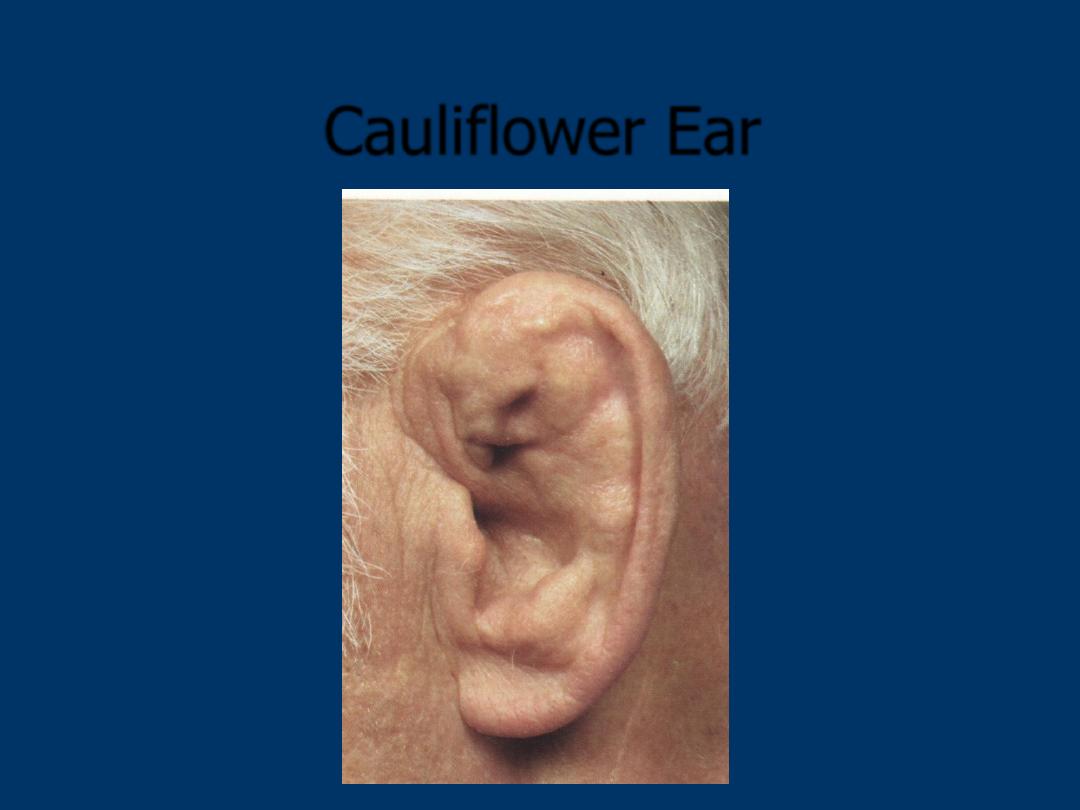
Cauliflower Ear
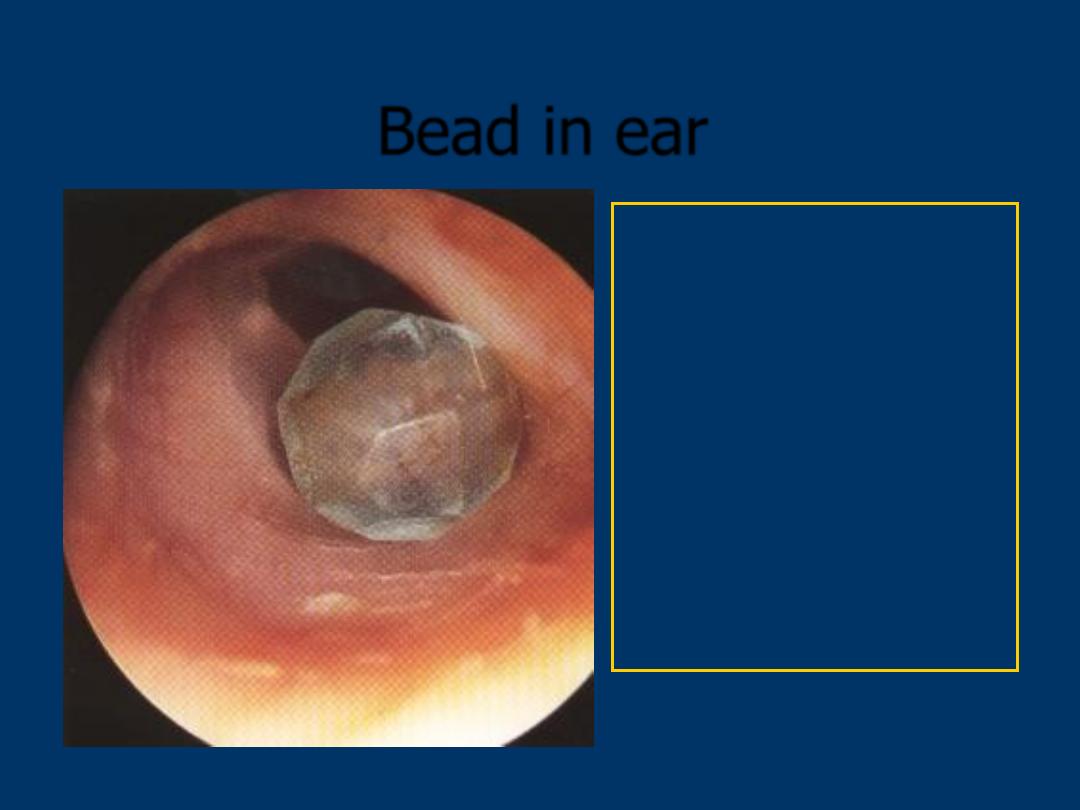
Bead in ear
Rx
: one attempt at
removal only.
Try syringing with warm
water
Do not use forceps for
round objects
Non urgent
ENT referral
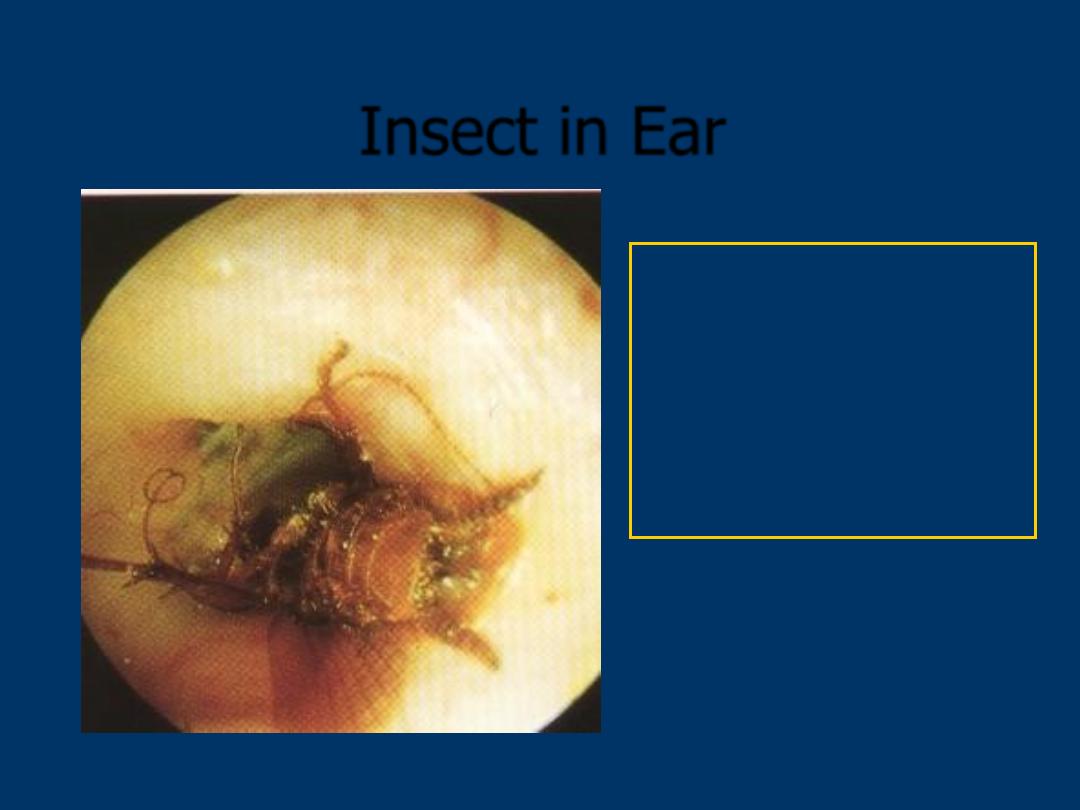
Insect in Ear
Rx
: Kill insect with
olive oil
Then try syringing with
warm water
Urgent
ENT referral
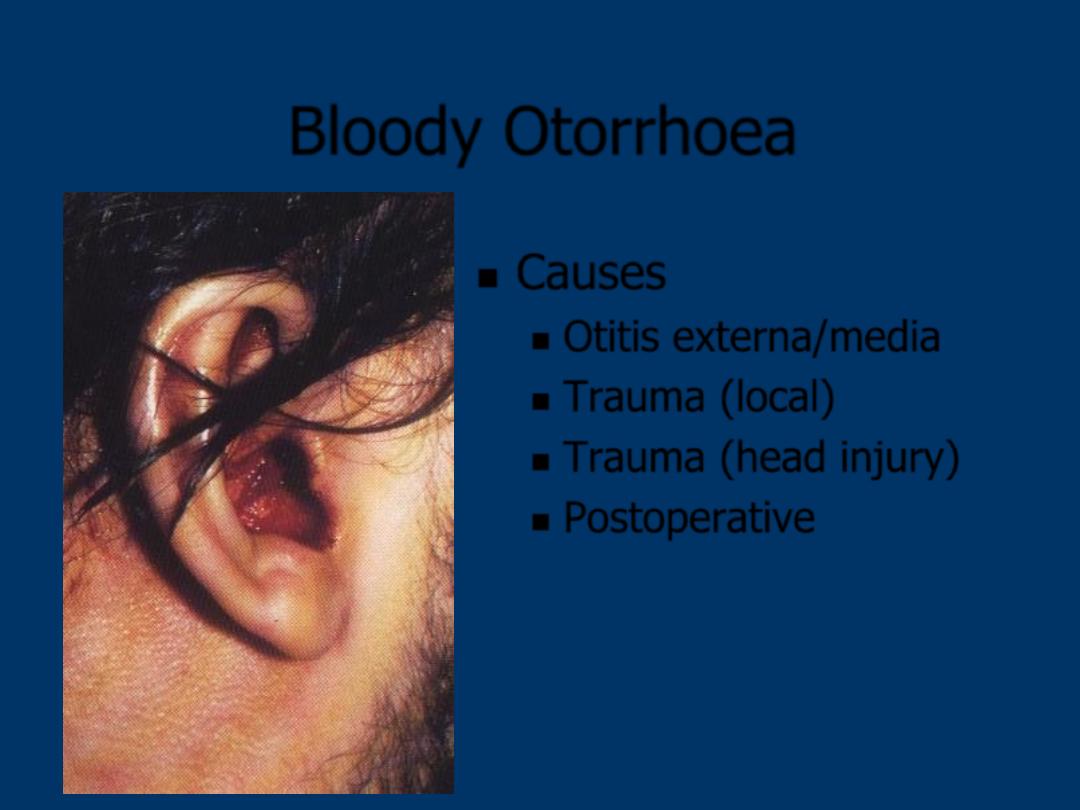
Bloody Otorrhoea
Causes
Otitis externa/media
Trauma (local)
Trauma (head injury)
Postoperative
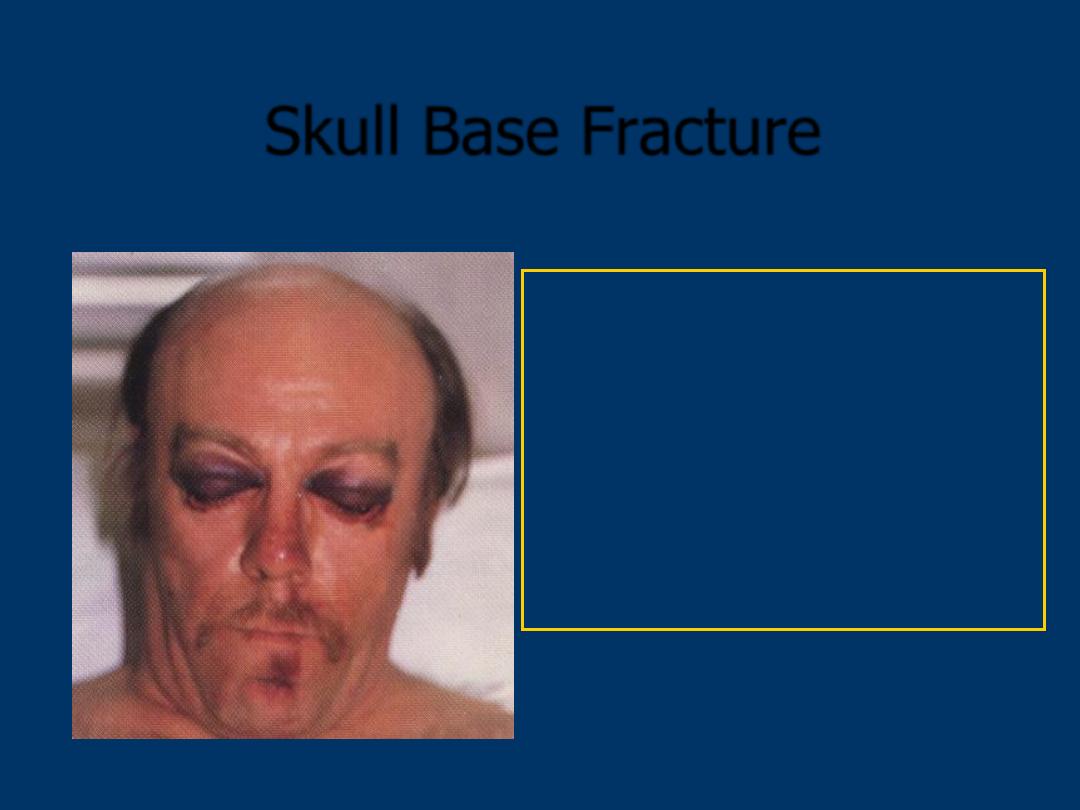
Skull Base Fracture
Rx
: Do not examine ears with
an auriscope.
Admit under the head injury team
Non urgent ENT referral
Unless VII Palsy – ENT
EMERGENCY
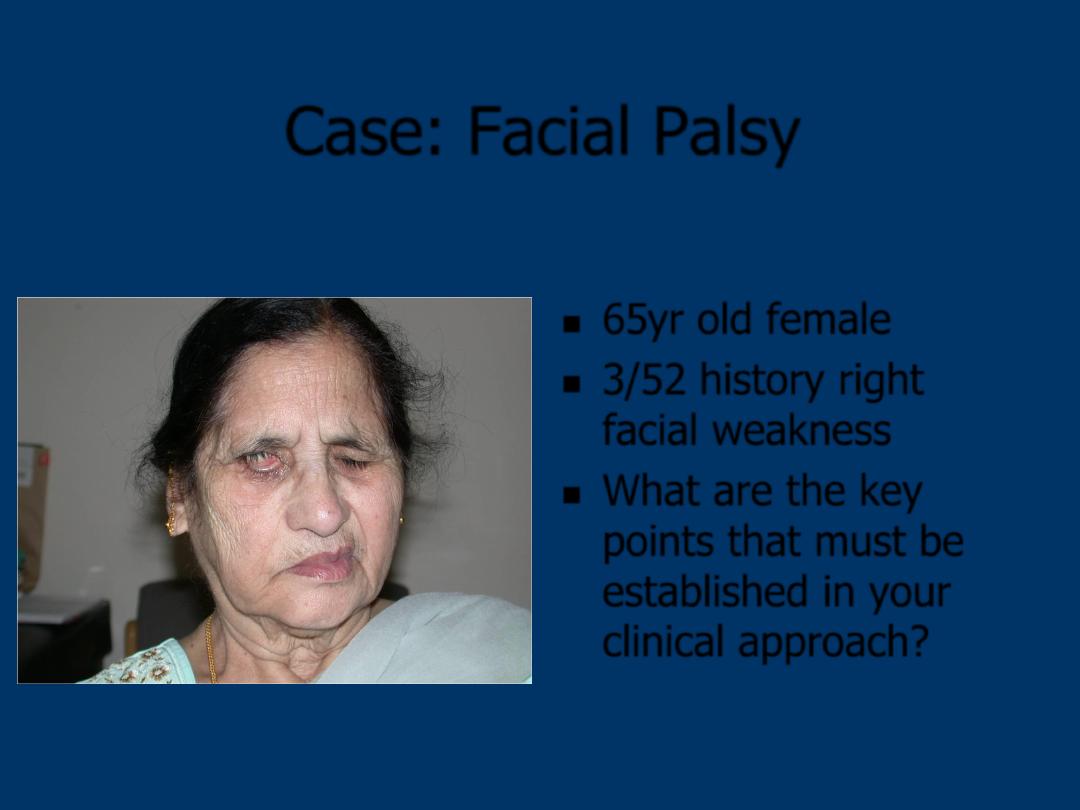
Case: Facial Palsy
65yr old female
3/52 history right
facial weakness
What are the key
points that must be
established in your
clinical approach?
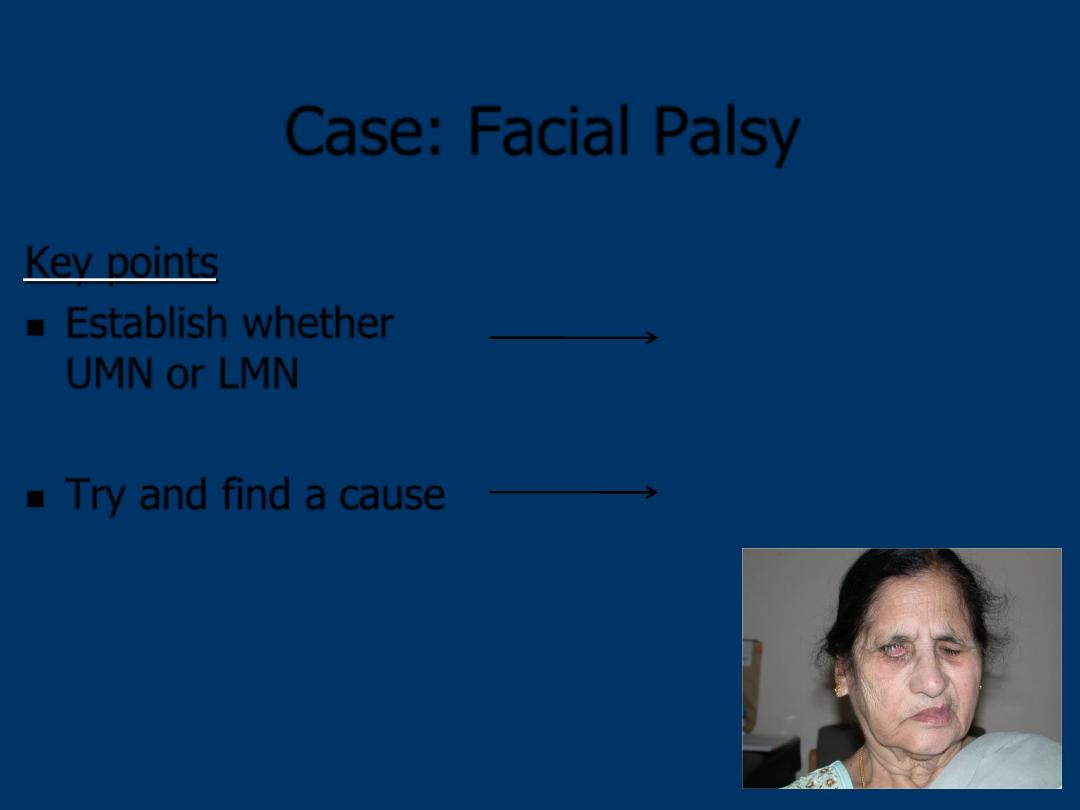
Case: Facial Palsy
Key points
Establish whether
UMN
or
LMN
Try and find a
cause
Forehead sparing = UMN
Thorough examination
Facial nerve palsy - causes
UMN (forehead sparing): CVA, MS, Ca
LMN (complete):
Intracranial
Acoustic neuroma
G-Barre
TB
Neurosarcoid
Glomus tumour
Lyme disease
Intratemporal
Trauma
Acute otitis media
Malignant otitis externa
Ramsey-Hunt syndrome
SCC
Cholesteatoma
Extracranial
Trauma
Malignant parotid tumour
Idiopathic
= Bell
’s Palsy
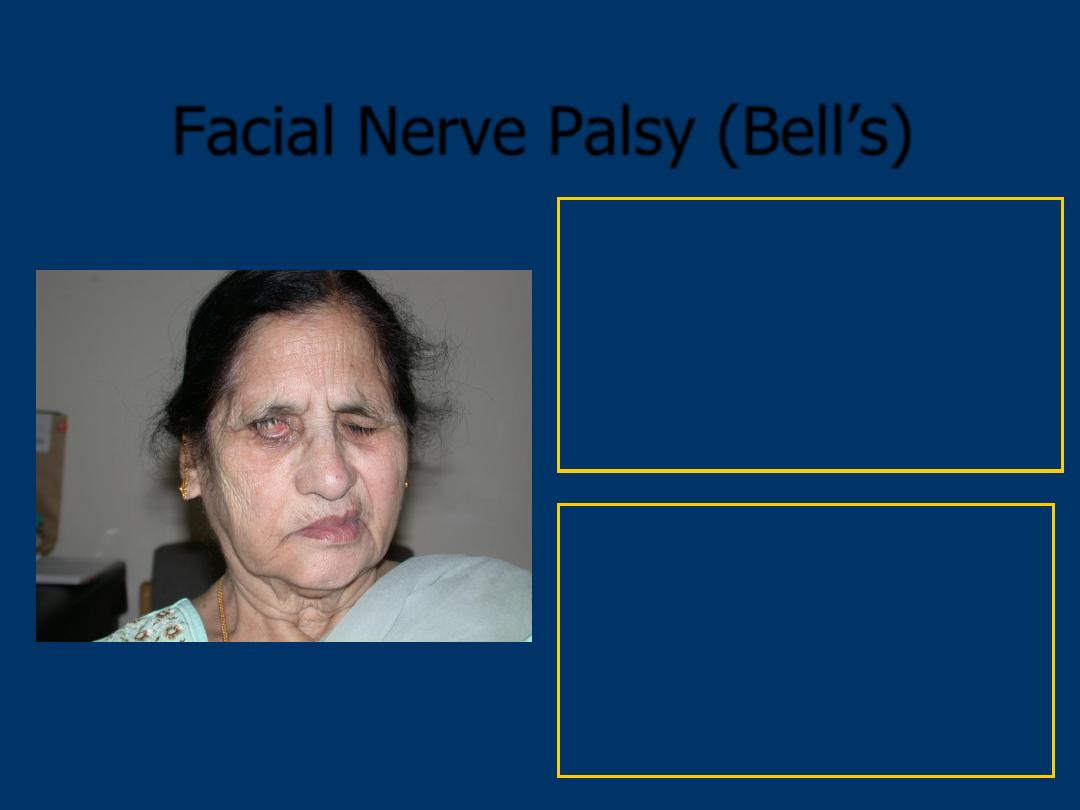
Facial Nerve Palsy (Bell’s)
Rx
: Prednisolone 30mg
Acyclovir 200mg 5x/day
Hypermellose eye drops
Lacrilube ointment
Red bulging ear drum =
URGENT ENT
review
If not, Non urgent ENT review
If poor eye closure =
Ophthalmology review
THE NOSE
Nasal Fracture
Rx
: Exclude other max-fax
fractures
Exclude CSF rhinorrhoea
Analgesia
Refer if
: Obvious deformity
(5-7 days)
Septal Haematoma
(URGENT)
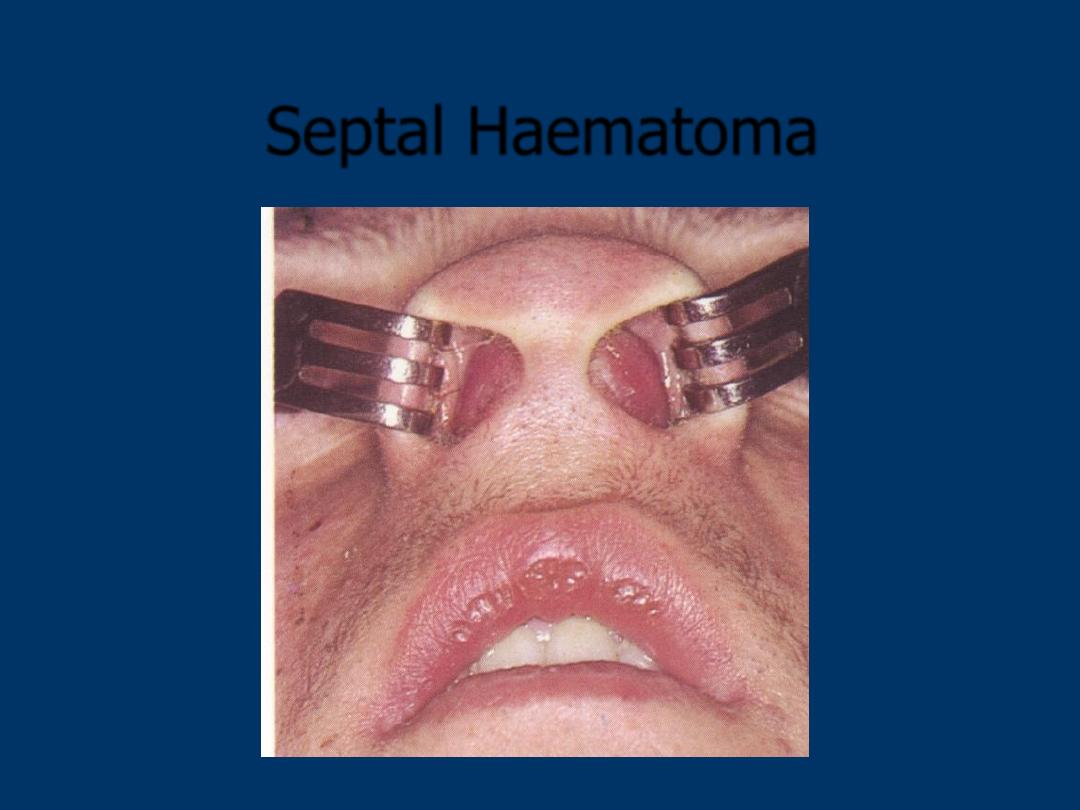
Septal Haematoma
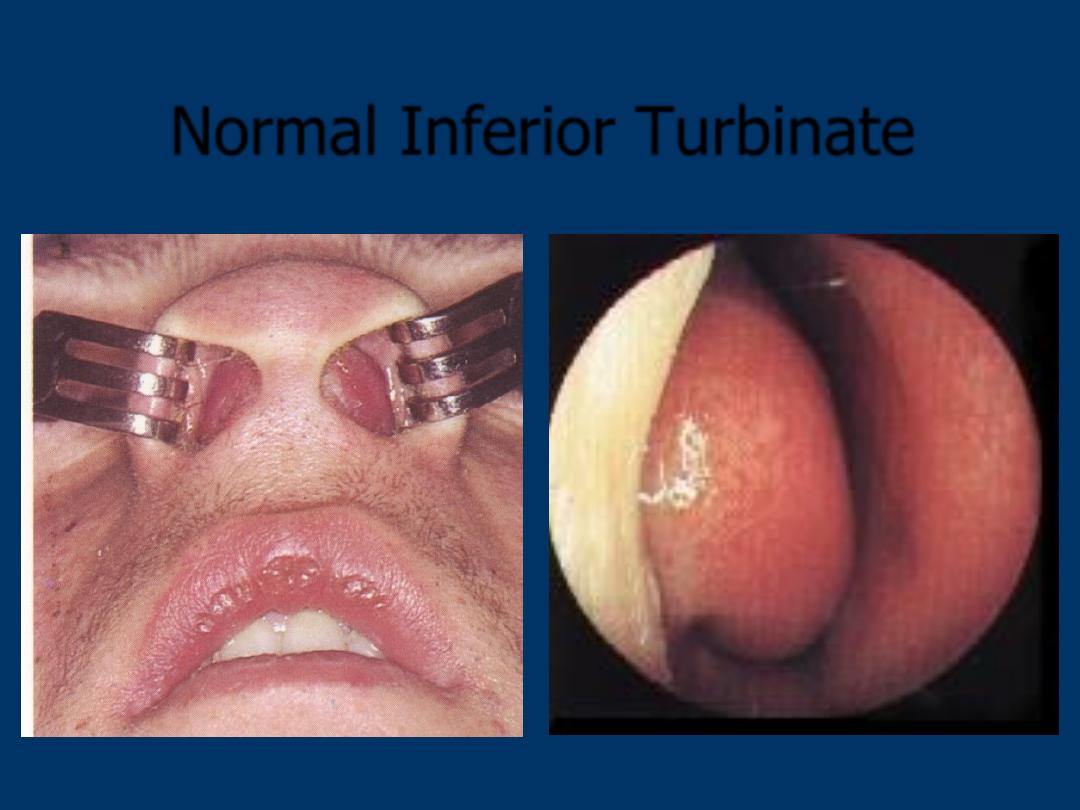
Normal Inferior Turbinate
Septum
IT
Epistaxis
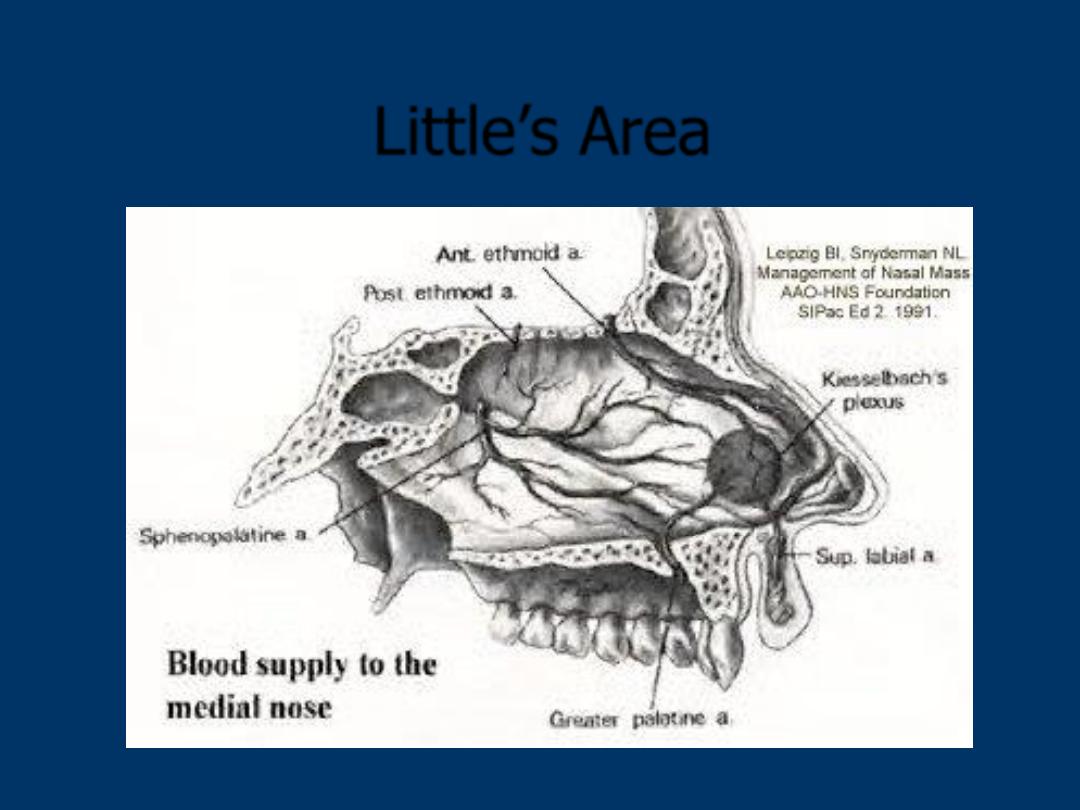
Little’s Area
Epistaxis
Children: Recurrent self limiting bleeds
Risk factors – URTIs, digital trauma
Adults:
Traumatic
Anterior bleed
Little’s area
Recurrent, self-limiting
Posterior bleed
Elderly
Medical comorbidities (hypertension, aspirin, warfarin)
More severe
Admission
Epistaxis
Rx
: RESUSCITATE
FBC, Clotting profile
Local pressure
(Cautery)
Nasal Packing
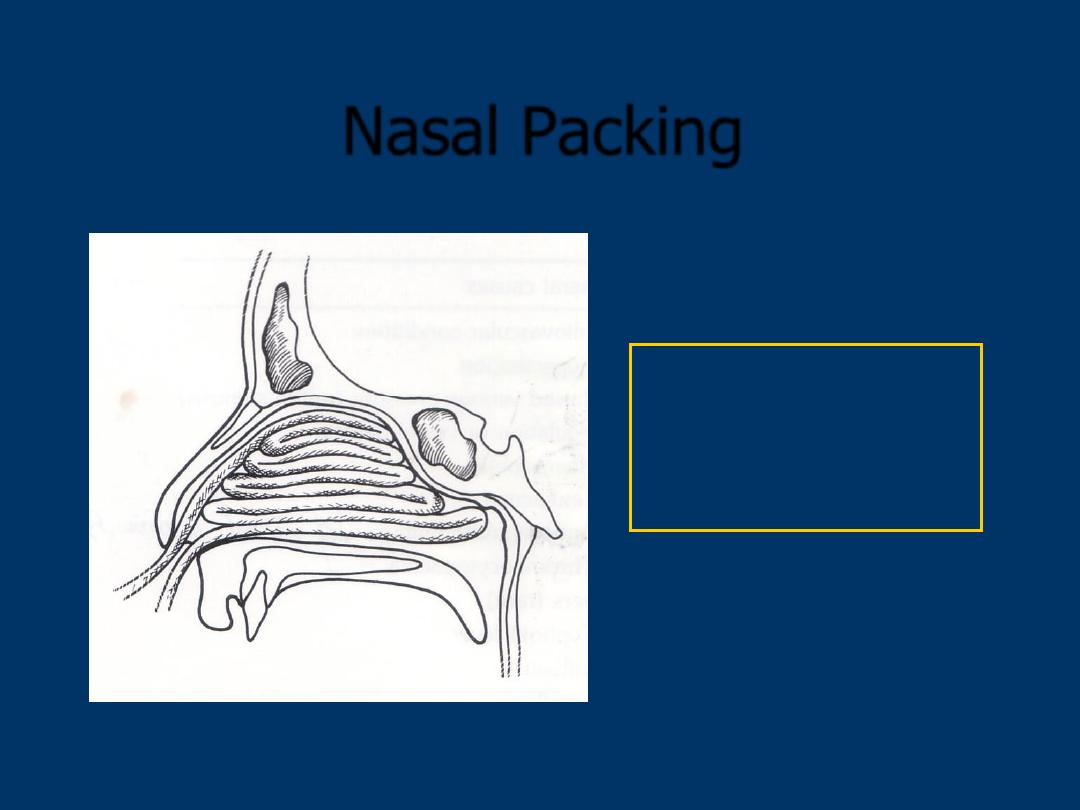
Nasal Packing
BIPP
Merocel
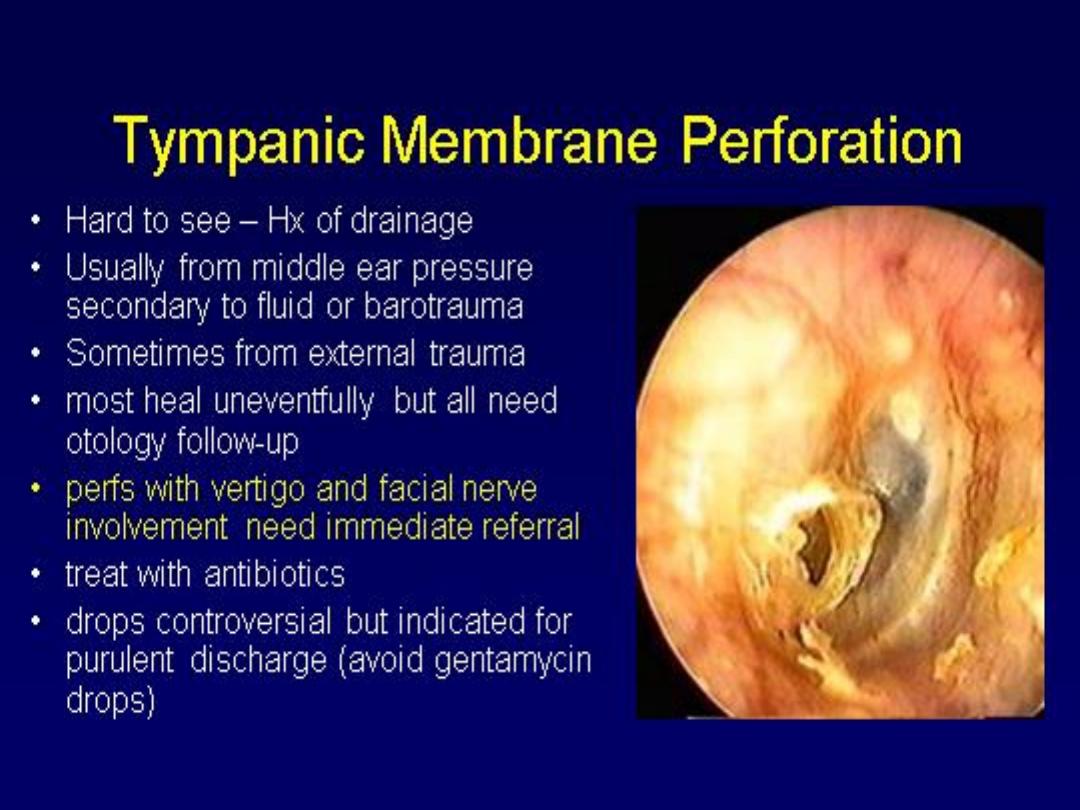
TM
Rapid Rhino
TM
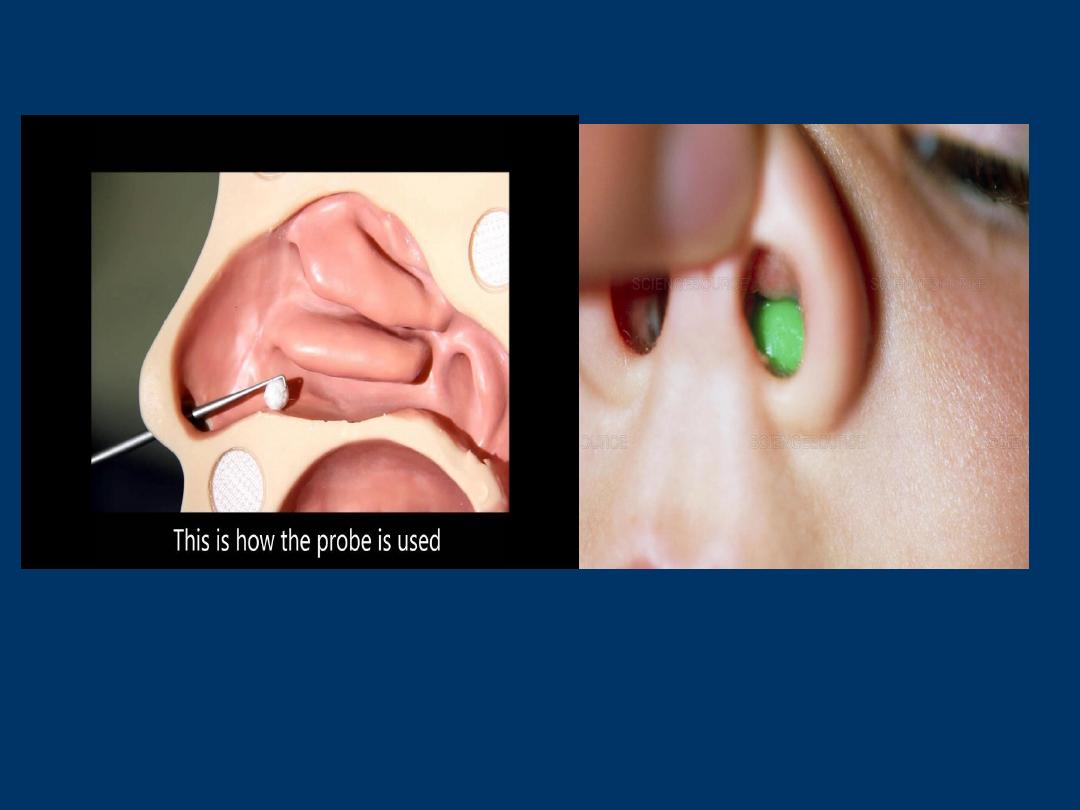
Foreign Body in Nose
Rx
: one attempt at removal
only.
Do not use forceps for round
objects
Urgent ENT referral

Orbital cellulitis – Chandler’s
classification
Grade 1
Periorbital cellulitis (preseptal)
Grade 2
Orbital cellulitis (postseptal)
Grade 3
Subperiosteal abscess
Grade 4
Intraorbital abscess
Grade 5
Cavernous sinus thrombosis
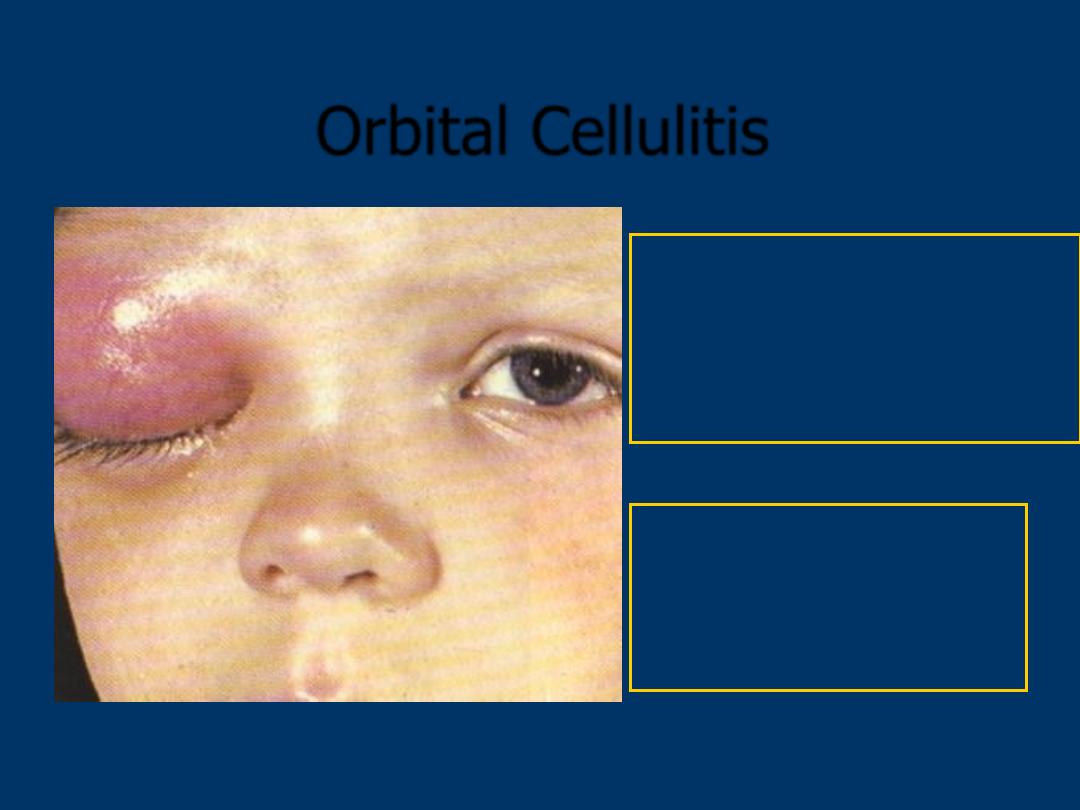
Orbital Cellulitis
Rx
: Systemic antibiotics
Decongestants
Analgesia
URGENT ENT referral
URGENT EYE referral
URGENT CT sinuses
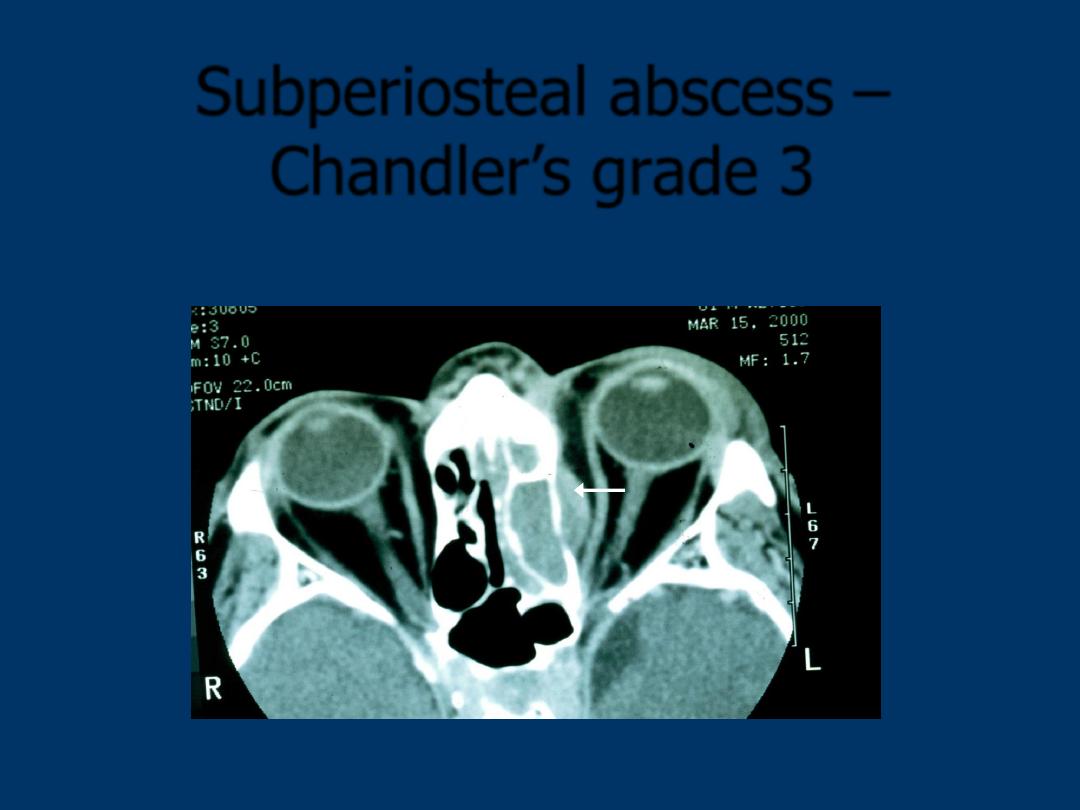
Subperiosteal abscess –
Chandler’s grade 3
Cavernous sinus thrombosis
Absence of valves in the orbital veins allows the
blood to flow to the cavernous sinus
Rapidly progressive chemosis, ophthalmoplegia
Severe retinal engorgement
High fever
Prostation
May progress to vision loss, meningitis, death
THE THROAT
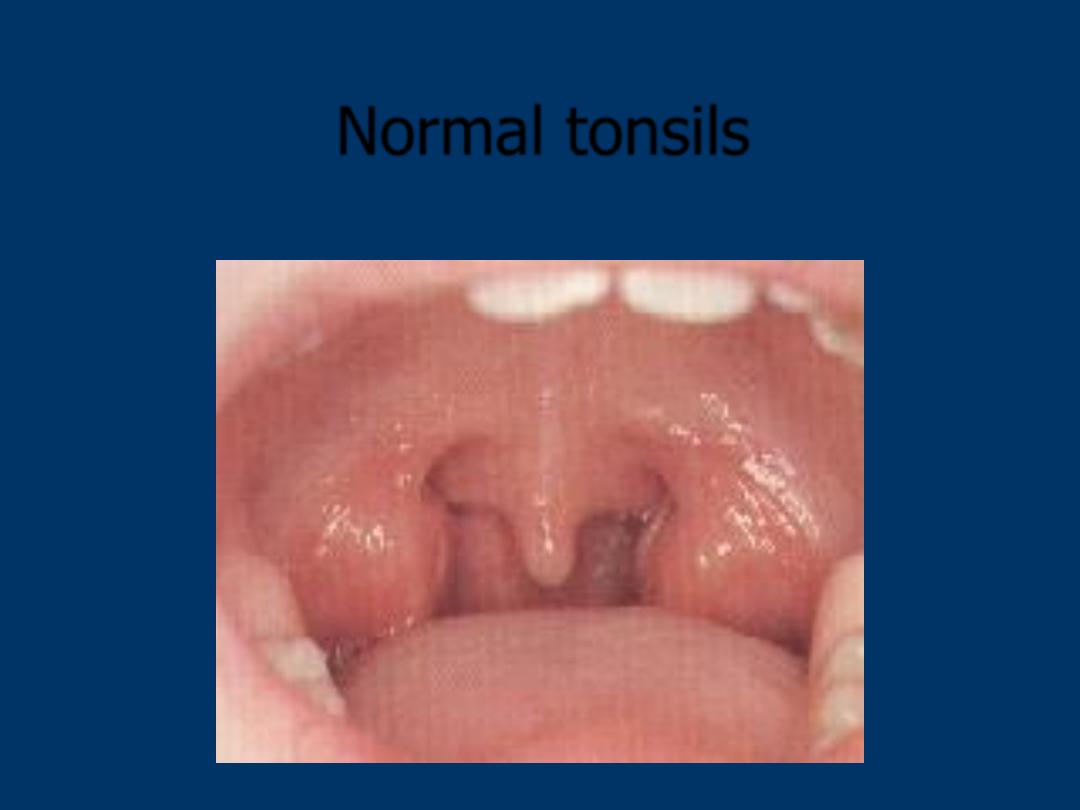
Normal tonsils
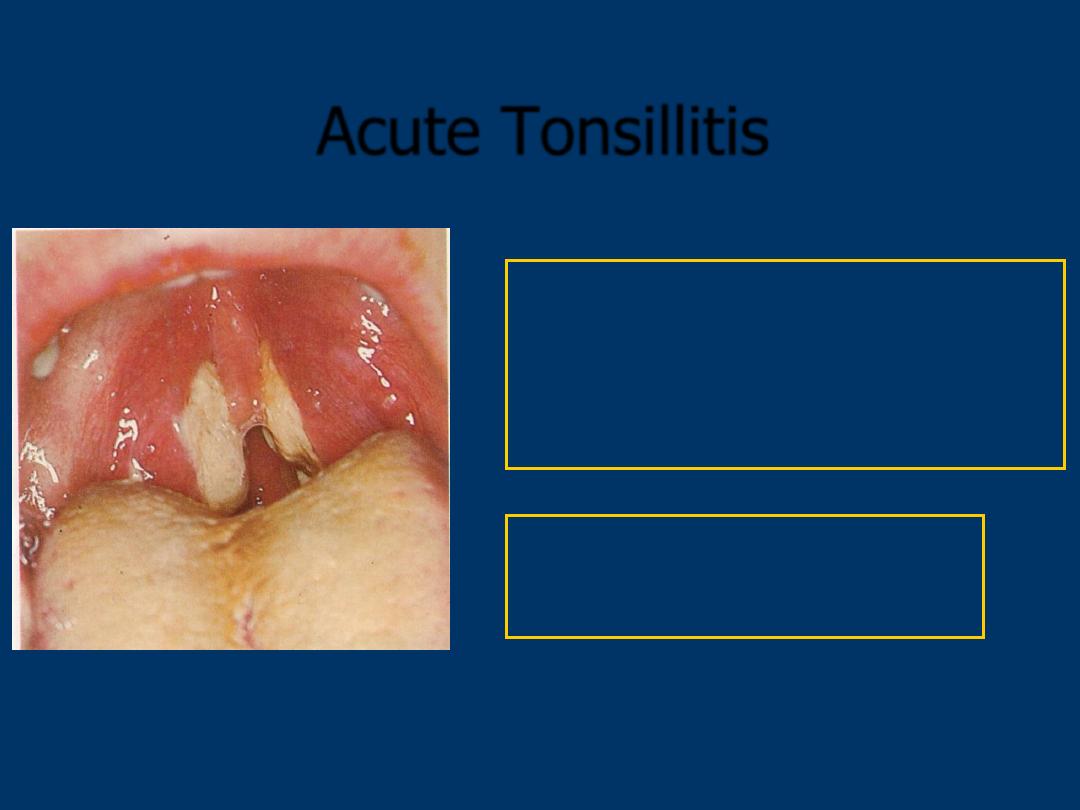
Acute Tonsillitis
Rx
: Penicillin V/ Metronidazole
Analgesia
FBC, Paul Bunnel, LFT
Refer if
: Complete dysphagia
Quinsy
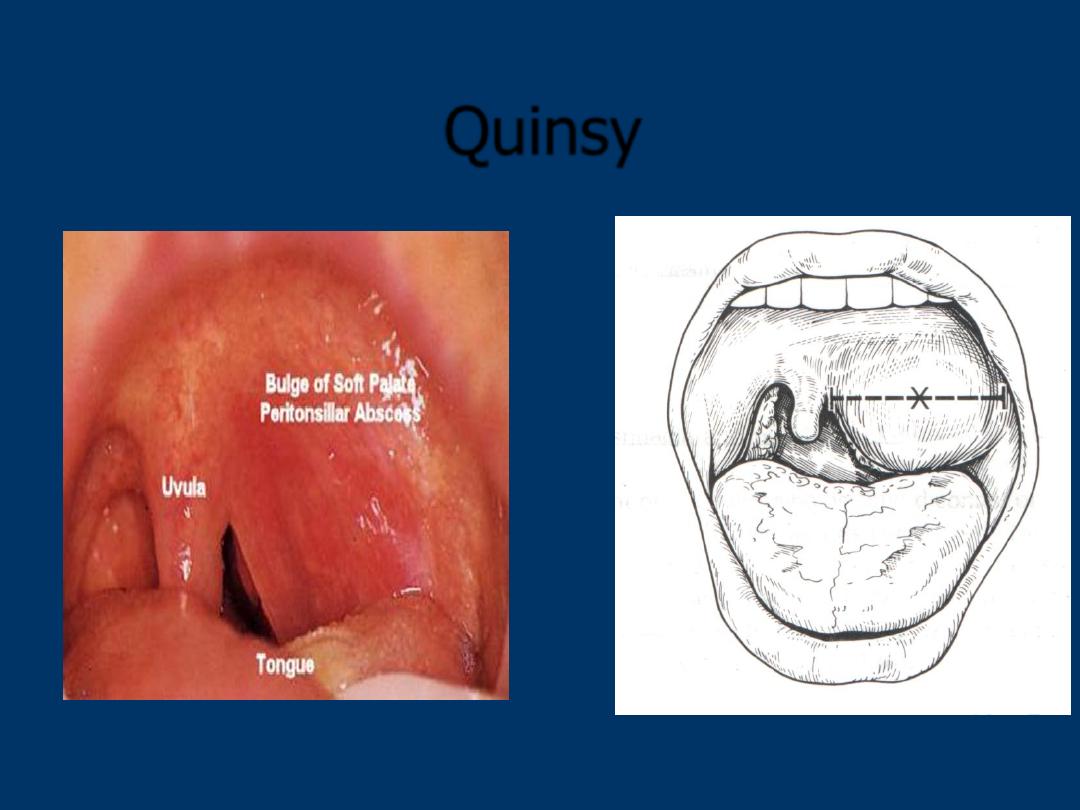
Quinsy

Peritonsillar Abcess
• Inferior - medial displacement of tonsil
and uvula
• dysphagia, ear pain, muffled voice,
fever, trismus
• Group A strep, Strep pyogenes,
Staph aureus, H. influenzae,
Anaerobes
• Treatment
- Antibiotics (clinda), I&D, +/-steroids
Retropharyngeal Abcess
• Anterior to prevertebral space
and posterior to pharynx
• Usually in children under 4
(lymphoid tissue in space)
• pain, dysphagia, dyspnea, fever
• swelling of retropharyngeal
space on lateral x-ray
• Complications – mediastinitis
• Drainage & AB.

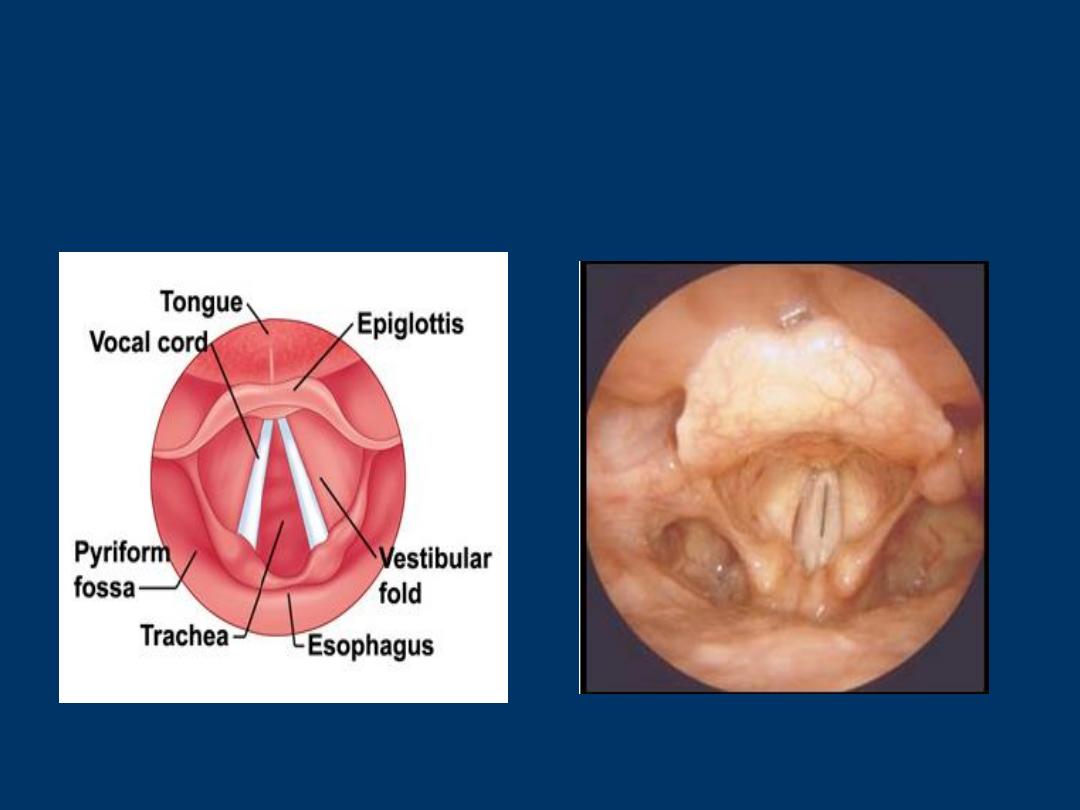
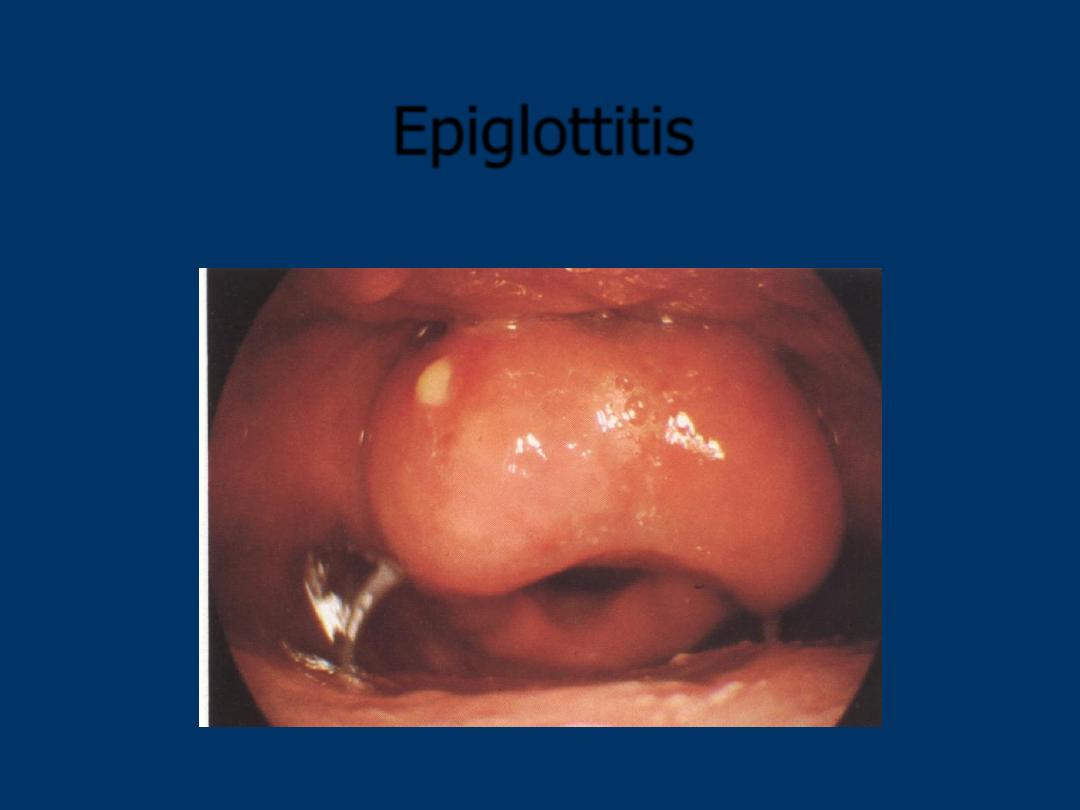
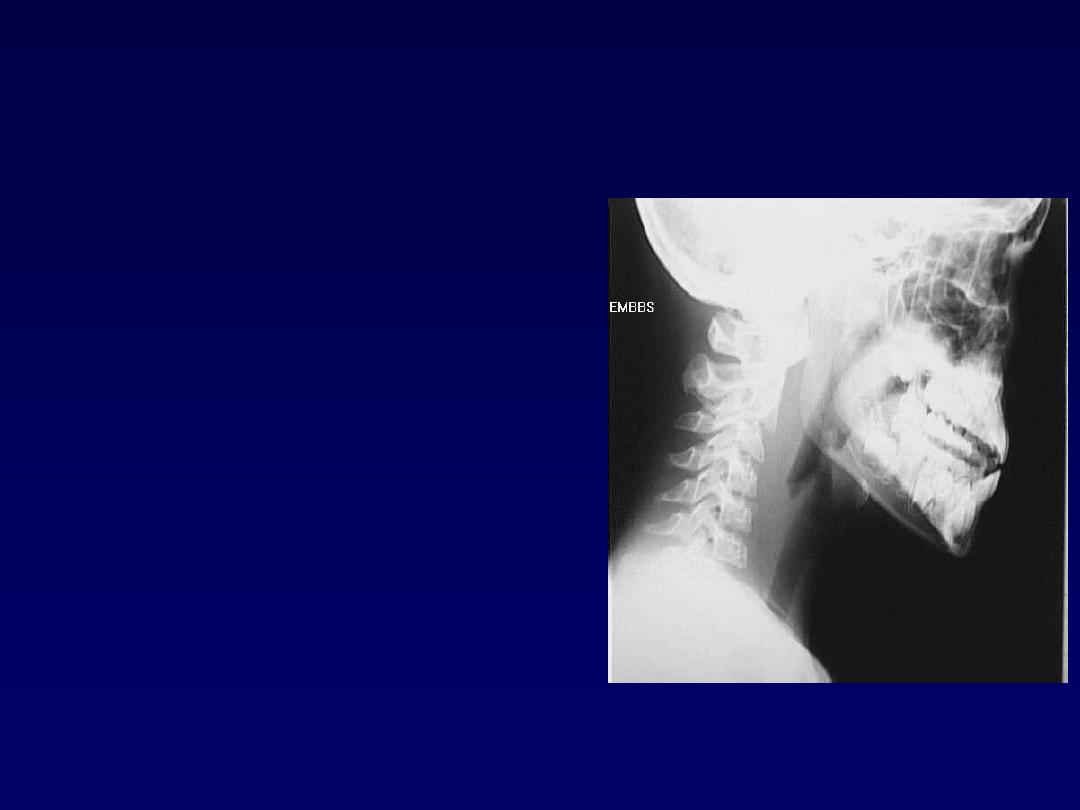
Epiglottitis
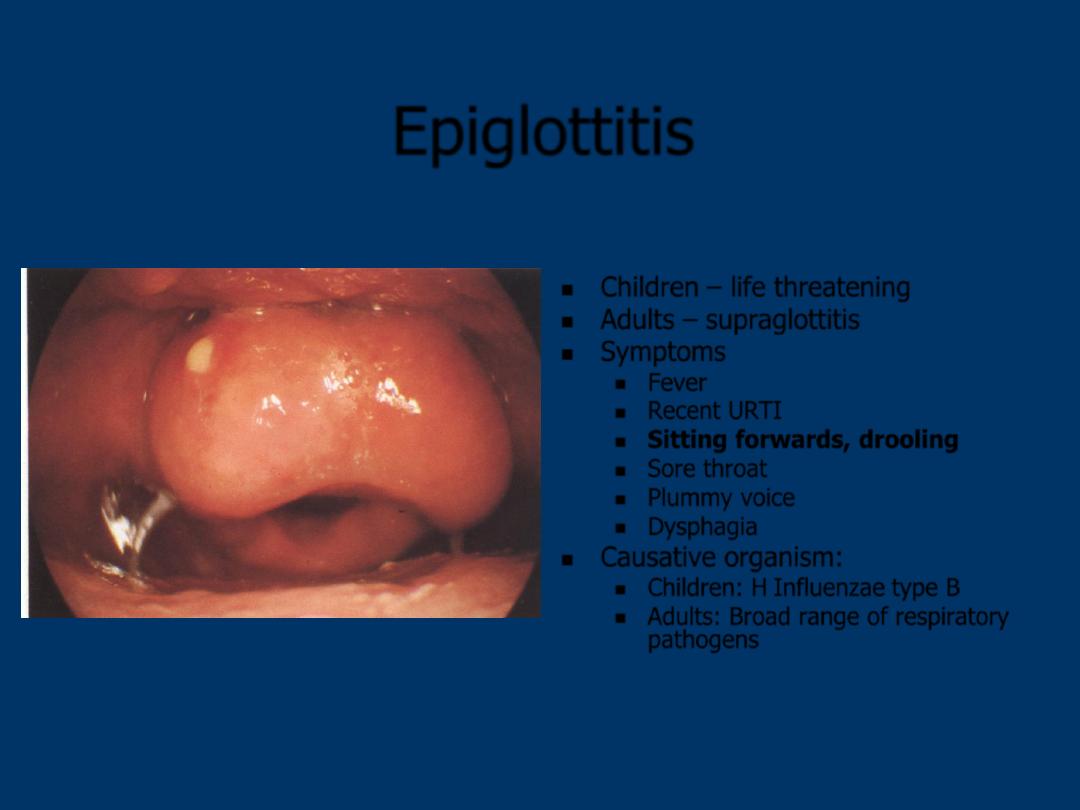
Epiglottitis
Children – life threatening
Adults – supraglottitis
Symptoms
Fever
Recent URTI
Sitting forwards, drooling
Sore throat
Plummy voice
Dysphagia
Causative organism:
Children: H Influenzae type B
Adults: Broad range of respiratory
pathogens
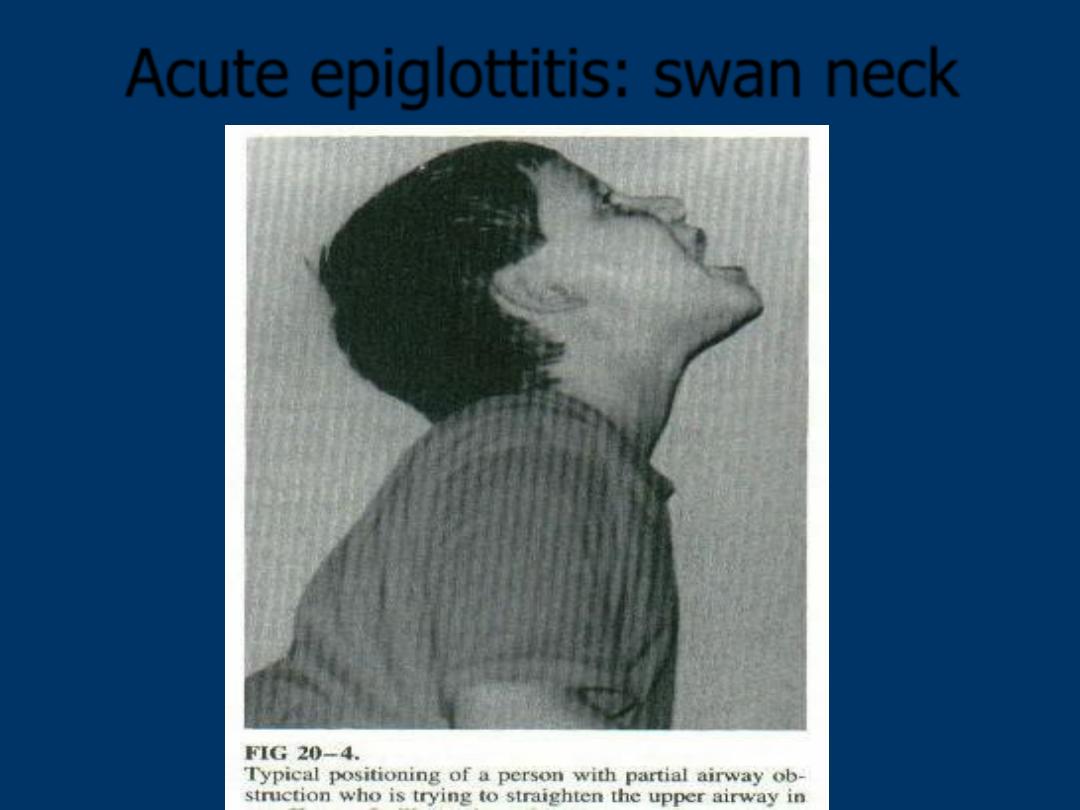
Acute epiglottitis: swan neck
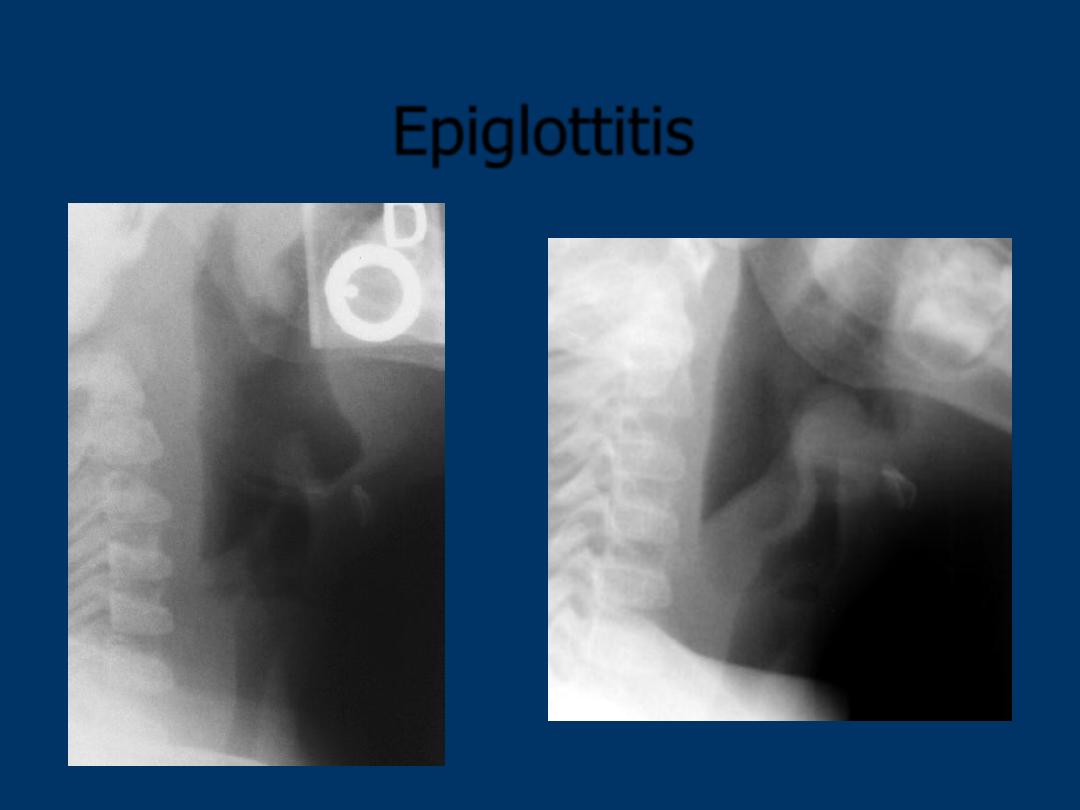
Epiglottitis
Epiglottitis v Croup
Epiglottitis
Croup
Cause
Bacterial
Viral
Age
Any
1-5yrs
Obstruction
Supraglottic
Subglottic
Fever
High
Low grade
Dysphagia
Marked
None
Drooling
Present
Minimal
Posture
Sitting
Recumbent
Toxaemia
Mild to severe
Mild
Cough
None
Barking, brassy
Voice
Muffled
Hoarse
RR
Rapid
Rapid
Laryngeal palpation
Tender
Not tender
Clinical course
Rapid resolution
Longer resolution
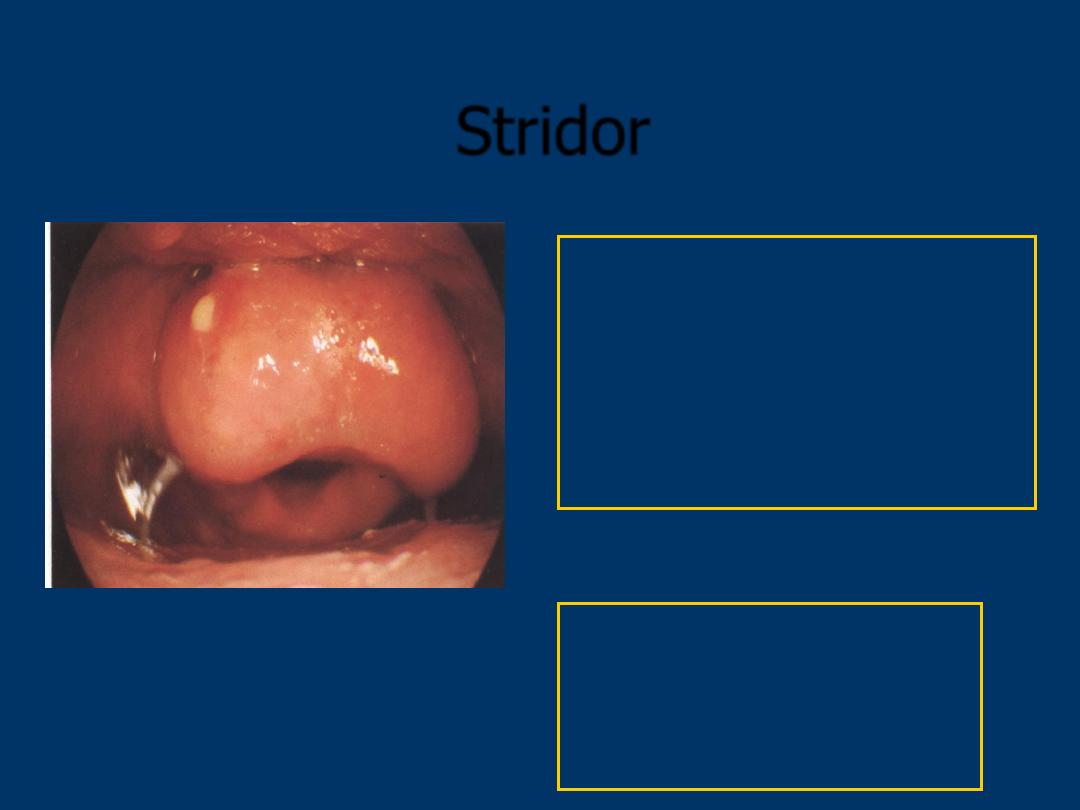
Stridor
Rx
: Oxygen
Adrenaline Nebulisers
Steroids
Antibiotics
URGENT
ENT Ref.
URGENT
Anaesthetic Ref.
URGENT
Paed. Ref.
Ludwig’s Angina
Rapid bilaterally spreading
cellulitis/inflammation with possible
abscess formation of superior
compartment of the suprahyoid space:
Submandibular, sublingual, submental
spaces
usually in elderly debilitated patients and
precipitated by dental procedures
massive swelling with impending airway
obstruction
Ludwig’s Angina
Etiology:
typically from an odontogenic infection
mandibular 2
nd
or 3
rd
molar
streptococcus, oral anaerobes
Clinical presentation
Very tender swelling under mandible
+ floor mouth
Usually little or no fluctuance
Severe trismus, drooling of saliva
Gross swelling, elevation,
displacement of tongue
Tachypnea and dyspnea may happen
Danger of upper airway obstruction
+ death
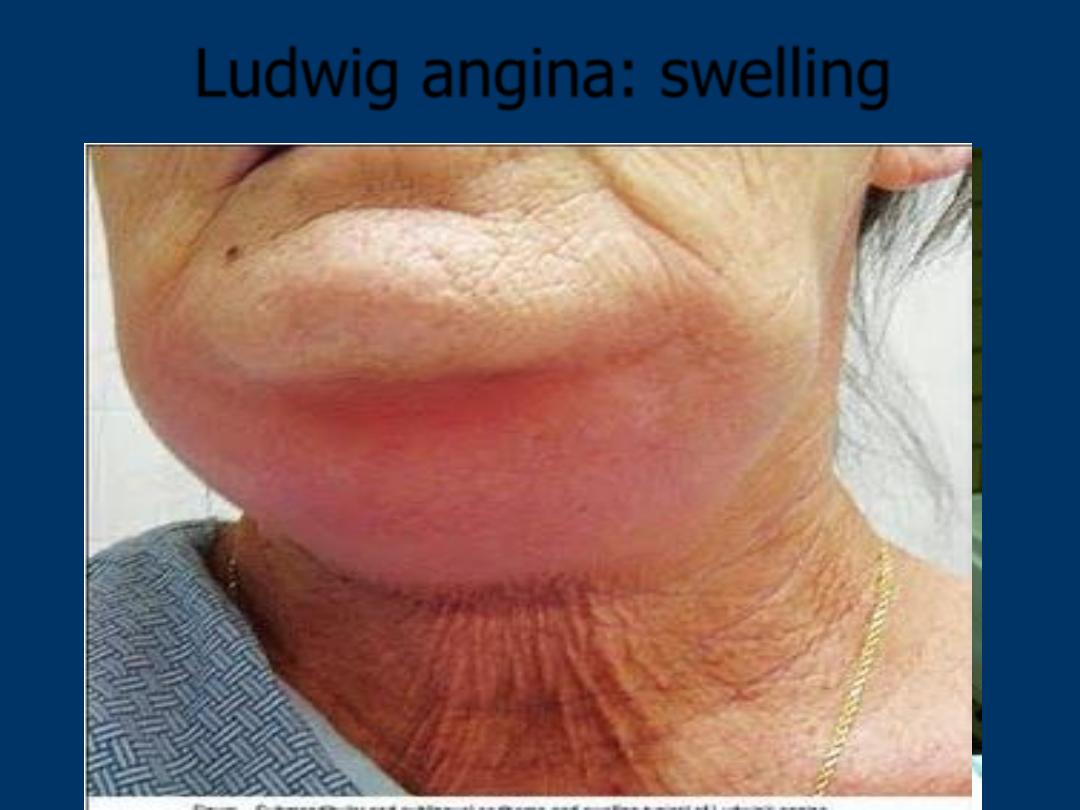
Ludwig angina: swelling
Management
Awake intubation vs tracheostomy if
needed
Admit ICU unless the airway is totally
safe (02 sat monitoring)
Drain the abscess
I.V. ATB: penicillin, clindamycin,
metronidazole
Emergency Trachy??
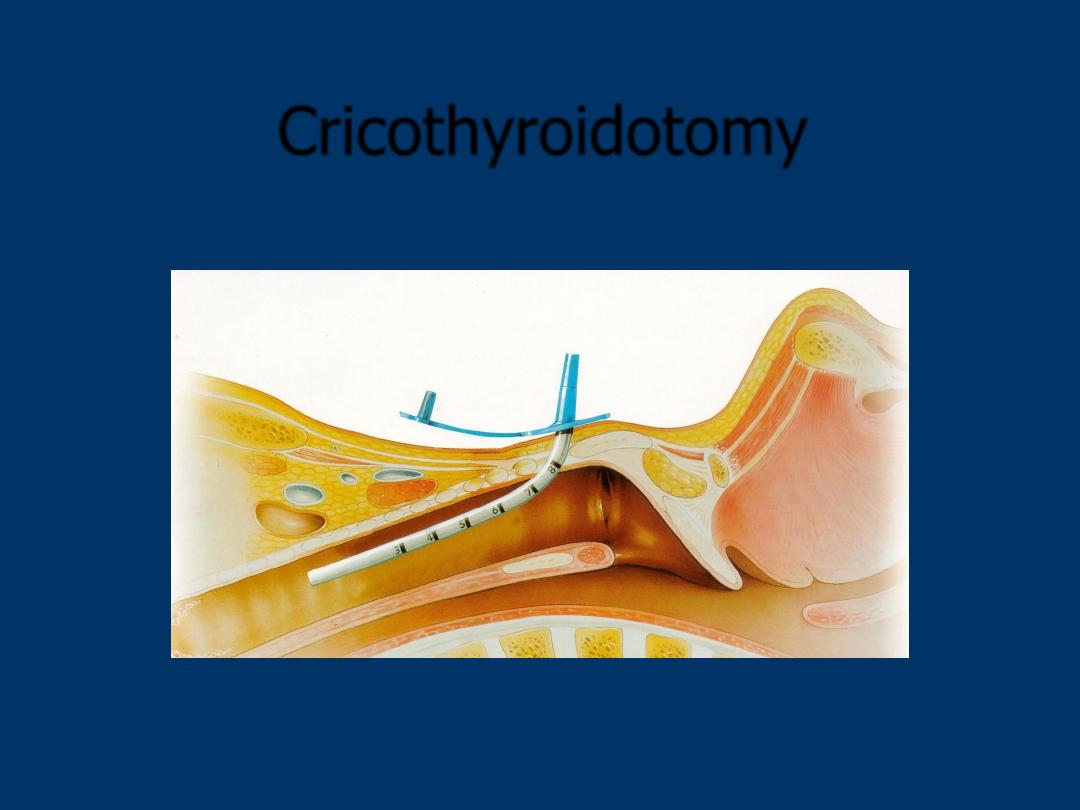
Cricothyroidotomy