
Dr.Nazzal Jabr
Anesthesia
4
Lec.
Airway control
Securing control of the airway is one of the most important skills required of the anaesthetist.
Whether for elective or emergency surgery, and whether the need for airway control has been
predicted or not, the safety of the patient depends on the anaesthetist’s ability to intervene to
ensure adequate oxygenation and ventilation should the need arise.
Equipment and techniques for routine airway management
Before embarking on general anaesthesia, the equipment required should be to hand and its correct
function checked. A preoperative checklist such as that proposed by the Association of Anaesthetists
of Great Britain and Ireland is particularly.The minimum equipment required includes:
• Source of pressurized oxygen (plus bag-valve-mask or anaesthesia circuit)
• Selection of face masks
• Selection of oropharyngeal and nasopharyngeal airways
• High-flow suction and suction catheters
• Two laryngoscopes
• Selection of tracheal tubes
• Selection of laryngeal mask airways
• Magill’s forceps
• Sterile lubricating gel
• Ties and padding to secure tracheal tube
• Gum-elastic or other suitable bougie
Non-relaxant anaesthesia
If relaxant anaesthesia is not required (e.g. for body-surface surgery in the patient not at risk for
aspiration) then inhalational anaesthesia via a face mask is appropriate.
Supporting the airway
Whatever the means of induction, once the patient is unconscious, it is necessary to support the
airway. There is a tendency for the airway to become partially obstructed at this stage because the
tongue falls back against the posterior wall of the pharynx. Induction will normally have occurred
with the patient supine, head resting on a pillow. This allows the anaesthetist to extend the head on
the neck at the same time as applying a jaw thrust and opening the mouth. If it is impossible to open
the airway using these techniques, an artificial airway is required. Two methods are available: the
oropharyngeal and the nasopharyngeal airway.

Dr.Nazzal Jabr
Anesthesia
4
Lec.
The oropharyngeal (Guedel) airway
It is a curved tube that has a flanged and reinforced oral end. The flange enables correct positioning
at the incisor teeth, and the reinforcement prevents the patient from obstructing or severing the
device by biting down. This airway is available in a range of sizes.
The nasopharyngeal airway
It is a soft curved tube with a flanged nasal end and a bevelled pharyngeal end. It is also available in
a range of sizes.
Face mask
For brief procedures, anaesthesia can be maintained using a face mask, with or without airway
adjuncts. For longer procedures, when it is desirable for the anaesthetist to have both hands free,
the standard mask can be supported by a harness.
The laryngeal mask airway (LMA)
It was designed to provide a connection between the artificial and anatomical airways in a less
invasive way than with a tracheal tube, and yet with greater convenience and reliability than a
conventional face mask. The standard LMA is made from silicone and is designed for multiple
patient (up to 40) uses. It consists of a silicone bowl surrounded by a thin-walled elliptical ring that
can be deflated to form a thin wedge shape, and which when inflated in the space posterior to the
pharynx creates a seal around the laryngeal aperture. This seal permits ventilation of the airway
under positive pressure. The LMA is available in a variety of sizes.
Relaxant anaesthesia
Anaesthesia requiring a muscle-relaxant technique most commonly requires tracheal intubation.
Indications for relaxant techniques and/or intubation are:
• Provision of clear airway
• Airway protection from blood, oral or gastric secretions
• Facilitation of suctioning of airway
• Prone, sitting or other position, airway inaccessible
• Abdominal, thoracic anaesthesia
• Likelihood of postoperative respiratory support
• Administration of positive end-expiratory pressure.

Dr.Nazzal Jabr
Anesthesia
4
Lec.
Tracheal intubation
The laryngoscope
It is consists of a handle (which houses the batteries) and a detachable blade, which has a screw-in
bulb. Alternatively, the bulb may be in the handle, and a fibre-optic bundle transmits the light to the
blade.
Two basic types of laryngoscope are available:
Curved-blade (Macintosh): are most commonly used for adults and larger children (the tip is
placed in the vallecula, anterior to the epiglottis).
Straight-blade (Magill): are most often used for smaller children, because the epiglottis is
longer and more floppy in this age group (the tip is inserted posterior to the epiglottis and lift
it from behind).
Endotracheal tubes (ETT)
An extensive range of tracheal tubes is available. Tracheal tubes are usually inserted via the mouth,
or if necessary via the nose (e.g.for intraoral surgery). Tube size is measured by the internal
diameter, ranging from 2.5 mm to about 10 mm in 0.5 mm increments. The tube is connected to the
anaesthetic circuit at the proximal end with a tapered connector of suitable size. The distal end is
bevelended and may have, in addition to the end hole, a side opening (Murphy eye) to allow passage
of gas should the bevelled end be occluded by abutting on the tracheal wall.
Types of ETT
Uncuffed (plain) tubes: which are used in children, to avoids the potential for ischaemic
damage on the tracheal lining from high cuff pressure and maximizes tube size available.
Cuffed tubes: which provides a seal enabling positive-pressure ventilation and preventing
aspiration of secretions into the airway.
Preformed ETT: used usually for face and neck operations.
Armored ETT: used for head and neck surgery and operation that need positioning especially
prone position.
Double lumen ETT: for one lung ventilation.
Dr.Nazzal Jabr
Anesthesia
4
Lec.
Breathing Systems
A ‘breathing system’ is the name given to apparatus that delivers and removes gas and
vapour to
or from a patient. The three main functions of the breathing system are:
to supply adequate oxygen
to remove carbon dioxide
to supply adequate inhalational anaesthetic agent.
Essential components of a breathing system
Tubing (hose): which is corrugated to prevent kinking.
Reservoir bag: this stores fresh gas when the patient is exhaling and estimate the respiratory
rates during inspiration.
Adjustable pressure-limiting valve (APL valve): this is a one-way valve.
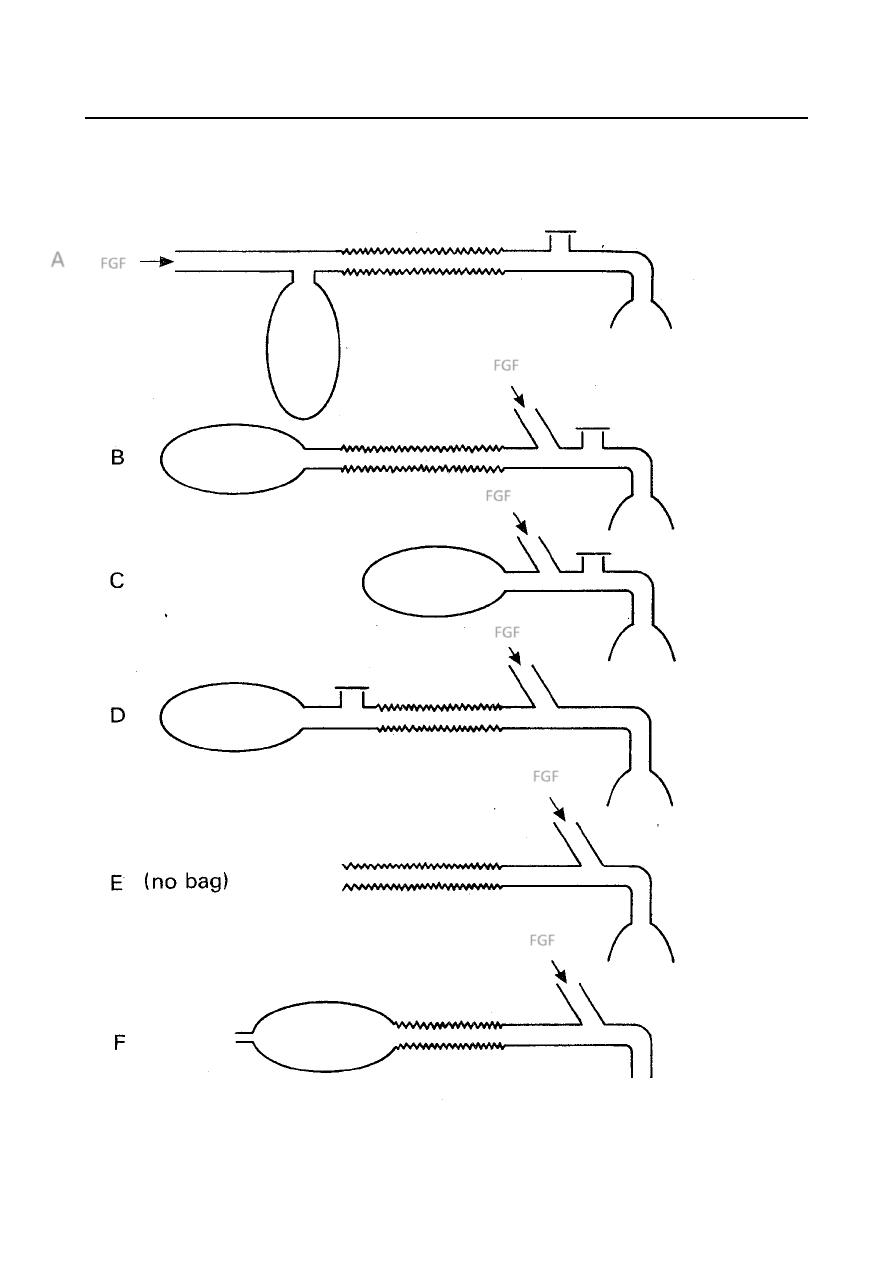
Mapleson circuits classification
In 1954 Mapleson described and analyzed five different anesthetic systems, and they are classically
referred to as Mapleson systems and designated A to E. Thenafter, Willis et al added the F system to
the five original systems.
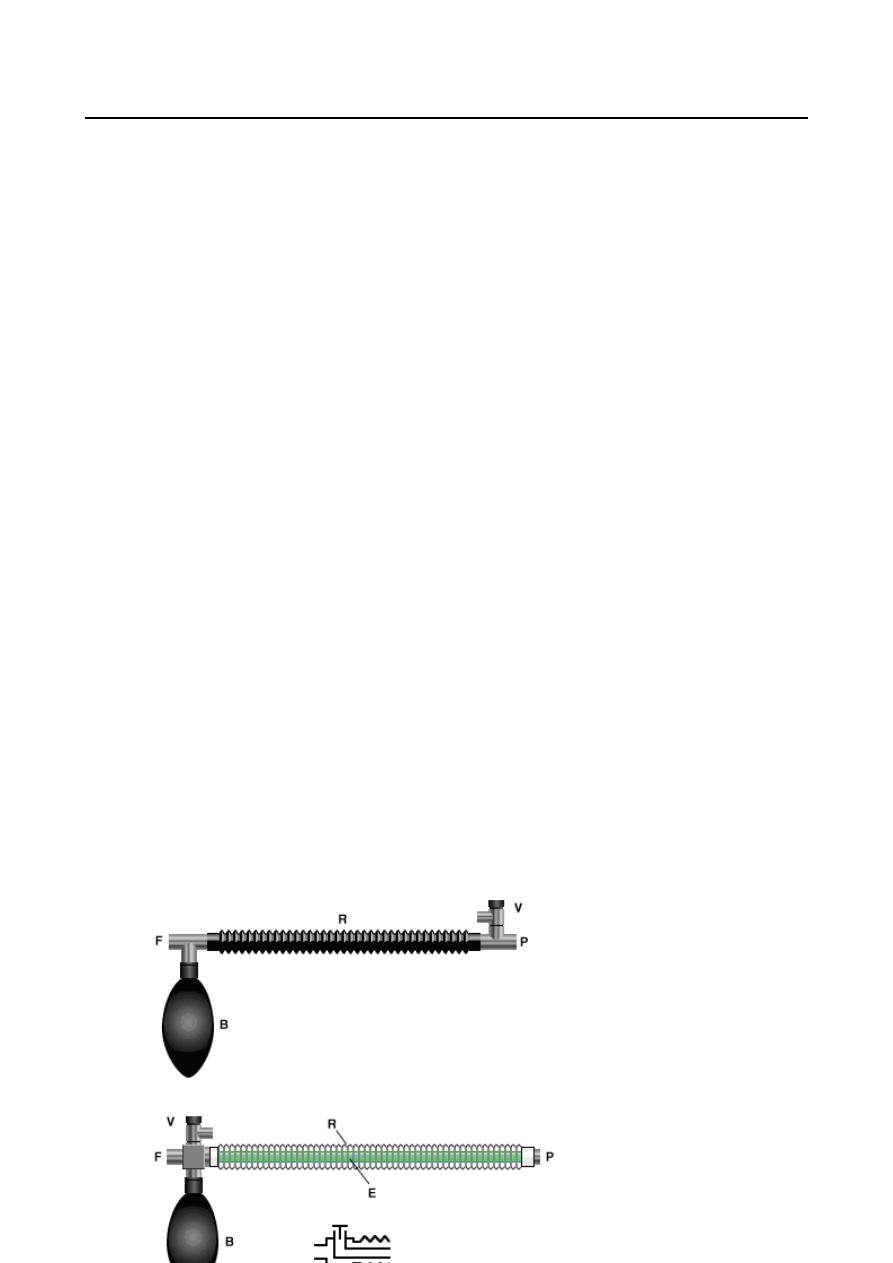
Mapleson A (Magill) System:
Classically describes the Magill system. The APL valve
is close to the patient making this system
heavy at the patient’s end. (Lack) solved this problem by creating a co-axial arrangement where the
expiratory gases were carried up an inner hose to the APL.
Magill
Dr.Nazzal Jabr
Anesthesia
4
Lec.
Mapleson B and C:
In both systems, the FGF, reservoir bag and APL are near the patient, creating a compact and
portable system. However, they are both used mainly for patient transport and in postoperative
recovery units.
Mapleson D:
System is efficient for IPPV.The Bain system is a coaxial version, which is particularly useful for
limited-access surgery because of its light weight.
Mapleson E:
The Ayre’s T-piece is a valveless, lightweight system, with low internal resistance and dead space, it
is used for pediatrics.
Mapleson F:
The Mapleson F or Jackson Rees modification of the Ayres T Piece is a basic system for use with very
small patients. Adding an open-ended reservoir bag to the expiratory limb of the Ayre’s T-piece
allows manual control of ventilation, observation of breathing and assessment of lung compliance.
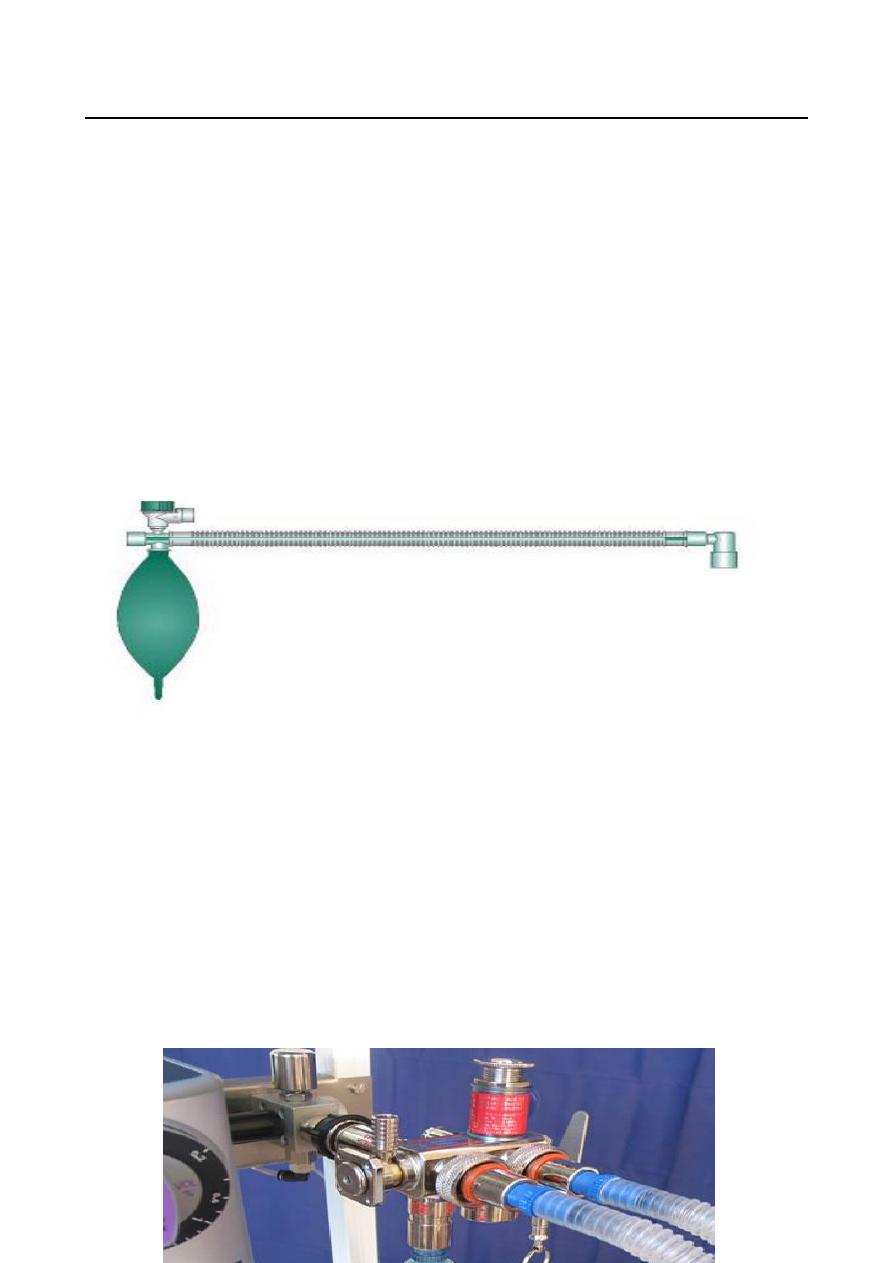
Humphrey ADE system
:
It is a low-flow multipurpose system that appears to combine the best of the Magill (mapleson A),
Bain (mapleson D) and T-piece (mapleson E) systems but not their disadvantages.
Lack
Dr.Nazzal Jabr
Anesthesia
4
Lec.
The Mapleson classification of anaesthetic breathing systems
FGF
FGF
A
FGF
FGF
FGF
FGF