Tumors Of The Kidney
• Benign Tumors :
They rarely cause clinical problems, usually small and are
often an incidental finding at autopsy or nephrectomy. These
include
• cortical adenoma, oncocytoma, angiomyolipoma Renal
Fibroma or Hamartoma.
• Malignant Tumors :
On the contrary to benign tumors, malignant tumors
are clinically of great importance
Pediatric Tumors And Tumor-Like Conditions
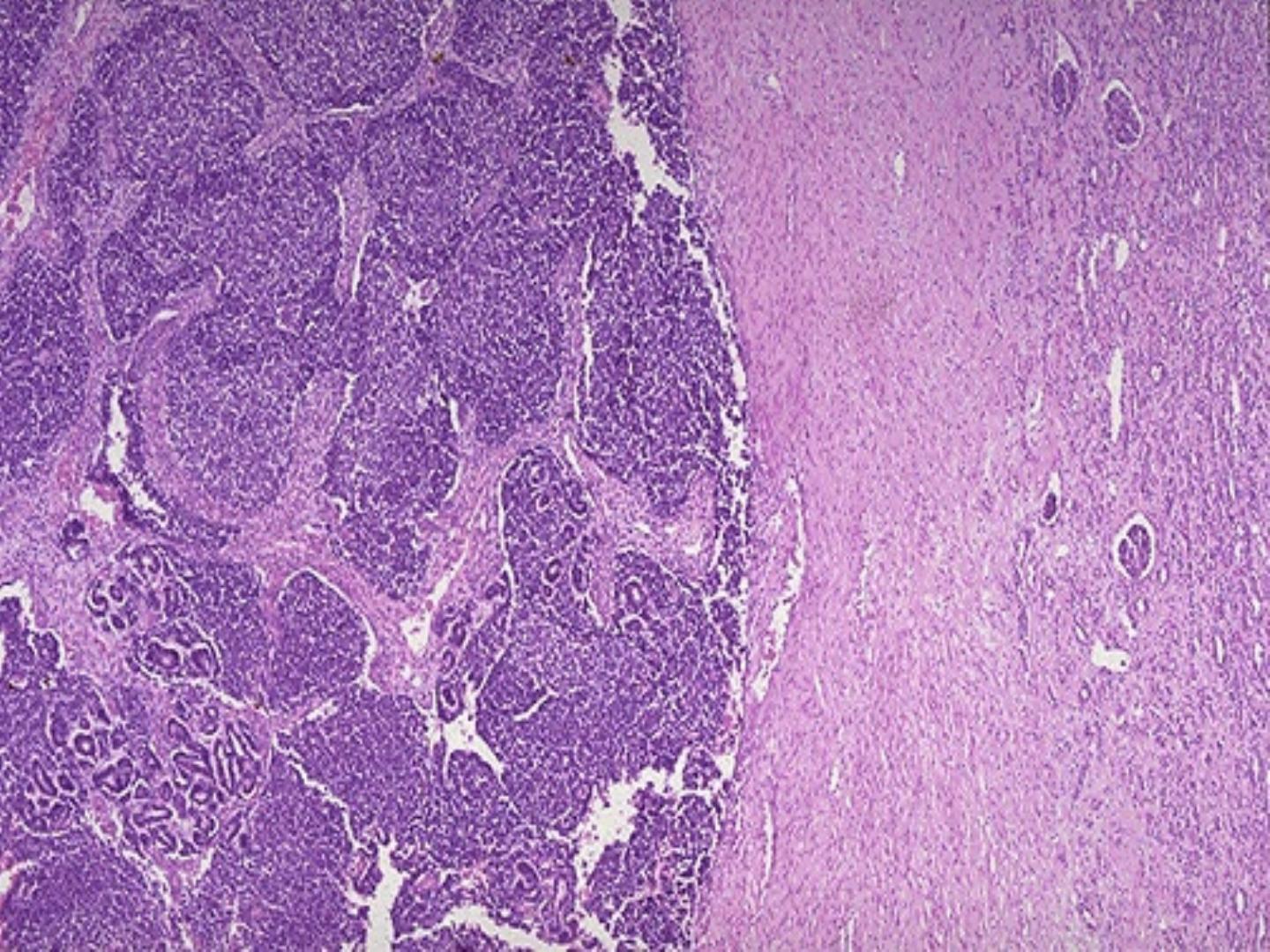
1/Nephroblastoma (Wilm’s Tumor)
• It is seen primarily in infants and children.
• There is no sex predilection.
• The classical clinical presentation in form of an
abdominal mass
,
hematuria and pain are rare.
• Other features include; hypertension, proteinuria and sometime
tumor rupture.
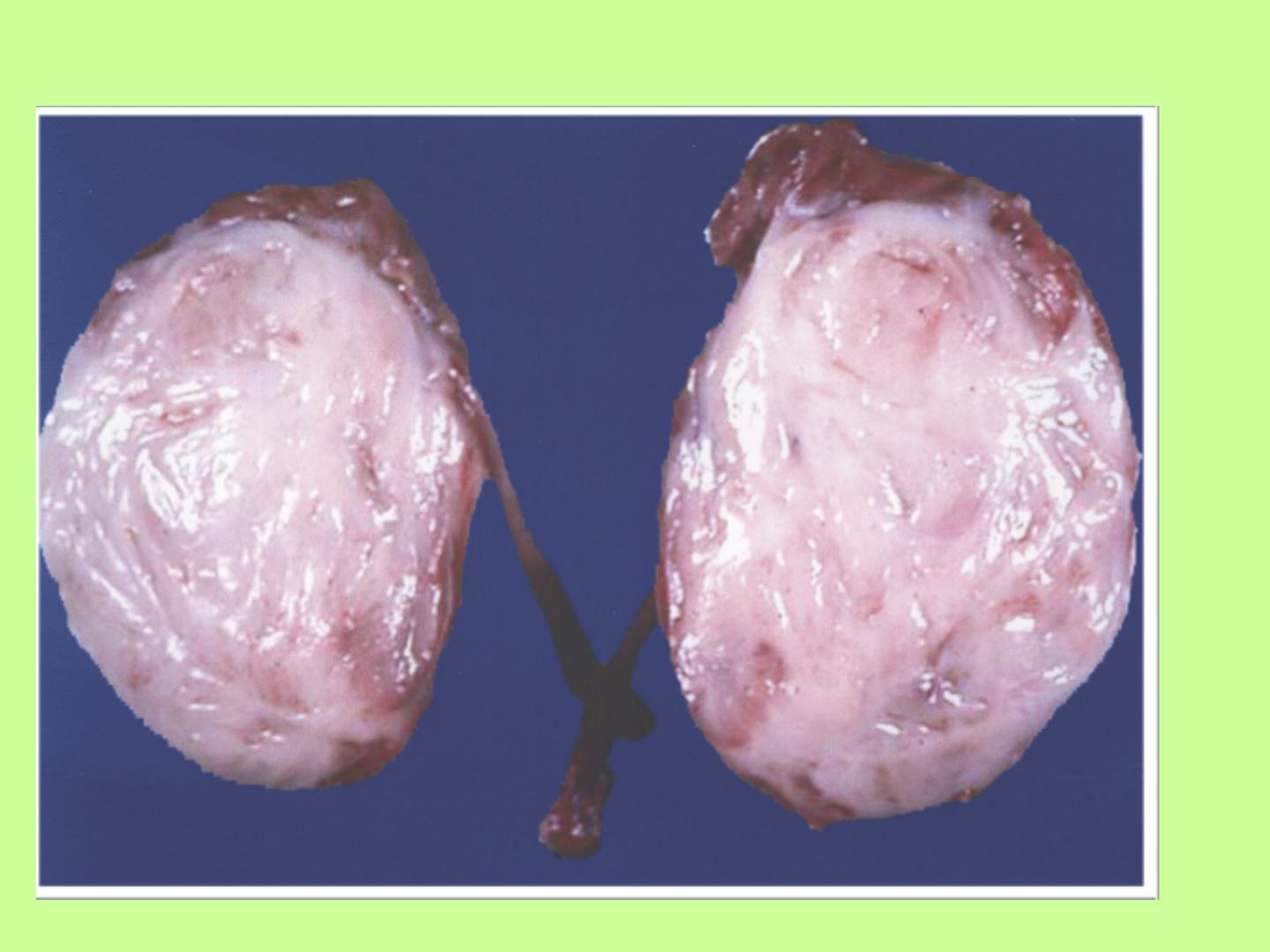
Morphologic features
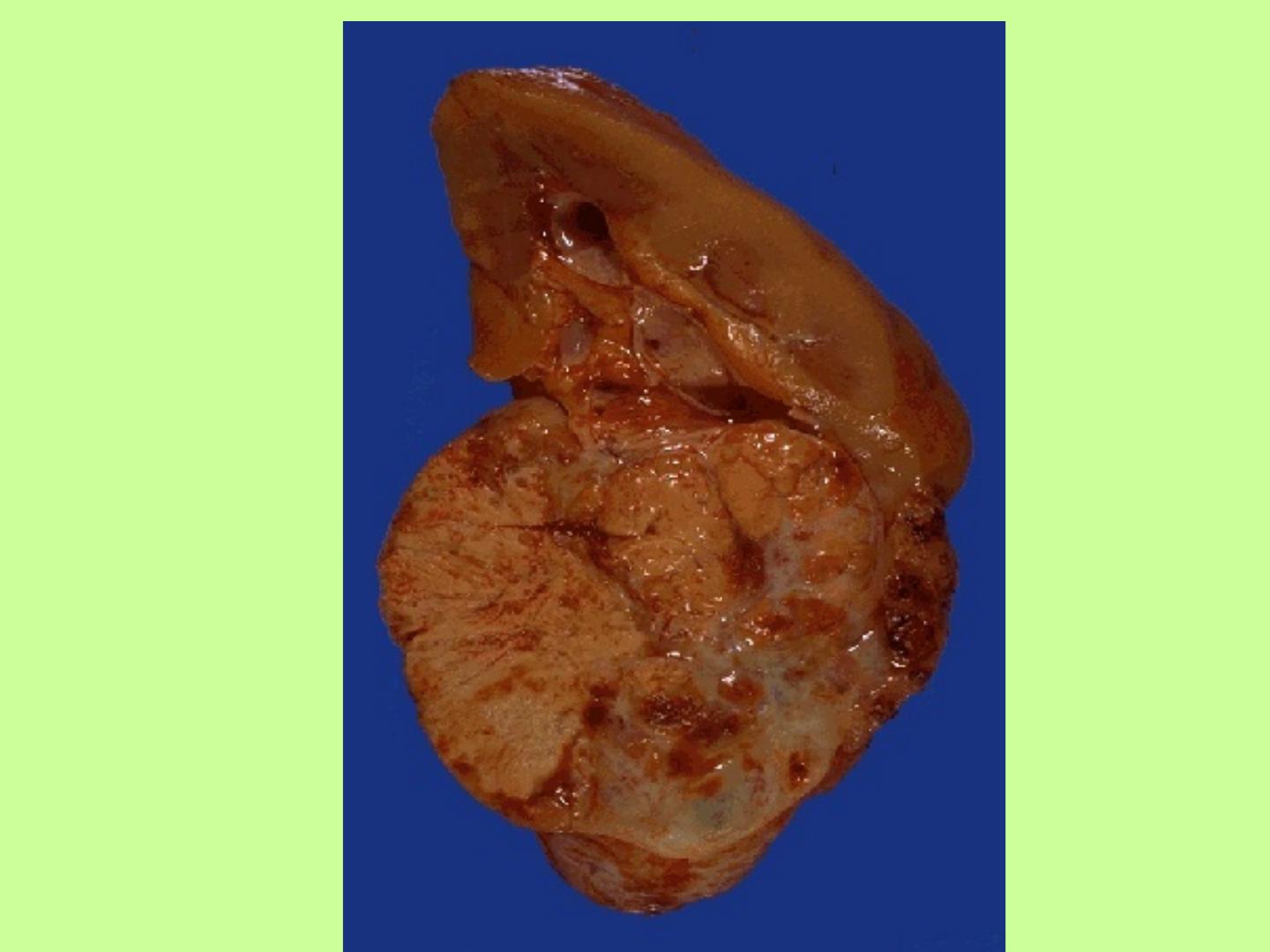
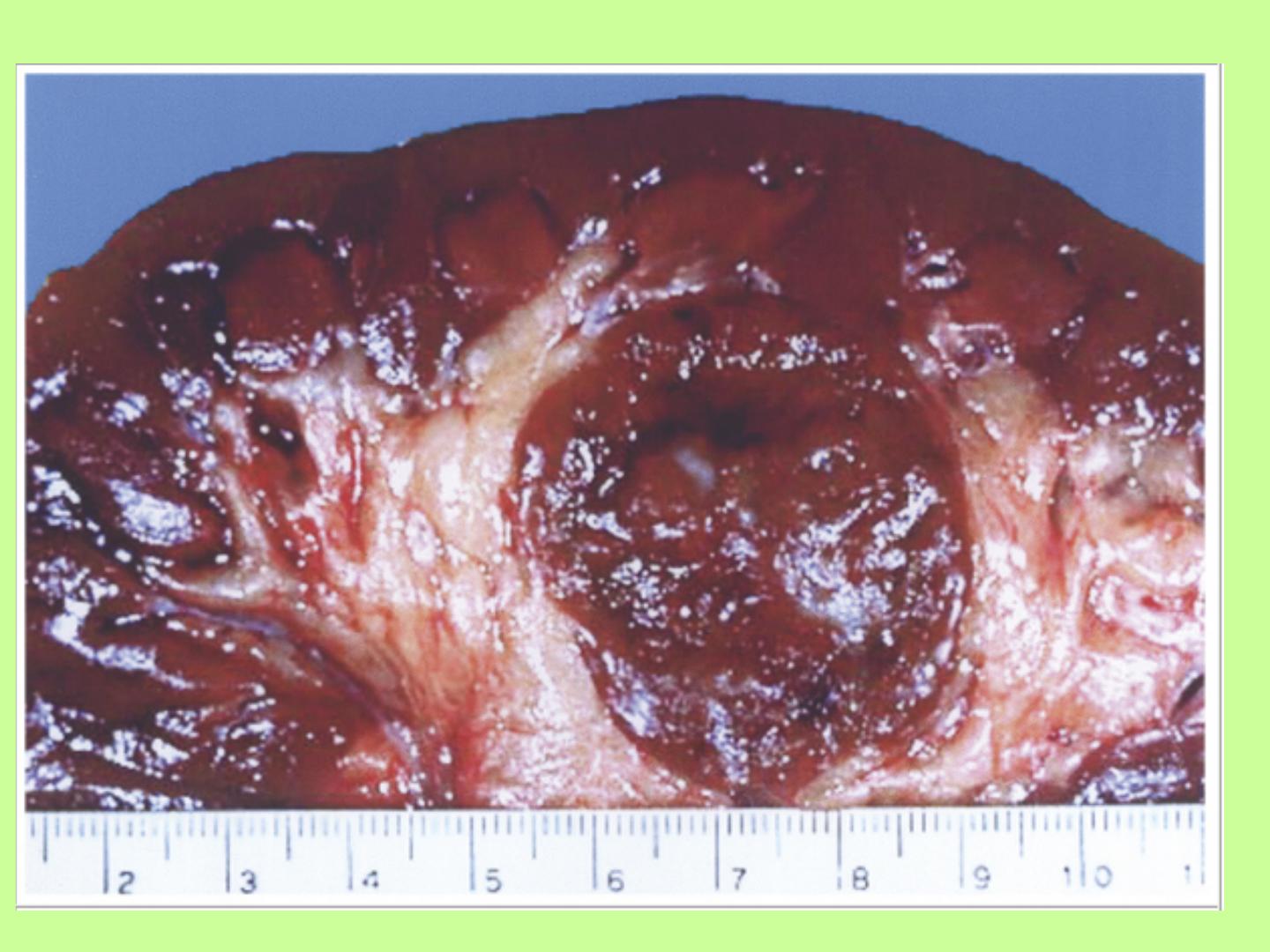
Grossly:
• Tumors are solitary, well circumscribed, rounded and of soft in
consistency.
• The size is variable, with a median weight of 550gm.
• The cut section is predominantly solid and pale gray or tan and
often exhibits areas of cystic change, necrosis, and hemorrhage.
• Multicentric foci are found in 7% of cases.
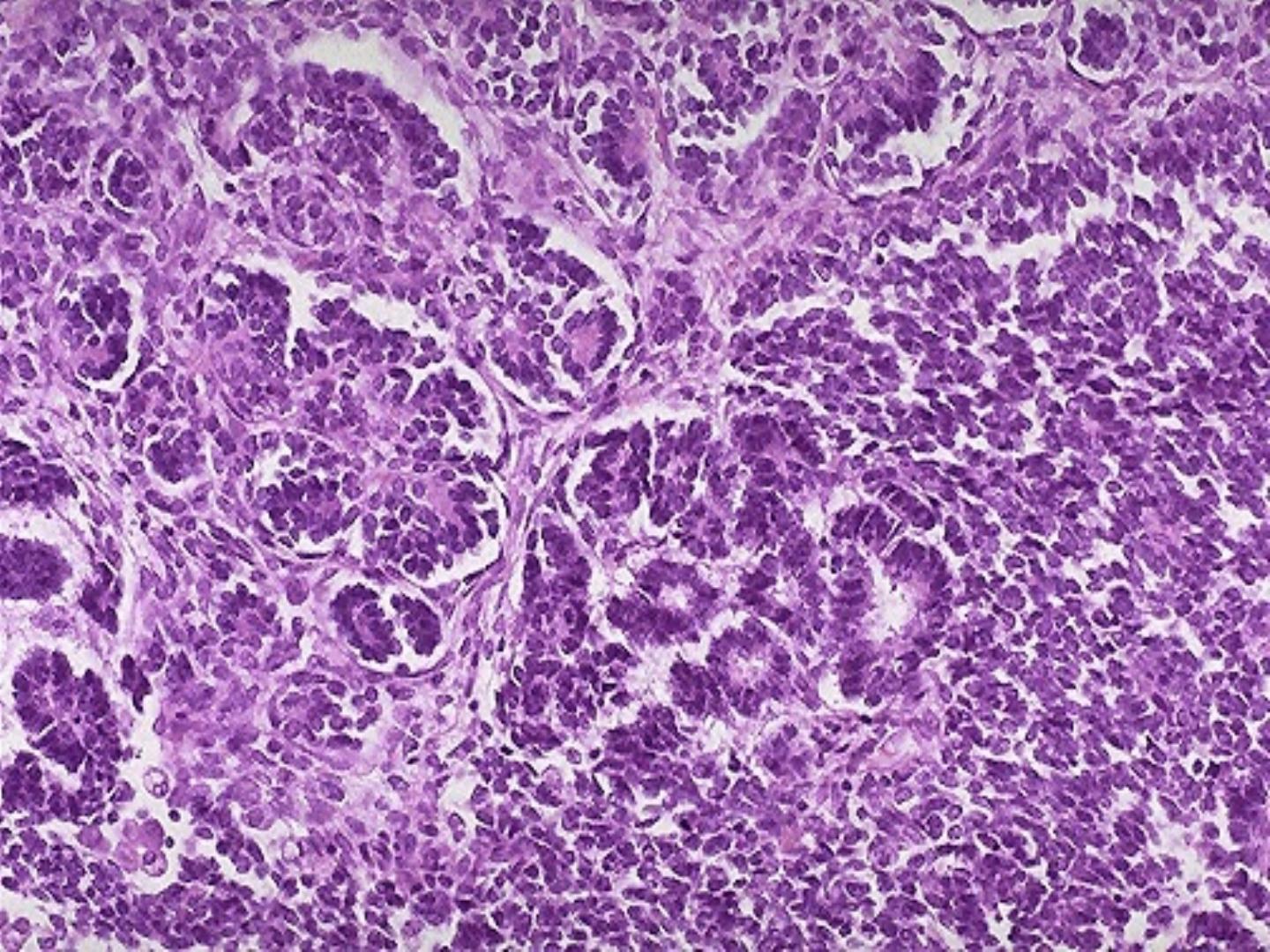
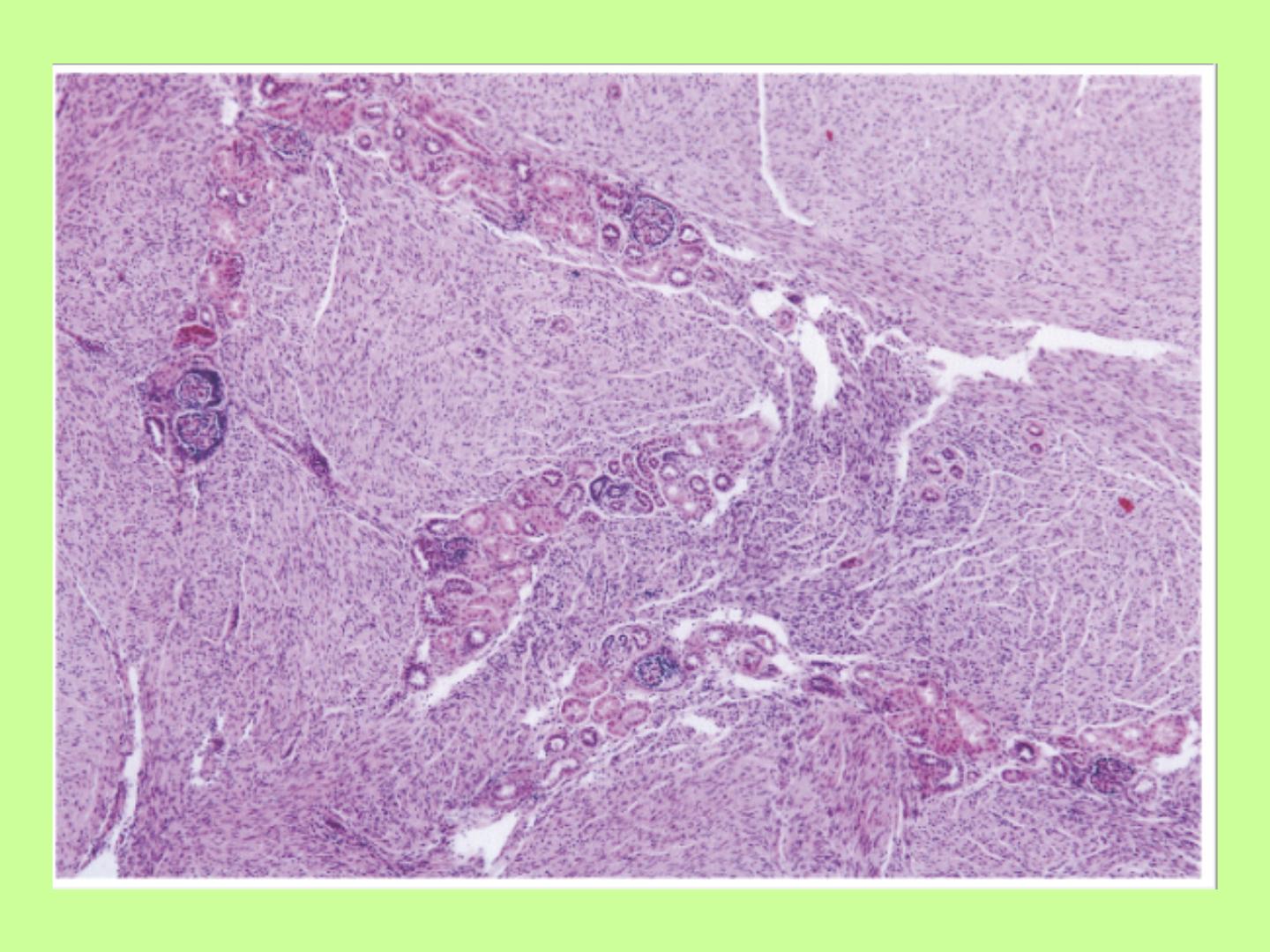
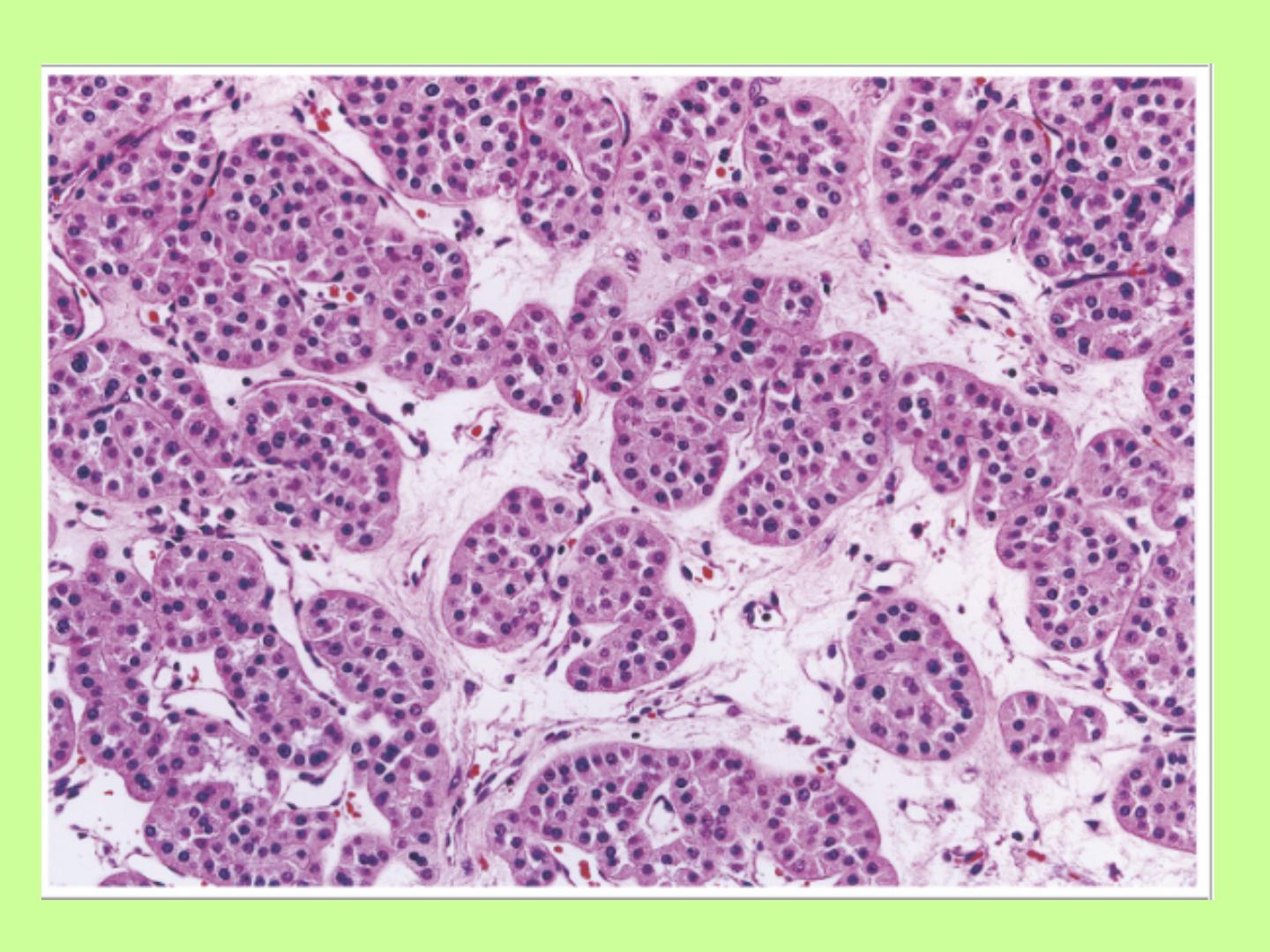
Microscopically:
• Three major components are identified
– 1. Undifferentiated blastema.
– 2. Mesenchymal (stromal) tissue.
– 3. Epithelial tissue
.
• Anaplastic features may be present focally or
extensively.

Molecular genetic features
• The genetic loci predisposing to nephroblastoma are:
1. WT1 located on 11p13.
2. WT2 located on 11p15.5.
3. Other chromosomal abnormalities include, 1, 7q,
12, & 16.
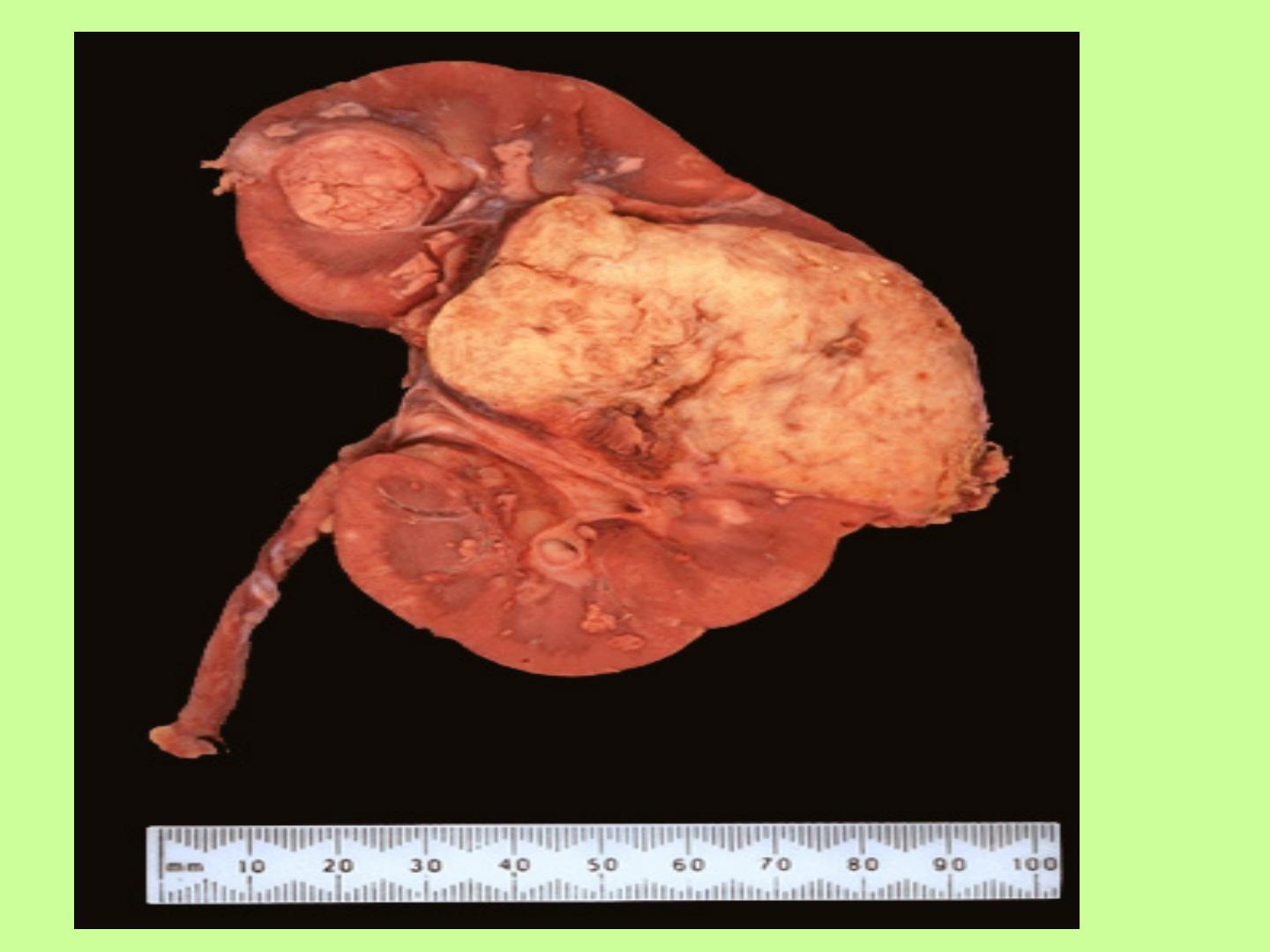
Mesoblastic Nephroma
• It is congenital renal neoplasm, usually discovered in
patients before they reach 6 months of age.
• Grossly, the tumor is solid, yellowish/grayish to tan with
a whorled configuration.
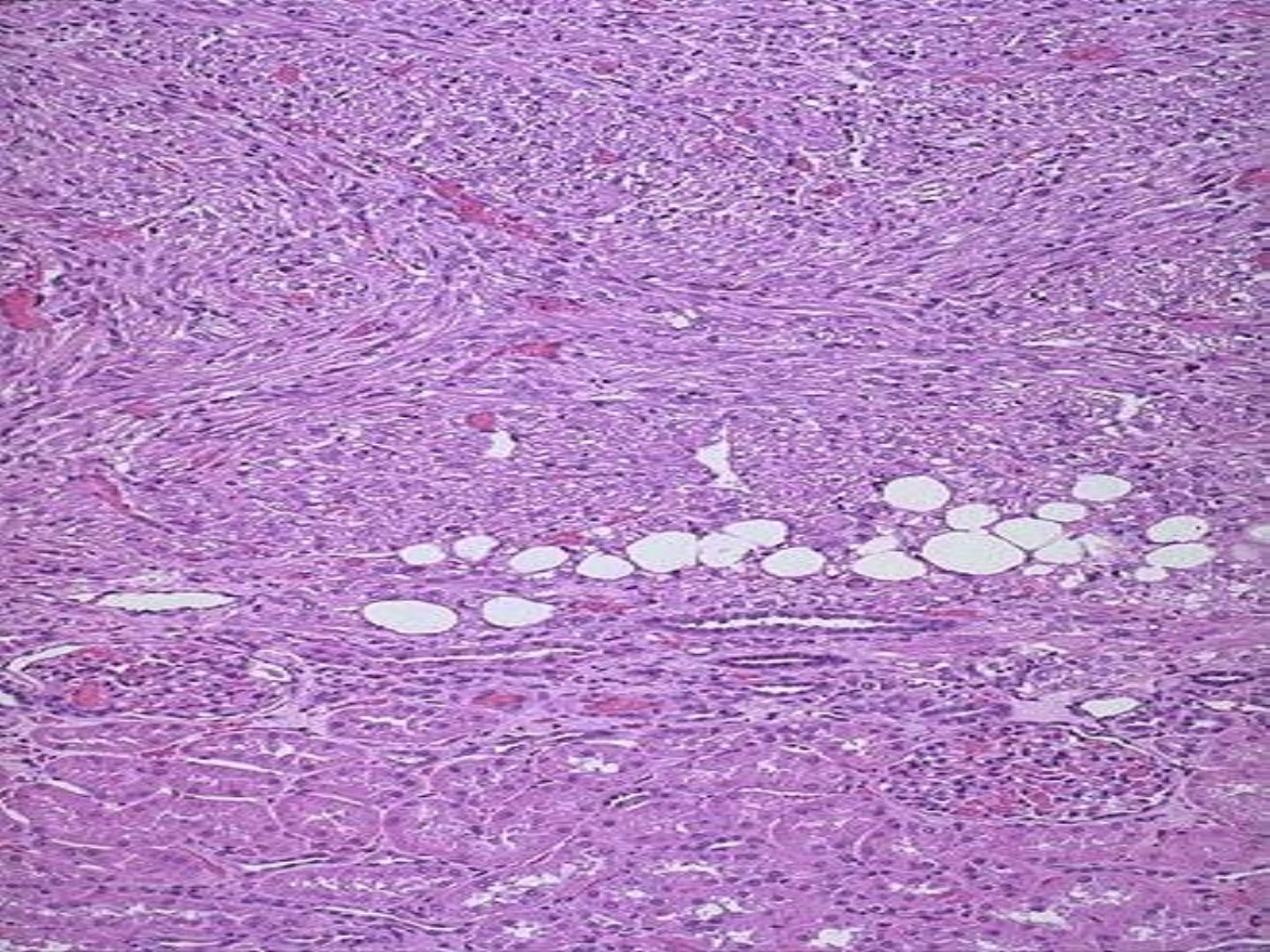
• Microscopically: A variably cellular growth of spindle
cells is the predominant feature.
• The large majority of mesoblastic nephromas are cured
following nephrectomy. In up to 7% of the cases,
recurrence may develop.
Adult Tumors And Tumor-Like Conditions:
1/Renal Cell Carcinoma
• Average age at diagnosis is 55-60 years. Rarely may
occur during childhood.
• The M:F ratio is 2:1,
• Epidemiology, there are many risk factors;
1. Tobacco is the most significant factor.
2. Obesity, particularly in women.
3. Hypertension.
4. Unopposed estrogen therapy.
5. Exposure to, asbestos, petroleum products, and heavy
metals.
Conditions that may be complicated by renal cell carcinoma are
the followings;
• 1. von-Hippel-Lindau (VHL) disease, renal cell carcinoma occurs
in more than 50% of individuals with this syndrome.
• 2. Acquired cystic renal disease, about 50% of the patients on
long-term dialysis develop renal cysts, 7% of cases are
complicated by cancer.
• 3. Adult form of polycystic kidney disease and multicystic
nephroma.
• 4. Lymphoma.
Clinical features
• It usually presents with
hematuria, flank pain or
abdominal mass
. However, this diagnostic triad occurs
in only 9% of the patients.
• Other manifestations are weight loss, anemia, fever, and
symptoms caused by metastatic deposits.
• Rarely paraneoplastic manifestations may occur.
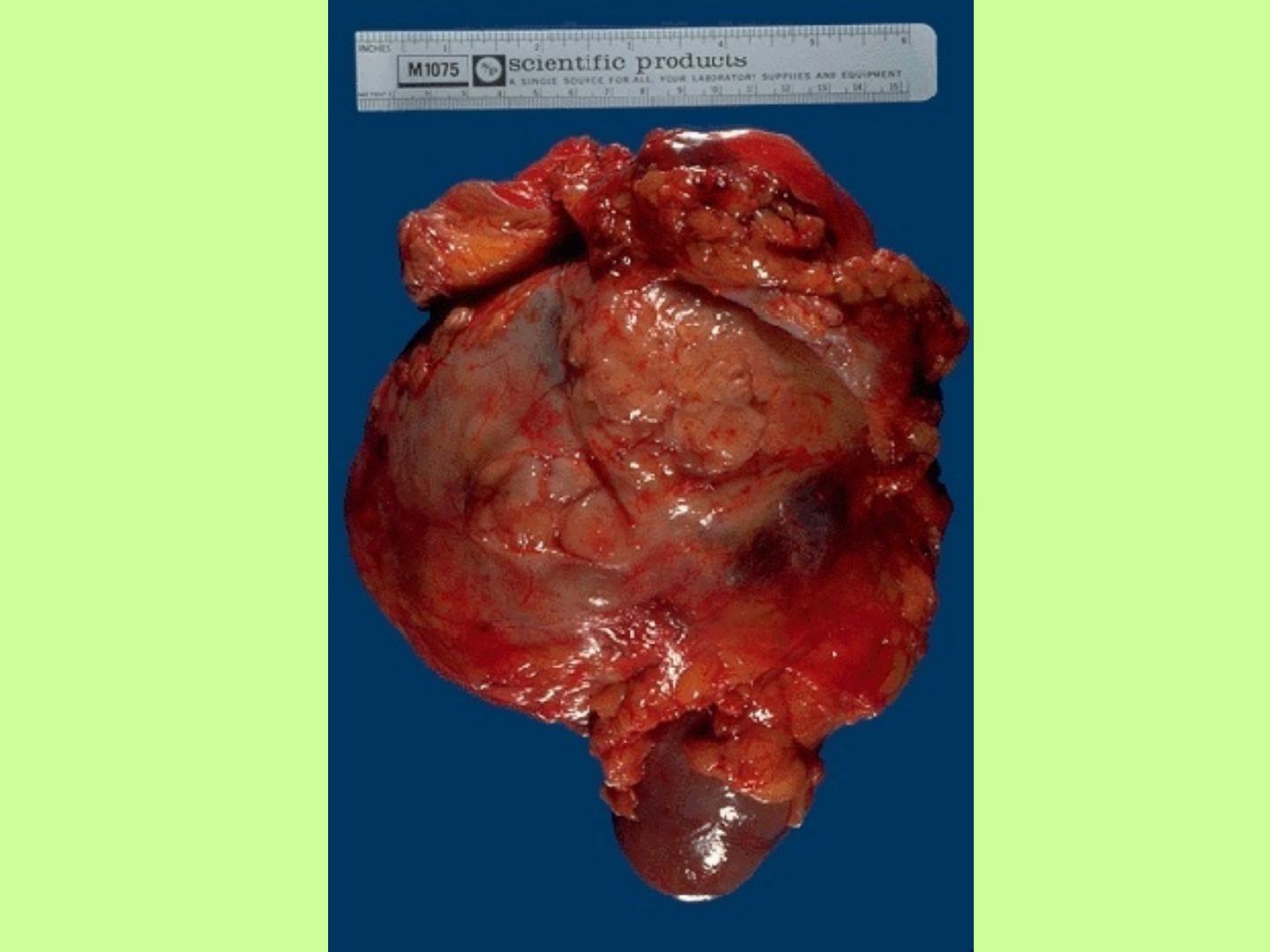
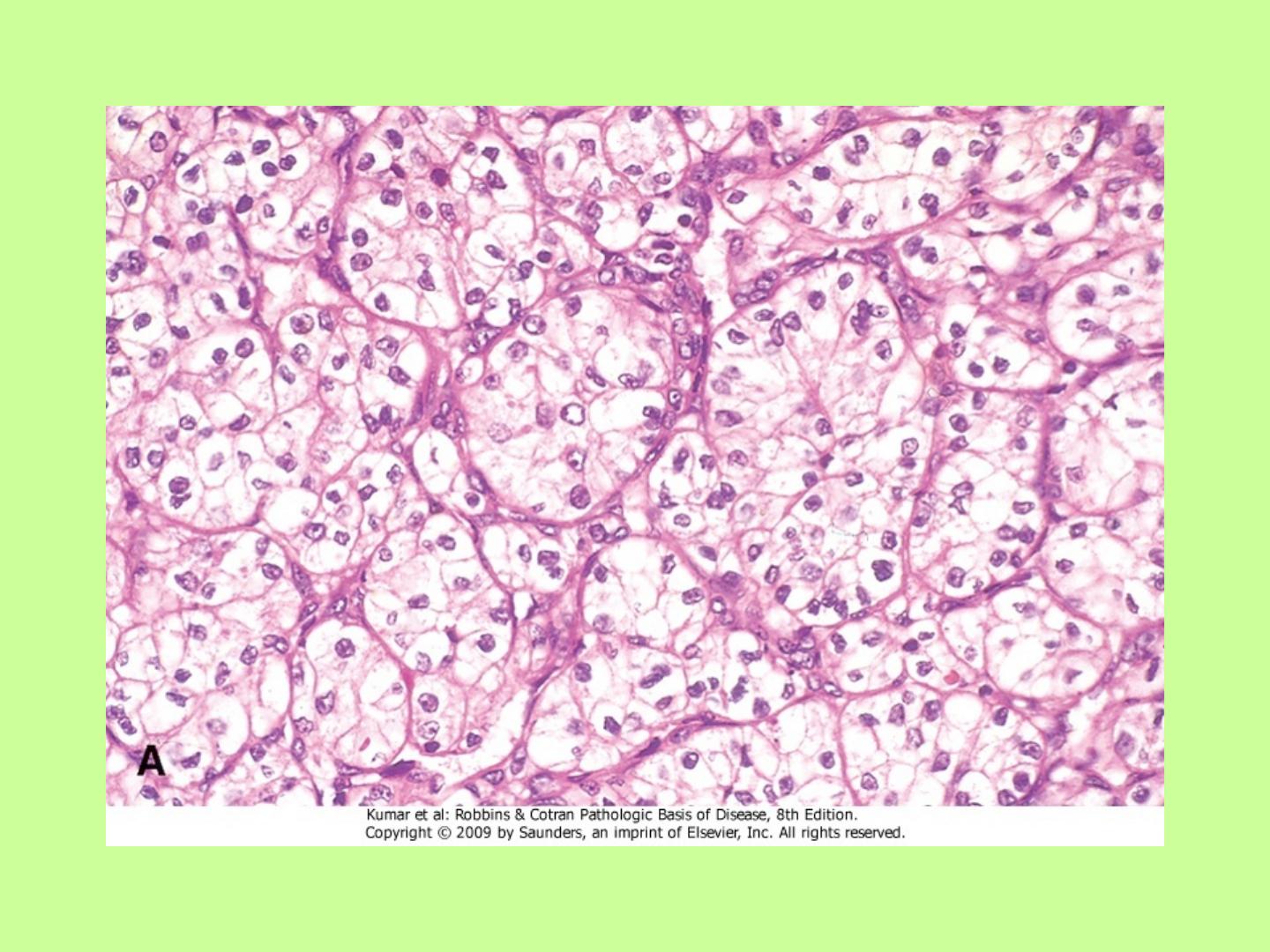
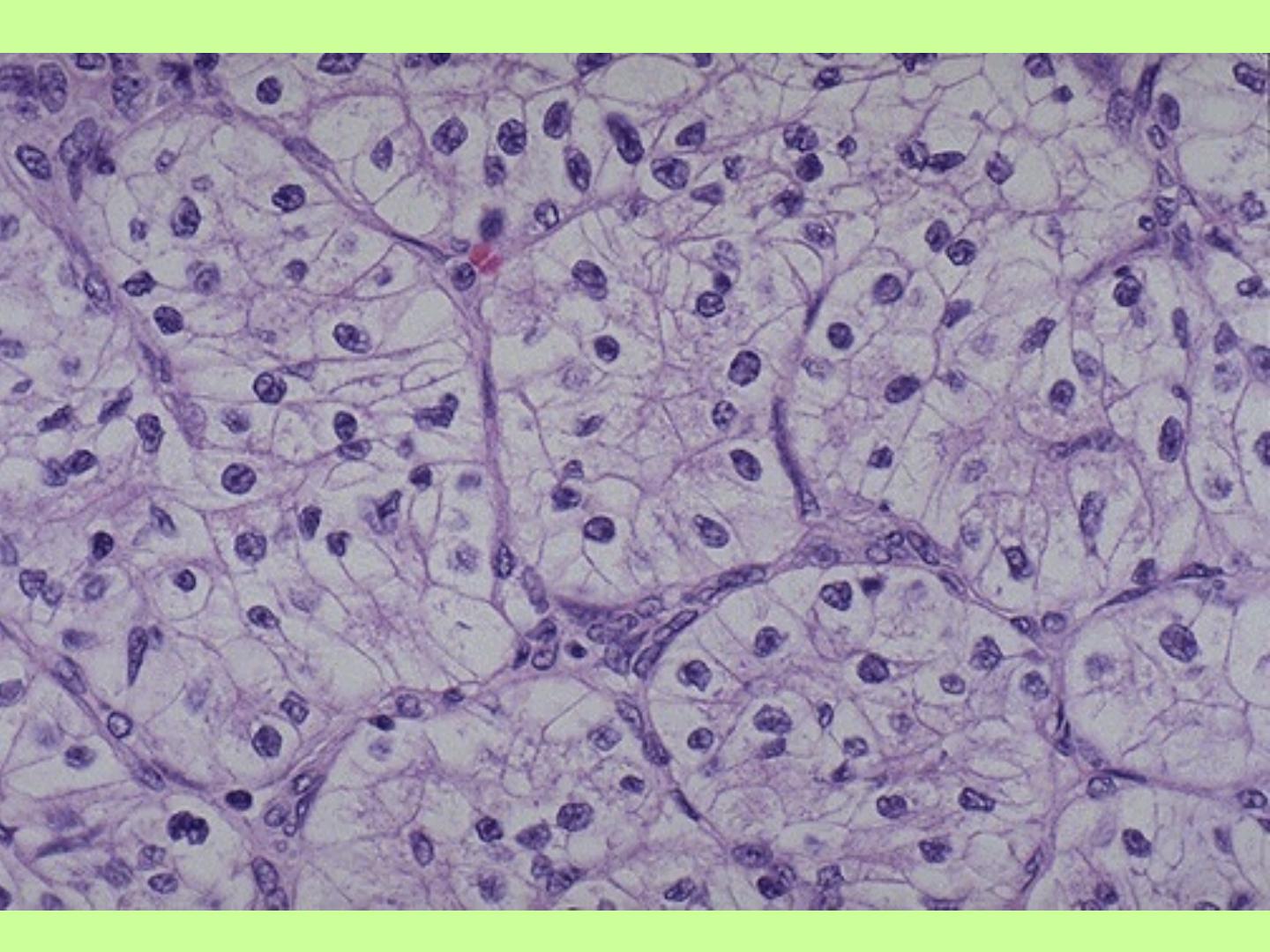
Morphologic features
• Grossly, most renal cell carcinomas are well delineated
and cortical in location. Usually the cut surface is solid
golden/yellow in color.
• Areas of hemorrhage, necrosis, calcification, and cystic
change are common findings.
• Microscopically, tubular and glandular growth of tumor
cells with large nuclei, and cytoplasm ranging from
granular to clear.

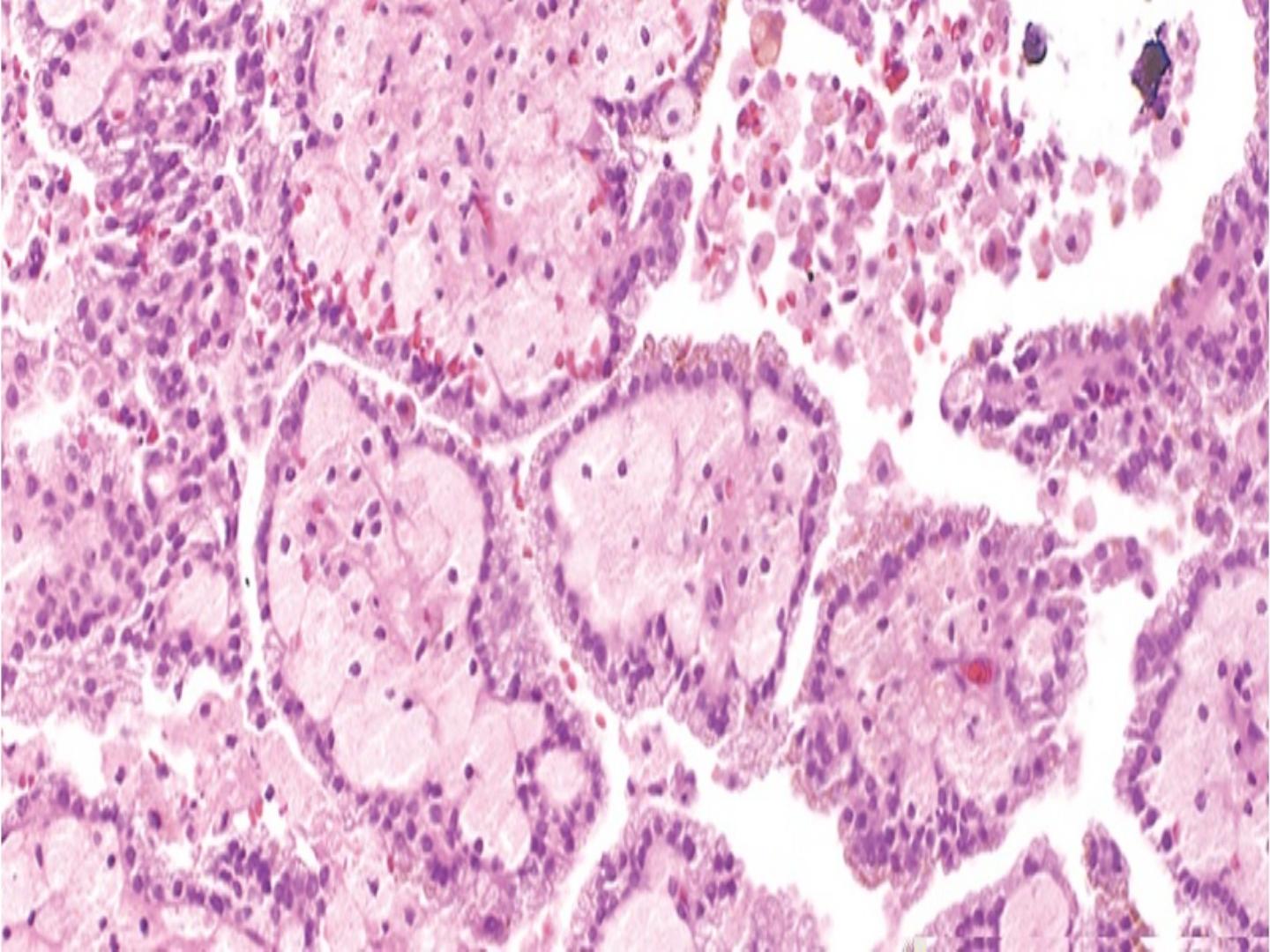
Other microscopic type
Papillary renal cell carcinoma,
• It comprises about 15% of all cases of renal cell
carcinoma.
• Renal tumors arising in patients on chronic
hemodialysis are of this type.
• Microscopically, complex papillary formations are
seen, and psammoma bodies are numerous. Stroma
is heavily infiltrated by neutrophils and foamy
macrophages.
• As a group, papillary renal cell carcinoma has a
better prognosis than conventional RCC
Spread and metastasis
• About 1/3 of renal cell carcinomas are found to invade
perinephric fat and/or regional lymph nodes at the time of
operation.
• Renal vein invasion is seen on only 10% of cases.
• Approximately 1/3 of patients with renal cell carcinoma
already have distant metastases at the time they seek medical
advice, lung and skeleton, being the most common sites.
• Metastases can also develop in the adrenals, liver, skin, soft
tissue, CNS, ovary, and almost any other site. Sometimes,
these metastases develop years or decades after the removal of
the primary tumor.
Oncocytoma
• Oncocytomas make up approximately 7% of all primary
nonurothelial epithelial renal neoplasms.
• Grossly, they are typically solid and mahogany brown, often
have a central stellate scar, and can reach huge sizes.
• Microscopically, are composed of entirely of cells with abundant
acidophilic granular cytoplasm, arranged in alveolar or tubular
fashion.
Angiomyolipoma
• Most patients are adults.
• Approximately 1/3 of the patients with this tumor suffer from
tuberous sclerosis
• Grossly, the tumor may closely simulate renal cell carcinoma,
because of the admixture of yellow areas and hemorrhagic areas.
• Microscopically, there is admixture of mature adipose tissue,
tortuous thick-walled blood vessels, and bundles of smooth
muscle
Tumors of Renal Pelvis and Ureters
Transitional Cell Carcinoma
;
Most cases occur in adults.
• There is a history of analgesic abuse and/or coexistence of
renal papillary necrosis in approximately 1/4 of cases.
• Cases have been seen following administration of thorotrast
• Grossly, the tumors are soft, grayish/reddish masses, often
diffusely involving the entire renal pelvis and may extend to
the ureters. Tumors of the ureters might be located anywhere
along their length.