DENTAL CARIES
Dr.Manar MudhafarPh.D.,Oral Pathology
The Scientific Language Is Latin or Sometimes Greek.WHY????????
THE ORIGIN OF THE WORD CARIES IS,LATIN:Meaning :ROTTENNESS.
Dental Caries
Is almost the most common cause for tooth loss.World-wide.
Essential requirements for development ofdental caries
1. Bacterial plaque biofilm2. Cariogenic (acidogenic) bacteria
3. Plaque biofilm stagnation sites
4. Susceptible tooth surfaces
5. Fermentable bacterial substrate (sugar)
6. Time
RAMPANT CARIES

.
Extensive caries of deciduous incisors and canines.
This pattern of caries is particularly associated with the use of
sweets and sweetened infant drinks
The stagnation area in an occlusal pit. A ground section of a molar showing the size of the stagnation area incomparison with a toothbrush bristle placed above it. The complete inaccessibility of the stagnation area to cleaning is obvious.
Wordwide problem
Oral conditionin an elderly Chinese man
Massive dental plaque in an adult Kenyan man. The oral hygiene among these populations is very bad with swollen gums, but people rarely lose their teeth becauseof periodontal loss of attachment. Dental caries is the principal cause of tooth loss.

Worldwide problem
Fifty years ago
Danish and English adults,
including those with deep
caries lesions in molar teeth,
had their teeth repaired
using dental amalgam.
The figure shows poor
oral hygiene, old amalgam
restorations, fractured teeth,
and new lesions formed
adjacent to the fillings.
Re-restoration is needed
The restorative cycle

The restorations
In previous Figure have beenreplaced, but even these
very nice restorations will
deteriorate over time if
there is no proper oral
hygiene as part of caries
control. Hence, the
vicious circle of
re-restoration continues.
A pain-free, functioning, and good-looking dentition for a lifetime seems a reasonable goal! Is this what dentists do? Dentists practising general dentistry: provide amalgam and composite fillings, sealants, cosmetic dentistry, pulp and root canal treatment, crown and bridges, dentures, and dental implants. ALSO they do minor oral surgery, gum disease treatment, and occasionally Temporomandibular joint (TMJ) therapy, tobacco cessation, and nutrition counselling. The topics listed comprise the daily work in general dentistry, but do you realize that 85% of these are a direct consequence of dental caries? Yet dental caries is not mentioned as the main reason for most dental treatments. Restorative treatment is the focus of dentistry. The disease dental caries is the only disease which has been combatted with metals and composites for more than a century.
Restorative cycle
Adult patient with an extracted lower first molar and amalgam restorations.The remaining amalgams have been polished and the patient has been
carefully instructed on how to control dental caries. Therefore, there are several
arrested, almost black, caries lesions in the exposed root surfaces of the upper
premolars and lower second molar.
Restorative cycle
An adult who has so far not had appropriate caries control and hasentered the restorative cycle. In the upper jaw, the central incisor has an ill fitting jacket crown. There is a 5-unit bridge replacing the premolars and a plastic
restoration is present on the distal surface of the canine. Here, the dentist has
probably tried to repair a secondary caries attack next to the gold. The second
molar has been extracted. In the lower jaw the first molar has also been extracted.
Buccal amalgam restorations are present on the second premolar and molar, but
notice the one in the molar is plaque covered. There is a gold foil restoration on the
first premolar. These are time-consuming to insert and therefore expensive, which
indicates that this patient has actually invested in restorative care. What will happen
to this dentition over the next 5 years?

D.C. definition
It is a localized, chemical dissolution of a tooth surface brought about by metabolicactivity in a microbial deposit (a dental biofilm) covering a tooth surface
at any given time. The dental biofilm (called dental plaque) is a microbial
biomass composed of resident bacteria from saliva (see Chapter 2). The dental
biofilm is disturbed when brushing the teeth. The micro-organisms metabolize
sugars from the diet and, as a waste product, produce acid. This acid can demineralize
enamel, dentine, and cementum, and the lesions manifest themselves
clinically in a variety of ways as will be described.
Dental caries lesions result from a shift in metabolic activity accompaniedby a gradual change in ecology of the dental biofilm, where an imbalance inthe equilibrium between tooth mineral and biofilm fluid develops.
However,
the biofilm is a prerequisite for caries lesions to occur. Dissolution (demineralization)occurs when acid forms and biofilm pH drops below a certain level.
Redeposition (remineralization) of minerals occurs when biofilm pH goes up
again. These changes take place at the interface between the biofilm and the
tooth surface numerous times during a day, and can be modified extensively.
D.C. classification
Active fissure
caries on the occlusal
surface of a molar.

Inactive
occlusal surface caries.These lesions are not cavitated.
D.C.
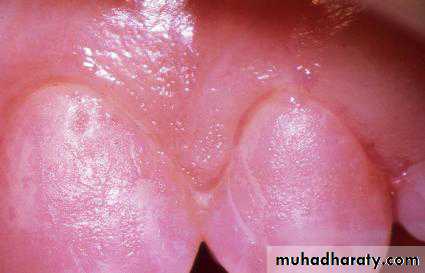
Buccal surface with active enamel caries lesion. The early stagesoften appear chalky white (also called ‘white spot’ lesion)

Inactive or arrested caries lesion on an approximal surface. Such lesions are often partly stained.
D.C.

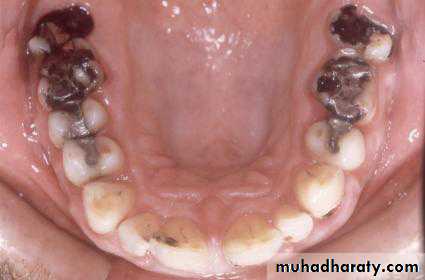
Figure shows Heavily restored dentition with many inappropriate
restorations, where new caries lesions continue to develop as the rootsurfaces are exposed. These new lesions at the margins of the restorations are called secondary or
recurrent caries, and they are then restored.
TYPES OF D.C.
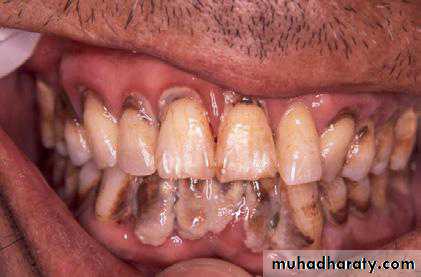
The patient has invested in expensive gold restorations. However, a new lesion is developing on mesial surface of the lateral incisor.
Note the staining (the patient is a smoker!) of the margins of old silicate fillings and along the enamel-cementum junctions.

RAMPANT , means:FAST
Rampantcaries in a child.
These are deciduous teeth.
DECIDUOUS,means: FALLING.

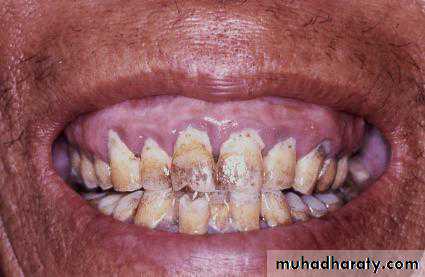
Rampant caries also in adults.
Figure shows Rampantcaries in an adult. The
patient was a baker and
such lesions have been
designated ‘baker’s caries’.
Rampant caries
is the name given to multiple active lesions occurring in the
same patient .
This frequently involves surfaces of teeth
that do not usually experience dental caries. Sometimes the patients with rampant caries are classified according to the assumed causality, e.g. bottle or nursing caries in children, and bakers’ caries, radiation caries, and drug-induced caries ???when seen in adults.
Early childhood caries (ECC) is caries in the age group 12–30 months, and there is a specific pattern that differs from caries in older children. The upper incisors are the most vulnerable . This is simply caries on teeth that are not clean, exposed to carbohydrates, and located in an area of the mouth, where oral clearance is low
In order to be able to control dental caries it is necessary to understand how a lesion develops and progresses with time, if not interfered with.
D.C.
A tooth from Imperial Rome 2000years ago with a large
approximal caries cavity.
PATHOLOGY OF D.C.
The oral cavity is an open sink. The mucous membranes and teeth are constantly covered with a salivary film whose proteins adhere to all surfaces in the mouth. Saliva is not just a fluid flushing through the oral cavity, but a highly complex proteinaceous liquid that contains millions of microorganisms (bacteria).Depending on their different surface properties (different species have different surface proteins comprising their cell wall, which coat the surface of each cell) they stick to the salivary proteins at the surfaces of mucous membranes and teeth. These oral microorganisms comprise the endogenous flora of the mouth. They are living in symbiosis with the cells of the human body and comprise what is today called the metagenome.
META:Gr.:after,beyond,over.
GENOME: the complete gene complement of an organism.
Until recently, traditional bacteriological methods were used to isolate andculture microorganisms in the laboratory, but it was realized that only a fewcould be cultivated!
According to some estimates, about 99% of prokaryotic species
remain to be characterized.
For this reason alone, it does not make sense to think that a particular ‘caries microorganism’ exists. There are also implications for the many attempts to find
salivary microbial and biochemical biomarkers that might be used clinically to assess caries risk.
The fact that the oral cavity is stuffed with bacteria does not mean that they
need to be eradicated. They comprise part of the individual and each patient has his/hers own endogenous flora, but as a health professional one should always
maintain correct personal hygiene (wash hands, use gloves, do not touch the dental chair/lamp, etc., with spit on the fingers) to avoid spreading infections between patients.
A dental biofilm is defined as a microbial community growing on a tooth surface.
Microorganisms attach to all surfaces that are covered with a proteinaceous film and stick to them. In the oral cavity, however, the squamous epithelial cells desquamate and, hence, mucosal surfaces, such as cheeks, lips, and palate, do not allow growth of a biofilm, whereas tooth surfaces are stable. Wherever there is a stagnation area (between teeth, dental grooves, and fissures, along the gingival crevice, along filling margins, orthodontic brackets, dentures, etc.), a biofilm will form.
If left undisturbed there is a microbial succession, continued growth and an increased species diversity resulting in a ‘mature’ or climax type of biofilm within a week. This structure is often referred to as dental plaque.
STAGES OF ENAMEL CARIES
The early (sub-microscopic) lesion• Phase of non-bacterial enamel crystal destruction
• Bacterial invasion of enamel
• Cavity formation
• Undermining of enamel from below after spread into dentine.
Early enamel caries, a white spot lesion, in adeciduous molar. The lesion forms below the contact point, and in consequence is much broader than an interproximal lesion in a permanent tooth.
DENTAL BIOFILM
Cervical half of two teeth demonstrating a24-hour dental biofilm.

After application of a disclosing solution, the dental biofilm is more easily discernible.
Dental biofilms of unknown age in an (a) African adult and in an (b) elderly Chinese. It is obvious that these patients do not use oral hygiene measures.Note how much difference there can be between individuals—and yet we talk about dental biofilm (or plaque) in general terms.

the enamel surface is in a state of dynamic equilibrium with its surrounding environment. When the cumulative result of the numerous pH fluctuations over months or years is a net loss of calcium and phosphate, of an extent that makes the enamel sufficiently porous to be seen in the clinic, it may be diagnosed as ‘a white spot lesion’.
dental caries lesions are a result of an imbalance in physiological equilibrium between tooth mineral and biofilm fluid.
These lesions (WHITE SPOTS)are a symptom of biofilm activity.
Exposure to acids may lead to two types of lesion, the caries lesion and erosion.

Eroded occlusal surfaces exhibiting different degrees of erosion, starting with a rounding of contours to almost total exposure of the dentine after removal by the acids of the covering enamel. (a) Molar and premolar with a little wear.(b) Premolars with deep wear down to the yellow dentine.

PATHOLOGY OF ENAMEL CARIES
Enamel, the hardest and densest tissue in the body, consists almost entirely of calcium hydroxyapatite with only a minute organic content. It forms a formidable barrier to bacterial attack. However, once enamel has been breached, infection of dentine can spread with relatively less obstruction.Preventive measures must therefore be aimed primarily at stopping the initial attack or at making enamel more resistant.
Enamel is rendered carious by acid diffusing into it and dissolving it.
Caries is not a simple solubilisation of enamel, but a dynamic process of alternating phases of demineralization and remineralization.
ENAMEL CARIES
ENAMEL CARIES
Early approximal caries. Ground section in water viewed by polarised light. The body of the lesion and the intact surface layer are visible. The translucent and dark zones are notseen until the section is viewed immersed in quinoline
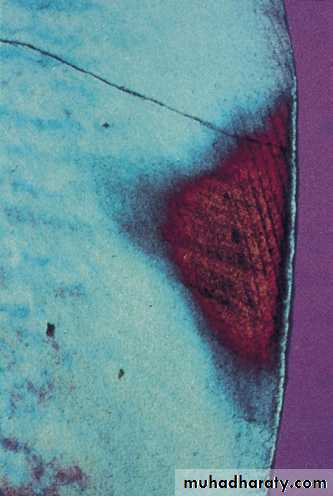
Early approximal caries. Ground section viewed by polarised light after immersion in quinoline. Quinoline has filled the larger pores, causing most of the fine detail in the body of the lesion to disappear, but the dark zone with its smaller pores is clear.
As noted earlier, the initial attack on enamel appears to be by highly mobile hydrogen ions permeating the organicmatrix to attack the surface of the apatite crystals
The apatite crystals become progressively smaller.
Microdissection of the translucent zone has shown that the apatite crystals have declined in diameter from the normal of 35–40 nm to 25–30 nm and in the body of the lesion to 10–30 nm. In the dark zone, by contrast, enamel crystals appeared to have grown to 50–100 nm and in the surface zone to 35–40 nm. These findings also support the theory that both demineralisation and remineralisation occur in phases. This changes,(WHEN????) once cavitation develops and demineralization comes to dominate the process. Until then, bacteria cannot physically penetrate enamel because of the intact surface layer.
When sections of teeth are examined in water with polarized light thepores in the enamel are filled with water. Water has a lower fracretive index thanenamel. The white spot caries lesion has a pore volume of more than 5% on a smoothsurface (a). When the same section is examined in a solution which has the samerefractive index as enamel, but a molecular size that does not allow it to sieve into thesmall pores at the advancing front of a lesion, a so-called dark znoe is observed (b).
When sections are examined by X-rays (microradiography) the calciumloss is directly shown as darker areas in the otherwise white, highly mineralizedenamel. Note how the surface enamel varies in mineral content, but is bettermineralized than the body of the lesion.
When examining the enamel surface of an active white spot caries lesion in the scanning electron microscope (SEM), however, the surface appears moth eaten because the spaces between the individual crystals are widened. It is porous and a probe tip will feel the roughness when gently moved across the lesion.
Low-power view of caries spreading along thealmeodentinal junction. Note how it spreads only a smalldistance in advance of caries in dentine. The amelodentinaljunction is only a little more susceptible to carious spread thandentine(WHY???).

Caries spread along the amelodentinal junction at higher power. The greater porosity and organic content here allows caries to spread preferentially laterally, though it only spreads to match the lateral extent of the surface caries, until a late stage

Process of enamel caries
• Permeation of the organic matrix by hydrogen ions causes sub-microscopic demineralisation• Microradiography confirms that these changes represent areas of increasing demineralization . • The dark zone is evidence that remineralisation occurs within the cavity
• The surface zone is largely formed by remineralisation • There is alternating demineralisation and remineralisation
• When demineralisation is predominant, cavity formation progresses
• When remineralisation is predominant, caries arrests but normal enamel cannot reform
• Bacteria cannot invade enamel until demineralization provides pathways large enough for them to enter
(cavitation).
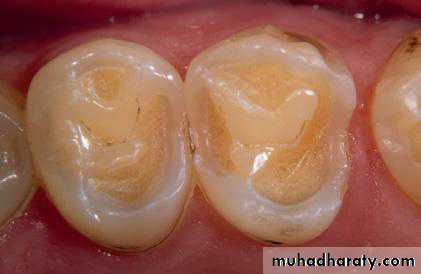
In occlusal surfaces a caries lesion starts at each side of a fissure and, because ofthe anatomy, the mineral loss occurs in the enamel following the prism direction. This creates a cone shape with the broad base towards the interior of a tooth. Therefore, when the enamel breaks down, the cavity appears bigger than assumed atthe surface because the dentine is involved at the base of the cone.
The description clinically reflected when comparing the occlusal lesion (a) before and (b) after opening the cavity in this lower second molar

Undemineralized section
A section of an approximal space between two neighbouring molars with two caries lesions extending into dentine, but without cavity formation. Note the dentine reactions involve all the dentinal tubules affected by the acid attack at the enamel surface.A bitewing radiograph showing caries in enamel and dentine on the mesial aspect of the upper first molar. A lesion is also visible on the mesial aspect of the lower first premolar.

This reflects the maximum possible effect of so-called remineralization. The surface areas of the lesions have diminished a little. As a result of good oral hygiene the gingival inflammation has disappeared and, as a consequence, the marginal gingiva has retracted exposing a cervical rim of sound enamel cervical to the inactive lesions, which are now left as scars in the enamel.

Scanning electron microscope pictures of surface enamel of an inactive caries lesion. Note how the surface appears polished, leaving small irregularities where crystals can be discerned. At the higher magnification of part of the small irregularity, it is evident that where the polishing cannot affect the bottom of these irregularities, the spaces between the crystals in inactive lesions have been reduced.
D.C.

A micro-computer tomography (micro-X-ray method) scan through a 2000-year-old Roman tooth with approximal lesions non cavitated lesion in the framed site and a large cavitated lesion in both pictures.
Note the mineral deposition walling-off the cavity along the borders of the dentine.
HISTOLOGICAL GROUND SECTION
Histological ground section throughan undemineralized molar with a large occlusal active caries lesion. Note that
the lesion almost extends to the pulp chamber and along the advancing
front there is a rim of tertiary dentine. It is also remarkable that, although
extensively demineralized, the gross Structure of the dentine remains.
Assuming that the pulp is vital, imagine what would happen if you choose to drill – or perform caries control where the softened dentine is partly removed, and partly remineralized.