
Hearing loss
Hearing loss: Is decrease person‘s sensitivity to sound
more than(20-25 dB HL) in 250-8000 Hz frequency rate.
* The people with hearing loss suffer emotional, social, and
communicative dysfunction.
*In children results in,
1.Delayed speech and language development.
2.Difficulties in learning, playing and developing social skills.
**Care must be taken for…
1*Unilateral sensori-neural hearing loss. with vertigo and tinnitus.
2*Abnormalities of nerves (other than hearing loss).
Classification of hearing loss according to severity.
Normal hearing. 20dB
Mild hearing loss 20-40dB HL
Moderate HL 40-70dB HL
Sever HL 70-90 dB HL
Profound HL 90-110db HL
Deafness >110dB HL
Physiology of hearing: The ear divided in to two parts.
1.Conductive apparatus: They magnify and transmit the sound wave
in to inner ear fluid. Consist
a. The Auricle ,and external auditory canal.
b. The tympanic membrane.
c. The ossicles.
d. The Eustachian tube.
e. Labyrinthine fluid.
2.Perceptive (sensory) apparatus: They convert the sound wave to
electrical nerve impulse. Consist of
a. End organ of hearing (organ's of corti).
b. Cochlear division of vestibule-cochlear N., to Auditory nuclei in brain
stem, to midbrain, to auditory cortex (superior temporal gyrus). where the
impulses perceived as sound
Classifications (Types)and causes of hearing loss:
I. Conductive Hearing loss (CHL).
(Due to external or middle ear pathology.)
I. External ear.
1.wax : The commonest cause .
2.Congenital meatal atresia.
3.Acquired meatal stenosis and atresia.
4.Foreign body.
5.Otitis externa.
6.Tumor *Benign Osteoma, exostosis, papilloma
.
**Malignant. squamous cell ca.
II. Middle ear.
1.Otitis media
*(Suppurative otitis media; acute and chronic),
**(Non-suppurative ;Otitis media with effusion, Adhesive otitis media).
2. Congenital middle ear defect (ex. fixation of footplate of stapes)
3.Otosclerosis.
4.Trauma.(perforated tympanic membrane, ossicular discontinuity,
Haemotympanium).
5.Tumor: *Glomus Tu. **squamous cell ca.
Treatment of conductive hearing loss
1*Wax removal : By probing, Suction, and ear syringing.
2*Surgical treatment, includes
a. Myringotomy with or without Grommet insertion. for Otitis
media with effusion.
b. Myringoplasty. Grafting of perforated TM.
c. Ossiculoplasty. Reconstruction of damaged ossicular chain.
d. Stapedectomy. For otosclerosis.
e. Resection of tumor: for osteoma. Glomus Tu.
f. Meatoplasty : widening of external ear canal, For meatal atresia or
stenosis.
3*Hearing Aids.
II.Sensori-neural Hearin loss (SNHL):
*Sensory : (Damage of cochlea, organs of corti) .
*Neural : (Damage of cochlear N. ,or neural pathway).
A. Congenital SNHL.
*.Waardenberg syndrome.* Pendred syndrome
*B. Acquired SNHL.
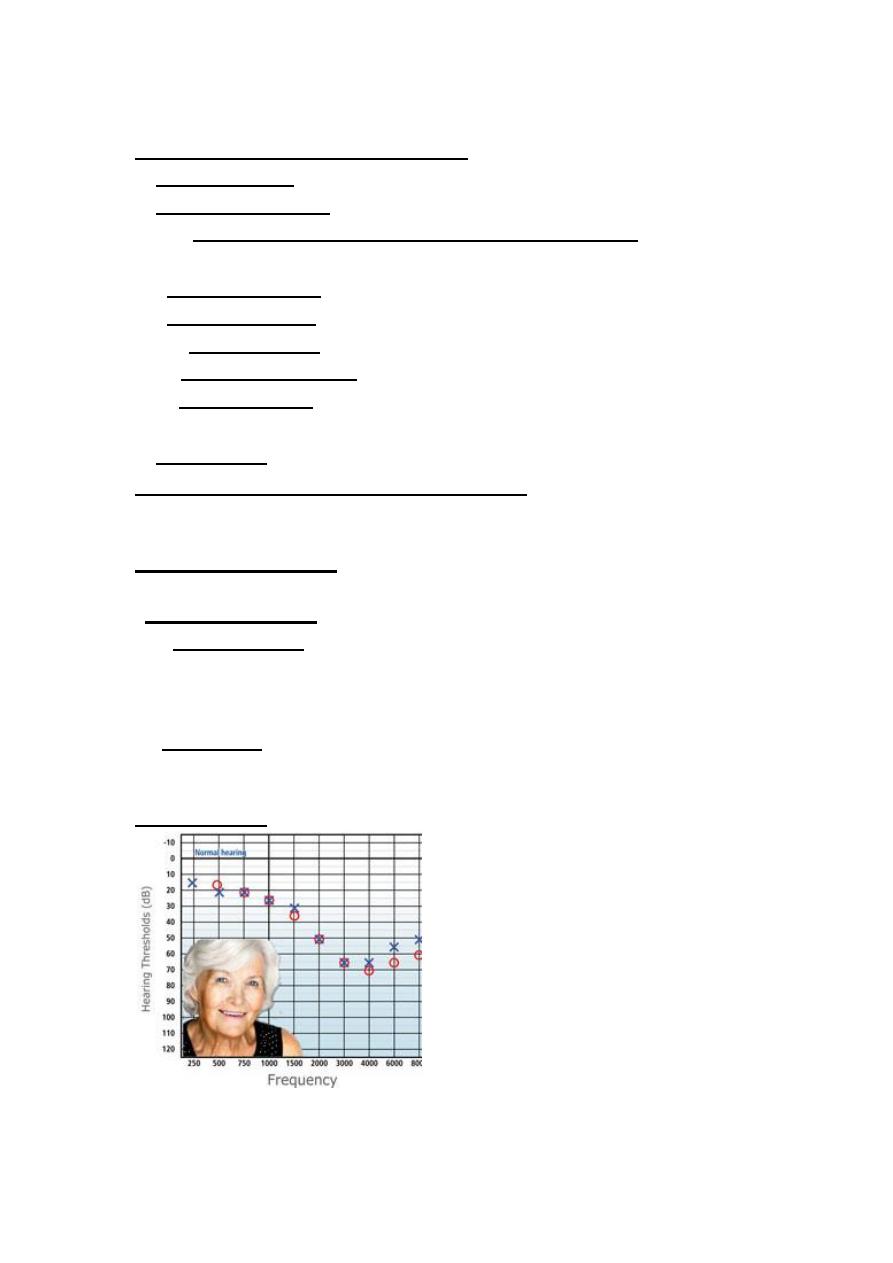
1.Presbyacusis.
Hearing loss due to degenerative changes of aging
process. started at 55-65 year .It is commonest cause of SNHL .Usually Pure
tone audiometery (PTA) shows ,bilateral symmetrical progressive high
frequency SNHL.
Risk factors;
Includes
1.Genetic susceptibility. 2.Noise exposure,
3.Metabolic and vascular diseases
.
Treatment:Hearing aids.
2.Noise-induced HL: Damage of hair cells due to exposure to load
sound.
A . Acute acoustic trauma.
Due to exposure to sudden intense sound
more than 140 dB SPL, of short duration ,commonly Gunshot, and blast injury
(explosion) ,Usually rupture of Tympanic membrane occurs
.
B.
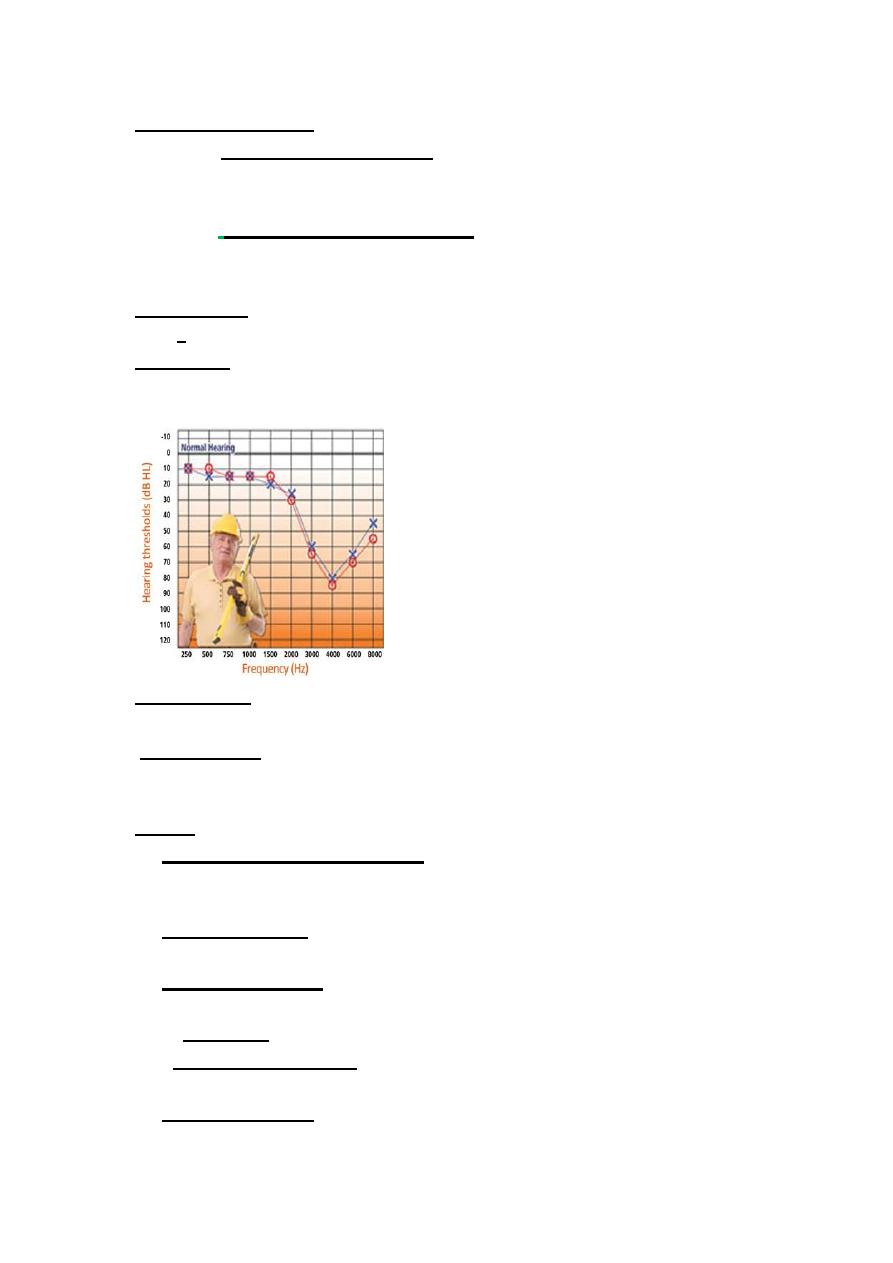
Chronic noise-induced HL:
When exposure to more than 90 dB
SPL ,for 8hr daily ,for 5 days/ in a week/ for 3months. commonly industrial
noise. cause permanent sensori-neural hearing loss and tinnitus
.
Audiogram (
PTA)show drop hearing threshold between 3-6 KHz (dip at 4
KHz), then deteriorate all frequencies involved.
Treatment :
*Prevention Using ear muff for protection .
*Hearing Aid
3.Ototoxicity: Damage to the cochlea and/or Vestibular part of inner ear
by drugs.
Rout of entry:
1.Parentral(I.V,I.M)commonly.
2.Oral.(Lasix,Chloroquine.)
3.Local (ear drops ex. Garamycin, Neomycin
Drugs.
1.Aminoglycosides antibiotic:
Garamycin& streptomycin (mainly
vestibulotoxic). Neomycin, Kanamycin, Tobramycin (mainly cochleotoxic).
Permanent SNHL.
2.Loop diuretics:
Frusemide, Bumitanide, Ethacrynic acid in high dose
(reversible high freq. SNHL)
3. Cytotoxic drug.
like Cisplatin, is cochleotoxic partially reversible on
with drawls of drug,& Cyclophosphamide.
4. Salicylate.
Aspirin in over dose causes tinnitus & flat SNHL, (reversible).
5.Antiprotozal agent.
Quinine &chloroquine, (Cochleotoxic HL,
permanent).
6.Anticonvulsant.
Phenytoinðsuximide.Vestibulotoxic (acute vertigo&
reversible.)
Treatment of Ototoxicity:
*Prevention.
1.Avoid or discontinue ototoxic drugs ,when satisfactory alternative.
2. Monitor of drug by estimate serum level of drug & serum creatinin.
3.Monitor hearing by audiogram and vestibular function (caloric test).
*Therapeutic : Hearing Aids. (no medical or surgical treatment)
4.Labyrinthitis:
Inflammation of the inner ear ( labyrinth). Clinically, vertigo
hearing loss ,Tinnitus of varying degrees and may affect one or both ears.
5.Meniere’s disease:
(Endolymphatic hydrops).
6.Acoustic neuroma:
(vestibular shwanoma). Slow growing benign tumor
,arise from shwan cells of VIII n. (commonly from vestibular nerve)
7.Trauma:
a. Transverse fracture temporal bone.
b. Iatrogenic (Ear surgery) . c. Blast injury.
8.Psychological hearing loss.
Sudden sensorineural HL
:
Is loss of 35 dB for three consecutive
frequencies within three days or less. may be unilateral, or bilateral.
Causes;
1. Vascular (Hemorrhage, thrombosis).
2.Viral infection( Mumps, rubella, Influenza virus) labyrinthitis.
3.Rissener’s membrane break. Ionic fluid imbalance from mixing perilymph
and endolymph results SNHL
Treatment.
Vasodilator (to improve cochlear circulation) like
*Inhalation of carbogen 5% Co2.
*Low molec. Weight dextran 40%
* Beta serc tab. )*Beta- histidine)
*Steroid important (prednisolon , hydrocortisone.)
Follow up by serial audiogram(Pure tone audiometry)
Prognosis.
40-70% improve, or get recovery
Bad prognosis
:*Old age *Total deafness *High frequency HL.
*Vertigo *Delay treatment
III. Mixed HL: (conductive &SNHL).
1. Advanced otosclerosis. ( cochlear otosclerosis).
2.Chronic suppurative otitis media. Due to *Absorption of toxin ,*use
of systemic & local ototoxic drugs.
3.Glomus tumor.
4.Trauma. Ex. mixed fracture temporal bone.
Treatment of Sensori-neural hearing loss.
Aim of treatment is restoration as much as possible of hearing loss. by
1. Hearing Aids.
a. Air conduction H A. b. Bone conduction HA.
c. Bone –anchored H.A d. Middle ear implantable hearing devices.
2. Cochlear implantation:
An electronic device that generates electrical stimulation of auditory
nerve directly.
Indications.For patient above 2 years of age with profound binaural
cochlear (sensory) hearing loss with relatively intact cochlear N.
with *Normal mentality and *No medical, surgical, or radiological
contraindications.
**Other means to help the deaf patient
3.Lip reading. for child with partial deafness
4.Sign language. for profound deafness.
5.Brain stem implants
Used for patient who have had both acoustic nerves destroyed.
Clinical assessment of hearing
Neonate *Startle at loud noises.
*(4-9 Mo)Turn eyes toward source of familiar sounds?
Voice test:
Whisper 30 dBHL.
Conventional voice 40-60 dBHL.
shouting voice >90 dBHL.
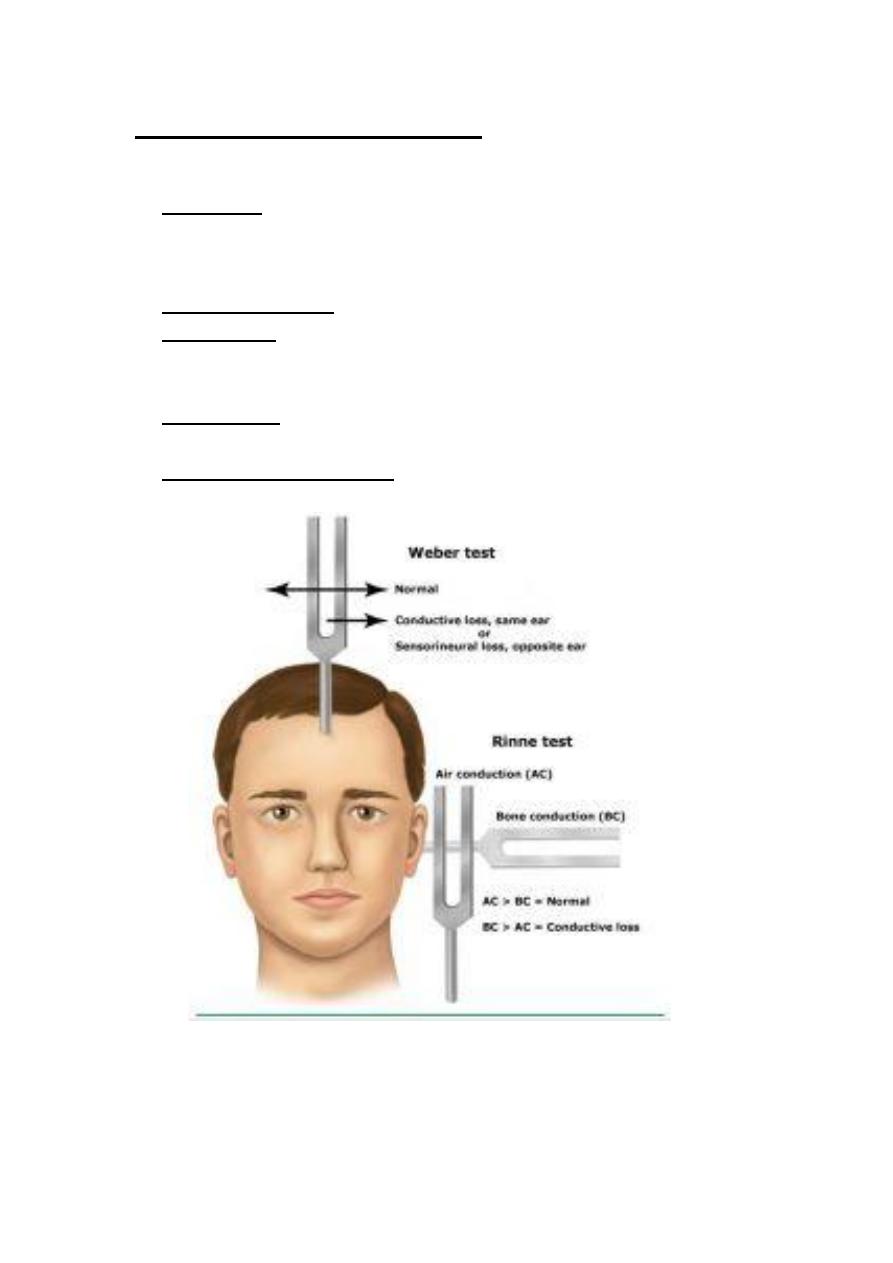
Tuning Fork Tests. usually use 512 Hz.
Renne’s test. *+ve (AC>BC).
*-ve (BC>AC).
*False Renne’s test .
Weber’s test. *Central
*Lateralized to Left, Right.
Absolute bone conduction.
* Equal . * Reduced
.
Audiological Tests
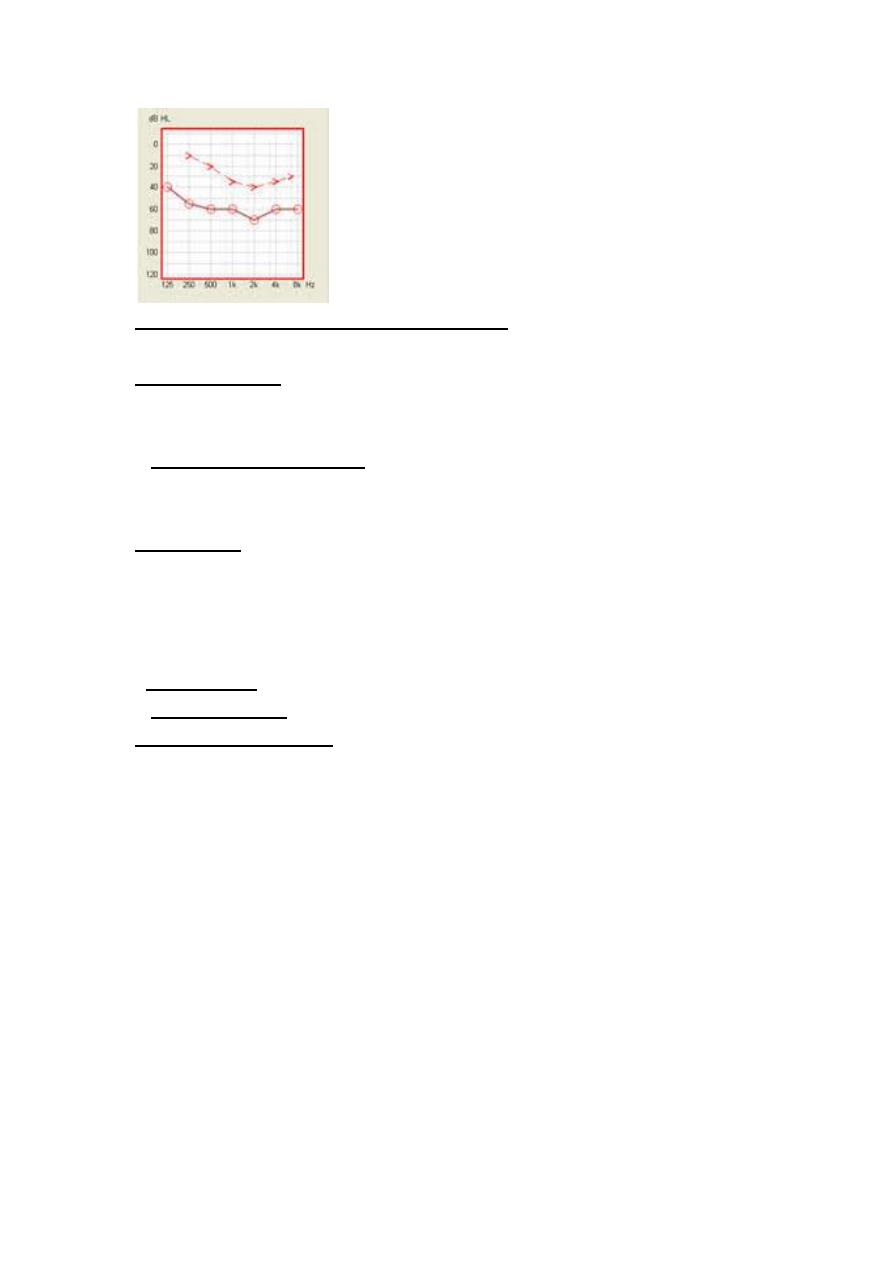
1. Pure tone audiometry.
Subjective test by electronic device for
measuring of hearing.
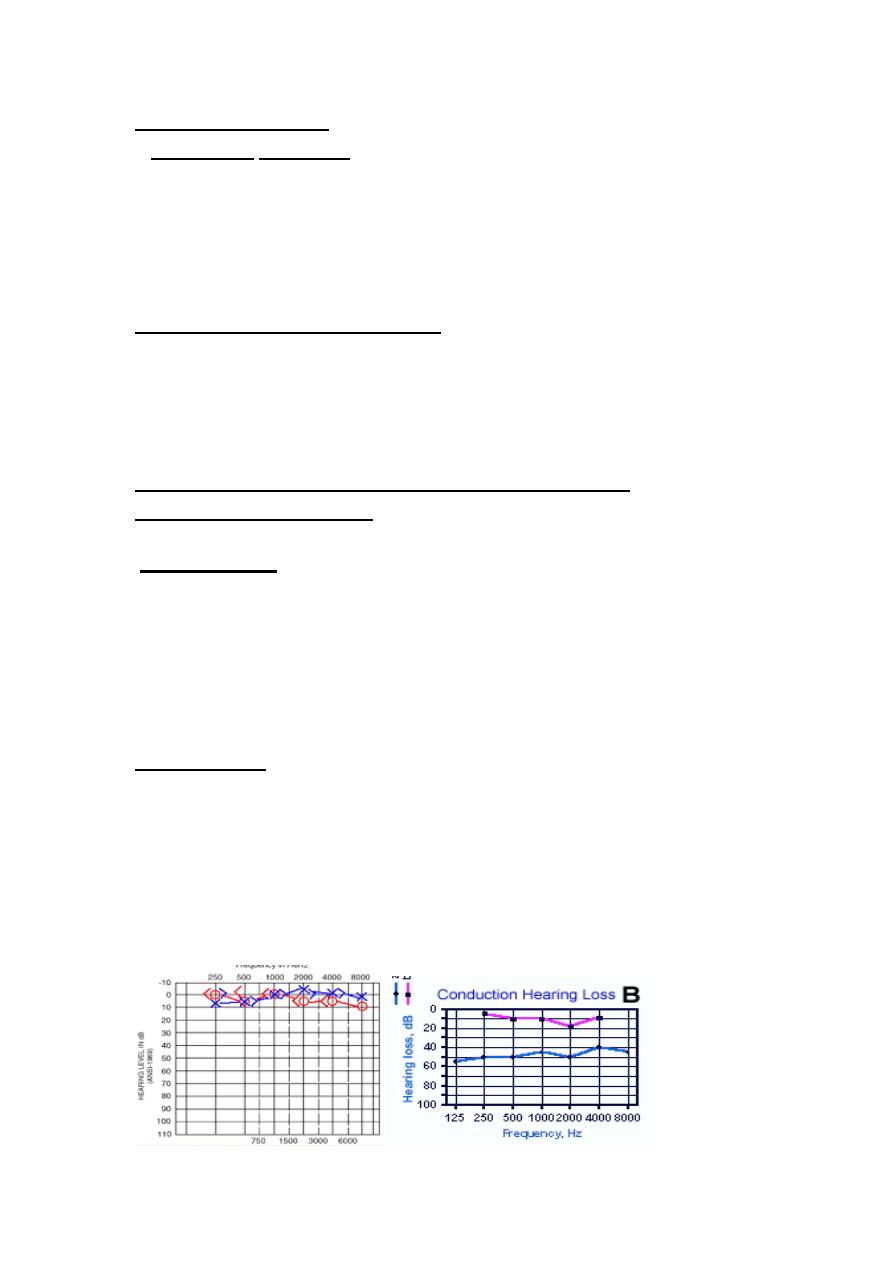
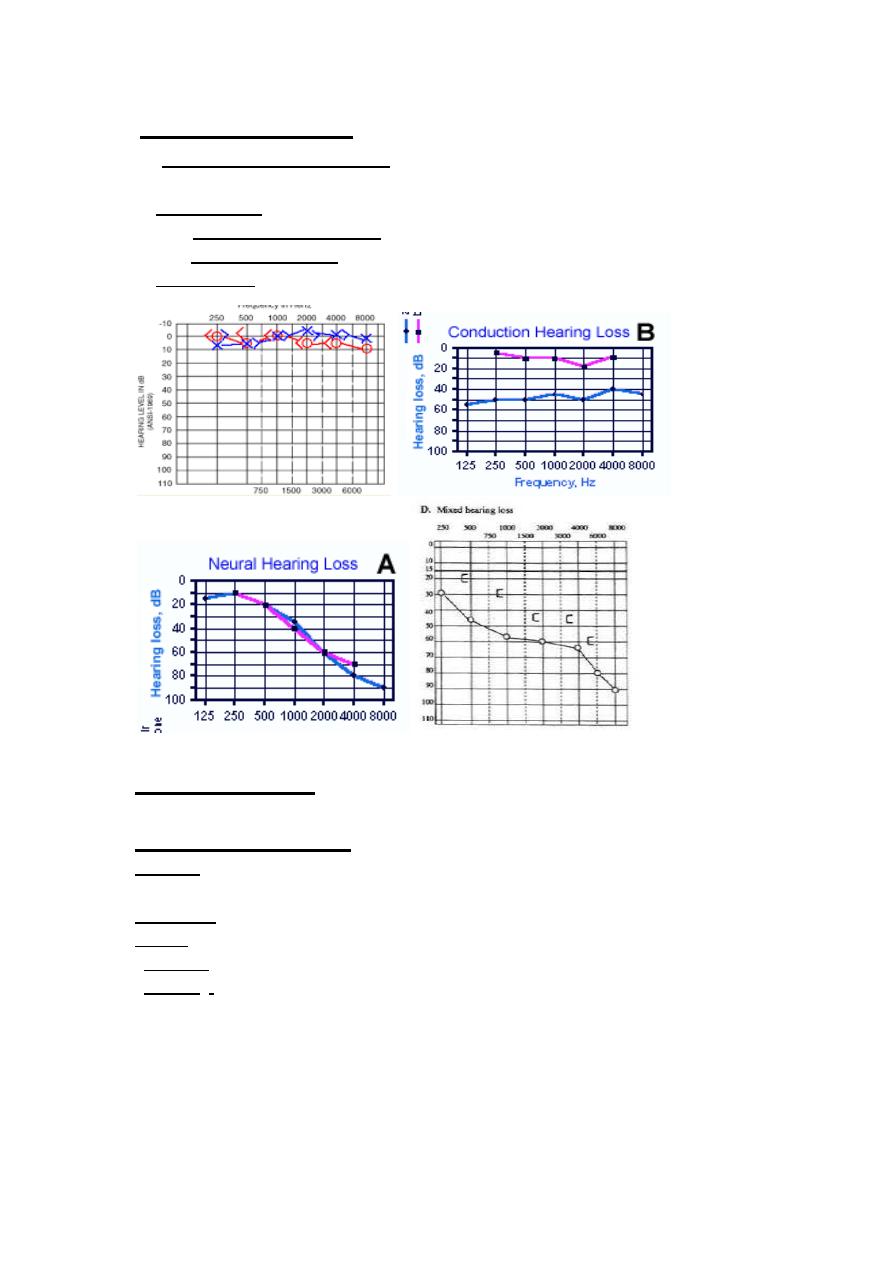
a*Normal; AC and BC are superimposed at -10_ 20 dB.
b*Conductive Hearing loss: Normal BC ,and reduce AC (A_B gap)
c*Sensory neural HL. Both BC ,and AC declined.
d*Mixed HL. Both BC ,and AC declined ,But more AC.
Tympanometry
: An objective test used for diagnosis of middle
ear disorders (conductive deafness).
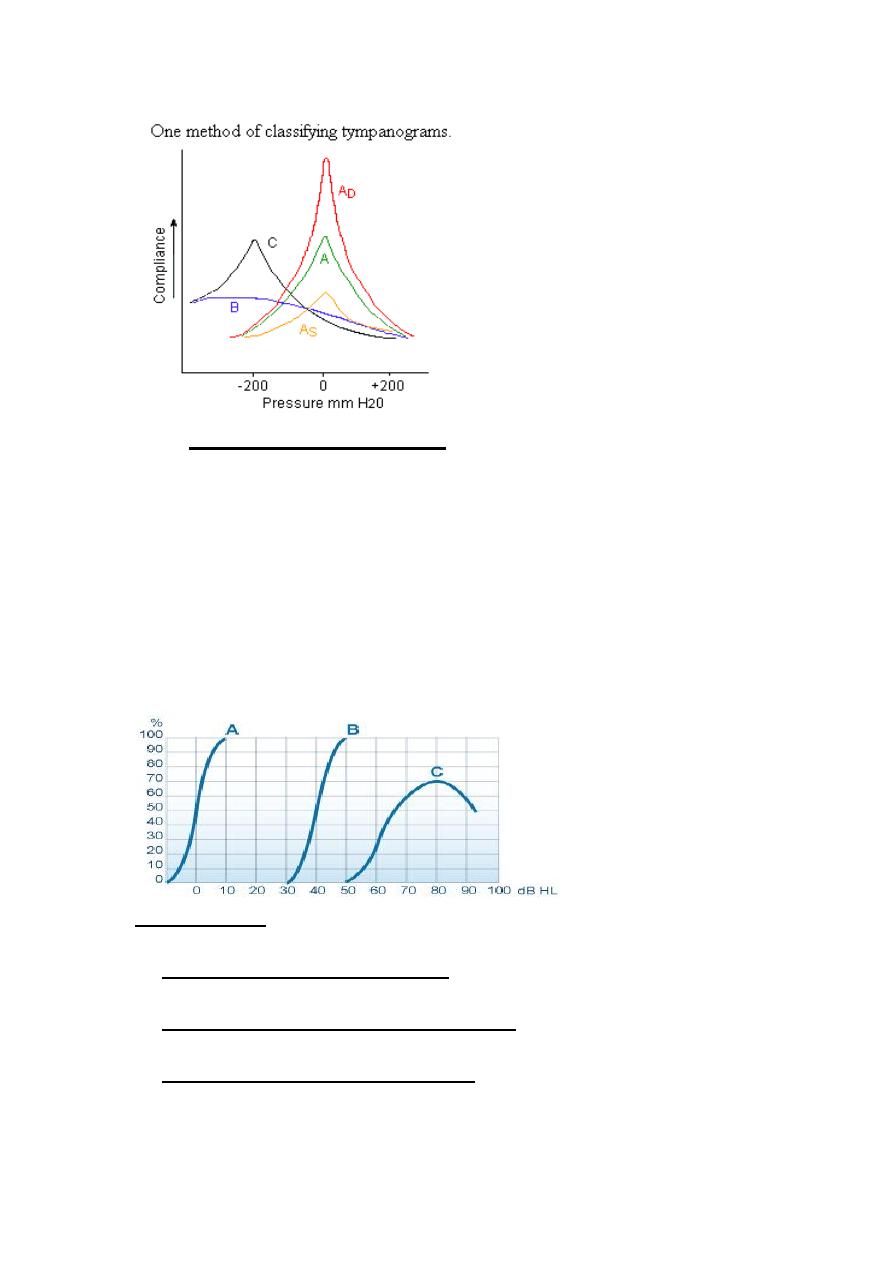
Types of tympanogram:
Type A. Normally peak at 0mm/H20 of 0.3-1.6 CC compliance.
{Normal, Sensory neural HL}.
*Type As .Shallow peak. {otosclerosis, adhesive otitis media}.
*Type Ad .deep peak {ossicular discontinuity.}
*Type B. Flat tympanogram.{ otitis media with effusion. cholesteatoma}
*Type C Negative pressure peak. (Eustachian tube dysfunction.
1.
Speech audiometry
:
Uses word recognition to asses patient ‘s
understanding of speech
Use list of words with extra number of syllables, each list may have 10-50
words usually phonetically balanced. the patient repeat each word. and the
score determined according to percentage of words that correctly identified.
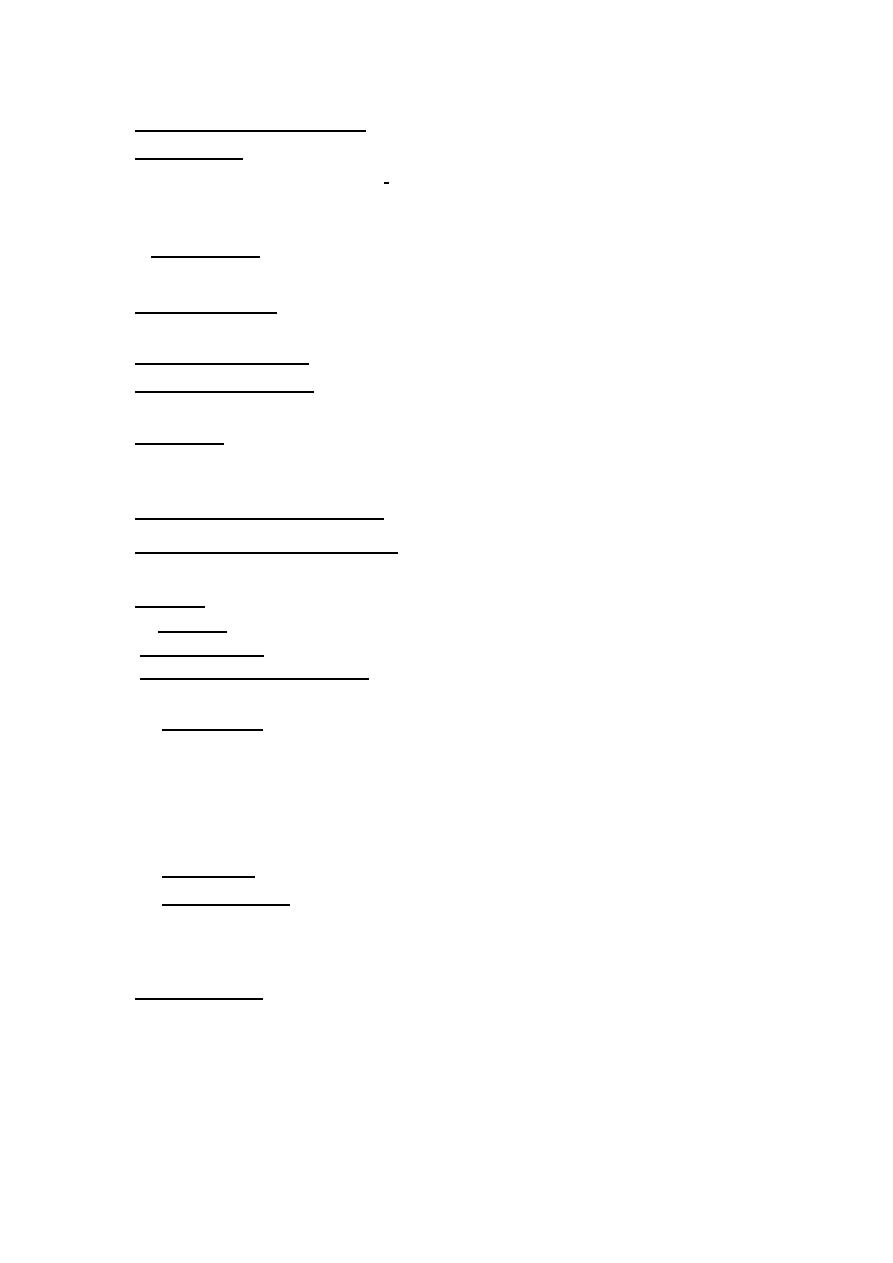
A )
) **90-100%=Excellent (normal).
# In conductive HL reach this score with magnification)
*70-90%=Good *50-70%=Fair (cochlear HL)
*30-50=poor (neural HL) *O-30%= very poor.
(A)normal,
(B)CHL ,
(C) Cochlear
Objective tests:
For sensori-neural HL. and used as screening tools for hearing
in neonates and children
1.Otoacoustic Emission (OAEs).
Objective test to measure the outer
hair cell function of organ’s of corti. use in screening.
2.Auditory Brainstem Response (ABR).
Objective test to measure
hearing sensitivity and site of lesion.
3.Electrocochleography (ECochG)