Diagnosis of dental caries

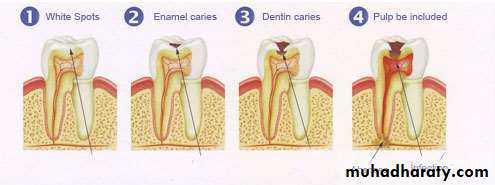
Dental caries
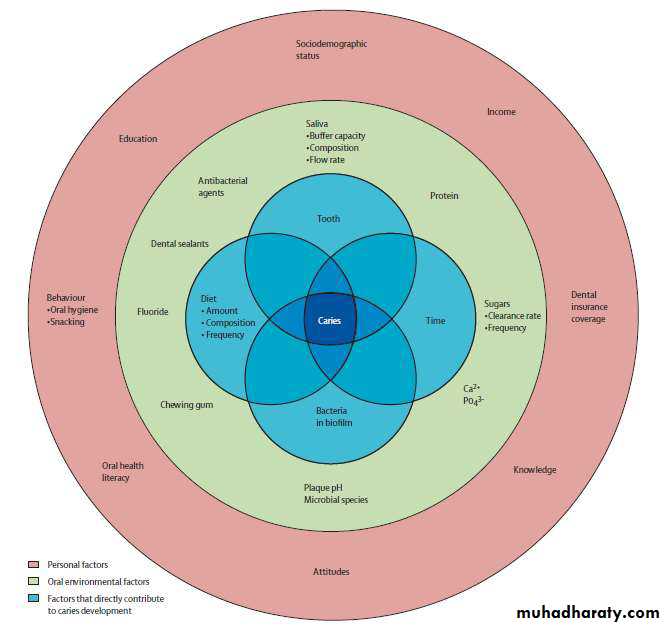
Is the localised destruction of susceptible dental hard tissues by acidic by-products from bacterial fermentation of dietary carbohydrates.(According to Shafer)
It can be defined as the microbial disease of the calcified tissues of teeth characterized by demineralization of the inorganic portion and destruction of organic substance of the tooth.
( According to WHO)
Caries is defined as a localized post eruptive, pathological process of external origin involving softening of the hard tooth tissue and proceeding to the formation of a cavity .For the WHO caries assessment system , the examiner recorded a surface as decayed only if it presented with detectably softened floor, undermined enamel or a softened wall.
According to this criterion, all the stages that precede cavitation as well as other conditions similar to the early stages of a carious lesion were considered sound.
Code Description Sound tooth : A crown is recorded as sound if it shows no evidence of treated or untreated dental caries. The stages of caries that precede cavitation as well as other conditions similar to the early stages of caries are considered sound because they cannot be reliably diagnosed.
Decayed crown Caries is recorded as present when a lesion in the pit and fissure or on a smooth tooth surface has an unmistakable cavity, undermined enamel, or a detectably softened floor or wall. Where any doubt exists, caries should not be recorded as present





The word diagnosis (plural, diagnoses) is derived from the Greek ‘‘dia’’ meaning
‘‘through’’ and ‘‘gnosis’’ meaning ‘‘knowledge’’. Thus, ‘‘to diagnose’’ implies that itis only through knowledge about the disease that a diagnosis can be established.
The examination and evaluation of carious lesions has traditionally been limited to physical criteria such as size, depth, and presence or absence of cavitation. The term for this is caries lesion detection.
The assessment of lesion activity together with lesion detection is essential to arrive at the disease diagnosis and the appropriate clinical treatment decision.
In addition to caries lesion detection, lesion or disease activity assessment must also consider etiologic factor evaluations, such as oral hygiene, count of cariogenic micro-organisms in plaque and saliva, use of fluoride, sugar intake, and also some socioeconomic aspects, such as family income and parents’ level of education.
The PRIMARY OBJECTIVE of caries diagnosis is to identify those lesions that require restorative treatment, those that require non-surgical treatment, and those persons who are at high risk for developing carious lesions.
Some decades ago, visual diagnosis (light and mirror) and probing, supplemented by bitewing radiographs were the only tools available for clinical diagnosis of caries. For epidemiologic surveys and for examination of most patients, these are still useful tools.
The traditional method of detecting caries signs is by visual inspection of dental surfaces, with the aid of a bright light and dental mirror if necessary to see teeth from all angles.
Reflecting light onto the mouth mirror also can be done to search for dark shadows that could indicate dentin lesions.
While the use of a dental probe continues to be controversial, it is extremely helpful when used correctly and judiciously. A probe is unnecessary if visual inspection detects a cavity.
CONVENTIONAL METHODS OFCARIES DETECTION
VISUAL-TACTILE METHOD
RADIOGRAPHY
CARIES DETECTING DYES
FIBEROPTIC TRANSILLUMINATION
ELECTRONIC CARIES MONITOR
Visual methods:
1. Detection of white spot, discoloration / frank cavitations• 2. Without aids, unreliable
3. Magnification loupes- Head worn prism loupes (X 4.5) or surgical microscopes(X 16) may be used
comfort, relatively inexpensive, available in various
magnification
4. Use of temporary elective tooth separation
Tactile methods:
Explorers are widely used for the detection of carious tooth structure
- Right angled probe- no.6
- Back action probe- no.17
- Shepherd's crook- no. 23
- Cow horn with curved ends- no.2

Use of explorer is not advocated because
1. Sharp tips physically damage smalllesions with intact surfaces
2. Probing can cause fracture & cavitation of
incipient lesion. It may spread the
organism in the mouth
3. Mechanical binding may be due to noncarious
Reasons:
Shape of fissure
Sharpness of explorer
Force of application
Path of explorer placement
why Use of explorer
• Explorer is useful to remove plaqueand debris and check the surface
characteristics of suspected carious
lesions.
• gentle pressure just required to blanch
a fingernail without causing any pain
or damage
• All surfaces of a tooth are cleaned of
debris and plaque, using an air
syringe and examined visually.
Suspicious areas are explored to
check for the surface texture.


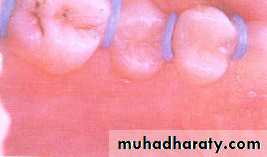
SMOOTH SURFACE CARIES
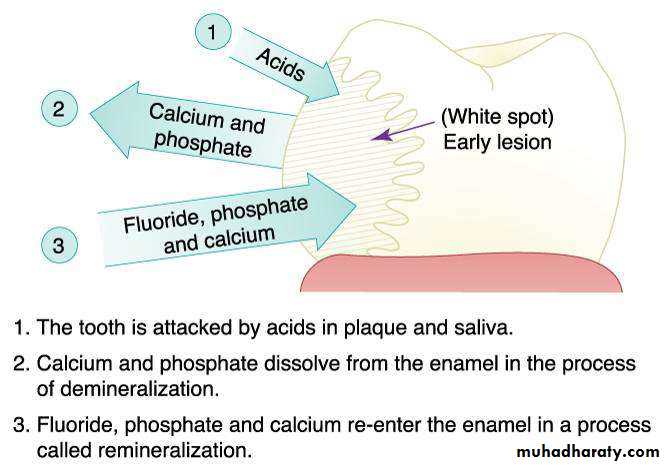
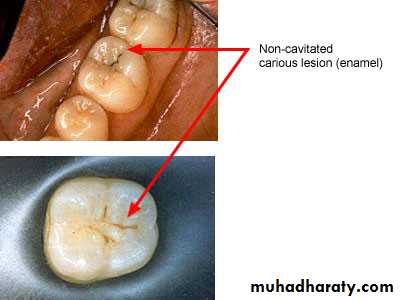
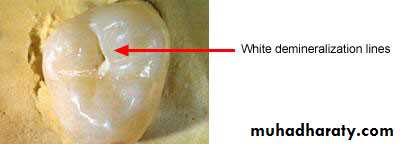
Non- cavitated:No signs of cavitation after visual or tactile examination.
Location: where dental plaque accumulates (gingival margin).
Surface characteristics: Matted (not glossy) when a tooth is dried.

Non-cavitated carious lesion


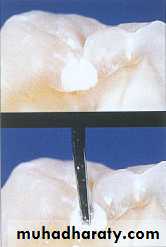
Cavitated Lesions:
Where there is visual breakdown of a tooth surface, it is classified as cavitated carious lesion. An active cavity on a smooth surface has soft walls or floors shown below: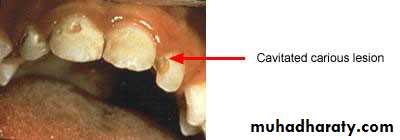
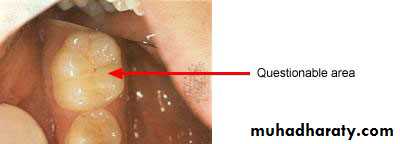
Questionable Area:
All stained smooth coronal tooth surfaces that do not have the characteristics of non-cavitated or cavitated lesions are classified as questionable shown below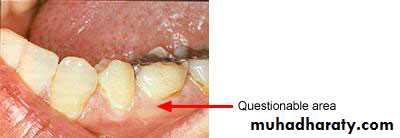
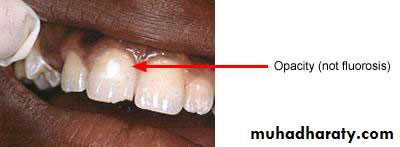
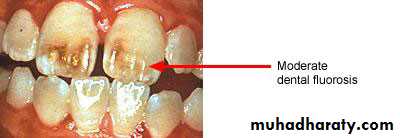
Non-Carious Enamel Opacities


Caries in Pit or Fissure Surfaces
• 1. All discolored areas should be explored using gentle• pressure.
• 2. There is no need to penetrate a suspected lesion with an explorer.
• 3. If a discolored and non-cavitated area is soft when explored, it is recorded as non-cavitated carious pit or fissure.
• 4. A cavity is detected when there is an actual hole in the
• tooth in which an explorer could easily enter the space.
• 5 . An active cavity has soft walls or floors (detected using
gentle exploring).
6. If there is visual enamel opacity under an ostensibly sound or stained pit or fissure, then the enamel is undermined because of dental caries and the tooth surface is classified with a non-cavitated carious lesion in dentin.
Pit and Fissure CariesNon-cavitated carious lesion
Enamel

Dentin
If a discolored area is hard when gently explored then it should be marked as questionable.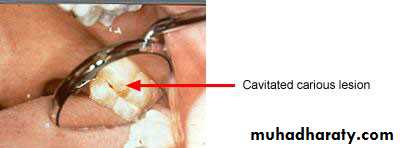
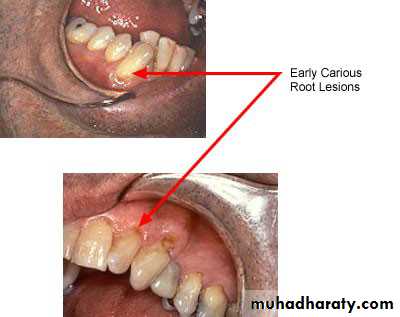
Root Caries
• Root surface caries comprises of a continuum ofchanges ranging from minute discolored areas to
cavitation that may extend into the pulp
For diagnostic purpose; they may be:
Active root surface lesion:
• well-defined area showing yellowish or light brown
discoloration
• covered by visible plaque
• presence of softening/ leathery consistency on
probing with moderate pressure
Inactive root surface lesion (arrested):
• well-defined dark brown/ black discoloration
• smooth and shiny• hard on probing with moderate pressure
Active lesion

Questionable
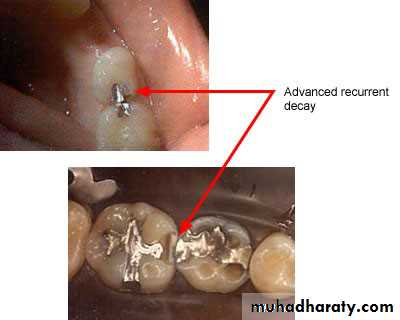
Recurrent cariesIt is diagnosed whenever there is softness due
to caries at a defective margin, and when the tip
of a periodontal probe can enter the defect
without any resistance.
A restoration with a discolored margin or a small
marginal ditch (<0.5 mm or the head of the
probe) is recorded as an early recurrent
carious area. A larger defect should be
classified as advanced recurrent carious area
There are two valid indicators of recurrent (secondary) caries:
• softness at the margin of a filling that is detectedusing an explorer or
• presence of a large defect (a minimum diameter of
0.4 mm) at a margin of a filling with softness in the
area.
Large defects are associated with a high level of colonization with cariogenic bacteria.
Marginal discoloration by itself is not a valid sign for
dental caries.
Nursing bottle caries Vs Rampant caries
Specific form of rampant caries Acute, widespread caries withearly pulpal involvement of
teeth that are usually immune to
decay
Primary dentition affected Both dentitions affected
C/F: specific pattern- maxillary
incisor ®molars
Mandibular incisors not affected
Rapid appearance of new lesionsMandibular incisors also
affected


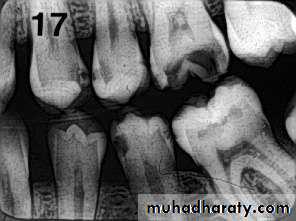
RADIOGRAPHY
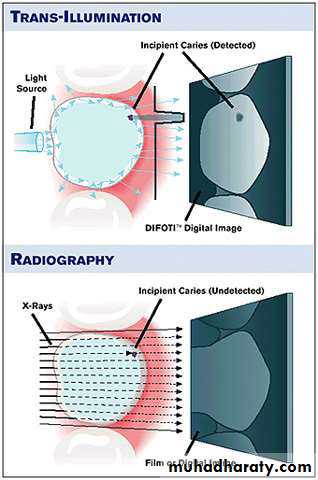
Carious lesions are detectable radio graphically when there has been enough demineralization to allow it to be differentiate from normal.They are valuable in detecting proximal caries which may go undetected during clinical examination.
On average they have around 50% to 70% sensitivity in detecting carious lesions.
40% demineralization is required for definitive decision on caries
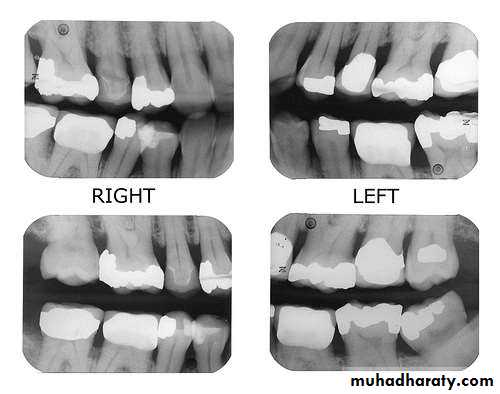
Radiographic examinations include;
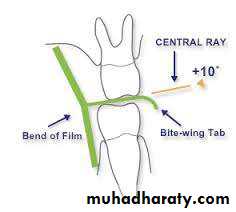
• Bitewing radiographs• IOPA radiographs using paralleling technique
• Dental panoramic tomograph
The two important decisions related to radiographic examination are
• when to take a radiograph and
• how to evaluate a radiograph for presence of signs of dental caries.
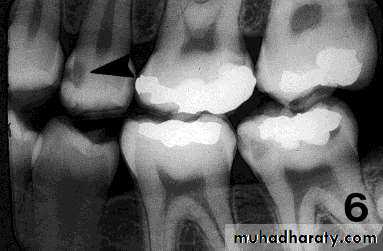
PIT & FISSURE CARIES
Incipient occlusal lesions:Not very effective.
Caries starts on the walls
of the pits & fissures and
tends to spread
perpendicular to the DEJ
Only detectable change is
a fine gray shadow at the
DEJ.

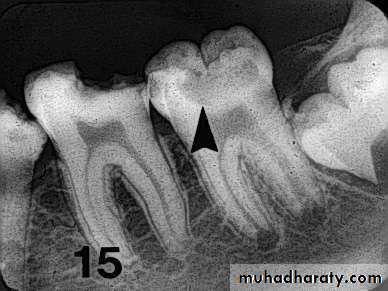
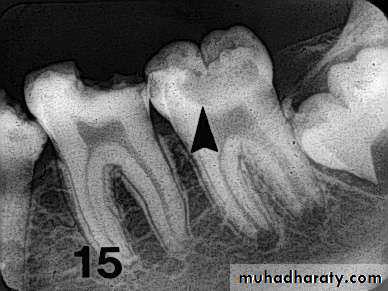
Moderate occlusal lesions:
Moderate occlusal lesions: First to induce specific changes
helping in a definitive diagnosis
Broad based, thin radiolucent
zone in dentin with minimal or
no changes in enamel
Presence of a band of increased
opacity between the lesion and
the pulp chamber due to
calcification within primary
dentin
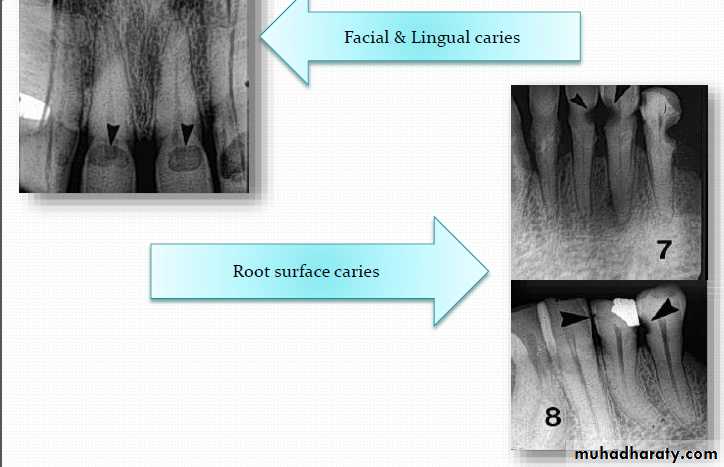
This feature is not seen in
buccal caries
Severe occlusal lesions:
Readily observed bothclinically and
radiographically
Appear as large cavities in
the crowns of the teeth
However pulp exposure
cannot be determined


Incipient occlusal lesions

Incipient occlusal lesions
Moderate occlusal lesionsSevere occlusal lesions


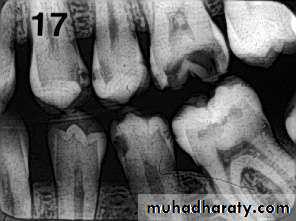
Advanced proximal lesions
Incipient proximal lesionsModerate proximal lesions
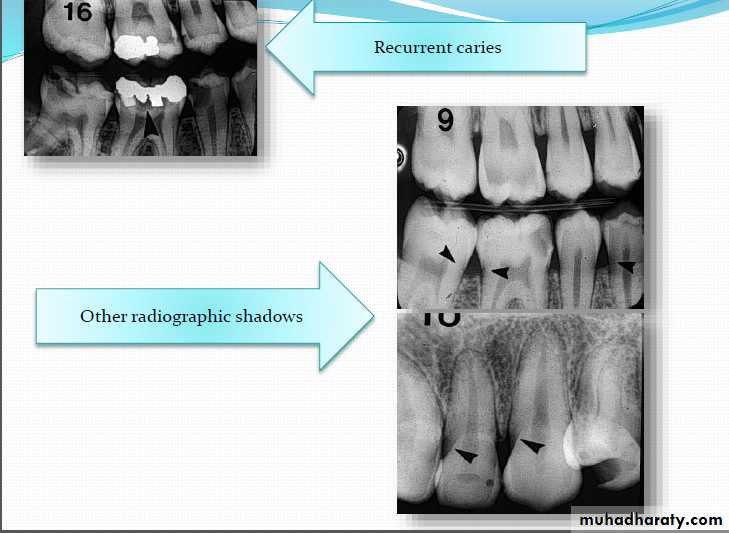
OTHER RADIOGRAPHIC SHADOWS
Radiolucent Cervical Burn out:- Evident at the neck of tooth
well demarcated above by
enamel cap& below by alveolar
bone level
- It is triangular in shape
being less apparent at the center
of tooth
-good alveolar bone height
will enhance cervical burn-out
Radiopaque zone beneath amalgam restorations
dentinTin & zinc ions are released into underlying
Newer Methods of Caries Detection and Assessment

DIGITAL IMAGING
A digital image is an image formed & represented by a spatially distributed set of discrete sensors & pixels2 types of non- film receptors
Direct digital imaging – digital image receptor
Indirect digital imaging – video camera for forming digital images of a radiograph
Two types of detectors are used in Direct digital imaging
Photostimulable phosphor ( PSP) –barium fluorohalide
Charged couple device (CCD) – silicon
Image is stored on a computer


Advantages:
1.Images are available in seconds2. Exposure is reduced 50-90%
3. Image size, contrast and density can be manipulated to
improve interpretation
4. Record keeping is vastly improved. All films are labeled,
filed and retrieved easily. Duplicate hard copies are the
same as originals and simple to make
5. Provision of teletransmission
COMPUTER IMAGE ANALYSIS
Software supports an operation where by a threshold isset up by the examiner which determines the program’s
display of lesion probability
the tomosynthesis of structures in 3D thereby increasing
the accurate detection of caries
Useful for monitoring carious lesion
Increased sensitivity but decreased specificity

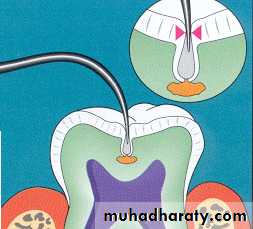
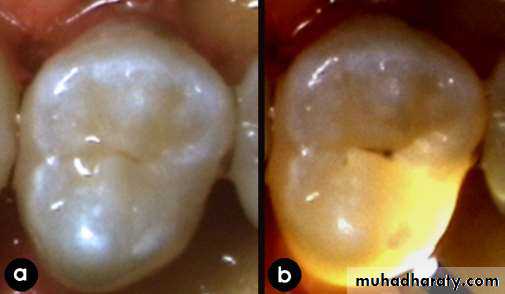
Fiber-optic transillumination
This effect can be achieved with a fiber optic illuminator, which is readily available at the handpiece coupler of the dental operatory and has been used for detection ofapproximal and occlusal caries.
Posterior approximal caries can be diagnosed with the light probe positioned on the gingivae below the cervical margin of the tooth, whereby the light passes through the tooth structures and approximal decay produces a dark shadow on the occlusal surface.
Although this device has the advantage that the examination is done with an operating light source already available in general practice, it is only useful for approximal and occlusal lesions; its sensitivity and specificity are not sufficient for detection of very early caries. Besides, it is not quantitative and therefore not useful as a caries monitor over time. However, studies on the diagnostic efficacy of this device present conflicting results.

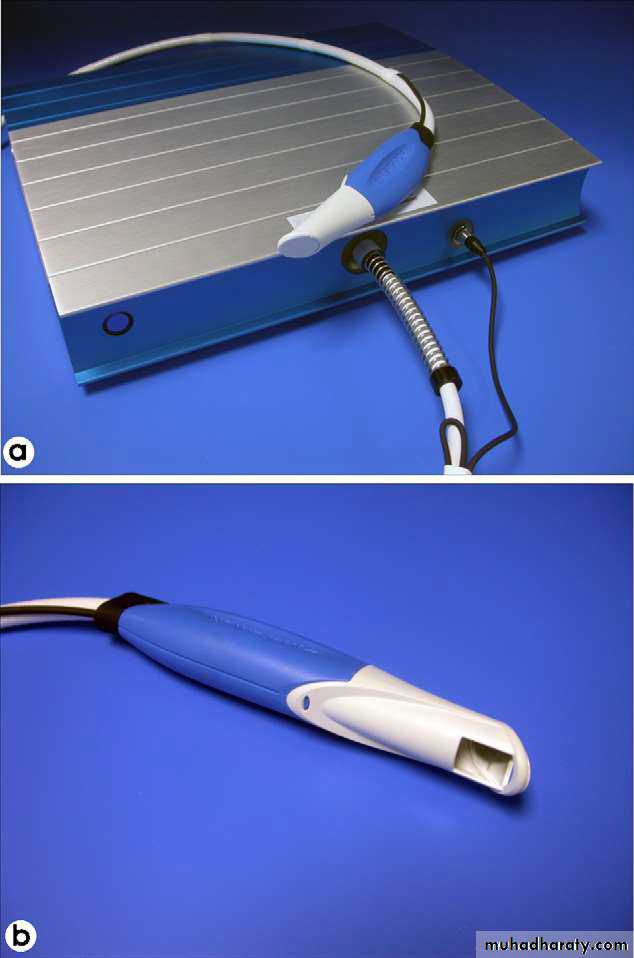
Digital imaging fiber-optic transillumination
FOTI was designed for detection of approximal and occlusal caries, digital imaging fiber-optic transillumination DIFOTI is used for detection of both incipient and frank caries in all tooth surfaces.DIFOTI can also be used to detect fractures, cracks, and secondary caries around restorations.
Digital Fiberoptic Transillumination
is a relatively new method of detecting Dental Caries with modern technology. In this technique of detecting Dental Caries, there is make the use of fiberoptic light for detecting caries and the image can be seen with the help of digital camera attached to it.
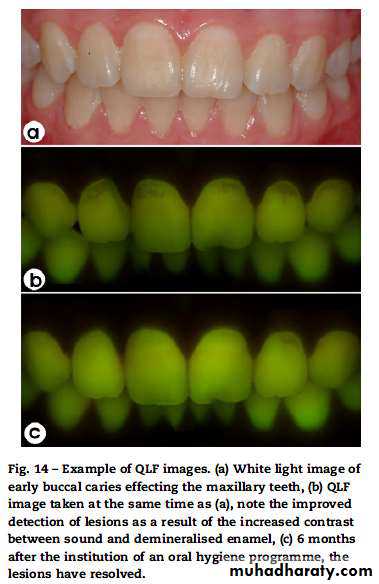
Quantitative Light-induced Fluorescence
Another dental diagnostic tool for detection of early carious lesions is quantitative light-induced fluorescence (QLF), which is based on auto-fluorescence of teeth.When the teeth are illuminated with high intensity blue light, the resultant autofluorescence of enamel is detected by an intraoral camera which produces a fluorescent image.
The emitted fluorescence has a direct relationship with the mineral content of the enamel.
Laser fluorescence—DIAGNODent
The DIAGNODent (DD) instrument (KaVo, Germany) is another device employing fluorescence to detect the presence of caries.
Using a small laser the system produces an excitation wavelength of 655 nm which produces a red light. This is carried to one of two intra-oral tips; one designed for pits
and fissures, and the other for smooth surfaces.
Unlike the QLF system, the DD does not produce an image of the tooth; instead it displays a numerical value on two LED displays.

DIAGNODent pen
Due to this limitation, a new version of the method was designed and introduced, named DIAGNOdent pen. This new version permits the assessment of both occlusal and proximal surfaces.

FIBEROPTIC TRANSILLUMINATION
Different index of light transmission fordecayed & sound tooth. Decayed tooth
structure has decreased index &
appears dark


Factors affecting electrical measurements
1. Porosity2. Surface area
3. Thickness of the tissues
4. Hydration of enamel
5. Temperature
6. Concentrations of ions in the dental tissue
fluids