
Anxiety disorders د.وليد عزيز العميدي
Anxiety is a state associated with intense feelings of dread accompanied by somatic complaints
that indicate a hyperactive autonomic nervous system such as palpitations and sweating. Anxiety
is a state that has many effects . it influences the cognition and tends to produce distortion of
perception . it is differentiated from fear which is an appropriate response to a known threat ;
anxiety is a response to a threat that is unknown and vague .
Classification of anxiety disorders :
- Generalized anxiety disorder.
- Panic disorder.
- Agoraphobia.
- Specific phobia.
- Social anxiety disorder or social phobia.
- Anxiety due to another general medical condition.
- Substance/Medication-Induced Anxiety Disorder.
- Separation Anxiety Disorder.
- Selective Mutism.
Biology of anxiety : the following neurotransmitter systems are involved in anxiety :
Noradrenaline : this neurotransmitter is closely related to the central and peripheral effects of
anxiety .drugs that enhance its release (yohimbine) lead to an increase in anxiety , where as drugs
which reduce its release (clonidine) decrease anxiety levels.
Serotonin (5HT) : a reduction in the levels of 5HT .
GABA : is extremely widely dispersed throughout the brain and it acts as an inhibitory
neurotransmitter . when GABA receptors are blocked , symptoms of anxiety appear , whereas
stimulation of the action of GABA leads to a reduction in anxiety .
It is unlikely that any one neurotransmitter is responsible for all the changes seen in the anxiety
disorders , but a number of pathways interact to develop the symptoms.
Symptoms of anxiety :
1- Psychological arousal : fearful anticipation , irritability , sensitivity to noise , restlessness
, poor concentration and worrying thoughts.
2- Autonomic arousal : GIT ( dry mouth , difficulty in swallowing , epigastric discomfort ,
frequent or loose motions ) , respiratory (constriction in the chest , difficulty inhaling ) ,
CVS ( palpitations ) , GUS ( frequent or urgent micturition , failure of erection ,
menestural discomfort , amenorrhoea ).
3- Muscle tension : tremor , headache , aching muscles.
4- Hyperventilation : dizziness , tingling in the extremities , feeling of breathlessness.
5- Sleep disturbance : insomnia , night terror.
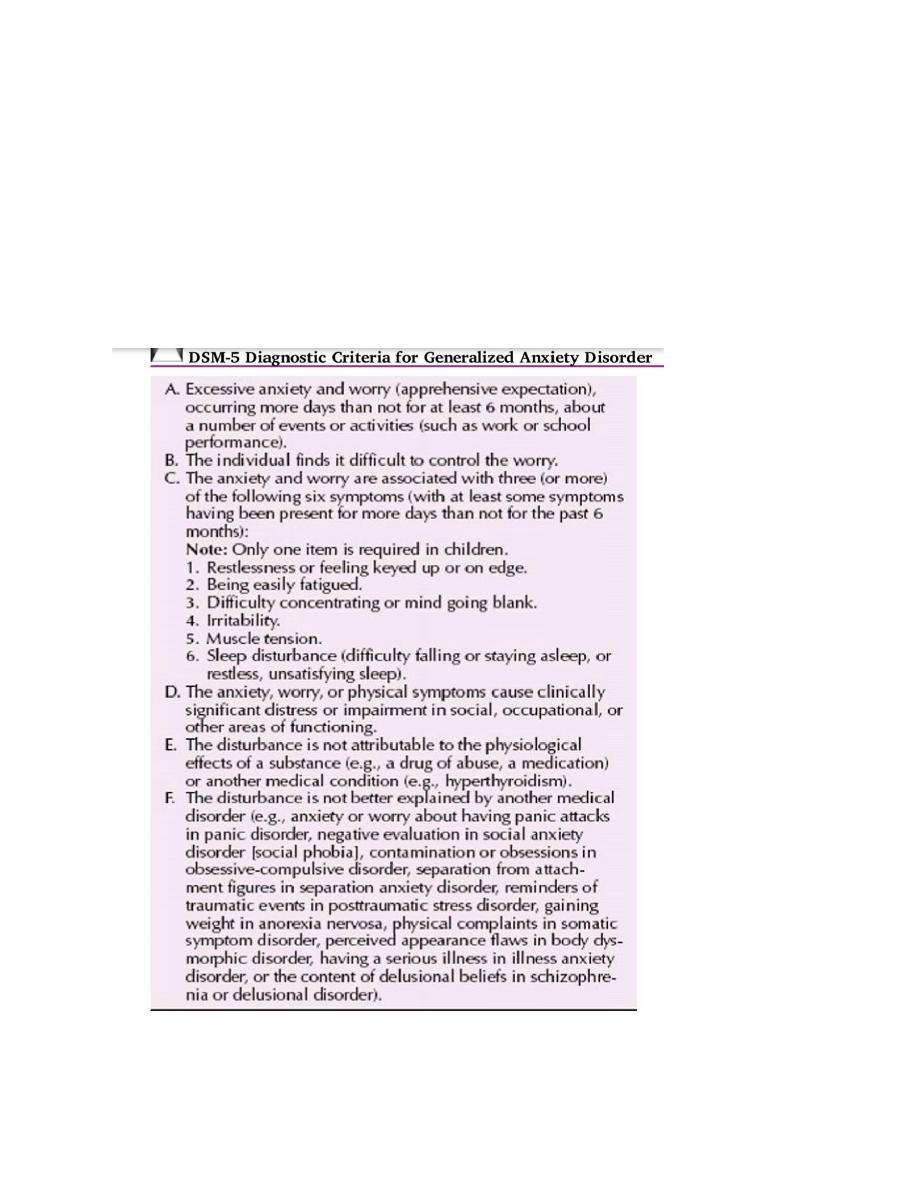
Generalized anxiety disorder : Generalized anxiety disorder is defined as excessive anxiety
and worry about several events or activities for most days during at least a 6-month period. The
worry is difficult to control and is associated with somatic symptoms, such as muscle tension,
irritability, difficulty sleeping, and restlessness. The anxiety is not focused on features of another
disorder, is not caused by substance use or a general medical condition, and does not occur
only during a mood or psychiatric disorder. The anxiety is difficult to control, is subjectively
distressing, and produces impairment in important areas of a person’s life.
Clinical signs : the face appears strained , the brow is furrowed , and the posture is tense . the
person is restless and may tremble . the skin is pale and sweating is common , especially from
hands , feet and axillae .

Epidmeology : life time prevalence 3 – 8 % of population , M/F = 1/2 , age of onset variable but
usually early adulthood.
Treatment : psychological : The most effective treatment of generalized anxiety disorder is
probably one that combines psychotherapeutic, pharmacotherapeutic, and supportive approaches
. The major psychotherapeutic approaches to generalized anxiety disorder are cognitive-
behavioral, supportive, and insight oriented.
Pharmacological treatment : - short term treatment : longer acting benzodiazepines is appropriate
for short term treatment of GAD .e.g. diazepam in a dose from 5mg twice daily in mild cases to
10mg three times a day in the most severe . anxiolytic drugs should seldom prescribed for more
than 3 weeks because of the risk of dependence when given for longer .buspirone is similarly
effective for short term management of GAD and less likely to cause dependence , but has
slower onset of action . Beta adrenergic antagonist are sometimes used to control anxiety
associated with severe palpitations that have not reponded to other treatment .
- Long term treatment : both tricyclic and specific serotonin reuptake inhibitors can be
used for this purpose . antipsychotics given in low doses can also be employed but their
use is usually restricted to anxiety in people with aggressive personalities or people who
have become dependant on other drugs.
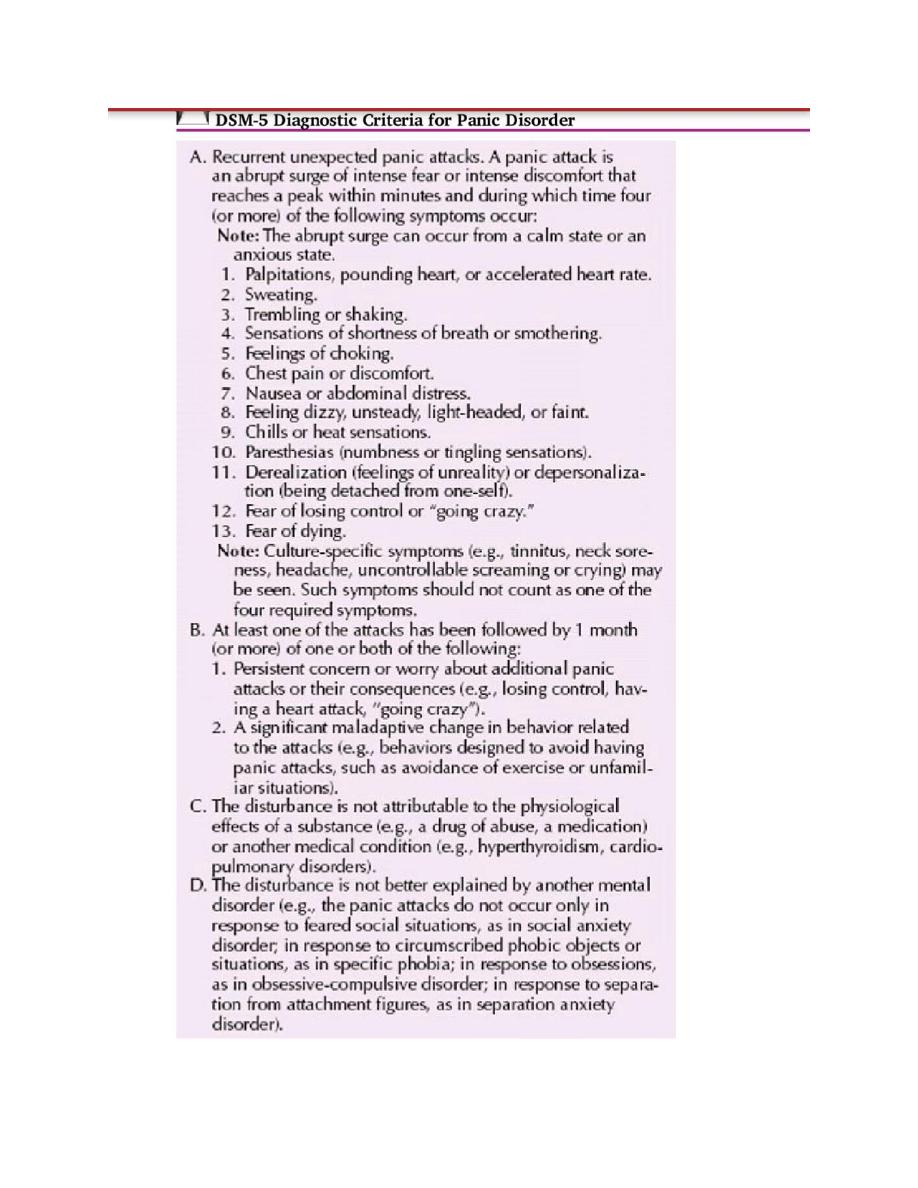
Panic disorder : An acute intense attack of anxiety accompanied by feelings of impending
doom is known as panic disorder. The anxiety is characterized by discrete periods of intense fear
that can vary from several attacks during one day to only a few attacks during a year. Patients
with panic disorder present with a number of comorbid conditions, most commonly agoraphobia,
which refers to a fear of or anxiety regarding places from which escape might be difficult.
Important features of panic attacks :
- Anxiety builds up quickly.
- The symptoms are severe .
- The person fears a catastrophic outcome.
About 20% of patients with panic attacks may also display agoraphobia.
Panic disorder is about twice as frequent among women as among men.

Aetiological theories : - Genetic : first degree relatives of those with panic disorder have a 5
times greater likelihood than members of general population of developing the disorder.
- Biochemical : panic attacks can be easily induced in this group by yohimbine , and this
suggests an abnormality of noradreneric receptors ,also it can be induced by sodium
lactate , flumazenil and cholecystokinin while panic attacks can be reduced by
imipramine which affects both 5HT and noradrenergic systems.
- Hyperventilation : some people can induce panic attacks by hyperventilation .
spontaneous attacks are believed to arise from involuntary hyperventilation.
- Cognitive :, concerns about physical illness are more common in anxious patients who
experience panic attacks than in those who do not . this suggests are spiraling effect in
which anxiety leads to physical symptoms which lead to anxiety , which leads to physical
symptoms , which lead to anxiety…..
Treatment : Drug treatment : treatment with benzodiazepines ( Alprazolam) is the most rapid
form of short term relief for panic disorder. All SSRIs are effective for panic disorder. Paroxetine
has sedative effects and tend to calm patients immediately, which leads to greater compliance
and less discontinuation, but this must be weighed against its weight gain potential. Citalopram,
escitalopram , fluvoxamine, and sertraline are the next best tolerated. At the present time, SSRIs
are considered the first-line agents for the treatment of panic disorder. Data, however, show that
among tricyclic drugs, clomipramine and imipramine (Tofranil) are the most effective in the
treatment of panic disorder. Cognitive behavioral treatment : breaking the spiraling thought
patterns of the person is the aim here , by learning to control the symptoms and reattribute them
so that the panic does not develop .
Phobic anxiety disorders : The symptoms of phobic anxiety disorder are the same as those of
generalized anxiety disorders , but there are three distinguishing features :
1- Anxiety in particular circumstances only .
2- Avoidance of circumstances that provoke anxiety.
3- Anticipatory anxiety when there is the prospect of encountering such circumstances.
The circumstances that provoke anxiety include situations such as crowded places , living
things such as spiders and natural phenomena such as thunder.
Phobic disorders are classified in three groups : simple phobia , social phobia and
agoraphobia.
Agoraphobia : Agoraphobia refers to a fear of or anxiety regarding places from which escape
might be difficult. It can be the most disabling of the phobias because it can significantly
interfere with a person’s ability to function in work and social situations outside the home.
When away from home or in crowds the person develops anxiety symptoms , often with a fear
that something awful will happen to them . This fear can develop following an episode of anxiety
in a public place. Afterwards , the possibility that the attacks might occur is sufficient to develop
the anxiety (anticipatory anxiety). Many situations provoke anxiety and avoidance , but there are
three common themes of distance from home , crowding and confinement . the situations include
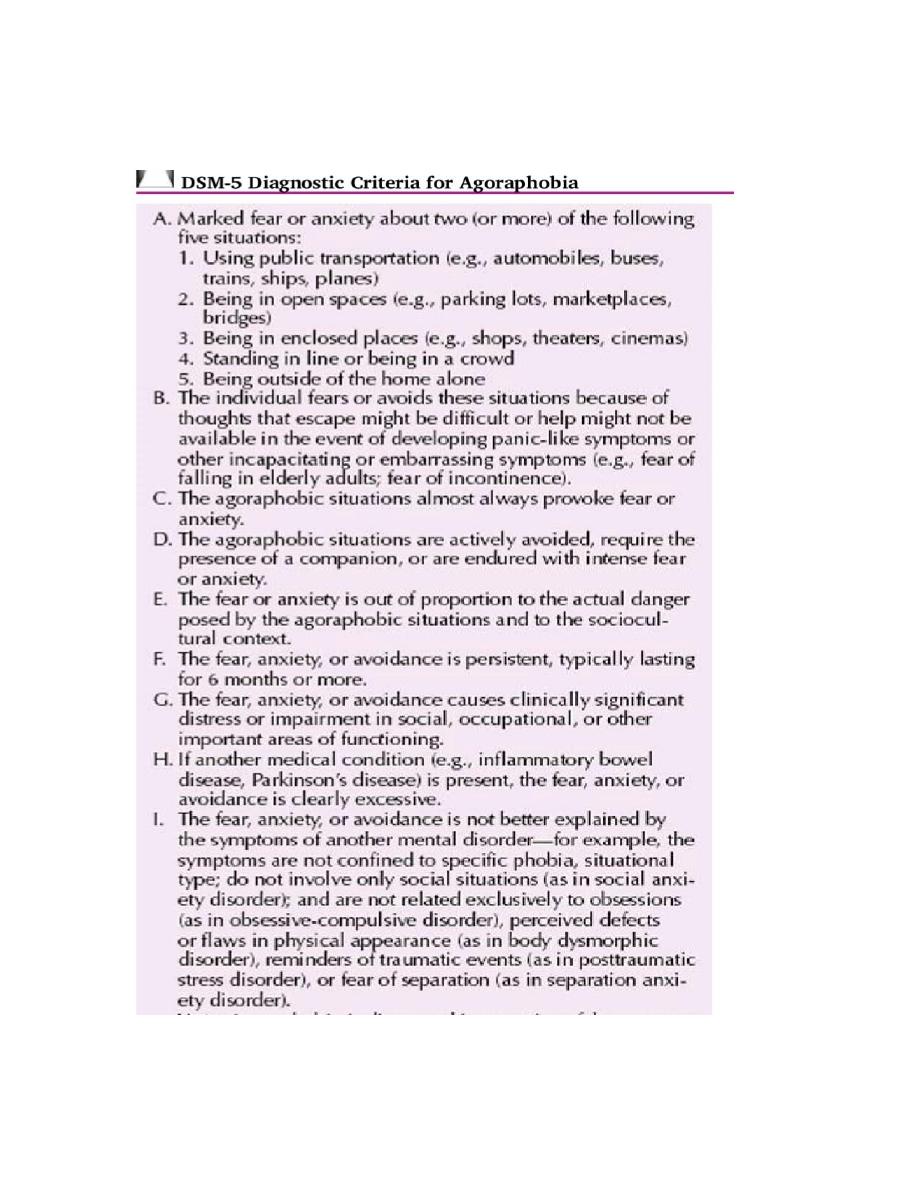
buses and trains , shops and supermarkets. The symptoms usually develop in the person`s
twenties or thirties and it is more common in women than men.

Aetiology : The development of anticipatory anxiety and avoidance after the first panic attack
can be understood in terms of conditioning. The agoraphobia is maintained by avoidance ,which
prevents deconditioning , and by apprehensive thoughts such as fear of fainting or social
embarrassment which set up vicious circles of anxiety.
Treatment :
Pharmacotherapy
:
Benzodiazepines : Alprazolam (Xanax) and lorazepam (Ativan) are the most commonly
prescribed benzodiazepines. Clonazepam has also been shown to be effective.
Selective Serotonin Reuptake Inhibitors. SSRIs have been shown to help reduce or prevent
relapse from various forms of anxiety, including agoraphobia.
Tricyclic and Tetracyclic Drugs
: clomipramine (Anafranil) and imipramine (Tofranil) are the most
effective in the treatment of these disorders. Dosages must be titrated slowly upward to avoid
overstimulation (e.g., “jitteriness” syndrome), and the full clinical benefit requires full dosages
and may not be achieved for 8 to 12 weeks.
Psychotherapy
:
Supportive Psychotherapy. Supportive psychotherapy involves the use of psychodynamic
concepts and a therapeutic alliance to promote adaptive coping
Insight-Oriented Psychotherapy. In insight-oriented psychotherapy, the goal is to increase the
patient’s development of insight into psychological conflicts that, if unresolved, can manifest as
symptomatic behavior.
Behavior Therapy. . Techniques include positive and negative reinforcement, systematic
desensitization, flooding, implosion, graded exposure, response prevention, stop thought,
relaxation techniques, panic control therapy, self-monitoring, and hypnosis.
Cognitive Therapy. This is based on the premise that maladaptive behavior is secondary to
distortions in how people perceive themselves and in how other perceive them.
Virtual Therapy. Computer programs have been developed that allow patients to see
themselves as avatars who are then placed in open or crowded spaces (e.g., a supermarket). As
they identify with the avatars in repeated computer sessions, they are able to master their
anxiety through deconditioning
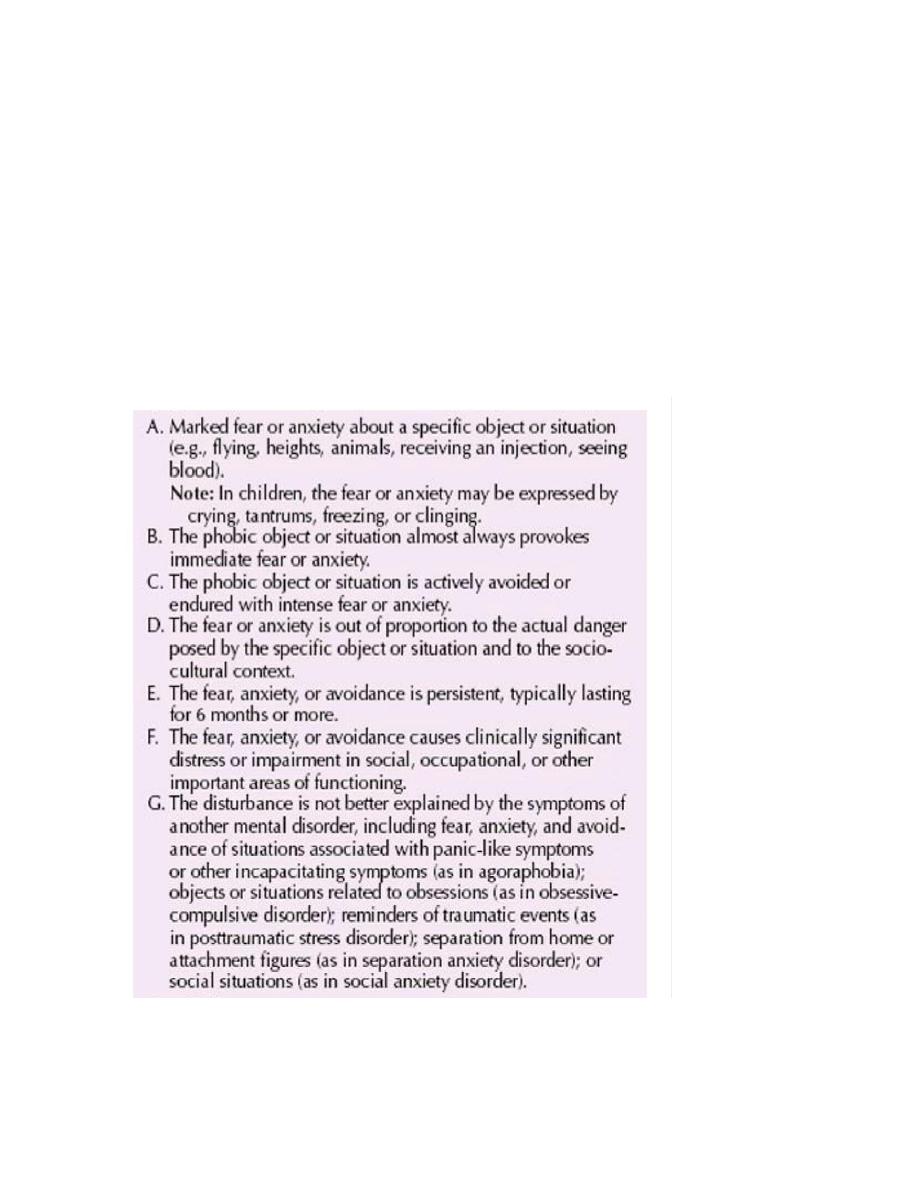
Specific phobia : The term phobia refers to an excessive fear of a specific object, circumstance,
or situation. A specific phobia is a strong, persisting fear of an object or situation. The diagnosis
of specific phobia requires the development of intense anxiety, even to the point of panic, when
exposed to the feared object. Persons with specific phobias may anticipate harm, such as being
bitten by a dog, or may panic at the thought of losing control; for instance, if they fear being in
an elevator, they may also worry about fainting after the door closes.
The lifetime prevalence of specific phobia is about 10 percent. Specific phobia is the most
common mental disorder among women and the second most common among men, second only
to substance-related disorders.
The DSM-5 includes distinctive types of specific phobia: animal type, natural environment type
(e.g., storms), blood-injection-injury type (e.g., needles), situational type (e.g., cars, elevators,
planes), and other type (for specific phobias that do not �t into the previous four types).
The key feature of each type of phobia is that fear symptoms occur only in the presence of a
specific object . The blood injection- injury type is differentiated from the others in that
bradycardia and hypotension often follow the initial tachycardia that is common to all phobias.
The blood-injection-injury type of specific phobia is particularly likely to affect many members
and generations of a family. One type of phobia of recently reported phobia is space phobia, in
which persons fear falling when there is no nearby support, such as a wall or a chair. Some data
indicate that affected persons may have abnormal right hemisphere function, possibly resulting
in visual spatial impairment. Balance disorders should be ruled out in such patients.
DSM-V criteria of specific phobia :
Treatment : A common treatment for specific phobia is exposure therapy. In this method,
therapists desensitize patients by using a series of gradual, self-paced exposures to the phobic
stimuli, and they teach patients various techniques to deal with anxiety, including relaxation,

breathing control, and cognitive approaches. The cognitive-behavioral approaches include
reinforcing the realization that the phobic situation is, in fact, safe.
In systemic desensitization the patient is exposed serially to a predetermined list of anxiety-
provoking stimuli graded in a hierarchy from the least to the most frightening.
In imaginal
flooding, patients are exposed to the phobic stimulus for as long as they can tolerate the fear until
they reach a point at which they can no longer feel it. Flooding (also known as implosion) in
vivo requires patients to experience similar anxiety through exposure to the actual phobic
stimulus
.
β-adrenergic receptor antagonists may be useful in the treatment of specific phobia,
especially when the phobia is associated with panic attacks. Benzodiazepines may also be of
benefit.
Social phobia : Social anxiety disorder (also referred to as social phobia) involves the fear of
social situations, including situations that involve scrutiny or contact with strangers. Persons with
social anxiety disorder are fearful of embarrassing themselves in social situations (i.e., social
gatherings, oral presentations, meeting new people). They may have specific fears about
performing specific activities such as eating or speaking in front of others, or they may
experience a vague, nonspecific fear of “embarrassing oneself.” In either case, the fear in social
anxiety disorder is of the embarrassment that may occur in the situation, not of the situation
itself.
Various studies have reported a lifetime prevalence ranging from 3 to 13 percent for social
anxiety disorder , females are affected more often than males , The peak age of onset for social
anxiety disorder is in the teens, although onset is common as young as 5 years of age and as old
as 35 years.
ETIOLOGY
:
Several studies have reported that some children possibly have a trait characterized by a
consistent pattern of behavioral inhibition. This trait may be particularly common in the children
of parents who are affected with panic disorder, and it may develop into severe shyness as
the children grow older. First-degree relatives of persons with social anxiety disorder are about
three times more likely to be affected with social anxiety disorder than are first-degree relatives
of those without mental disorders.
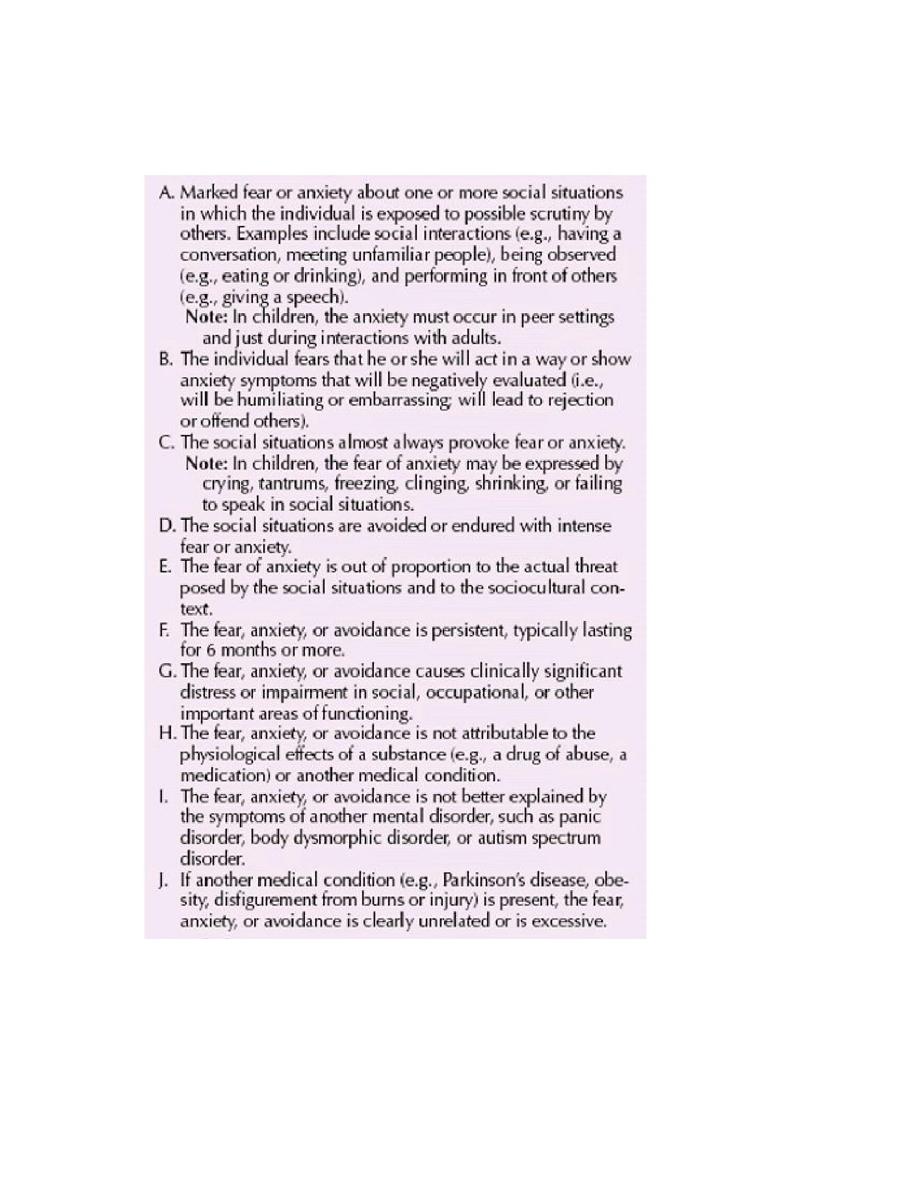
DSM-5 Diagnostic Criteria for Social Anxiety Disorder

Treatment :
Psychological treatment :
- Cognitive behavior therapy : is the psychological treatment of choice for social phobia,
combines exposure to feared situations with procedures to reduce the patient`s anxiety provoking
thoughts.
- Relaxation training : given alone appears to be ineffective for social phobia.
- Dynamic psychotherapy : may help some patients particularly those whose social phobia
is associated with pre-existing problems in personal relationships.
Drug treatments : SSRIs are often the first choice ( paroxetine , fluvoxamine and sertraline ) the
onset of action may take up 6 weeks , medication is usually continued for 9 months to a year.
Benzodiazepines can be used for short term relief of symptoms but should not be prescribed for
long because of the risk of dependancy . Beta-adrenergic blockers such as atenolol may achieve
short-term control of tremor and palpitations , which can be the most handicapping symptoms of
specific social phobias such as performance anxiety.
ANXIETY DISORDER ATTRIBUTABLE TO ANOTHER MEDICAL CONDITION
Many medical disorders are associated with anxiety. Symptoms can include panic attacks,
generalized anxiety, and other signs of distress. In all cases, the signs and symptoms will be due
to the direct physiological effects of the medical condition.
Etiology
: Hyperthyroidism, hypothyroidism, hypoparathyroidism, and vitamin B12 deficiency
are frequently associated with anxiety symptoms. A pheochromocytoma produces epinephrine,
which can cause paroxysmal episodes of anxiety symptoms. Other medical conditions, such as
cardiac arrhythmia, can produce physiological symptoms of panic disorder. Hypoglycemia can
also mimic the symptoms of an anxiety disorder. The diverse medical conditions that can cause
symptoms of anxiety disorder may do so through a common mechanism that involves both the
noradrenergic system and the serotonergic system. Each of these conditions is characterized by
prominent anxiety that arises as the direct result of some underlying physiological perturbation
.
SUBSTANCE-INDUCED ANXIETY DISORDER :
A wide range of substances can cause symptoms of anxiety that can mimic any of the DSM-5
anxiety disorders. Although sympathomimetics, such as amphetamine, cocaine, and caffeine,
have been most associated with the production of anxiety disorder symptoms, many
serotonergic drugs (e.g., LSD and MDMA) can also cause both acute and chronic anxiety
syndromes in users. A wide range of prescription medications is also associated with the
production of anxiety disorder symptoms in susceptible persons.
Diagnosis
The diagnostic criteria for substance-induced anxiety disorder require the presence of prominent
anxiety or panic attacks. The DSM-5 guidelines state that the symptoms should have developed
during the use of the substance or within 1 month of the cessation of substance use; however,
clinicians may have difficulty determining the relation between substance exposure and anxiety
symptoms.
