1
Injuries of lower limbs د.عادل الهنداوي
Injuries of the hip &femur
Dislocation of the hip:
according to the position of head of
femur relative to the acetabulum, it can be: posterior, anterior or
central(with acetabulum #).
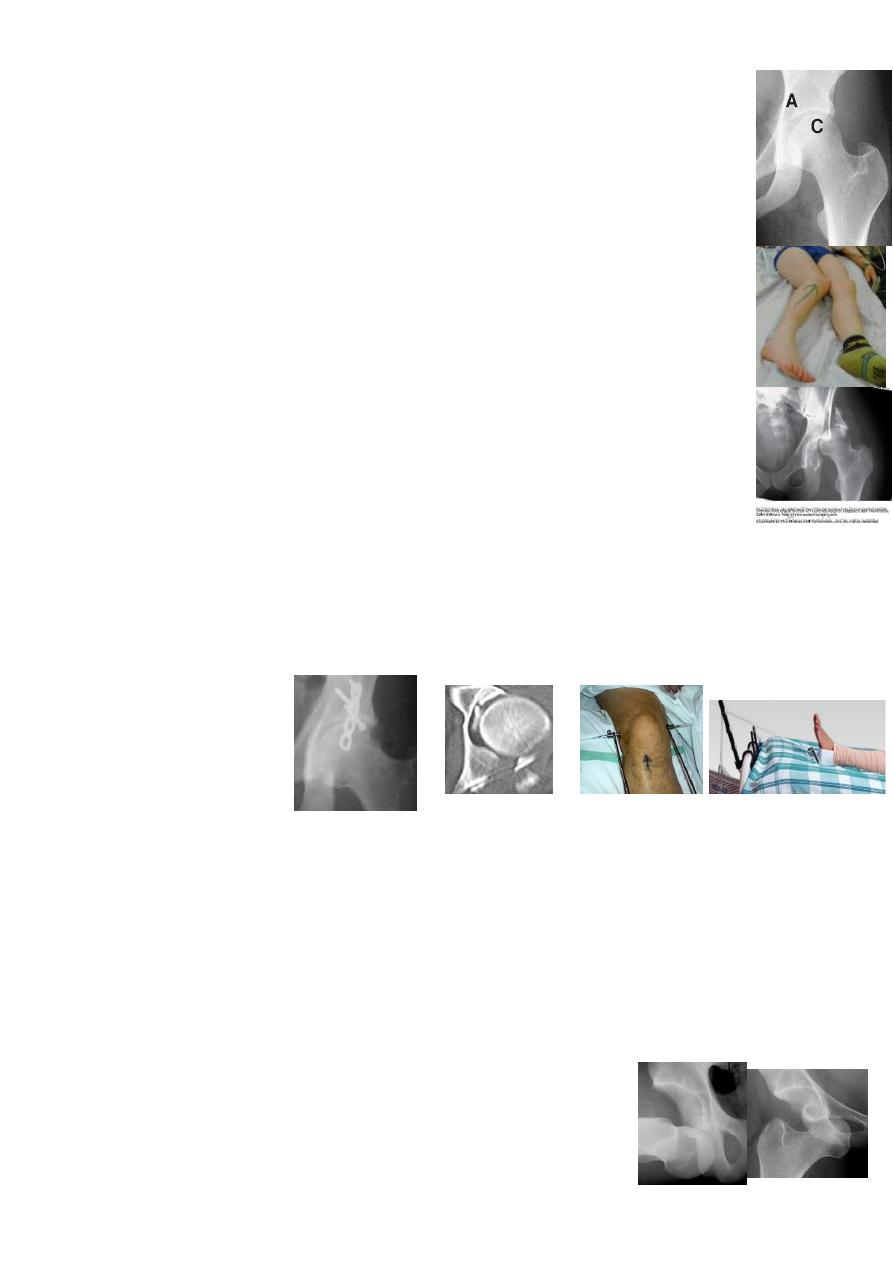
Posterior dislocation: is the commonest.
MOI: usually dashboard injury to the knee with hip flexed &adducted; if
abducted, there is in addition a # of the posterior acetabular wall(hip #-≠).
CF: the leg is short, adducted, internally rotated &flexed(unless the
femur is #). The sciatic nerve may be injured.
X-ray: AP view: the femoral head is out of &above the acetabulum. If
any # is suspected, CT scan is needed.
Treatment: urgent closed reduction UGA: apply leg traction while
flexing the hip &knee (90˚) then increase the upward traction with hip
internal &external rotation; if reduction is successful, you will feel a
'clunk'. Checking x-ray is essential to confirm reduction &to exclude a #.
If the dislocation associated with acetabular fracture: 3-6weeks traction→
3weeks crutches. if the post reduction CT shows a trapped bone fragment
inside the joint or a still displaced large bone segment (which may ↓ hip
stability), then surgery is indicated: to remove or fix the bone fragment.
Complications: early: 1-sciatic nerve injury; 2-vascular injury(rare);
3-associated femoral shaft #(the ≠ may be missed).
Late: 1-avascular necrosis: the incidence is 10%; if reduction is delayed
few hours, it increases to 40%. X-ray: ↑ femoral head density(seen after
the 6
th
week or later up to 2years).
2-myositis ossificans. 3-unreduced ≠: after few weeks, needs open
reduction. 4-Osteoarthritis: due to: a- cartilage damage; b- retained bone
fragment in the joint; c-avascular necrosis.
Anterior dislocation: is rare.
MOI: RTA or FFH.
CF: the leg is abducted, externally rotated &flexed.
X-ray: the head is in front of acetabulum & either superior
(over pubis or ilium) or inferior(over obturator foramen).
2
Treatment: the same as posterior ≠.
Complication: 1-in superior type, the head may press on the femoral
neurovascular bundle; 2-avascular necrosis is less common(<10%).
Central dislocation:
MOI: fall on the side.
CF: the leg is in normal position.
X-ray: the femoral head is pushed medially with acetabular floor#.
Treatment: 12weeks skeletal traction, sometime combined with
lateral traction in the greater trochanter.surgical fixation for acetabulum
may indicated
Fractures of the femoral neck:
common in old osteoporotics.
Risk factors: 1-weak bone due to: osteoporosis, osteomalacia, DM, CVA
(disuse), alcoholism &chronic diseases; 2-old ages who have
weak muscles &poor balance with ↑ tendency to fall.
MOI: in elderly, simple trauma: catching toe in a carpet or fall
on greater trochanter; in youngs, severe trauma: RTA or FFH.
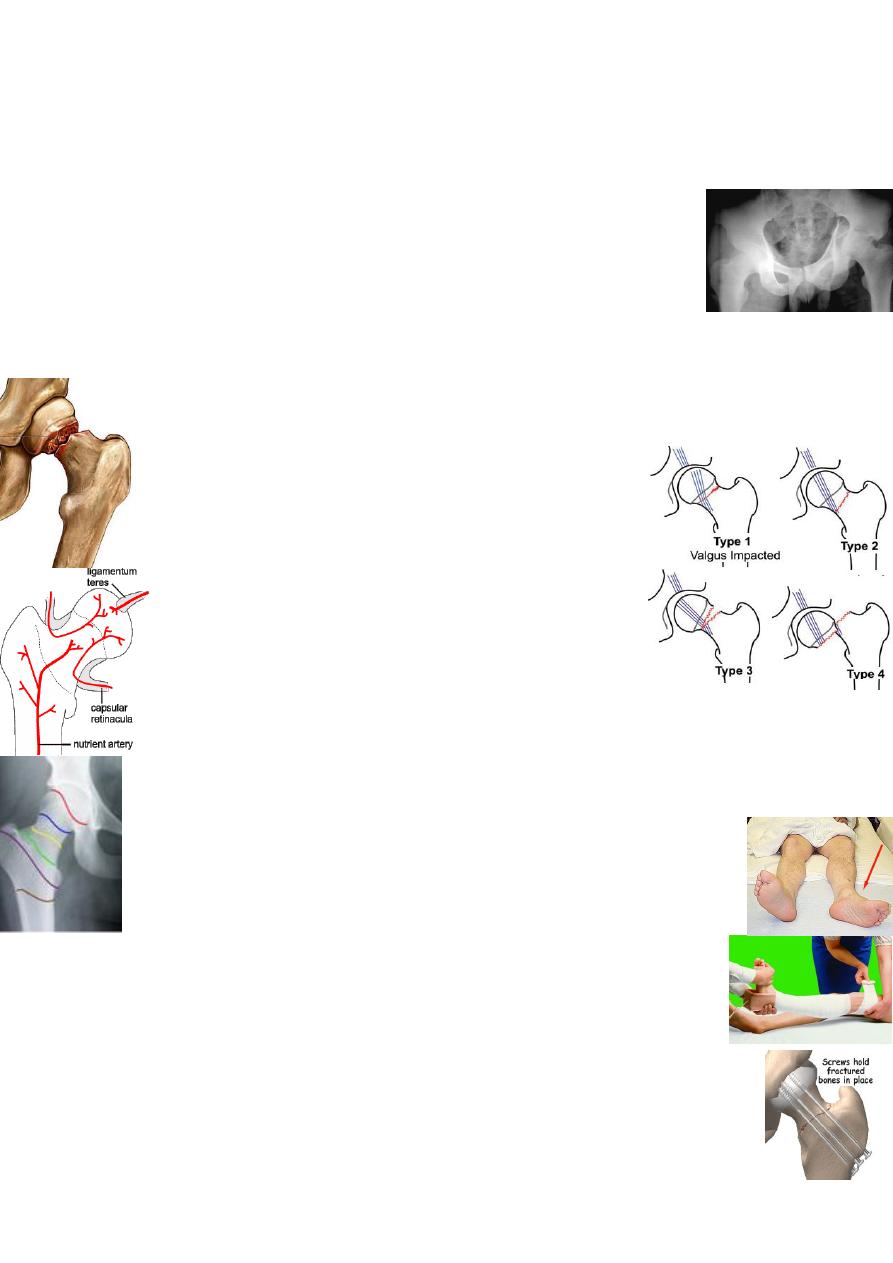
Garden's classification: 4 stages of progressive displacements:
Stage І: incomplete impacted #.
Stage П: complete undisplaced #.
Stage Ш: moderately displaced #.
Stage ІV: severely displaced #.
Healing problems:1-bone ischemia: the femoral head gets it's blood
from: a- ligamentum teres vessels(poor in elderly &in 20% not present);
b-intramedullary vessels (always interrupted by the #);
c-capsular vessels (usually kinked or torn in displaced #). Hence the high
incidence of avascular necrosis in displaced #.
2-poor union: due to: 1-poor blood supply; 2-the femoral neck # is intra-
capsular # &the synovial fluid will prevent clotting of # hematoma;
3-the femoral neck has no soft tissue attachment which could promote
callus formation. Hence the high incidence of nonunion.
CF: short &externally rotated leg.
X-ray: according to site of #, it can be: subcapital, mid-cervical
or basal. Assess the degree of # displacement by
matching of bone trabeculae-Garden's stages.
Treatment: is operative.
The aim is: 1-to keep the patient active to prevent complications of
recumbency
(
lying in bed→ DVT, pulmonary
embolism, pneumonia
&bed sore). 2-to 'ensure' # union by perfect reduction &secure fixation.
Initial treatment: skin traction to relief pain; preoperative preparation.
3
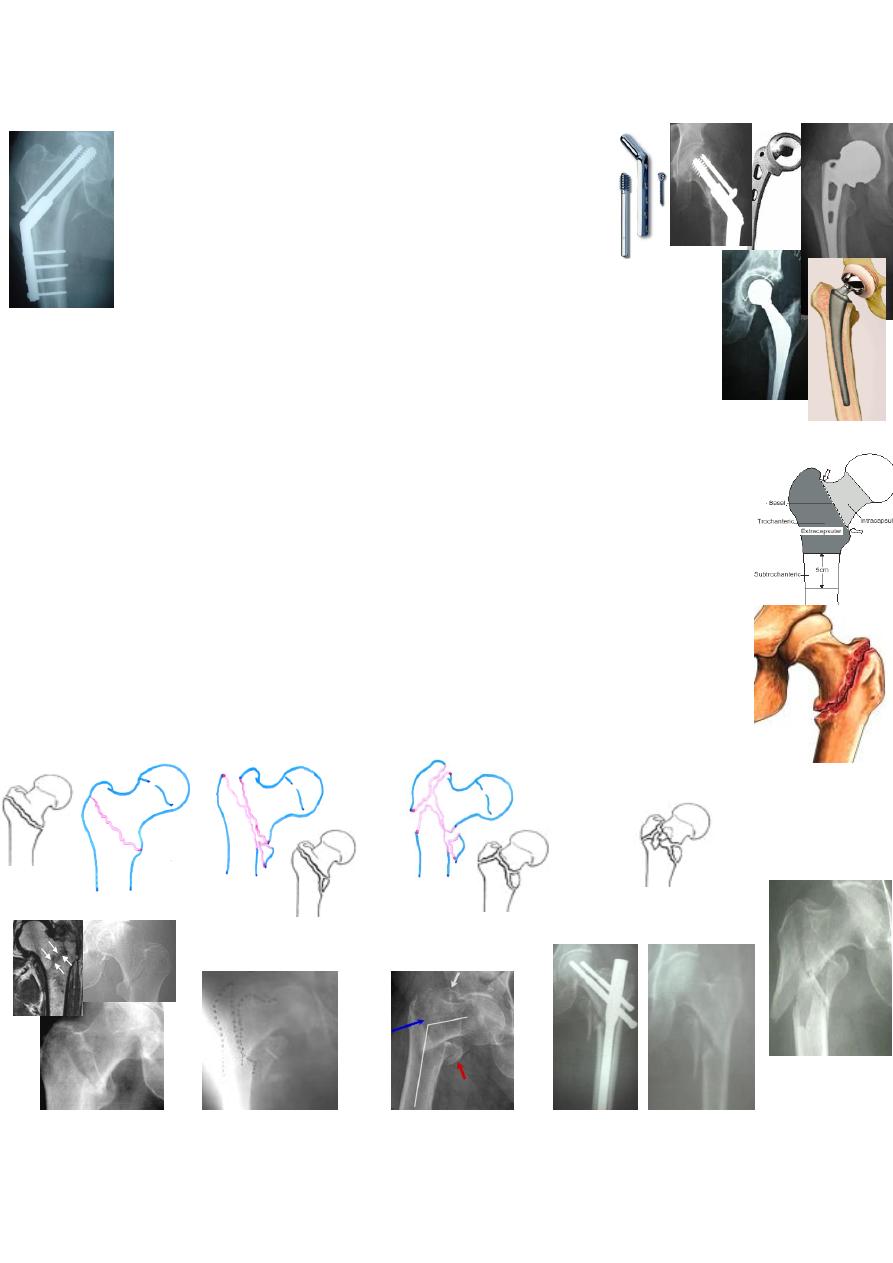
Operations: depending on the age &the degree of displacement:
1-internal fixation( cannulted screws or DHS):
Stage І&П(undisplaced #)→ internal fixation(IF);
Stage Ш&ІV(displaced #)→closed or open reduction
&IF(for patients aged <75years). If >75years:
2-prosthetic replacement: (for those with unpredictable union)
Partial hip replacement: for >75years(stage Ш&ІV) &pathological #.
Total hip replacement: for old #(acetabular damage) &with metastasis.
Post-operative: sit up in bed or chair &start activity from the 1
st
day.
Complications:
1-General: DVT, pulmonary embolism, pneumonia &bed sore. The
mortality is 20% within 4months.
2-Avascular necrosis: occur in 30% of displaced # & in 10% in
undisplaced #.
3-Non-union: occur in 30% of displaced # because of poor blood supply,
poor reduction, poor fixation &poor healing(like other intra-articular #).
4-Osteoarthritis: due to avascular necrosis &femoral head collapse.
Intertrochanteric fractures:
like neck # are common in elderly but
are extracapsular #, so unite quickly without avascular necrosis.
MOI: either direct fall on greater trochanter or indirect twisting injury.
CF: tender swelling &bruise of the upper thigh with short &externally
rotated leg.
X-ray: the # line pass from lesser to greater trochanter.
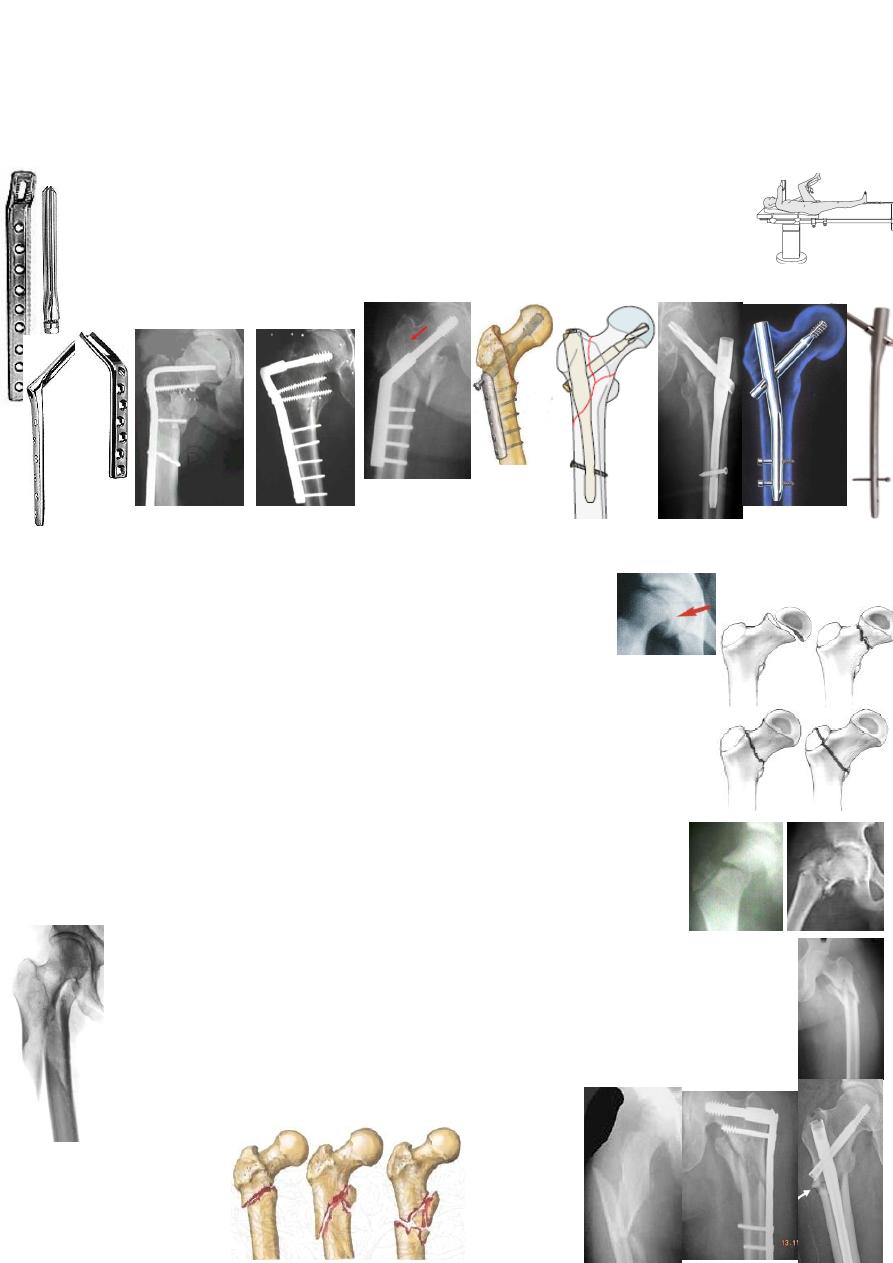
Kyle classification: depends on the degree of # instability.
: Type П: Type Ш: Type ІV:
І
Type
Undisplaced Displaced Displaced Severe comminution
Uncomminuted Lesser trochanter # Greater trochanter # Subtrochanteric extension
Minimal comminution Comminuted (also, reverse oblique #)
Varus Varus
4
*A fracture is considered unstable if: 1-the lesser trochanter is separated;
2- comminuting postermedial cortex; or 3- reverse oblique #.
Treatment: is almost always by internal fixation in order to:
1-obtain the best possible reduction; and 2-mobilize the patient early, thus
reducing the complications of prolonged recumbency.
Types of internal fixation: (closed or open reduction &angled device fixation):
Pin &plate Blade-plate Dynamic hip screw Intramedullary nail&hip screw
±condylar screw
Complications: Early: DVT &pulmonary complications.
Late: 1-failed fixation; 2-malunion(varus &external rotation);
3-nonunion(rare).
Proximal femoral fractures in children:
are uncommon.
MOI: severe trauma like RTA or FFH.
Delbet classification: according to the level of the #:
І: transepiphyseal, П: transcervical, Ш: cervicotrochanteric (basal),
ІV: intertrochanteric, V: subtrochanteric.
Treatment: undisplaced #→ 6-8weeks hip spica.
Displaced #→ CRPP or ORIF.
Complication: 1-avascular necrosis(40% especially in displaced type
І&П). 2- Coxa vara(due to malunion or physeal arrest), 3- shortening.
Subtrochanteric fractures:
may occur at any age following
severe trauma.
CF: swollen tender thigh with short &externally rotated leg.
X-ray: the # is below the lesser trochanter(transverse, oblique or spiral).
The proximal fragment is flexed &abducted while the distal is pulled up
&adducted.
Treatment: is ORIF: DHS for proximal # &locked IM nail for more distal #.
Conservative treatment by traction is possible but difficult: 3 months skeletal
traction in the sitting position.
Complications: 1- malunion; 2- nonunion(5%).

5