1
د.عادل الهنداوي
Orthopedics
Femoral shaft fractures
This is a fracture of young adults following high energy
injury; in elderly, it is pathological until proved otherwise.
MOI: Spiral # is caused by→ a twisting force;
Transverse &oblique #→ direct or angulation force;
Comminuted &Segmental #→ direct &indirect severe violence.
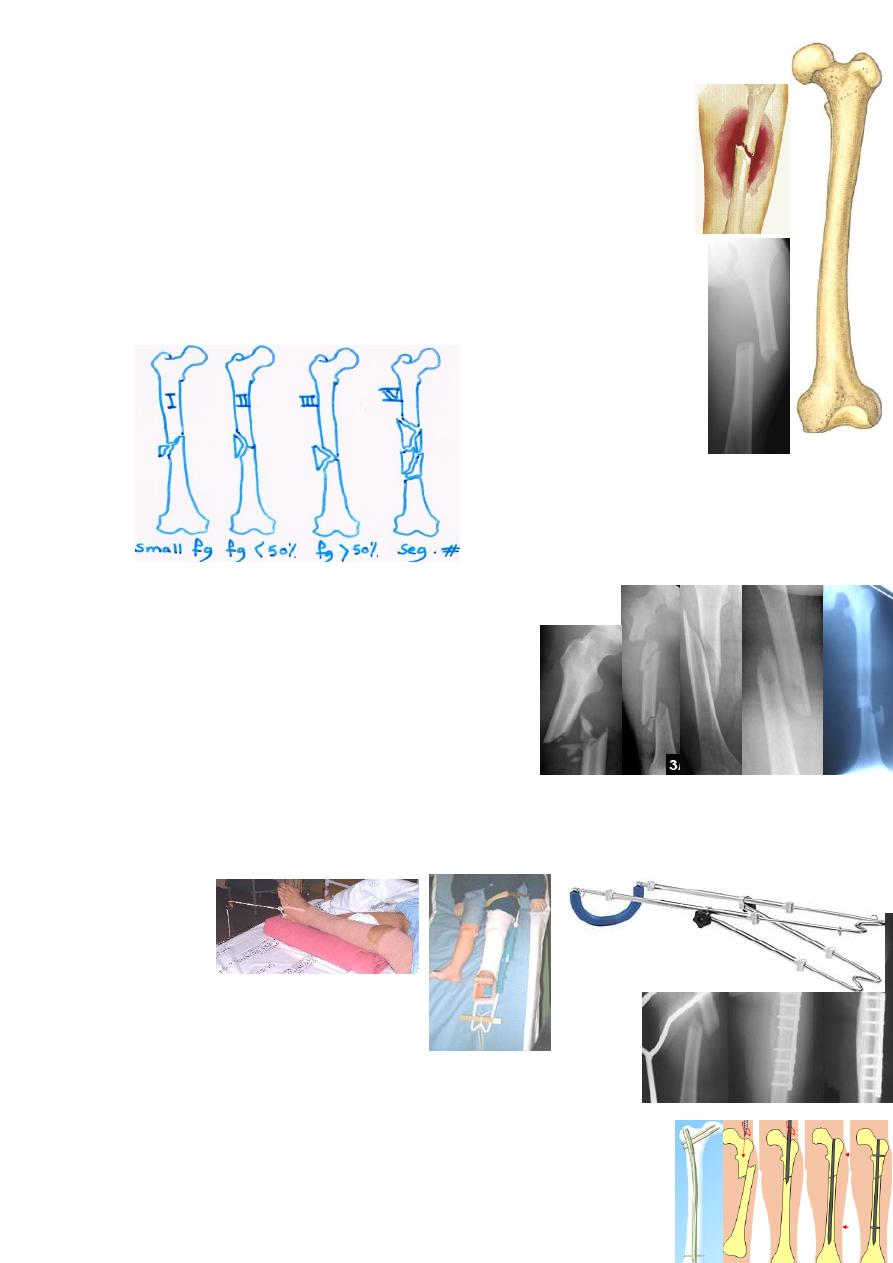
Winquist's classification: depend on degree
of # comminution which reflects # stability:
CF: short &externally rotated limb with deformed,
bruised &swollen thigh due to soft tissue bleeding
(1liter). Look for other limb or pelvic injury or
associated life- threatening injury. Exclude
neurovascular problem.
X-ray: always x-ray the hip(to exclude another
# or ≠) &the knee (floating knee). Those with
multiple injury, also need pelvic &CXR.
Emergency treatment: at the site of accident, the
limb should be splinted by tying to other limb or any available splint but
the ideal is Thomas' splint to: control pain, ↓ bleeding &make transfer easier.
Operative treatment:
Plating: lateral plate with 4-5screws in both fragments.
Intramedullary nailing: open or closed reduction with
ante- or retro-grade nailing→ for mid &upper 1/3 stable #.
2
Locked IM nailing: closed reduction with IM nail locked
by interlocking proximal &distal screws for unstable
comminuted # & for subtrochanteric &lower 1/3 #.
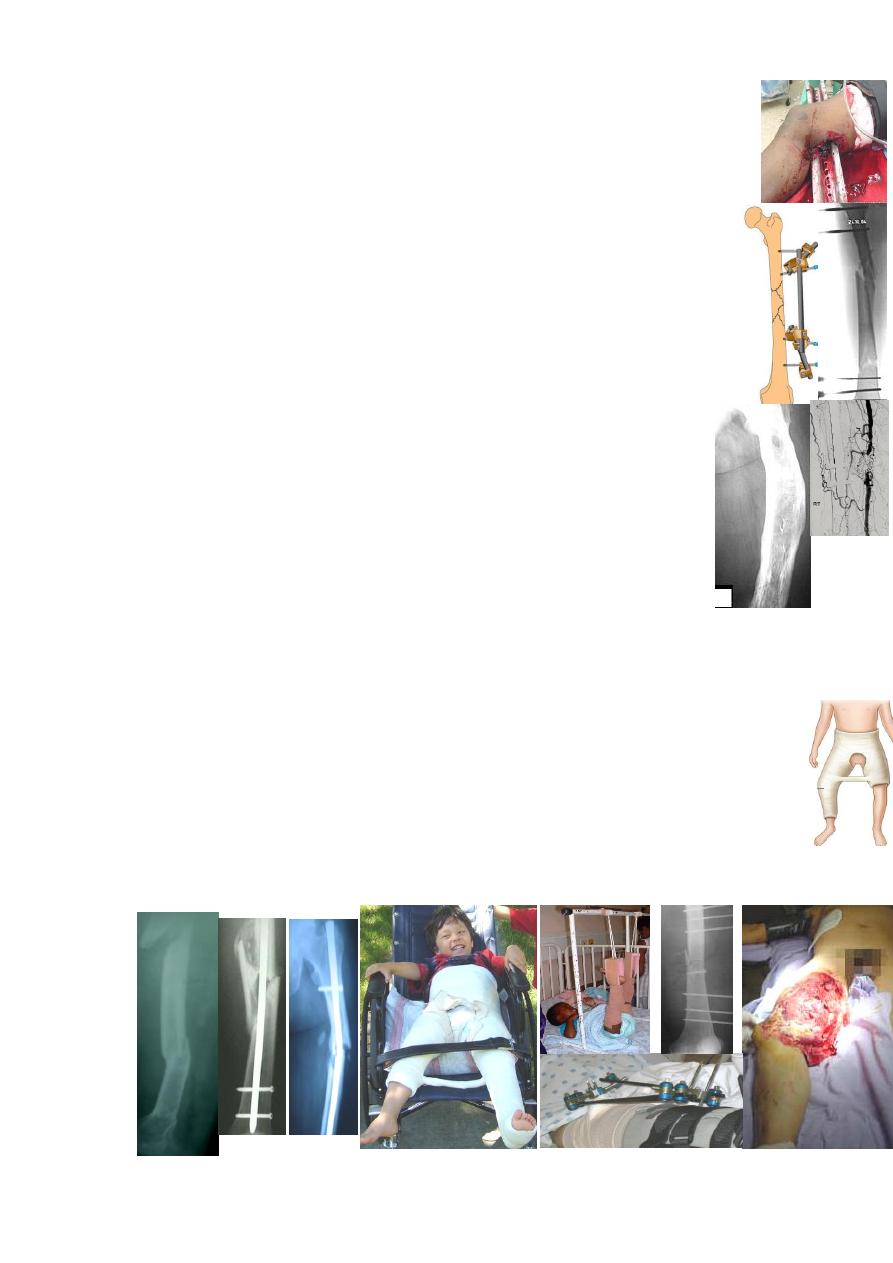
External fixation: closed reduction &percutaneous fixation for:
1-severe open #; 2-multiply injured patients; 4-severly comminuted #;
5-# with bone loss; and 5-# with vascular injury.
Fracture with vascular injury: warning signs are: 1-severe bleeding or
hematoma; and 2-distal ischemia. Investigations: 1-doppler; and 2-arterio
graphy. Ŗ→ quick # fixation &arterial repair or bypass(no >6hrs delay).
Complications: Early: 1-Shock: 1-2liters lost, Ŗ→ transfusion.
2-Fat embolism &ARDS: risk factors are multiple injury, chest
injury & shock. CF: ↑pulse rate, ↑temp, dyspnea, restless &petechial
hemorrhage. Investigation: blood gases. Ŗ→ supportive.
3-Thromboembolism; 4-Infection: in open # &after IF of closed #; Ŗ→
AB, debridement, external fixation.
Late: 1-Delayed union &nonunion: Ŗ→ rigid fixation &bone graft.
2-Malunion: angulation(<15°is accepted), shortening &malrotation.
3-Knee stiffness: due to soft tissue adhesion, Ŗ→ early physiotherapy.
4-Implant failure: due to early weight bearing before # healing.
Femoral shaft fracture in children:
are common; MOI: FFH or RTA.
Treatment: usually conservative, according to the age:
Infant(<2yr): 1-2weeks traction→ 4weeks spica cast(30°angulation is accepted).
Children(2-10yr): 2-3weeks traction→ 4weeks spica cast(20°
angulation &1cm shortening are accepted); or early CR &spica cast.
Teenager: 4-6weeks traction→ 6weeks spica cast.
Operative treatment: if traction fails to reduce the #→ internal or external fixation.
Angulation &shortening may be corrected to some extent with growth but rotation will not.
*
3
Supracondylar fractures of the femur:
seen in young
as a result of high energy injury or in old osteoporotic patients.
MOI: direct force; the distal fragment may be flexed by gastro-
cnemius pressing on popletial artery.
CF: swollen deformed knee; always palpate the distal pulse.
X-ray: transverse # line just above the condyles or comminuted #.
Treatment:
Conservative: for young with undisplaced or easily reduced #:
skeletal traction through upper tibia with knee in flexion for
6weeks→ cast-brace &partial weight bearing(PWB).
Operative: if closed reduction fails→ ORIF using angled device like L-plate
or better dynamic condylar screw(DCS)or locked IM nail. The advantages of
ORIF: easy nursing for elderly &knee movements can be started early
Complications: Early: arterial injury.
Late: knee stiffness &nonunion
Fracture-separation of the distal femoral epiphysis: is the adolescent equivalent
of supracondylar #. MOI: either hyperextension force→ forward displacement of
distal epiphysis or angulation force→ lateral shift of epiphysis.
CF: swollen deformed knee; the popliteal artery may be obstructed
by lower femur. X-ray: usually Salter-Harris type П.
Treatment: closed reduction &cast splint or ORPP or screw fixation.
Complications: 1-Vascular injury in hyperextension deformity→ urgent reduction.
2-Physeal arrest causing varus or valgus deformity or shortening.
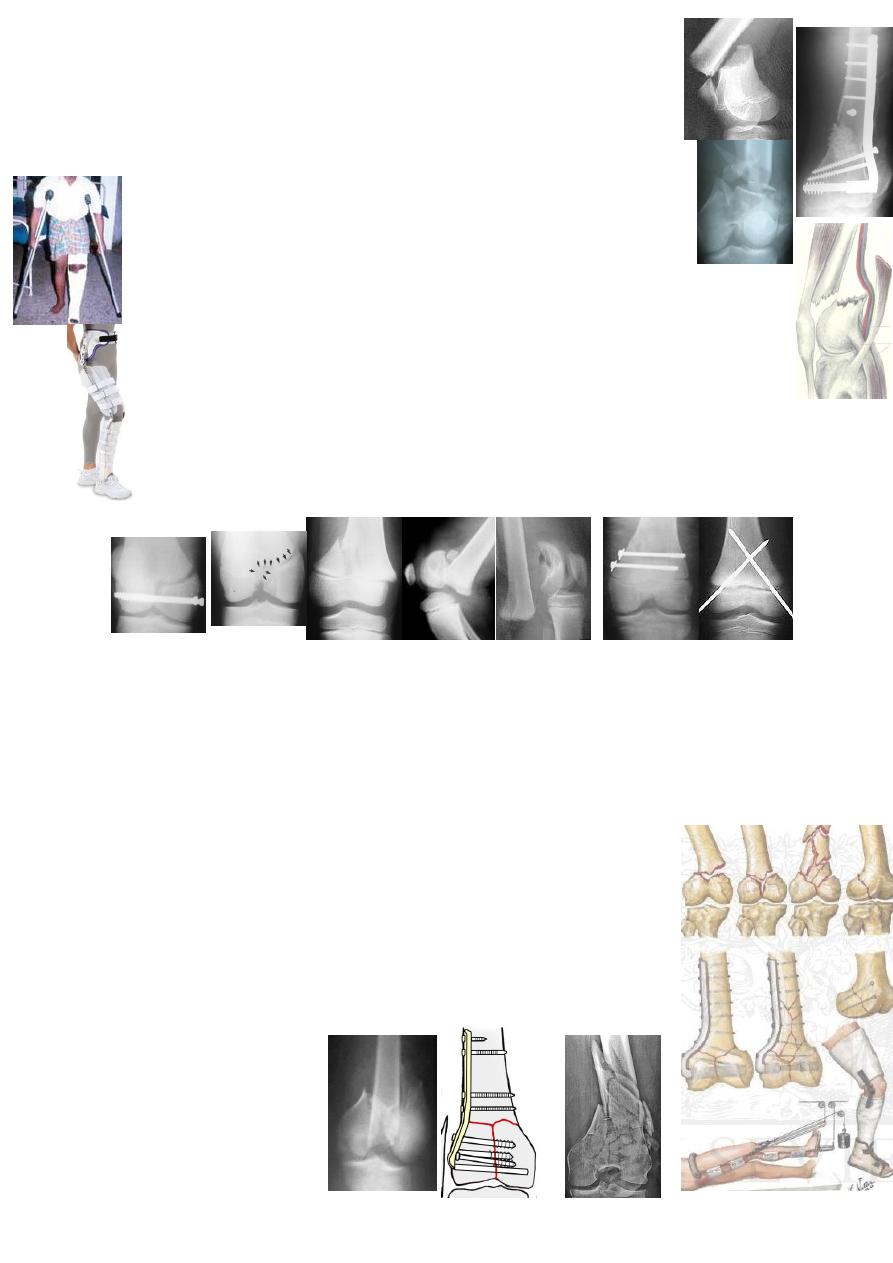
Femoral condyle fractures:
MOI: either direct force or FFH; or in association with supracondylar #.
CF: swollen deformed knee with 'doughy' feeling of the haemarthrosis.
X-ray: one condyle is # &pushed up or both condyles are # in T- or Y-shape.
Treatment:
Conservative: 6weeks skeletal traction→ cast brace. If reduction fails:
Operative: ORIF using: cannulated screws, blade-plate or DCS.

4