Orthopedics
Perthes' disease
(Legg-Calvẻ-Perthes disease)
Is a painful disorder of childhood characterized by avascular
necrosis of the femoral head. Incidence →1/10000. ♂:♀ ratio
is 4:1; Age → 3-12 years. more → 4-8 yrs. Cause: is unknown.
Pathogenesis: how the FH become ischemic?
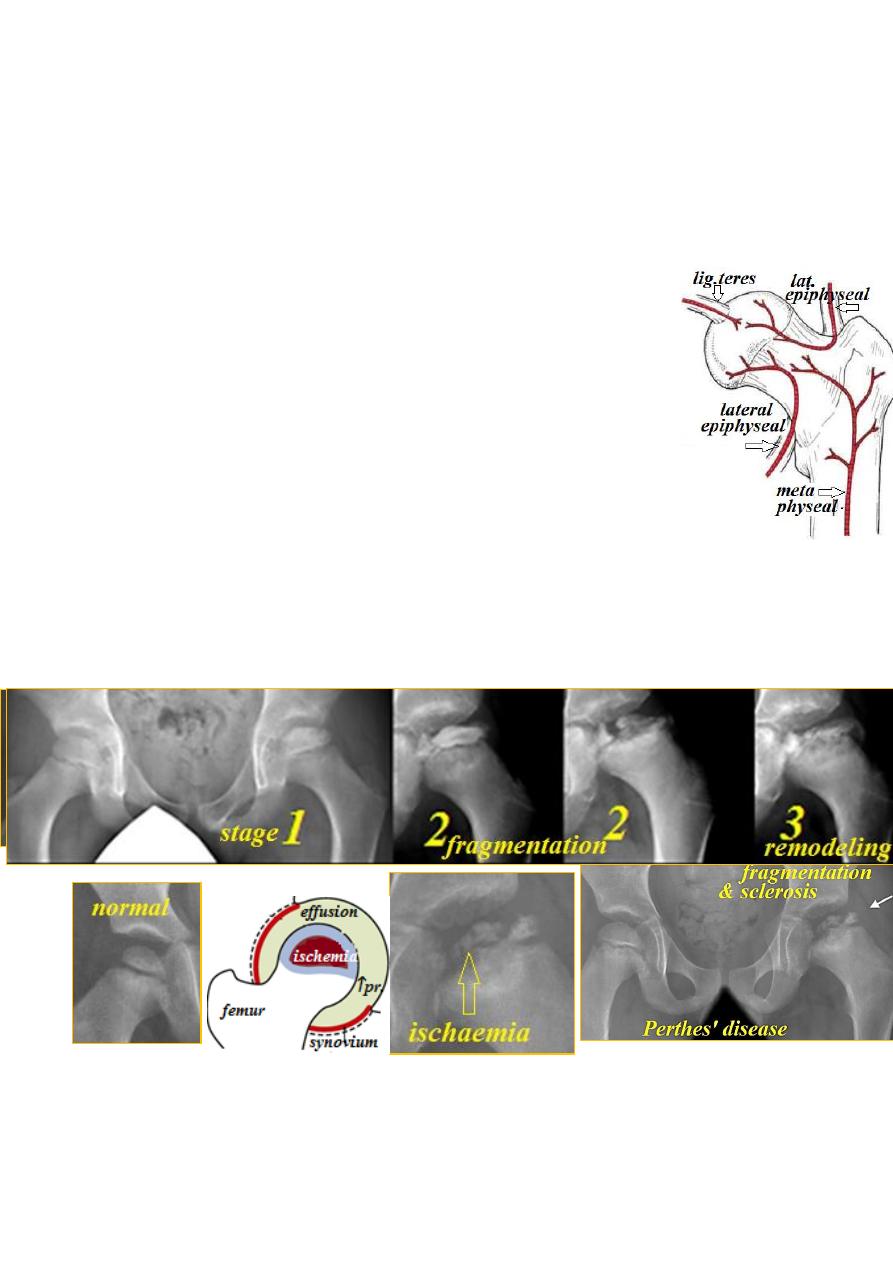
Normally, the blood supply of the FH depends on the age:
Before 4 years→ it comes from 3 sources: 1-lig. teres(small amount) ;
2-lateral epiphyseal vessels; 3-metaphyseal vessels penetrating growth
disc which ↓ gradually& disappear at 4 yrs. to reappear gradually
&become full with epiphyseal closure.
By the age of 7 yrs the vessels in the lig. teres have developed, so there
is a critical period between the age of 4-7 yrs. in which the FH depends
entirely on lateral epiphyseal vessels. Any condition causing effusion
(trauma or synovitis) will stretch the capsule → venous stasis →↑ intra
osseous pressure → ischemia.
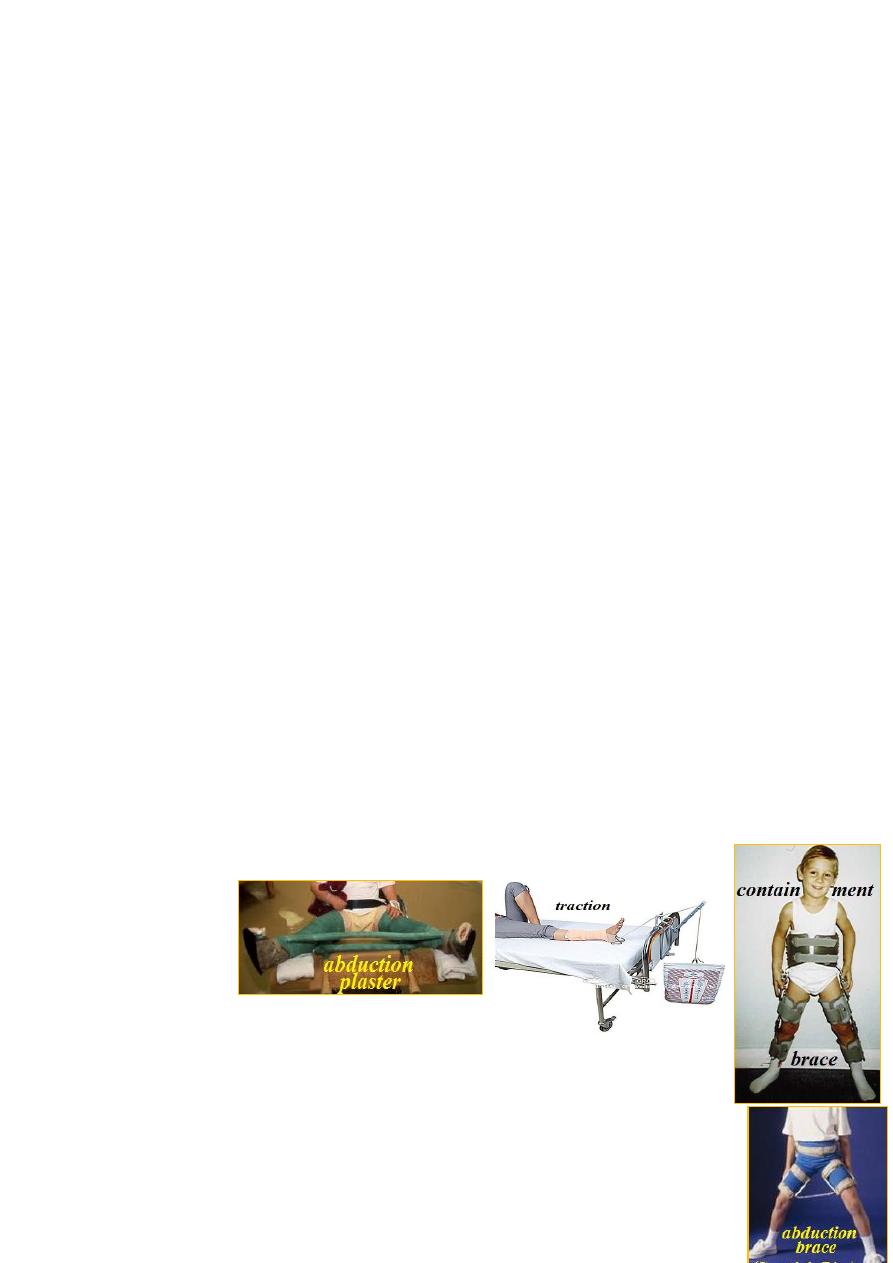
Pathology: the condition takes 2-4 years to complete healing passing
through 3 stages:
Ι-ischaemic &bone death: all or part of bony nucleus of FH is dead;
on x-ray it looks smaller as it stops growing while the cartilage
remains viable &becomes thicker causing ↑ joint space on x-ray.
ΙΙ-revascularization &repair: within weeks, revascularization
begins gradually &new bone will form replacing the dead bone
causing ↑bone density on x-ray. At the same time, dead bone is resorbed
giving rise to fragmentation on x-ray. The metaphysis looks porous,
wider & cystic. In severe cases, the acetabulum also involved.
ΙΙΙ-distortion &remodeling: if repair process is rapid, the head will
restore its normal shape. If it is slow, the head will collapse &later
growth will be distorted (flat, oval or mushroom) which gradually
enlarge &displace laterally away from the acetabulum.
CF: a boy of 4-8 years complains of pain &start limping for weeks on
end or recur intermittently.
O/E: the child looks otherwise well. The hip early is Irritable (extremes
of all ROM are painful &limited). Later, limitation of abduction in
flexion &internal rotation.
Ḑ: Early X-ray is normal except slight widening of j. space. Bone scan
at this stage shows cold area.
Later: small dense FH → flattening of FH.
Still later: FH collapse→ fragmentation→ lateral displacement.
Metaphysis become wider, rarefied &cystic.
Note: the involvement of the FH is variable, sometime, only a small area
is involved or 50% or 75% or 100% of FH.
After healing: large deformed FH, short F neck + subluxation.
Ŗ→ while the hip is irritable, the child should be in bed with skin
traction until pain subsides usually 3 wks. Then allowed restricted
activities &checked regularly every month (symptomatic Ŗ).
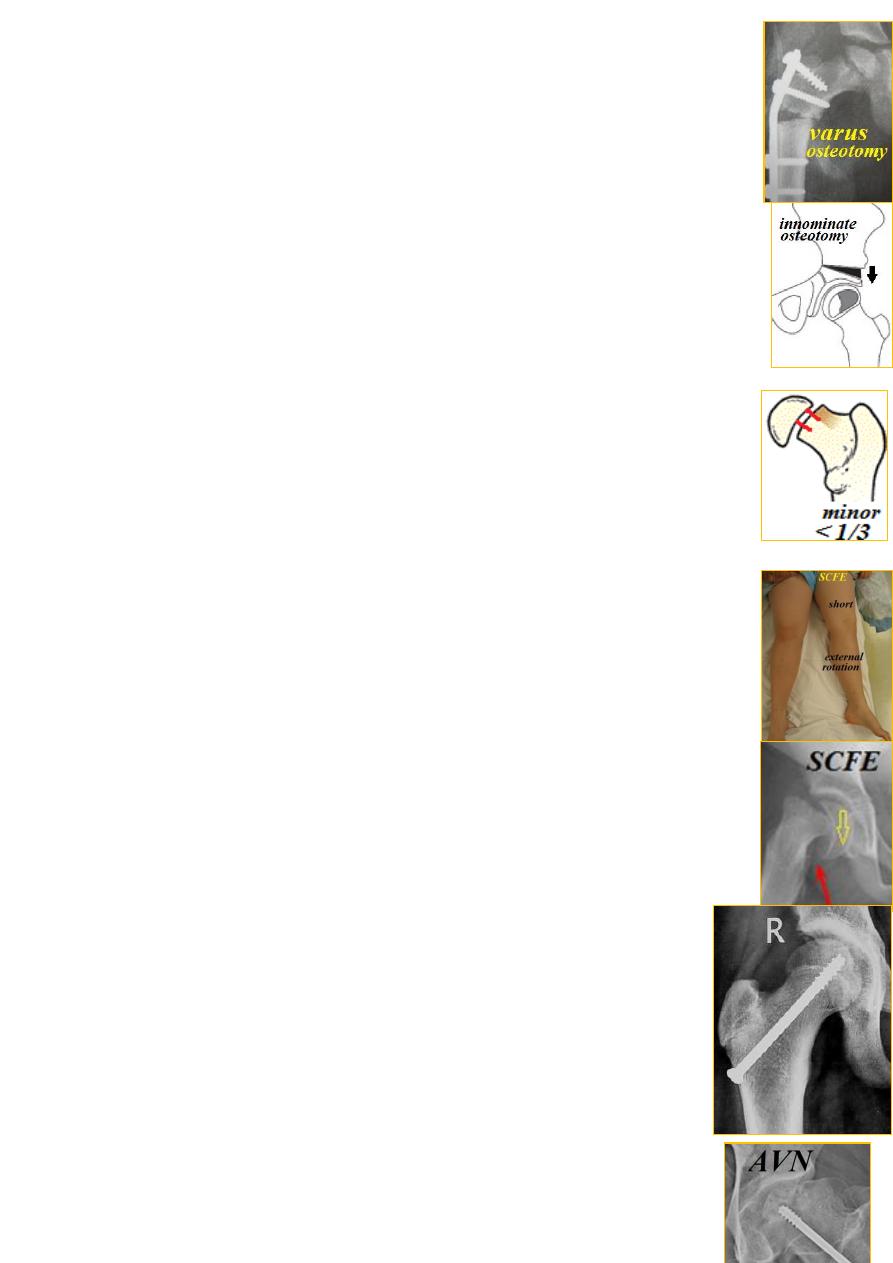
If the condition get worse→ do containment of the FH within
the acet. so it retains its normal shape during repair process.
Either by holding the hip widely abducted by plaster or splint
for 1-2 years; or by surgery (subtrochanteric varus osteotomy
or innominate osteotomy).
Prognosis:
1- boys have better prognosis than girls.
2- the grater the degree of FH involvement the more worse the prognosis.
3- the older the age the worse the prognosis.
4- progressive FH subluxation→ bad prognosis.
Slipped capital femoral epiphysis
Displacement of proximal femoral epiphysis(epiphysiolysis)
is uncommon. Usual age is 14 yrs.; ♂:♀ ratio 3:1. Left ˃ right;
if one side slips, there is 30% risk for other side to slip.
Etiology: 1-hormonal imbalance (hypogonadism or hypothyroidism);
2-trauma in 50% of cases.
Pathology: the disruption occurs through hypertrophic zone of the
physis. The femoral shaft rolls into external rotation with femoral
neck displaces anteriorly while the epiphysis remains in the acet.
This usually is associated with tear of anterior retinacular vessels.
CF: a child around puberty who is either fatty &sexually immature
or tall &thin. The condition in 30% of cases is acute &in 70% is
chronic or acute on chronic.
The presentation is painful limping which recurs with exercise.
O/E: short limb &externally rotated with limited ROM.
X-ray: AP view→ pass a line(Klein) with upper border of femoral
neck ,this normally should intersect part of epiphysis; if not→ slip.
Lat. view→ the angle between the growth plate & a line through the
center of the neck should be 90ᵒ ; if less→ slip.
Ŗ→ is surgical stabilization of the physis &this depends on the
degree of the slip:
1- Minor slip(˂1/3 slip): Ŗ→ fixation in situ by2-3 screws through
the neck into the epiphysis.

2- Moderate slip( 1/3 - 2/3 slip):Ŗ→ again accept the deformity &
do fixation in situ; after 2 yrs., if deformity is severe, do corrective
osteotomy below the neck.
3- Severe slip(˃ 2/3 slip): here the deformity is unacceptable
&if untreated → OA. So the Ŗ→ is ORIF using 2-3 screws.
Complication: 1-Avascular necrosis of the FH due to forceful
manipulation or operation which damage posterior retinacular vessels.
2-coxa vara; 3-other side slip, Ŗ→ prophylactic fixation in pre-slip stage.
4- chondrolysis; 5-secondary OA.
Pyogenic arthritis
Usually seen in children; the organism is usually staph. It either starts
as arthritis or secondary to osteomyelitis of upper femur.
CF: ill child &in pain; the limb is held still.
O/E: hip tenderness &restricted all ROM.
X-ray: early: soft tissue swelling &lat. FH
displacement. U/S→ hip joint effusion.
The best is aspiration of pus from the joint.
Ŗ→ drainage by arthrotomy, antibiotics, rest the hip in abduction splint
or traction.
Complication: if untreated, the FH &neck may be destroyed→
pathological hip dislocation.
Avascular necrosis-AVN(osteonecrosis-ON)
The FH is the commonest site of AVN. It is either post-traumatic or non-
traumatic. Age is 20-50 yrs.
Non-traumatic ON: seen in:1-high dose steroid; 2-chemoŖ; 3-radiation;
4-alcohol abuse; 5-septic arthritis; 6-Perthes' disease.
Staging(Ficat): Stage Ι-pain, limp &limited ROM; x-ray: normal;
bone scan: FH ischemia. MRI:marrow ischemia.
Definite Ḑ: bone biopsy.
Stage ΙΙ-x-ray early changes: patchysclerosis, cystic lesion &fracture
line.
Stage ΙΙΙ- x-ray shows collapse of the FH.
Stage ΙV- secondary OA changes.
Ŗ→ stage Ι & ΙΙ: osseous decompression to relief venous stasis
&intraosseous compartment syndrome by removing a core (7mm)
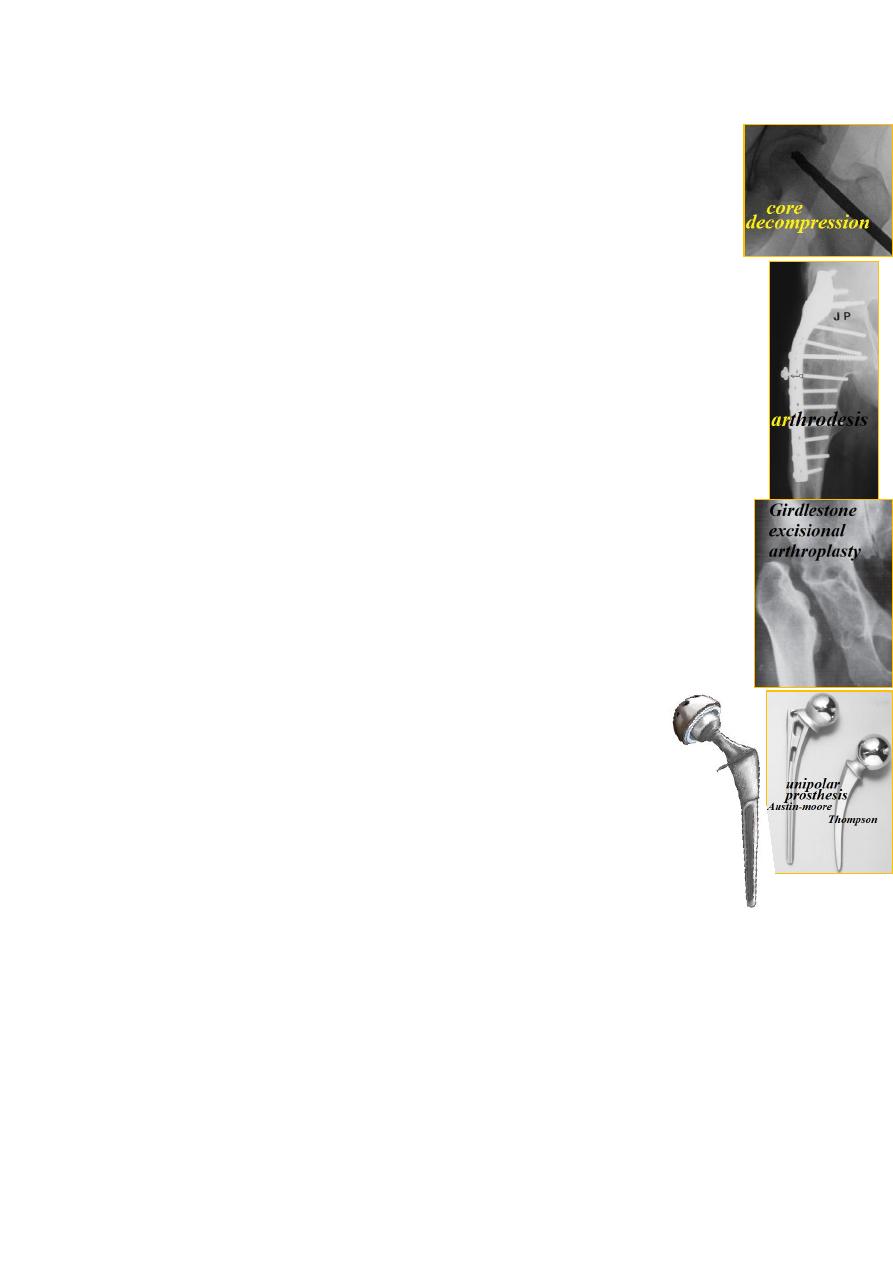
of bone from the neck. This may also improve the blood supply to
FH by growth of new granulation tissue with new blood vessels.
Stage ΙΙΙ: if the collapse affects only small segment of FH
&the patient is young(˂40 yrs.)→ realignment osteotomy
to displace the necrotic segment away from the line of
maximum stress of weight bearing.
Stage ΙV→ partial or THR.
Prognosis→ usually poor &most patient will need THR.
Arthrodesis:
is surgical fusion of the hip; it reliefs pain &provides
stability but at the cost of movement though lumbosacral movement
gives some compensation.
Indications: any condition causing hip destruction when osteotomy
& arthroplasty are contraindicated.
Position: 20ᵒ flexion; 10ᵒ adduction &some external rotation.
Arthroplasty
Excisional arthroplasty: excise the head & create a pseudojoint;
it is the last choice when all other operations fail e.g. THR failure
due to infection.
Replacement arthroplasty: either partial or total hip replacement.
partial hip replacement: replace only the FH.
Total hip replacement(THR): replace both femoral head &acet.
Indications: for patients ˃ 50 yrs. with hip destruction;
Contraindications: latent sepsis.
Complications:
1-general complications of elderly like DVT;
2-operative complication (sciatic n. injury or fracture femur);
3-postoperative dislocation;
4-heterotopic bone formation;
5-infection (early &late);
6-aseptic loosening.
