1
Injuries of the pelvis
Fractures of the pelvis account for less than 5% of all skeletal injuries, over 10% of
these patients will have associated visceral injuries & in this group the mortality rate is
in excess of 10%.
Surgical anatomy
It is important to know what dose pelvic ring mean in order to understand pelvic #:
The pelvic ring is made up of the two innominate (hip) bones & the sacrum,
articulating in front at the symphysis pubis & posteriorly at the sacroiliac joints.
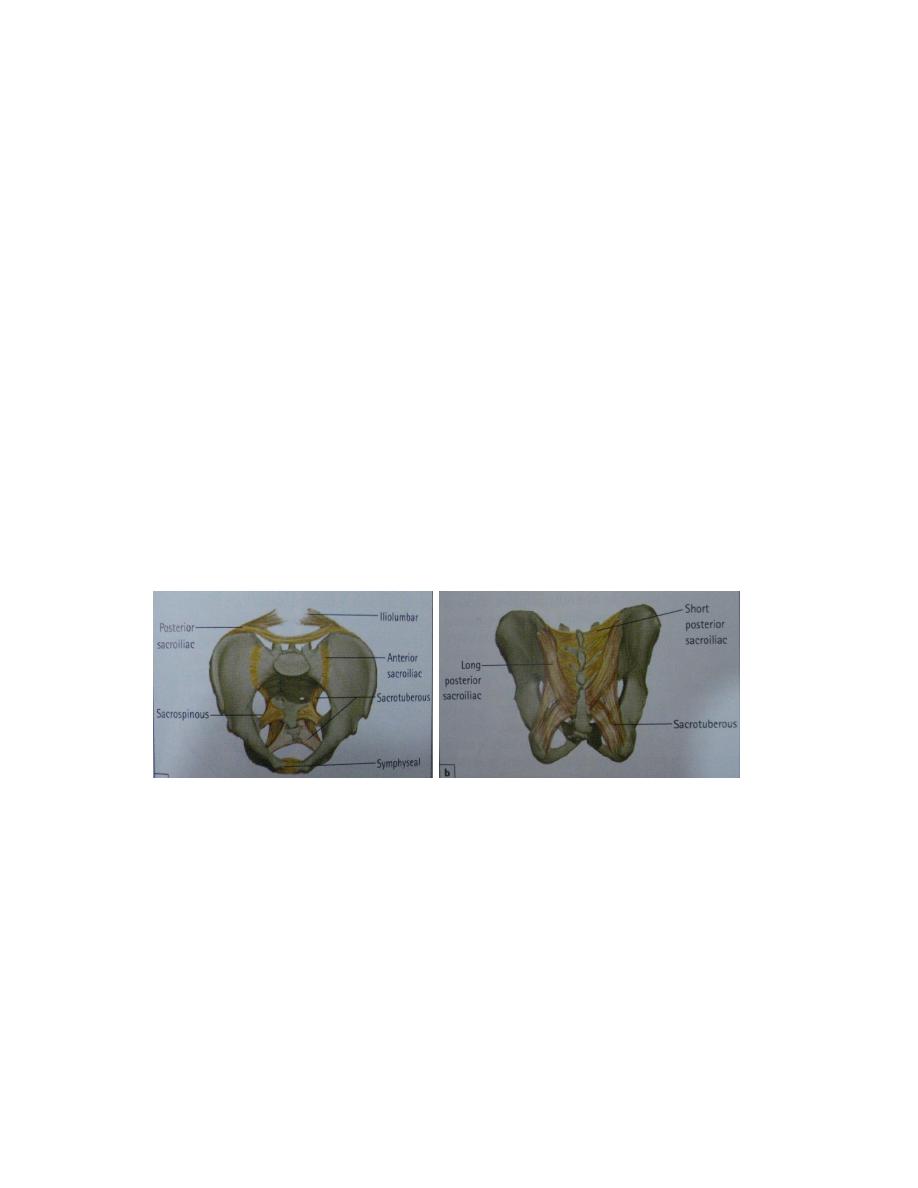
The stability of this ring depends upon the rigidity of the bony parts & the integrity of
the strong ligaments that bind the three segments together across the symphysis pubis
& the sacroiliac joints. The strongest &most important of the stabilizing ligaments are
the sacroiliac (anterior &posterior) &iliolumbar ligaments; these are supplemented by
the sacrotuberous &sacrospinous ligaments & the ligaments of the symphysis pubis.
Types of pelvic injury
Pelvic injury can be divided into 4groups:
• Isolated #with an intact pelvic ring.
• Fractures with a broken ring, these may be stable or unstable.
• Fractures of the acetabulum.
• Sacrococcygeal fractures.
2
Isolated fracture
Avulsion fractures
A piece of bone is pulled off by violent muscle contraction; this is usually seen in
athletes& sportsmen. The anterior superior iliac spine can be pulled off by
Sartorius, the anterior inferior iliac spine by rectus femoris, the pubis by adductor
longus & part of the ischium by the hamstrings.
Direct fractures
Caused by a direct blow to the pelvis, usually after a fall from height, which may
fracture the ischium or the iliac blade.
Treatment: By rest & analgesia. The patient can walk when pain subsides.
Stress fractures
These usually involve the pubic rami in patient with osteoporosis or osteomalacia
during normal activity because their bone is weak.
Treatment: By treating the underlying cause (osteoporosis) by calcium & vitamin
D supplement &encourage movement.
Fractures of the pelvic ring
Because of the rigidity of the pelvic ring, a break at one point in the ring (anteriorly
or posteriorly) must be accompanied by a break at a second point opposite to the
first point. Usually the second break is not visible either because it reduces
immediately or because the sacroiliac joints are only partially disrupted in this case
the injury is stable. But if there is displacement at the two points then the injury is
unstable &the pelvis cannot withstand load-bearing.
3
Classification& Mechanisms of injury of pelvic ring
(
Young & Burgess)
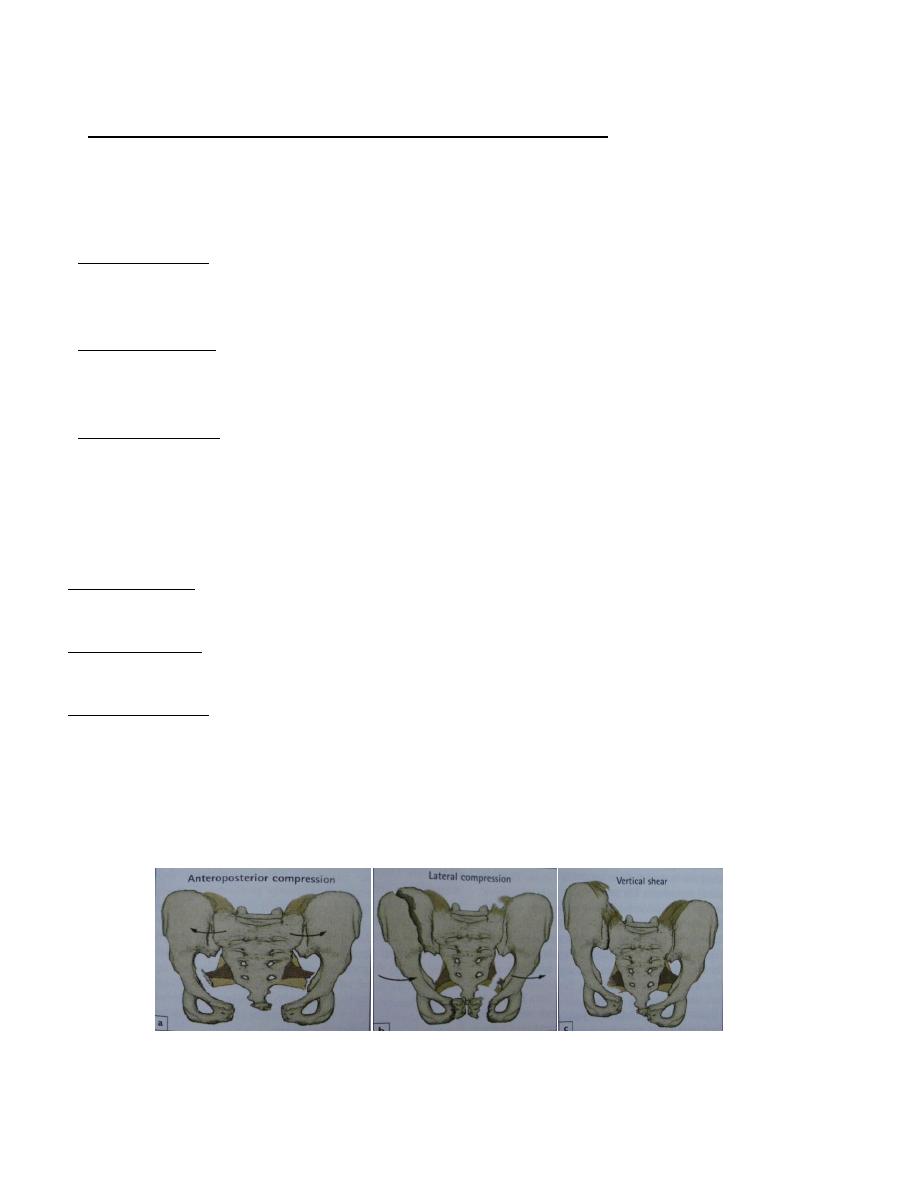
Anteroposterior compression (APC): the open book pattern, this injury is usually
caused by a frontal collision between a pedestrian & care, the innominate bones are
externally rotated with disruption of the symphysis.
*APC-I injuries; there is slight (less than 2 cm) diastasis of the symphysis &there is
some strain of the anterior sacroiliac ligament (invisible on x-ray).the pelvic ring is
stable.
*APC-II injuries; the diastasis is more than 2 cm &the anterior sacroiliac ligaments
are torn. Therefore the pelvis is rotationally unstable, but because the posterior
sacroiliac joint is intact the injury is vertically stable.
*APC-III injuries; the anterior &posterior sacroiliac ligaments are torn. the one
hemi-pelvis is disconnected from the other anteriorly &from the sacrum
posteriorly. The ring is unstable both rotationally &vertically.
Lateral compression (LC): the close book pattern. This injury is caused by side –
to-side compression in road traffic accident or a fall from height.
*LC-I injuries; there is transverse # of pubic ramus (rami) with compression # of the
sacrum.
*LC-II injuries; there is # of the rami (anteriorly) with # of the iliac wing posteriorly
on the side of the impact, the ring remain stable.
*LC-III injuries; as the victim is run over the lateral compression force on one iliac
wing results in an opening Anteroposterior force on the opposite ilium.
Vertical shear (vs): This occur typically when someone fall from height onto one
leg. These are usually severe &unstable injuries. The hemi-pelvis is displaced in
cranial direction, damaging both the anterior &posterior sacroiliac ligaments
therefore the hemi-pelvis is totally disconnected.
APC LC VS
4
Clinical features:
Stable injuries; the patient is not severely shocked, has pain on attempting to walk
& there is localized tenderness. Damage to pelvic viscera is uncommon.
Unstable injuries;
*HISTORY: there is history of fall from height or severe road traffic accident, the
patient is in great pain &unable to stand, he may also unable to pass urine; there may
be neurological symptoms from nerve injury of lumbar &sacral plexuses.
*EXAMINATION: the patient is severely shocked, there may blood at external
meatus, there may be leg length discrepancy (in vertical shear), there may be
swelling or bruising of the lower abdomen, thighs, perineum, &the scrotum or the
vulva from extravasation of the urine.
Tenderness is wide spread &attempting to move blades of the ilium is very painful,
pulling or pushing the leg may reveal the vertical instability. Rectal examination
may reveal sacrococcygeal tenderness, tenderness of the prostate or high riding
prostate suggesting rupture of membranous urethra &dislocated prostate.
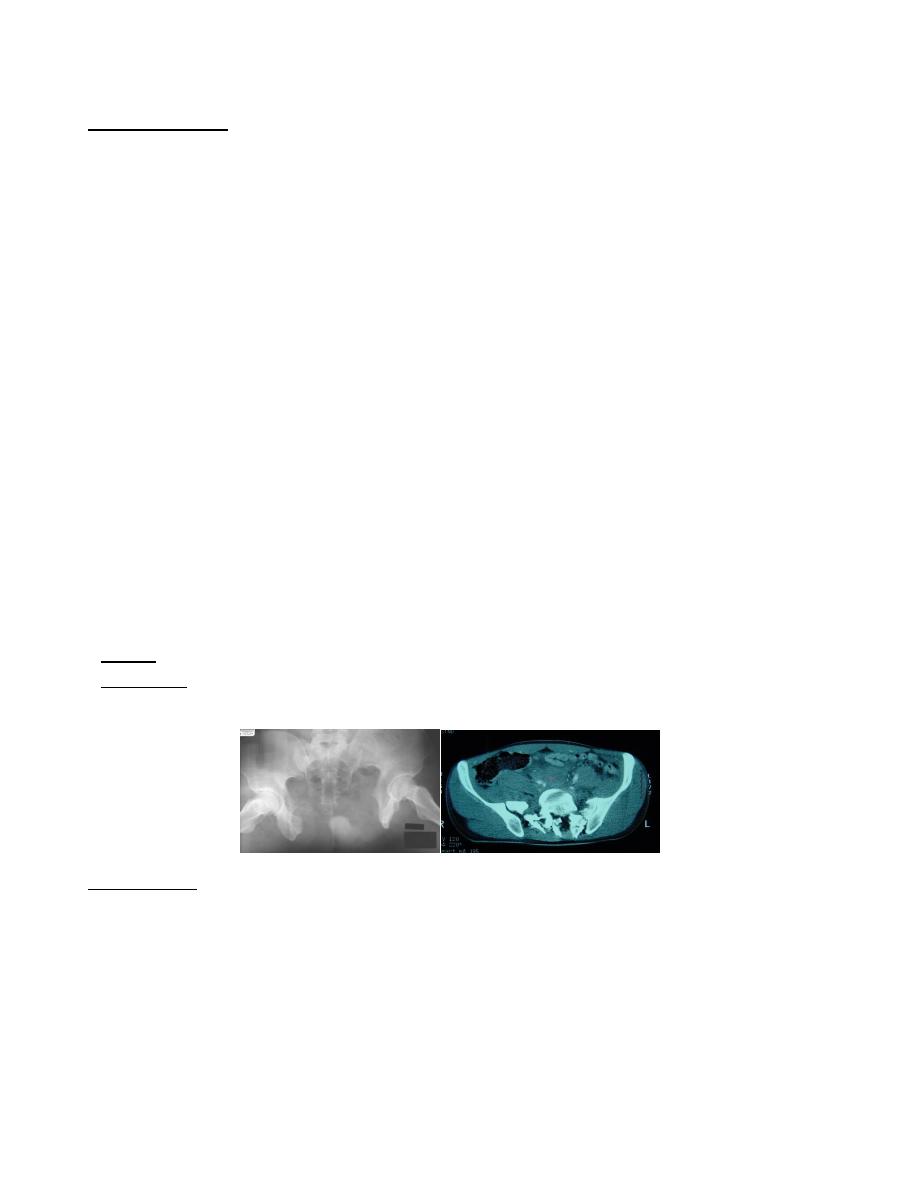
*IMAGINING:
X-ray; AP, inlet, outlet & 2 lateral views may.
CT-scan; is the best way of visualizing the nature of the injury especially the
posterior elements.
Management
Early management: (ABC)
The first step is to ensure clear airway & adequate ventilation, active bleeding
should control & shock treated by adequate fluid replacement &blood transfusion, if
necessary a painful #s are splinted & a single AP x-ray of the pelvis is obtained.
5
Treatment of severe bleeding
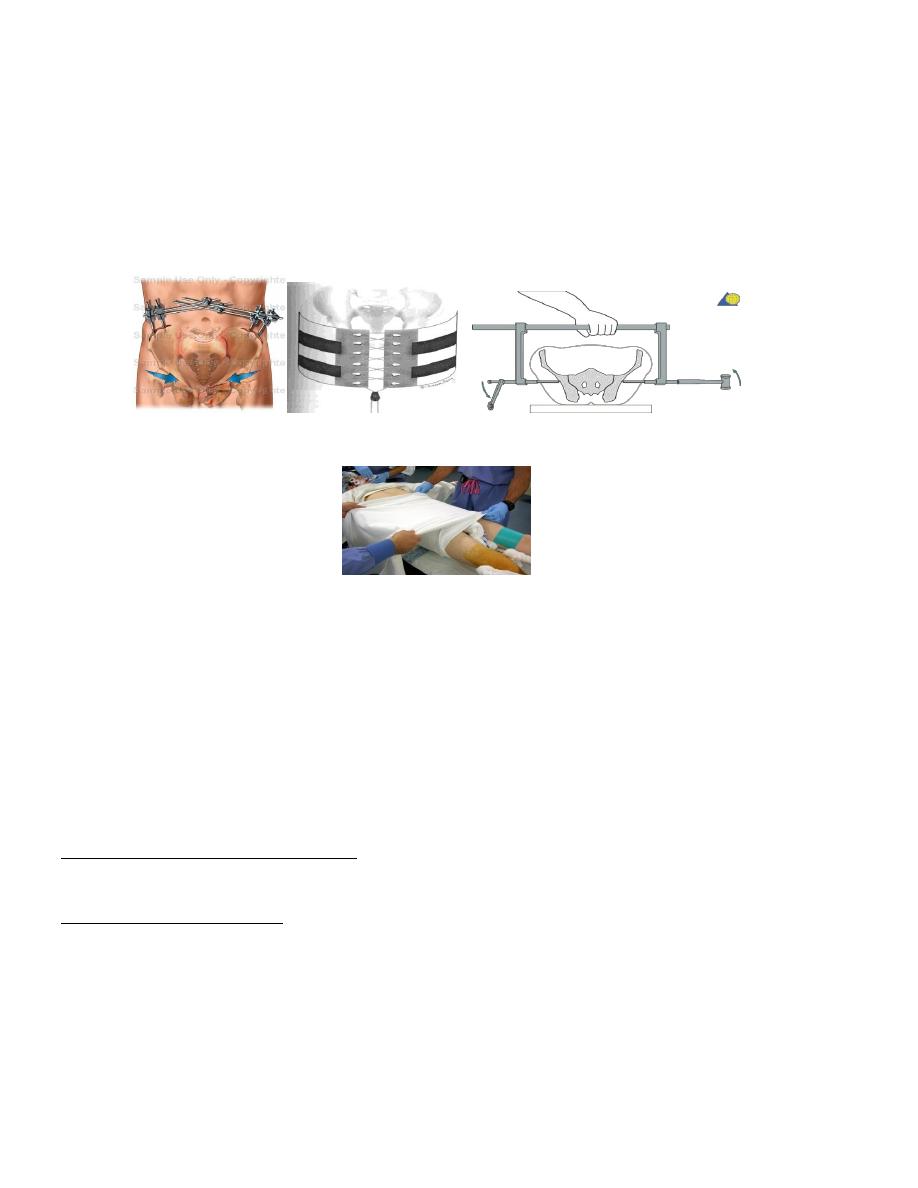
If there is an unstable # of the pelvis, hemorrhage will be reduced by;
1. Rapidly applying an external fixator, but if the patient is unfit for surgery, then an
alternative methods, 2. Pelvic clamp, 3. Pelvic Binders, 4. Sheet tied around the
pelvis, 5.pneumatic antishock trouser.
External fixator Pelvic Binders Pelvic clamp
Sheet
All the above measures act by;
(1) Decreasing the bleeding at the # site (2) decreasing the size of the pelvic cavity
& increased the tamponade effect of the haematoma.
If there is persistent shock & there is no evidence of intra-abdominal or
retroperitoneal hemorrhage, then we do angiography with embolization.
Definitive treatment of the #
Isolated # & minimally displaced #need only bed rest with lower limb traction for 4-6
weeks until the patient is comfortable then allowed up using crutches.
APC (open book )injuries; APC-I (separation of the symphysis <2cm) usually treated
by bed rest with posterior sling or elastic girdle to close the book,
APC-II (separation >2 cm) these injuries require closing the book by lateral
compression of the two hemi-pelvis, then applying an anterior frame external fixator.
6
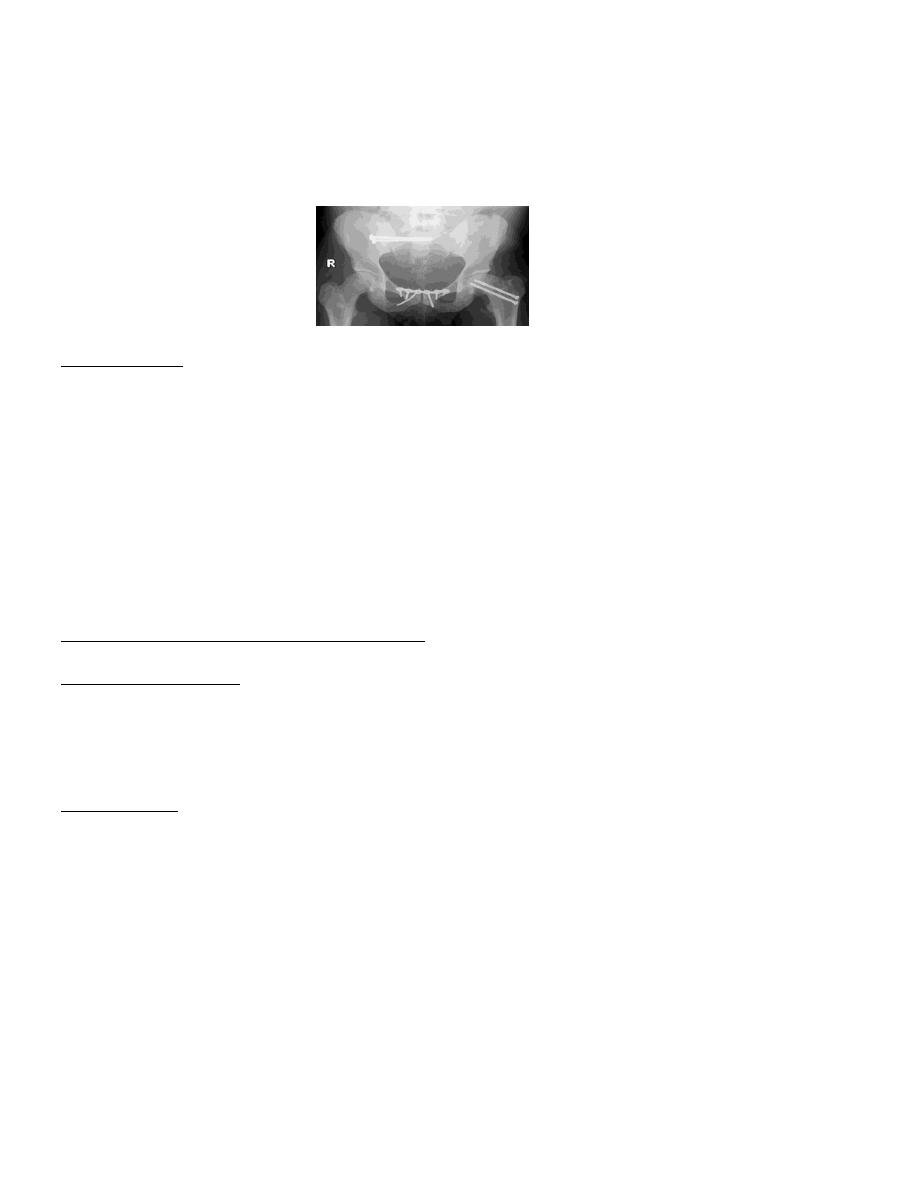
For APC-III & VS Can be treated by skeletal traction on the lower limb to reduce the
vertical displacement combined with external fixator or by anterior plate &screw
fixation of symphysis pubis with posterior screw fixation of the sacroiliac joint.
Complications
Early complications: Severe bleeding & shock. Sepsis & Nerve injury involving
injury to the branches of the lumbar & sacral plexus & sciatic nerve. Visceral injuries
(bladder, urethra &rectum).
Late complications: Urogenital problems; urethral injuries sometime result in
stricture, incontinence or impotence & Persistent sacroiliac pain which may require
arthrodesis of sacroiliac joint.
Fracture of the acetabulum
Mechanism of injury
It is caused either by a blow on the side (as in a fall from height) or by a blow on the
front of the knee (as in dashboard injury) usually the head of the femur is driven into
the pelvis.
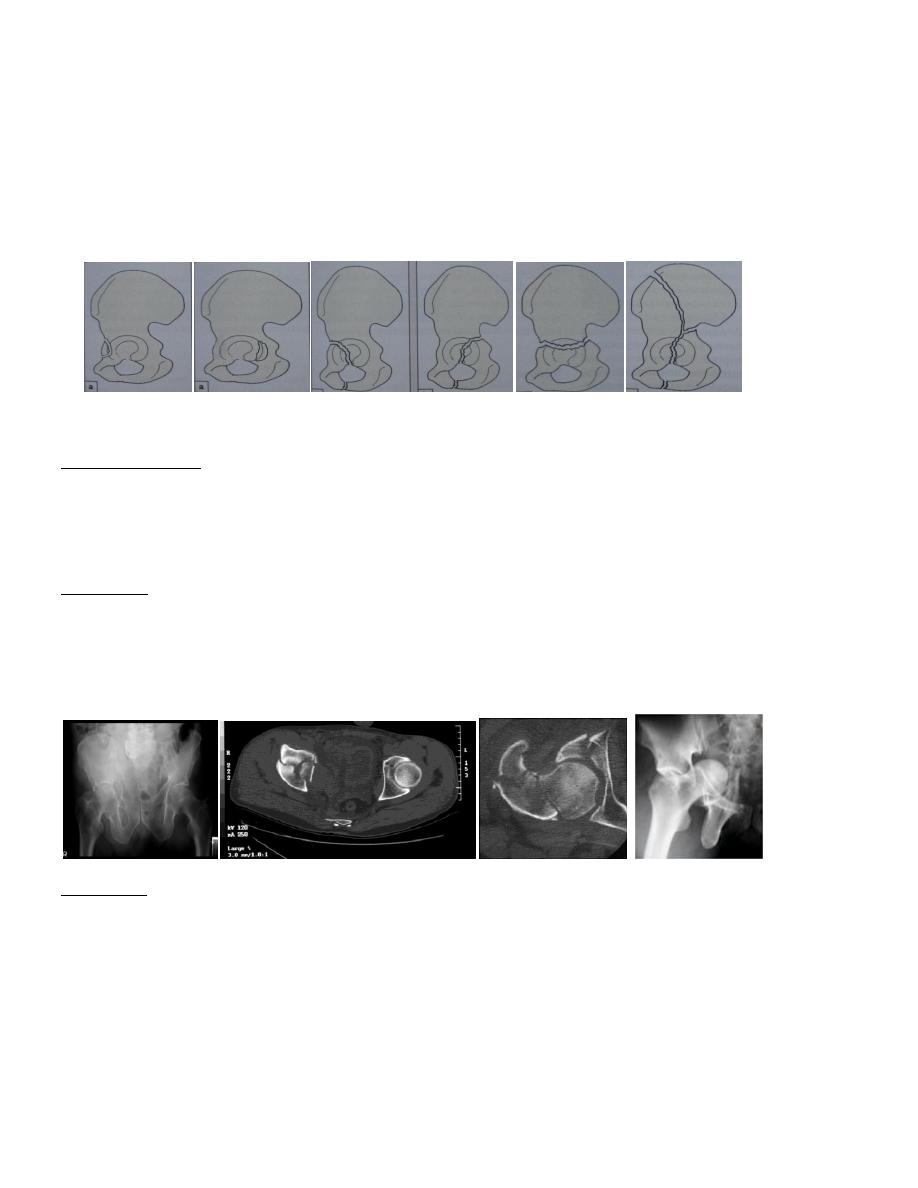
Classification According to Tile’s classification it is divided into 4 types:
Type –I; Acetabular wall #, involve the anterior or posterior part of the acetabular
rim, these #s affect the depth of the socket & may lead to hip instability.
Type-II ; Acetabular column # ,either anterior or posterior column #
*Anterior column extend from symphysis pubis along the superior pubic ramus
across the acetabulum to the anterior part of the ilium
*Posterior column extend from ischium, across the posterior aspect of the acetabular
socket to sciatic notch & the posterior part of the hip bone.
7
Type-III; Transverse #, the # run transversely through the acetabulum, separating
the iliac portion above from the pubic &the ischial portions below. Sometime a
vertical split into the obturator foramen resulting in T- fracture.
Type-IV; Complex #, There is damage to either the anterior or posterior columns
or both, as well as the roof or the wall of the acetabulum.
Acetabular wall # Acetabular column # Transverse # Complex #
Clinical features
There is a severe injury either a fall from height or traffic accident ,the Patient may
be severely shocked ,there may be bruising around the hip, neurological examination
testing Sciatic, femoral, obturator & pudendal nerves.
Imagining
*X-ray; will show the # type, the degree of comminution & the amount of
displacement.
*CT-scan; particularly helpful if surgical treatment is planned.
Treatment
Emergency treatment
The first priority is to treat the shock & reduce the dislocation then traction is applied
through the distal femur, occasionally a lateral traction through the greater trochanter
is needed for central hip dislocation.
8
Definitive treatment
Non operative treatment: By closed reduction with skeletal traction for 6-8 weeks
to unload the articular cartilage &prevent further displacement of the #, it is
indicated in; Acetabular # with minimal displacement (<3mm). Displaced # that
doesn’t involve the roof of the acetabulum. Patient with medical contraindication
to operative treatment including local sepsis.
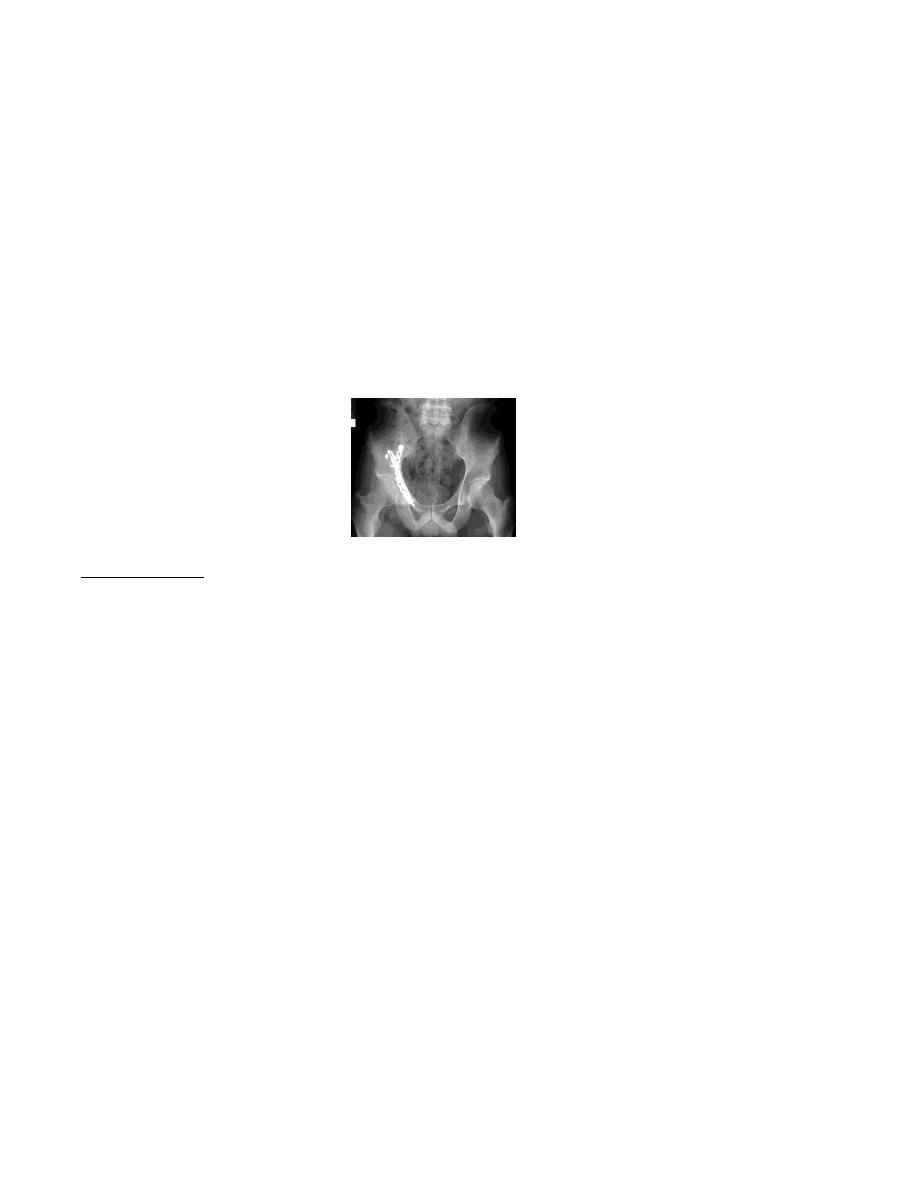
Operative treatment: By open reduction & internal fixation of the #, it is indicated
in; (1)If the dislocation cannot be reduce by close method, (2)unstable hips that
dislocate after close reduction(3) Associated femoral head #.(4) Retained intra-
articular bone fragment.
Complications
• Iliofemoral venous thrombosis.
• Sciatic nerve injury.
• Heterotopic bone formation (myositis ossificans).
• Avascular necrosis of femoral head.
• Loss of joint movement & secondary osteoarthritis.

9