The Shoulder
Dr.Mushtaq Talib Hussein
M.B.Ch.B ,F.I.B.M.S(ortho.),C.A.B.O (ortho.)
CLINICAL ASSESSMENT
S
YMPTOMS
Pain is the commonest symptom. However, ‘pain in the shoulder’ is not necessarily
‘shoulder pain
,
Beware the trap of referred pain. Mediastinal disorders, including
cardiac ischaemia, can present with aching in either shoulder.
Weakness may appear as a true loss of power, suggesting a neurological disorder.
Instability symptoms may be gross and alarming(‘my shoulder jumps out of its
socket when I raise my arm’).
Stiffness may be progressive and severe – so much so as to merit the term ‘frozen
shoulder’.
SIGNS
The patient should always be examined from in front and from behind. Both upper
limbs, the neck, the outline of the scapula and the upper chest must be visible.
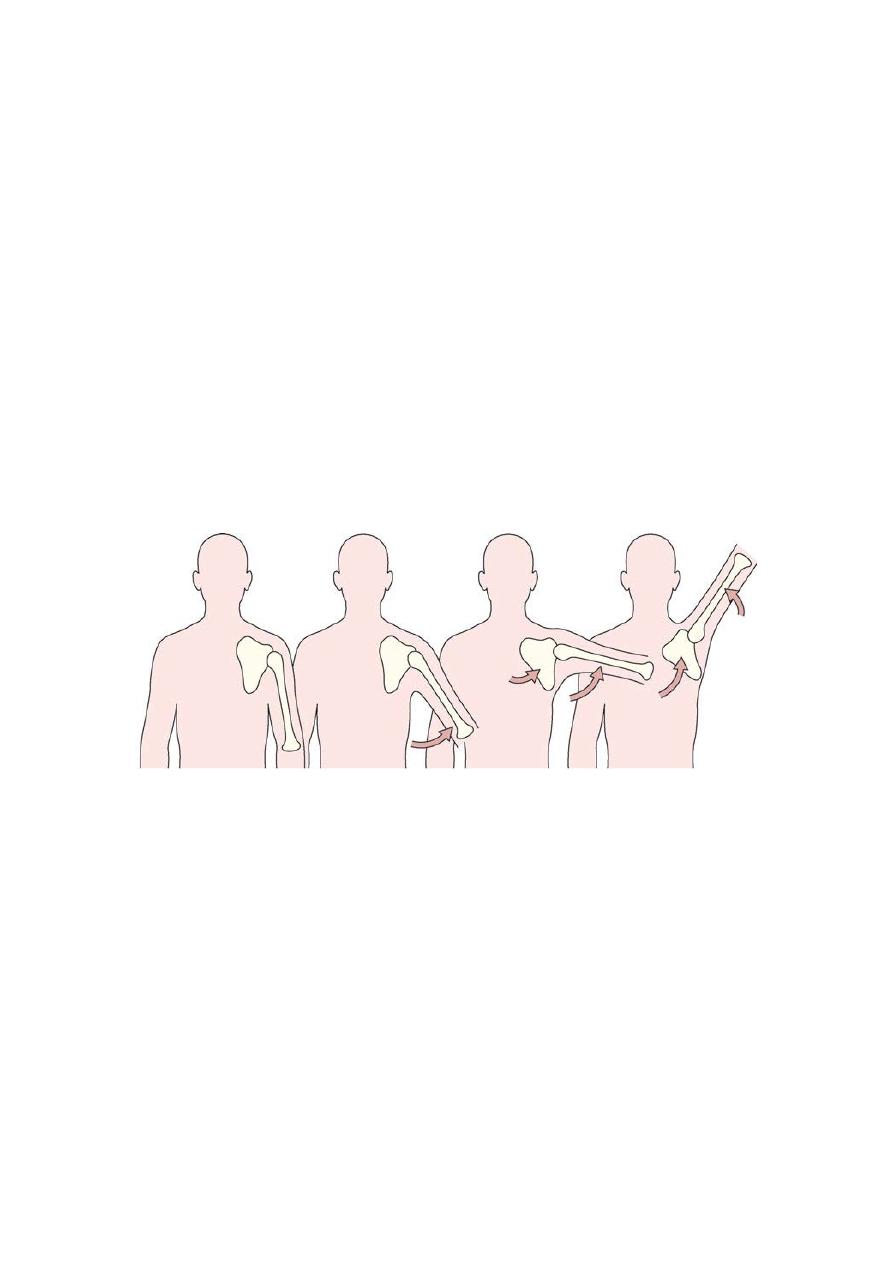
A b c d
Scapulo-humeral rhythm (a–c)
During the early phase of abduction, most of the movement takes place at the gleno-
humeral joint. As the arm rises, the scapula begins to rotate on the thorax (c). In the
last phase of abduction, movement is almost entirely scapulo-thoracic (d).
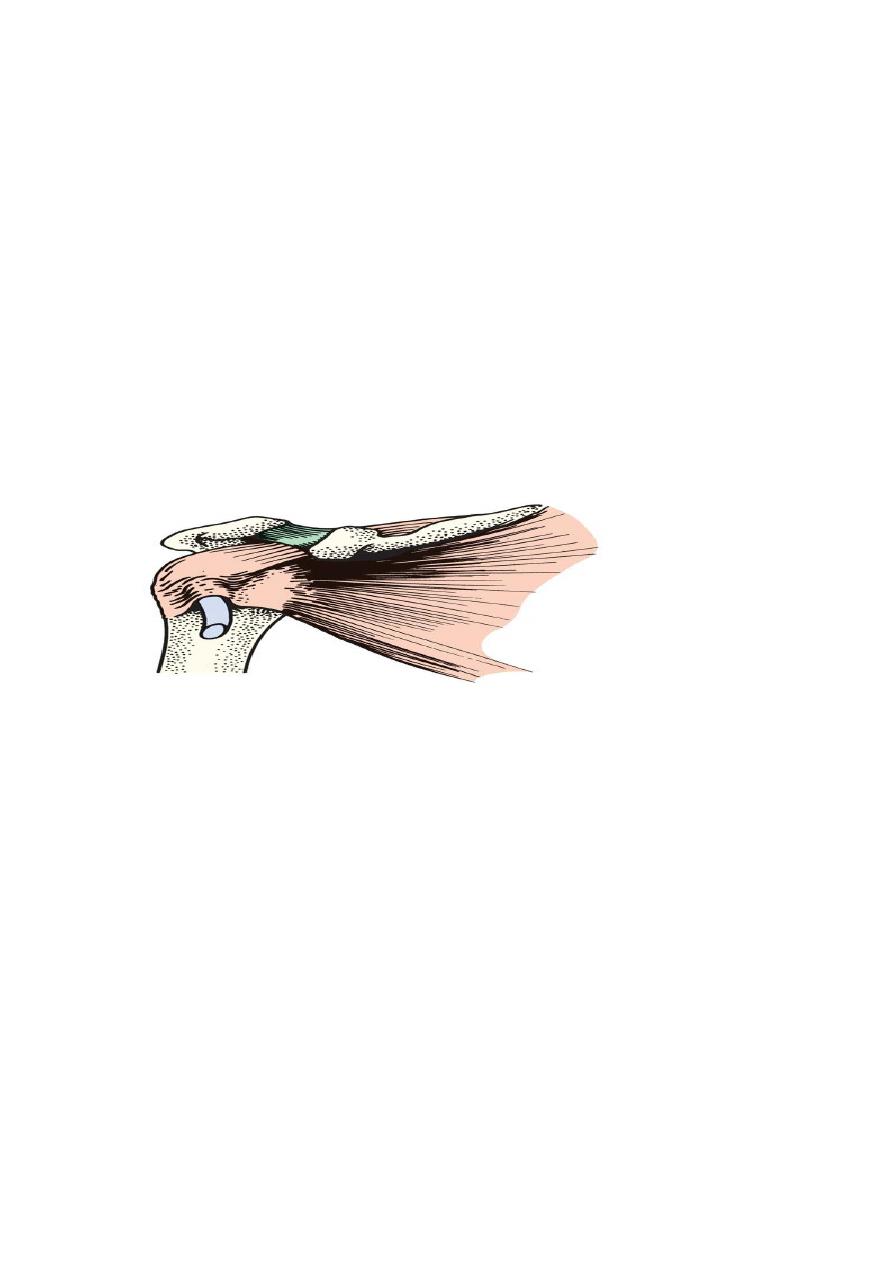
DISORDERS OF THE ROTATOR CUFF
The rotator cuff is made up of the lateral portions of the infraspinatus, supraspinatus
and subscapularis muscles and their conjoint tendon which is inserted into the greater
tuberosity of the humerus.
The main function of the conjoint structure is to draw the head of the humerus firmly
into the glenoid socket and stabilize it there when the deltoid muscle contracts and
abducts the arm.
‘rotator cuff syndrome’, which comprises at least four conditions with distinct
clinical features and natural history:
• supraspinatus impingement syndrome and tendinitis
• tears of the rotator cuff
• acute calcific tendinitis
• biceps tendinitis and/or rupture.
IMPINGEMENT SYNDROME, SUPRASPINATUS TENDINITIS AND CUFF
DISRUPTION
Pathology
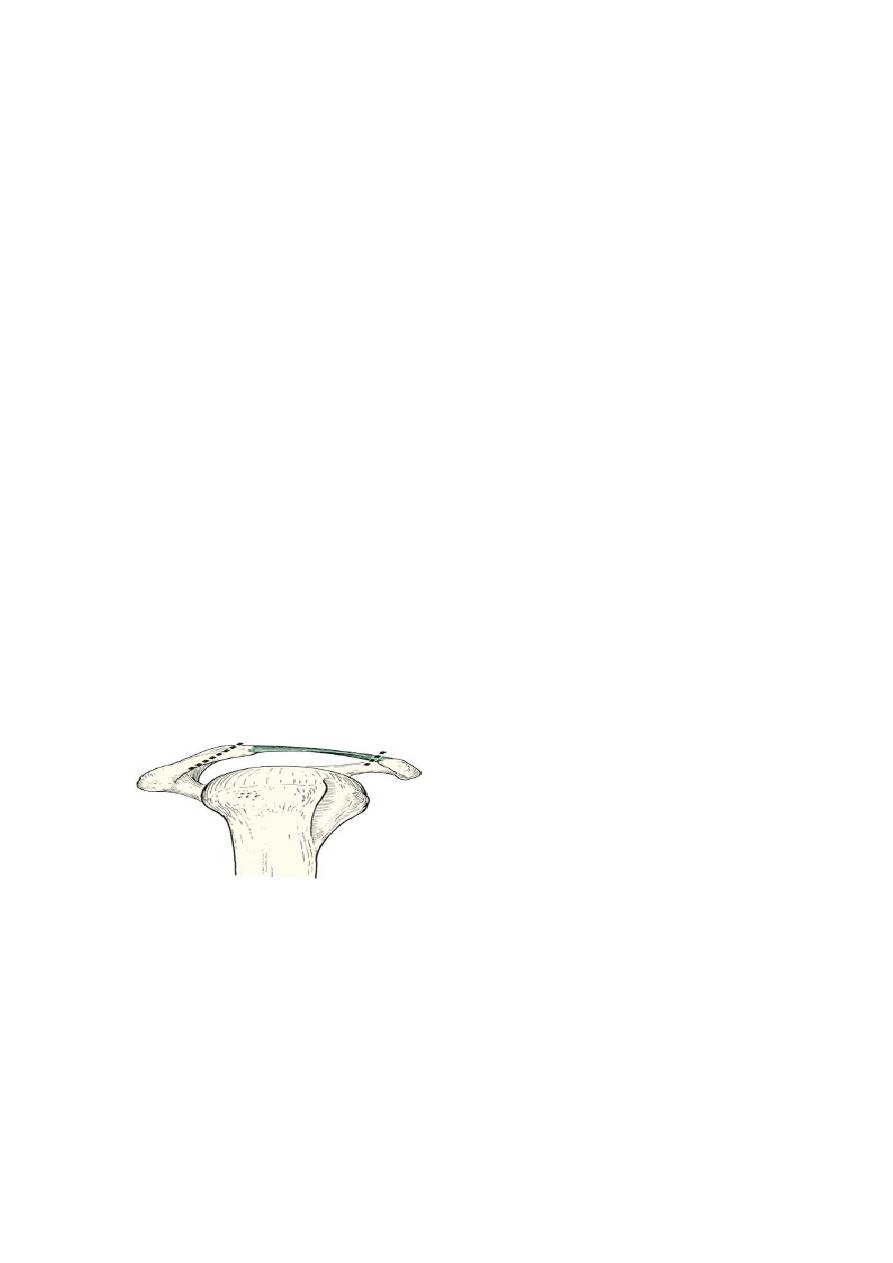
Rotator cuff impingement syndrome is a painful disorder which is thought to arise
from repetitive compression or rubbing of the tendons (mainly supraspinatus) under
the coracoacromial arch.
If the arm is held persistently in abduction and then moved to and fro in internal and
external rotation (as in cleaning a window, painting a wall or polishing a flat surface)
the rotator cuff may be compressed and irritated as it comes in contact with the
anterior edge of the acromion process and the taut coracoacromial ligament.
This attitude (abduction, slight flexion and internal rotation) has been called the ‘
impingement position’
Other factors which may predispose to repetitive impingement are osteoarthritic
thickening of the acromioclavicular joint, the formation of bony ridges or ‘
osteophytes’ on the anterior edge of the acromion, and swelling of the cuff or the
subacromial bursa in inflammatory disorders such as gout or rheumatoid arthritis.
The mildest injury is a type of friction, which may give rise to localized oedema and
swelling (‘tendinitis’). This is usually self-limiting
Sometimes – perhaps where healing is slow or following a sudden strain – the
microscopic disruption extends, becoming a partial or full-thickness tear of the cuff;
CLINICAL FEATURES
Three patterns are encountered:
• Subacute tendinitis – the ‘painful arc syndrome’,
due to vascular congestion, microscopic haemorrhage
and oedema.
• Chronic tendinitis – recurrent shoulder pain due to
tendinitis and fibrosis.
• Cuff disruption – recurrent pain, weakness and loss
of movement due to tears in the rotator cuff.

Subacute tendinitis (painful arc syndrome)
The patient develops anterior shoulder pain after vigorous or unaccustomed activity,
e.g. competitive swimming or a weekend of house decorating. The shoulder looks
normal but is acutely tender along the anterior edge of the acromion.
Subacute tendinitis is often reversible, settling down gradually once the initiating
activity is avoided.
TESTS FOR CUFF IMPINGEMENT PAIN
• The painful arc: On active abduction scapulohumeral rhythm is disturbed and pain
is aggravatedas the arm traverses an arc between 60 and 120 degrees.
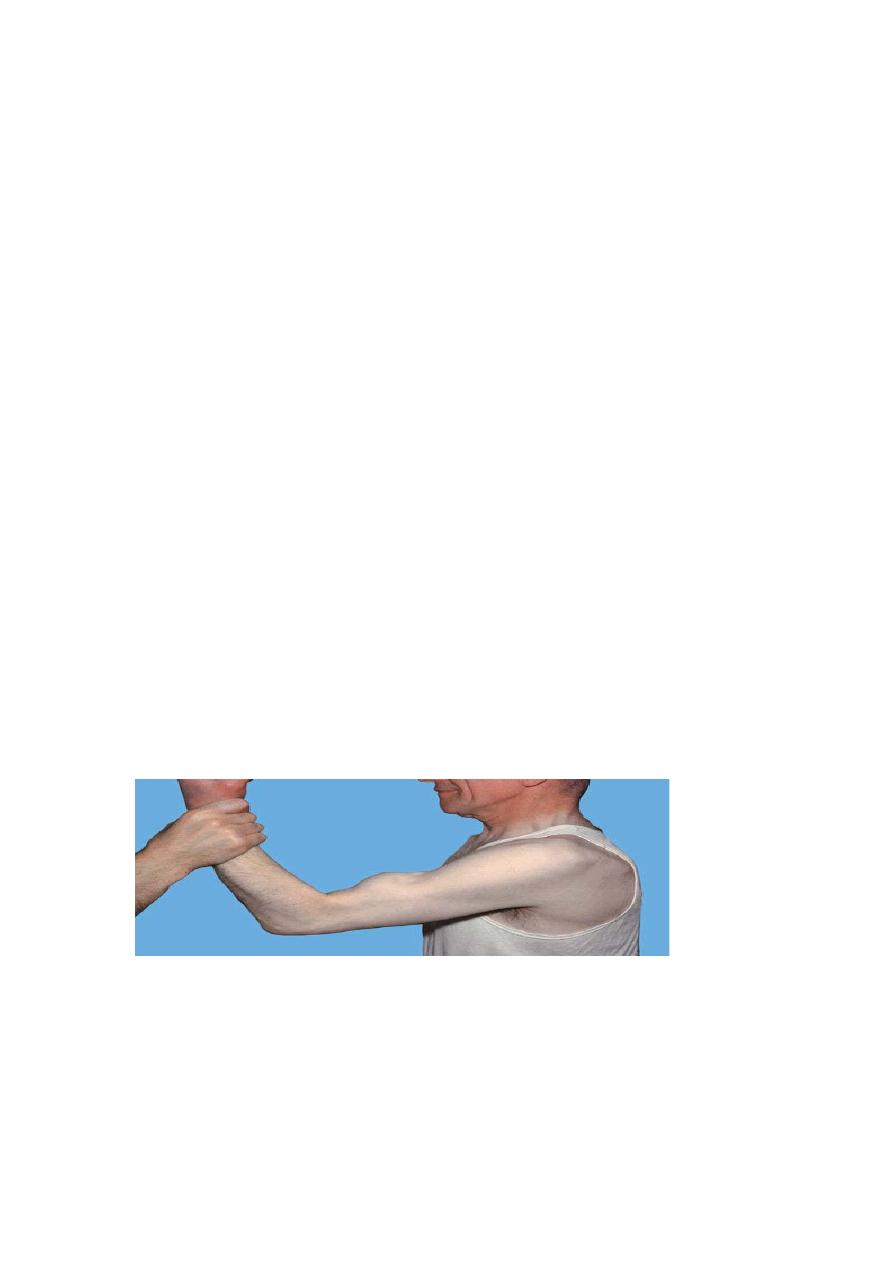
.Neer’s impingement sign: The scapula is stabilized with one hand while with the
other hand the examiner raises the affected arm to the full extent in passive flexion,
abduction and internal rotation, thus bringing the greater tuberosity directly under the
coracoacromial arch. The test is positive when pain, located to the subacromial space
or anterior edge of acromion, is elicited by this manoeuvre.
Neer’s test for impingement: If the previous manoeuvre is positive, it may be
repeated after injecting 10 mL of 1 per cent lignocaine into the subacromial space; if
the pain is abolished (or significantly reduced), this will help to confirm the diagnosis.
Chronic tendinitis
The patient, usually aged between 40 and 50, gives a history of recurrent attacks of
subacute tendinitis, the pain settling down with rest or anti-inflammatory treatment,
only to recur when more demanding activities are resumed.
Characteristically pain is worse at night; the patient cannot lie on the affected side and
often finds it more comfortable to sit up out of bed. Pain and slight stiffness of the
shoulder may restrict even simple activities such as hair grooming or dressing. The
physical signs described above should be elicited.
Cuff disruption
The most advanced stage of the disorder is progressive fibrosis and disruption of the
cuff, resulting in either a partial or full thickness tear. The patient is usually aged over
45 and gives a history of refractory shoulder pain with increasing stiffness and
weakness.
Partial tears may occur within the substance or on the deep surface of the cuff and are
not easily detected, even on direct inspection of the cuff. They are deceptive also in
that continuity of the remaining cuff fibres permits active abduction with a painful
arc, making it difficult to tell whether chronic tendinitis is complicated by a partial
tear.
A full thickness tear may follow a long period of chronic tendinitis, but occasionally
it occurs spontaneously after a sprain or jerking injury of the shoulder. There is
sudden pain and the patient is unable to abduct the arm.
With a complete tear, pain has by then subsided and the clinical picture is
unmistakable: active abduction is impossible and attempting it produces a
characteristic shrug; but passive abduction is full and once the arm has been lifted
above a right angle the patient can keep it up by using his deltoid (the ‘abduction
paradox’); when he lowers it sideways it suddenly drops (the ‘drop arm sign’).
IMAGING
X-ray examination X-rays are usually normal in the early stages of the cuff
dysfunction, but with chronic tendinitis there may be erosion, sclerosis.
MRI effectively demonstrates the structures around the shoulder and gives valuable
ancillary information (regarding lesions of the glenoid labrum, joint capsule or
surrounding muscle or bone).
TREATMENT OF CUFF DISORDERS
Conservative treatment
Uncomplicated impingement syndrome (or tendinitis) is often self-limiting and
symptoms settle down once the aggravating activity is eliminated. Patients should be
taught ways of avoiding the ‘impingement position’. Physiotherapy, including
ultrasound and active exercises in the ‘position of freedom’, may tide the patient
over the painful healing phase. A short course of non-steroidal anti-inflammatory
tablets sometimes brings relief.
If all these methods fail, and before disability becomes marked, the patient should be
given one or two injections of depot corticosteroid into the subacromial space. In most
cases this will relieve the pain,
Surgical treatment
The indications for surgical treatment are essentially clinical; the presence of a cuff
tear does not necessarily call for an operation.
If symptoms do not subside after 3 months of conservative treatment, or if they
recur persistently after each period of treatment, an operation is advisable.
The object is to decompress the rotator cuff by excising the coracoacromial ligament,
undercutting the anterior part of the acromion process, this can be achieved by open
surgery or arthroscopically.
ACUTE CALCIFIC TENDINITIS
Acute shoulder pain may follow deposition of calcium hydroxyapatite crystals,
usually in the ‘critical zone’ of the supraspinatus tendon slightly medial to its
insertion, occasionally elsewhere in the rotator cuff.
The condition is not unique to the shoulder, and similar lesions are seen in tendons
and ligaments around the ankle, knee, hip and elbow.
Clinical features
The condition affects 30–50 year-olds. Aching, sometimes following overuse,
develops and increases in severity within hours, rising to an agonizing climax. After a
few days, pain subsides and the shoulder gradually returns to normal.
X-RAYS
Calcification just above the greater tuberosity is always present.
Treatment
NON-OPERATIVE TREATMENT
Conservative treatment is successful in up to 90 per cent of patients. The main
methods are non-steroidal anti-inflammatory drugs, subacromial injection of
corticosteroids, physiotherapy, extracorporeal shockwave therapy, needle aspiration
and irrigation.
OPERATIVE TREATMENT
While operative treatment is still a controversial issue, there is wide agreement that
surgery is indicated for patients with severe disabling symptoms which have persisted
for more than 6 months and are resistant to conservative treatment.
LESIONS OF THE BICEPS TENDON
Tendinitis
The long head of biceps is subject to tenosynovitis because of its anatomy; the tendon
has a synovial sheath and follows a constrained path in the bicipital groove.
Bicipital tendinitis usually occurs together with rotator cuff impingement; rarely, it
presents as an isolated problem in young people after unaccustomed shoulder strain.
Two manoeuvres that often cause pain are: (1) resisted flexion with the elbow straight
and the forearm supinated (Speed’s test); and (2) resisted supination of the forearm
with the elbow bent(Yergason’s test).
Rest, local heat and deep transverse friction usually bring relief.
Rupture
Rupture of the tendon of the long head of biceps usually accompanies rotator cuff
disruption.
The patient is usually aged over 50. While lifting he or she feels something snap in
the shoulder and the upper arm becomes painful and bruised. Ask the patient to flex
the elbow: the detached belly of the biceps forms a prominent lump in the lower part
of the arm.