1
NEONATOLOGY
Definitions:
A newborn baby from birth to age 28 days .
:
Neonate
if born after 37
(full term)
A baby at term
:
Term baby
weeks gestation and before 42 weeks gestation.
delivered
infant
Live born
:
baby
(Premature)
Preterm
before 37 weeks from the first day of the last menstrual
period. Those born before 28 weeks of gestation are
called (extreme prematurity).
born after 42 weeks gestation .
An infant
:
Post term
:
)
.
W
.
B
.
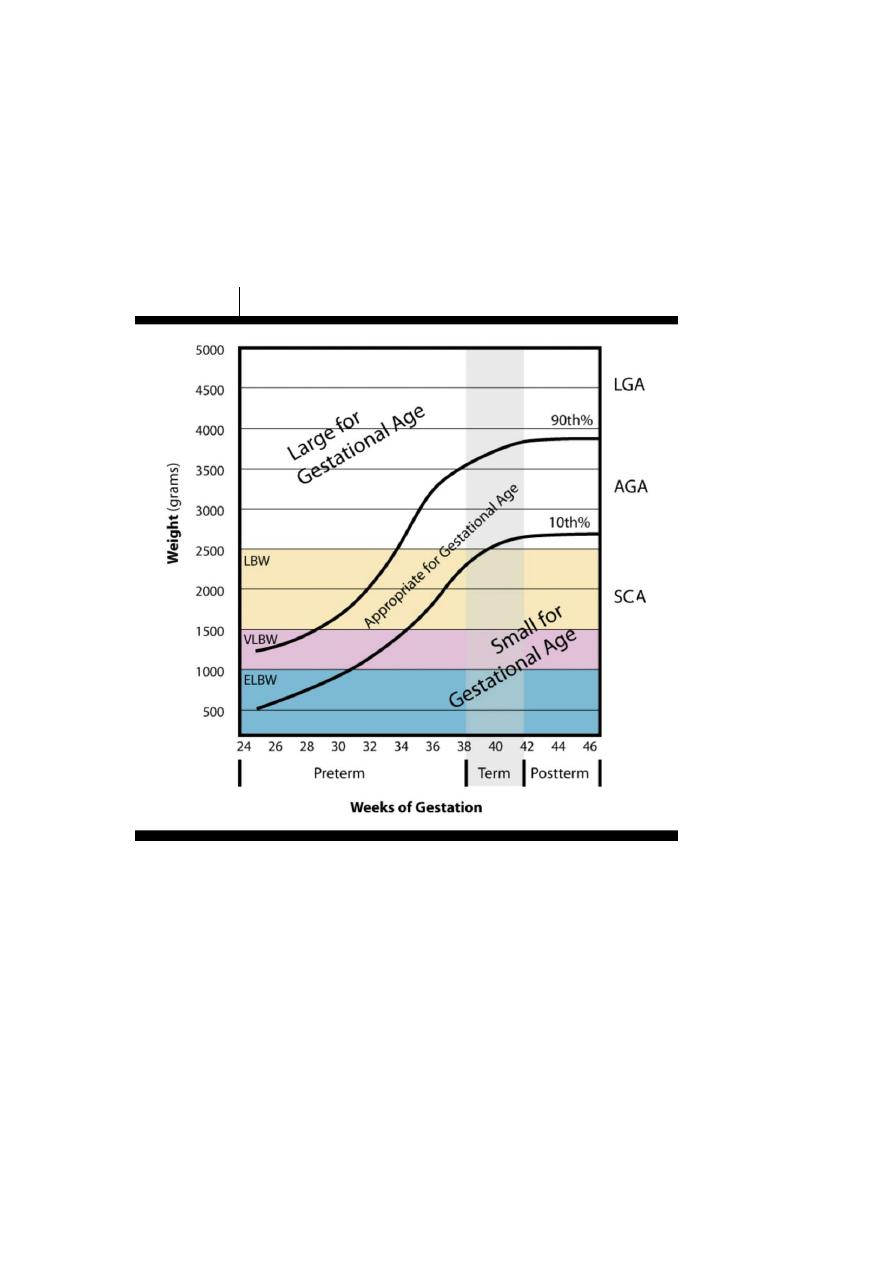
Low birth weight ( L
An infant whose birth weight is 2500g. or less.
Not all preterm infants are L.B.W. and not all L.B.W.
infants are preterm.
:
(V.L.B.W.)
Very low birth weight
Birth weight is 1500g. or less .
:
)
.
W
.
B
.
L
.
h weight (E
Extremely low birt
Birth weight is 1000 g. or less .
:
small for date
or
(S.G.A.)
Small for gestational age
Birth weight is below the 10
th
. percentile for gestation.

2
:
)
.
A
.
G
.
Large for gestational age (L
.
percentile for age
.
th
90
the
Birth weight is greater than
:
rate
tal mortality
Neona
The number of deaths of infants in the period from birth
to 28 days of life and is expressed per 1000 of live births.
:
)
.
U
.
C
.
I
.
(N
Unit
are
Intensive C
Neonatal
The provision of life support systems such as assisted
ventilation , monitoring of heart rate ,respiratory rate,
blood gases, & total parenteral nutrition(T.P.N.).
.
3
:
(N.B.B.)
Examination of the Newborn Baby
- All newborns should be examined at least twice; one soon
after birth, and the other on the fifth day. The question to be
answered” is the infant normal ? In the first examination,
you are restricted to elicit gross physical abnormalities, even
mild anomalies should be explained to parents to allay
anxiety. The baby should be kept warm during the
examination.
- A normal newborn should pass stool within 48-72 hours
and urine within 24 hours after birth.
- General examination: The infant should cry lustily at
birth; weak cry may indicate severe respiratory distress,
sepsis, hypotonia or birth asphyxia, while a high pitched cry
(cerebral cry or shrill) may indicate increased intracranial
pressure.

4
- A constant low pitched inspiratory stridor is heard in
congenital laryngomalacia which resolves by 12-18
months.
.
cold and hot weather
,
is seen in polycythemia
Plethora
-
The skin is covered by a greasy material secreted by
epithelial cells called vernix caseosa which protects the skin
from the effect of the amniotic fluid.
.
- Occasionally, one half of the body may appear red and the
other half is pale (harlequin color change) which is usually
.
transient and of unknown significance
5
6
- Cyanosis :Central cyanosis is pathological and peripheral
or acrocyanosis is normal( more in the preterm babies).
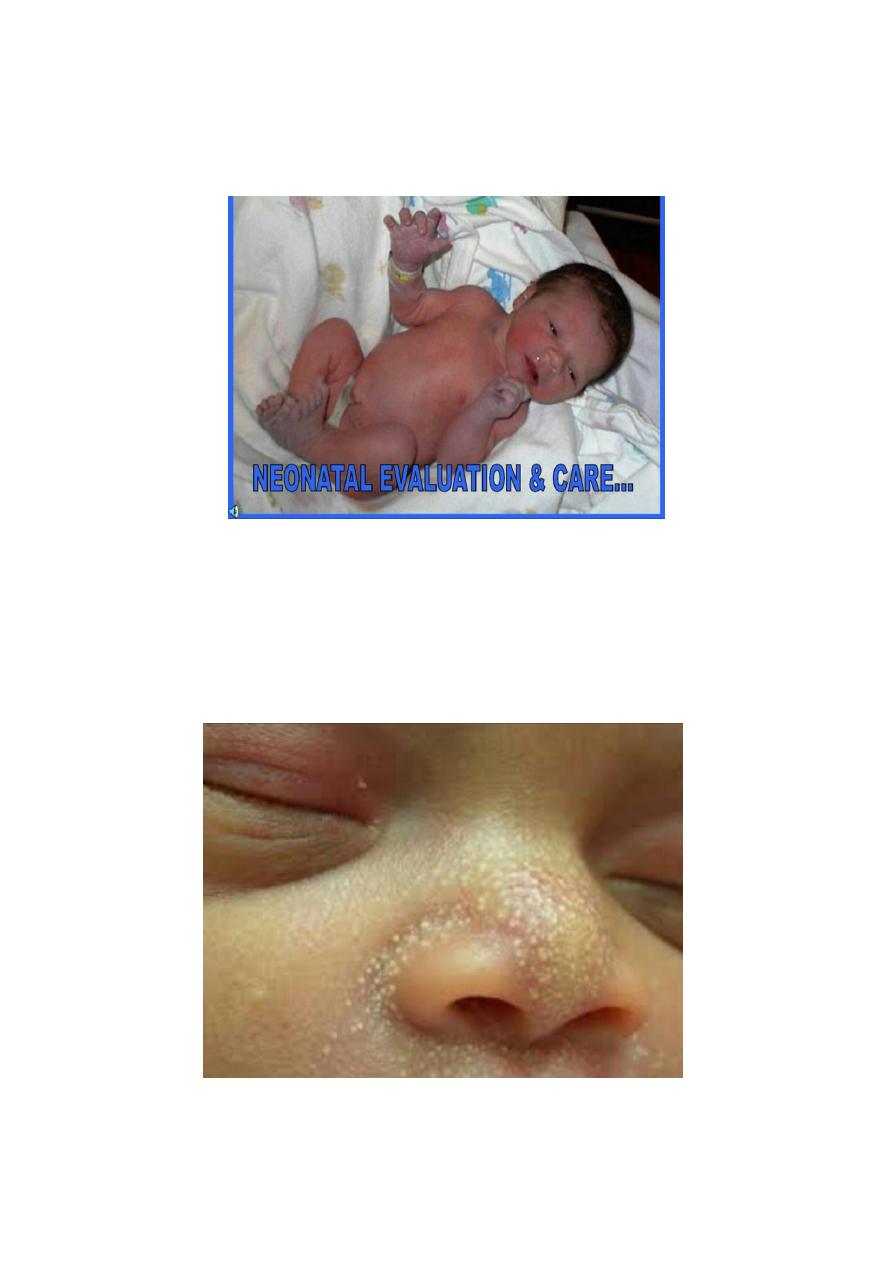
-Milia: Small sebaceous cysts, pinpoint in size, whitish
spots seen on the nose, cheeks and forehead, it disappears in
a few weeks spontaneously, it is a normal finding.

7
-Erythema toxicum neonatorum : red blotchy, macular
patches with a white center seen all over the body,
sparing the soles and palms. It affects 50% of full term
infants, less common in preterm infants. Pustules may be
seen in the center containing eosinophils.
They usually appear on the first few days and disappear
.
spontaneously
8
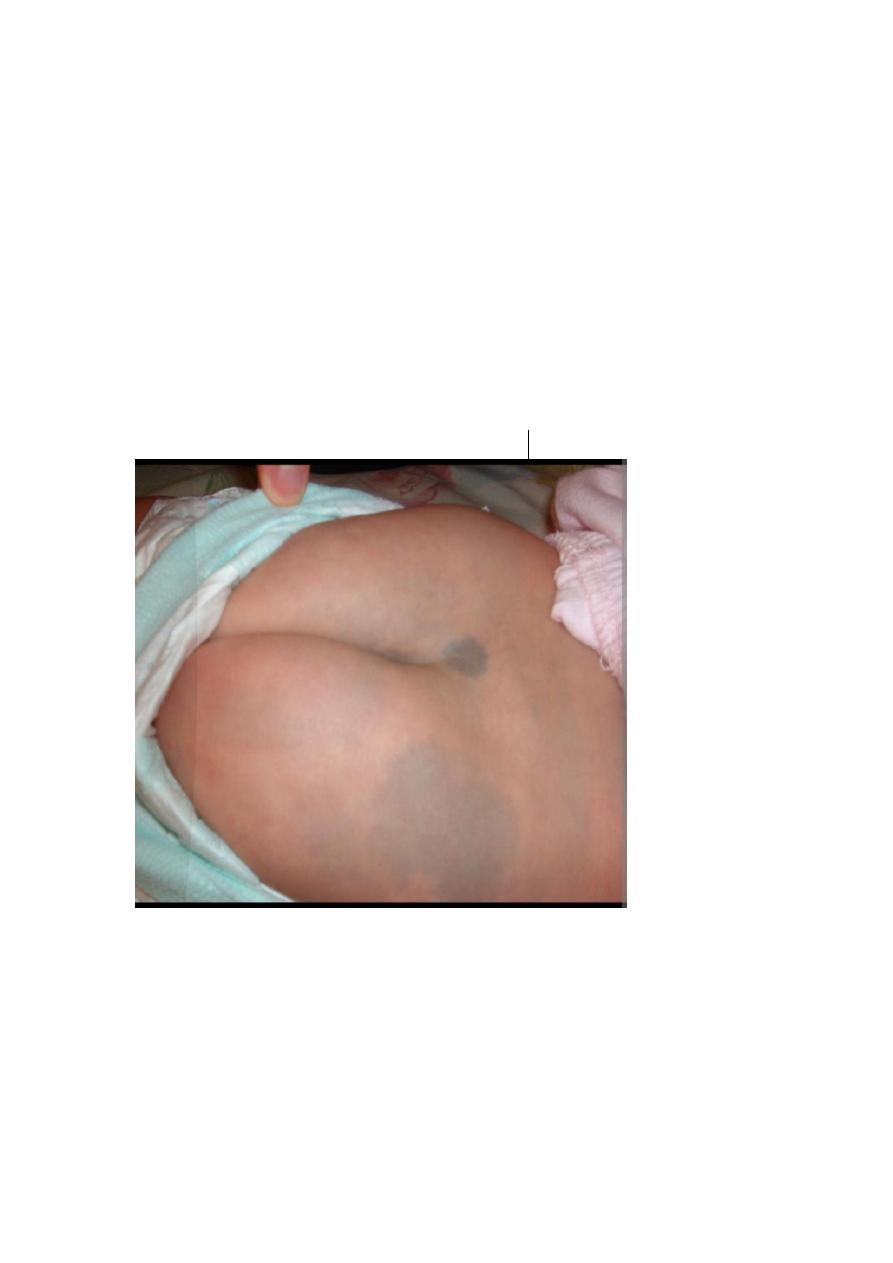
- Mongolian spots: blue, gray, flat, macular lesions seen
normally over the sacrum, sometimes on the upper back,
legs, hands and rarely on the face.
They may be solitary, numerous or patchy.
They are seen in colored children much more than whites.
They usually fade during the first few years of life.
.
be misdiagnosed as bruises
They may
9
-
- Occipito-Frontal Circumference ( O.F.C.):
Average head circumference at birth is 35cm.
-
Weight:
average weight 3.5 kg, neonates lose 5-10%
birth weight in the first few days of life and regained by
by10days.
Length: average length of the newborn baby is 51cm.
-
Fontanelles:
-
The average diameter of the anterior fontanelle is 3 cm, it
closes at 9-18 months. The posterior fontanelle measures
about the tip of the finger usually closes by 3 months of age.

11
-Examination of the eyes:
Edema of the upper eyelids is a result of birth process.
Conjunctival and scleral hemorrhages are commonly seen
and disappear by time.
Look for cataract and glaucoma (megalocornea).
- Epstein pearls : are cysts containing keratin located on the
.
soft and hard palate
-Capillary hemangioma:
is commonly seen on the upper eyelids and forehead,
it disappears in the first year.
11
The breasts might be large in both sexes, this is caused by
maternal hormones and is usually evident on day 2 or 3 of
life, they may persist for a month.
Milk may be expressed from it by parents (witches milk),
this habit should be avoided because it may lead to abscess
(neonatal mastitis).
- Hips: examine hips for dysplasia(dislocation).
- Femoral artery: palpate both femorals by the index
fingers in the mid inguinal region, their absence indicates
coarctation of the aorta.
- CNS: Neonates may sleep up to 20 hours out of 24 hours if
left undisturbed.
Check activity, primitive (neonatal) reflexes, convulsions or
apnea.
:
LOW BIRTH WEIGHT BABIES
(Normal Birth Weight:2500-4000g.)
Definition of L.B.W.: A birth weight less than 2.5Kg.
They are 20 times more likely to die than normal infants & it
can affect the life of the individual by increasing diseases like
diabetes mellitus, hypertension, and C.V. diseases.
LBW is an indicator of public health status and is a cause of
70% of neonatal deaths.
Maternal causes of LBW:
1-Previous LBW
2-Poverty.
3-Low level of education.
4-No antenatal care.
5-Maternal age: <16 & >35 years.
12
6-Unspaced pregnancy.
7-Smocking,alcohol,drugs.
RETARDATION(I.U.G.R.):
INTRAUTERINE GROWTH
Definition:
Fetal growth below the 10
th
.centile for gestational age
and abdominal circumference is below 2.5
th
centile.
So S.G.A. is a statistical definition, while IUGR is a
clinical definition (clinical evidence of malnutrition).
CAUSES of IUGR:
Causes:
etal
a.F
1-Congenital infections.
2-Chromosomal abnormalities.
3-Congenital malformations.
4-Twin to twin transfusion.
Placental causes:
b.
1-Chronic abrutpio placentae.
2-Placental insufficiency.
3-Placental infarction.
).
cause
he commonest
(t
Constitutional
c.
The majority of cases are normal but small, and the
diagnosis is made after delivery by exclusion.
Maternal causes:
d.
1-Hypertension,D.M.,chronic illnesses.
2-Pre-eclampsia.
3-Malnutrition.
4-Smoking,alcohol,teratogens.
5-Short stature.
13
Problems of IUGR:
Treatment of I.U.G.R. :
1-Give more calories.
2-Monitor blood sugar level 2-4 hourly until it is stable.
3-Monitor serum calcium level.
Outcome of IUGR:
1-Most of them have normal growth in infancy and childhood.
2-Many are born prematurely.
3-Defective mental development.
Fetal death.
-
-Temperature instability.
-Perinatal asphyxia (the most important
problem).
Hypoglycemia, Hypocalcemia.
-
Polycythemia.
-
Congenital anomalies.
-
14
:
PREMATURITY
The problems of prematurity are due to poor
adaptation to extra uterine life due to immaturity of
organs:
Respiratory problems:
a-R.D.S.(respiratory distress syndrome).
b-Chronic lung disease: B.P.D.(bronchopulmonary
dysplasia).
c-Apnea.
Neurologic problems:
a-Hypoxic-ischemic encephalopathy(H.I.E.).
b-Intraventricular hemorrhage(I.V.H.).
c-Convulsions.
Cardiovascular complications:
a-Hypotension.
b-P.D.A.(patent ductus arteriosus).
Hematologic:
a-Anemia.
b-Hyperbilirubinemia.
c-Organ hemorrhage.
d-D.I.C.
Nutritional problems (especially in those born before
32 weeks of gestation).
G.I. problems (N.E.C. : necrotizing enterocolitis).
Metabolic:
Hypoglycemia, Hypocalcemia.
Renal problems :low G.F.R.

15
Temperature regulation e.g. hypothermia.
Ophthalmologic e.g. R.O.P.(retinopathy of prematurity).
MANAGEMENT OF THE PREMATURE INFANT :
1-Delivery: should be in a hospital well equipped with
resuscitation tools and highly experienced staff.
2-Neonatal management:
a-Thermal regulation either by overhead radiant warmer
or an incubator. The accepted skin temperature is
36-36.5c.
b-Oxygen therapy and assisted ventilation.
c-Fluid and electrolytes therapy.
d-Nutrition: enteral, N.G. tube or parenteral.
e-Management of hyperbilirubinemia.
f-Control of infections.
LONG TERM PROBLEMS OF PREMATURITY:
1-Poor growth and development.
2-R.O.P.
3-B.P.D.
4-Increased rate of post neonatal illnesses.
5-Increased frequency of congenital anomalies.
Immunizations:
The timing of immunizations of premature babies is
based on the infant's chronologic age, not on the
gestational age.
It may be advisable to delay administration of hepatitis B
vaccine until the infant weighs 2000 g. or more.
The full doses of all immunizations should be given.

16