


• Mosul university- College of dentistry-oral & maxillofacial surgery department
• Dr.Ziad H. Delemi• B.D.S, F.I.B.M.S (M.F.)
• DENTALMANAGEMENTOF THE MEDICALLYCOMPROMISED PATIENT
• Sexually Transmitted Diseases
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• 1- STD are transmitted by intimate contact that can result in oral manifestations.• 2-some STD can be transmitted by direct contact with lesions, blood, or saliva.
• 3-STD exhibit antimicrobial resistance.
• 4-some STD are incurable,but all are preventable.
• 5-dental health care workers can be an important component of STD control by providing diagnosis, education, and treatment.
• STDs have important implications for dentistry:
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• NEISSERIA GONORRHOEAE
• It is a G-ve diplococci
• aerobic microbe that replicates easily in warm, moist areas. It is a fragile bacterium that is readily killed by drying, so it is not easily transmitted by fomites. It develops resistance to antibiotics
• Majority of infections are asymptomatic
• Dx ???? culture
• Rx ???? ceftriaxone 125 mg IM
• cefixime 400 mg PO
• Can cause purulent conjunctivitis of the newborn
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• NEISSERIA GONORRHOEAE
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• SYPHILIS• Caused by spirochete Treponema pallidum
• Screening ???? VDRL nonspecific
• Dx ???? Dark field microscopy
• ???? Serological tests ???? become +ve 4-6 weeks after exposure
• Incubation period 10-90 days
•

• Mosul university- College of dentistry-oral & maxillofacial surgery department
• PRIMARY SYPHILIS• Chancre ???? Painless ulcer
• Forms at the site of entry
• Solitary
• 3 weeks after sexual contact
• Heals spontaneously in 2-4 weeks
• Inguinal Lymphadenopathy
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• PRIMARY SYPHILIS•
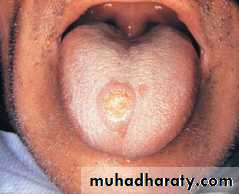

• Chancre
• Chancre• Mosul university- College of dentistry-oral & maxillofacial surgery department
• SECODRY SYPHILIS• Due to hematogenous dissemination of spirochetes
• 6wk-6mon after the 1ry chancer, Lasts for 2-6 wk
• fever, Arthralgia & malaise, generalized Painless lymphadenopathy, & patchy hair loss
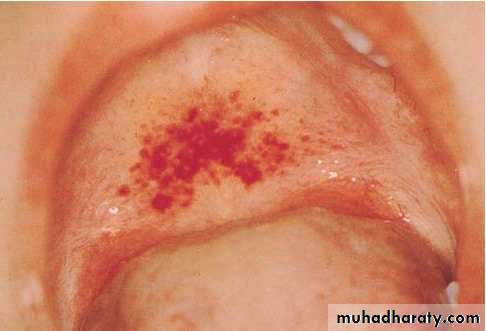
• Maculopapular rash over the skin & mucous membranes
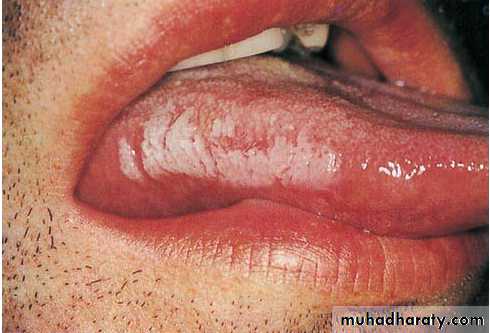
• Oral ulceration (snail tracked)
• Vulvar lesions ???? Mucous patches
• Condyloma latum ???? raised, flattened grayish-
• white lesions
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• SECODRY SYPHILIS

• rash

• Oral ulcer
• Mosul university- College of dentistry-oral & maxillofacial surgery department• TERTIARY SYPHILIS
• 1- oral lesions consist of diffuse interstitial glossitis & the Gumma. Interstitial glossitis should be considered a premalignant condition. The tongue may appear lobulated & fissured with atrophic papillae, resulting in a bald & wrinkled surface. Leukoplakia frequently is present. The oral gumma is a rare lesion that most commonly involves the tongue & palate. It appears as a firm tissue mass with central necrosis. Palatal gummas may perforate into the nasal cavity or maxillary sinus.
• 2- Neurosyphilis.
• 3-CVS ???? Aortic aneurism
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• Congenital Syphilis• After the 16th week, because before this time, the placenta prevents transmission of bacteria.
• The sequelae of early infection include osteochondritis, periostitis (frontal bossing), rhinitis, rash, & ectodermal changes. Syphilis contracted during late pregnancy may involve bones, teeth , eyes, cranial nerves, viscera, skin, & mucous membranes. A classic triad of congenital syphilis known as Hutchinson's triad includes interstitial keratitis of the cornea, eighth nerve deafness, &dental abnormalities (i.e., Hutchinson's incisors &mulberry molars).
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• Congenital Syphilis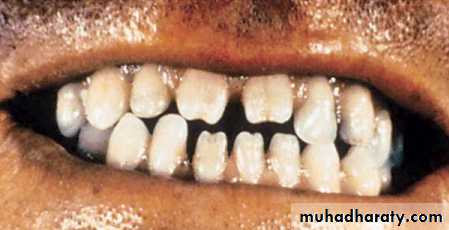
• Hutchinson's incisors
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• TREATMENT• 1RY , 2RY & first year of the latent phase
• Benzathine Penicillin G 2.4 million units IM
• Pt. allergic to penicillin ???? Doxycyclin 100 mg BD
• ???? 14 days
• Latent syphilis patients ???? Chest X- ray
• Lumbar puncture
• Tertiary syphilis & latent syphilis > 1Y
• Benzathine Penicillin G 2.4 M U ???? IM ???? weekly ????
• 3 successive weeks
• OR Doxycyclin 100 mg PO BD ???? 28 days
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• HERPES• HSV belongs to a family of eight human herpes viruses that includes cytomegalovirus, Epstein-Barr virus, varicella-zoster virus, human herpesvirus type 6 (HHV-6), human herpesvirus type 7 (HHV-7), and Kaposi's sarcoma–associated herpesvirus (HHV-8).
• HSV-1 is the causative agent of most herpetic infections that occur above the waist, especially on the mucosa of the mouth (herpetic gingivostomatitis, herpes labialis), nose, eyes, brain, and skin. Infection with HSV-1 is extremely common; most adults demonstrate antibodies to this virus. Transmission usually occurs through close contact, such as touching or kissing, and transfer of infective saliva. HSV-1 also is transmitted via sexual contact.
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• HERPES• 1-PRIMARY (FIRST) INFECTION ???? multiple vesicles which will ulcerate forming shallow superficial ulcers over the affected facial skin or external genitalia.
• 2-SECONDARY (RECURRENT ) HERPES
• The viruses that are already present in the nerve cells will be reactivated by various stresses such as generalized illness, menses, emotional stress or trauma
• It is less painful, circumscribed, not associated with generalized symptoms & lasts an average of 7 days
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• HERPES


• herpes labialis
• herpetic whitlow
• Primary herpetic gingivostomatitis
• Mosul university- College of dentistry-oral & maxillofacial surgery department• HERPES
• Dx Viral culture of a suspicious lesion
• Blood test for detection of antibodies ???? helpful to
• Dx asymptomatic individuals or to confirm a past
• infection
• Rx Acyclovir 200mg orally 5 times /day for 10 days
• ???? ⭣ duration of ulcerative lesions
• Improve the symptoms
• Used for 1ry infection
• -2ry infection ???? no Rx
• -Supportive care ???? keeping the area clean & dry
• xylocaine jelly
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• Pathophysiology & Complications
• Infection arises from intimate contact with a lesion or infective fluid (e.g., saliva). Epithelial cells are invaded, and viral replication occurs. With cellular destruction come inflammation and increasing edema, which result in formation of a papule that progresses to a fluid-filled vesicle. These vesicles rupture, leaving an ulcerated or crusted surface.
• Lymphadenopathy and viremia are prominent features. In normal individuals, the infection is contained by usual host defenses and runs its course within 10 to 20 days.
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• Pathophysiology and Complications• However, spread to other epidermal sites (e.g., herpetic whitlow [infection of the fingers], keratoconjunctivitis [eyes]) in neonates during childbirth. In rare cases, infants and immunosuppressed persons can develop systemic (meningitis)During the epithelial infection, progeny enter the ends of local peripheral neurons and migrate up the axon to the regional ganglion (HSV-1 primarily in the trigeminal, and HSV-2 primarily in the sacral), where they reside. After stimulation such as trauma, wind, surgery, and stress, sunlight, menses, or intercourse, the virus reactivates, migrates down the axon, and produces recurrent infection with lesions similar to the primary, but less severe in nature and more localized.
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• Shingles, is characterized by a painful skin rash with blisters in a limited area on one side of the body. The initial infection with varicella zoster virus (VZV) causes the acute (short-lived) illness chickenpox.In an immunocompromised individual, perhaps years or decades after a chickenpox infection, the virus may break out of nerve cell bodies and travel down nerve axons to cause viral infection of the skin in the region of the nerve. The virus may spread from one or more ganglia along nerves of an affected segment and infect the corresponding dermatome causing a painful rash.• Herpes zoster
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• Herpes zoster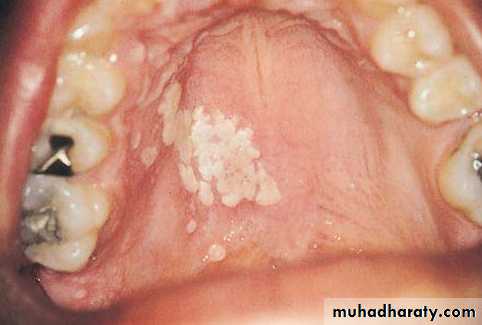
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• is an infection that is caused, by the Epstein-Barr virus (EBV), a lymphotropic herpesvirus. Other viruses may also produce features of acute infectious mononucleosis. It produces the classic clinical triad of fever, pharyngitis, & lymphadenopathy. Transmission of the virus occurs primarily by way of the oropharyngeal route during close personal contact (i.e., intimate kissing). Children, adolescents, & young adults are most commonly affected.• INFECTIOUS MONONUCLEOSIS
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• INFECTIOUS MONONUCLEOSIS
• Infectious mononucleosis
• Mosul university- College of dentistry-oral & maxillofacial surgery department• HUMAN PAPILLOMA VIRUS
• The most common STD
• It causes recurrent life long infection
• It causes Condylomata lata of palate
• It causes genital warts ???? Condyloma accuminata ???? may involve the perineum, vulva, vagina
• There is an association between HPV α Cervical carcinoma
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• HUMAN PAPILLOMA VIRUS


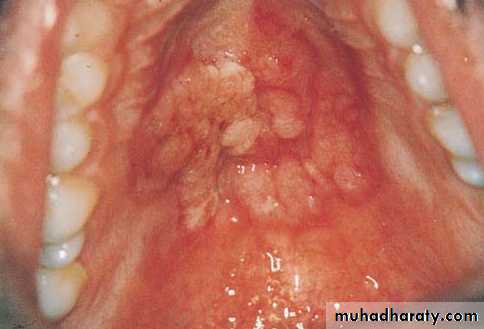
• Condylomata lata on the palate
• Mosul university- College of dentistry-oral & maxillofacial surgery department• Dental Management of the Patient With a STD
• • Gonorrhea: Little threat of transmission to dentist; oral lesions are possible
• • Syphilis : Untreated primary & secondary lesions infectious; blood also is potentially infectious.
• • Genital herpes: Little threat of transmission to dentist; oral lesions (possible from autoinoculation) are infectious.
• • HPV infection: Little threat of transmission to dentist; oral lesions are possible.
• Persons with STD are at risk for human immunodeficiency virus (HIV) infection.
• The dental management of patients with an STD begins with identification. Because they are potentially infectious, the obvious goal is to identify all individuals who have active disease. Unfortunately, this is not possible in every case because some persons will not provide a history or may not demonstrate significant signs or symptoms suggestive of their disease. The inability of clinicians to identify potentially infectious patients applies to other diseases as well, such as HIV infection and viral hepatitis. Therefore, it is necessary for all patients to be managed as though they were infectious.
• Dental Management of the Patient With a STD
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• AIDS• human immunodeficiency virus “HIV” , RNA virus, 2types HIV1, HIV2
• The virus has a predilection for cells of the immune system ???? T helper lymphocytes with CD4 marker, Monocytes
• ???? Breakdown of the body’s immune system
• Particularly “ cell mediated immunity”
• Genital ulcer disease ???? ↑ transmission of HIV
• Most cases of HIV are asymptomatic
• Transmitted by ???? Blood ???? IV drug users, hemophilia
• Sexually ???? homosexuals, heterosex
• Vertical transmission & breast milk
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• Generally, when the CD4 count drops to below 200, the patient is susceptible to several opportunistic infections, including P carinii pneumonia,toxoplasmosis,influenza, histoplasmosis, cytomegalovirus (CMV) infection,& mucocutaneous diseases such as candidiasis. neoplasms also may appear during AIDS.
• In saliva & tears low conc. Insufficient for infection
• Weak virus easily sterile by boiling &chemicals except gamma & dry heat
• AIDS
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• T-helper (CD4)>300\mm3, if > 200 mm3 \AIDS• Serological tests for antibodies
• Majority of infected Pt ???? produce Ab within 3 M
• Screening test ???? ELISA ???? for antibodies “nonspecific”
• Specific tests ???? Western blot
• PCR “most specific”
• AIDS Diagnosis
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• WHO criteria for AIDS:• Major :
• 1- weight loss >10 %
• 2- chronic diarrhea > 1 month
• 3- prolonged fever > 1 month
• Minor :
• A-persistent cough > 1 month
• B- generalized Pruritus
• C- recurrent herpes zoster, simplex infection
• D-oropharyngeal candidiasis
• E- generalized lymphadenopathy
• AIDS Diagnosis
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• INITIAL EXPOSURE OR INFECTION
• Flulike symptoms—fever, weakness, 10 to 14 days
• Asymptomatic stage
• SYMPTOMATIC STAGE
• Serologic evidence of infection
• T4/T8 ratio reduced to about 1
• Persistent lymphadenopathy
• Oral candidiasis
• Constitutional symptoms—night sweats, diarrhea, weight loss, fever, malaise, weakness
• Signs & Symptoms of HIV Infection
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• Signs & Symptoms of HIV Infection• ADVANCED SYMPTOMATIC STAGE
• Serologic evidence of infection
• T4/T8 ratio suppressed to less than 0.5
• HIV encephalopathy
• HIV wasting syndrome
• Major opportunistic infections
• Neoplasms—Kaposi's sarcoma, lymphoma, carcinoma of rectum
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• Signs & Symptoms of HIV Infection
• Infant with HIV:
• Microcephaly.
• Ocular hypertelorisim.
• Box-like forehead.
• Blue sclera.
• Wide palpepral fissure.
• Pendulous lip.
•

• Mosul university- College of dentistry-oral & maxillofacial surgery department
• Oral manifestations of HIV Infection• 1-Fungal infections:
• Oral candidiasis
• Cryptococcoses
• Histoplasmosis
• 2-Viral infections:
• Oral hairy Leukoplakia
• Herpes simplex stomatitis
• 3-Aphthus ulcer:
• Minor, major , herpetiform
• 4-Xerostomia
• 5-Gingival \perio disease:
• ANUG
• Necrotizing stomatitis
• 6-Neoplastic disease:
• Leukoplakia
• Sq. cell ca.
• Non-Hodgkin lymphoma
• Kaposi sarcoma
• Signs & Symptoms of HIV Infection
• Hairy Leukoplakia

• Kaposi sarcoma of the nose

• Condylomata accuminata of the gingiva
• Mosul university- College of dentistry-oral & maxillofacial surgery department• 1-Consult whenever possible with patient's physician to establish current status; if severe thrombocytopenia is present (<50,000), platelet replacement may be needed before surgical procedures are performed.
• 2-Determine whether prophylactic AB are needed to protect patients with severe immune neutropenia (<500 cells/mm) from postoperative infection.
• 3-Render only more immediately needed treatment for patients with advanced AIDS.
• Dental Management of the Patient With AIDS
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• CLASSIFICATION ACCORDING TO CLINICAL MANIFESTATONS & CD4 COUNT• GROUP A
• Initial viremia stage ???? 4-6 wk
• CD4 count ???? > 200 cells /µL
• Antibodies at a low level
• Acute mononucleosis-like illness or asymptomatic
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• LATENCY PERIOD
• Lasts up to 10 years
• GROUP B
• *Symptomatic but not with initial viremia & not with full blown picture of AIDS
• *CD4 counts > 200 cells / µ L
• *GIT ???? Malabsorption, Wt loss & diarrhea
• *ITP
• CLASSIFICATION ACCORDING TO CLINICAL MANIFESTATONS & CD4 COUNT
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• GROUP C• *CD4 count < 200 cells / µ L
• *Opportunistic infections ????
• Candidiasis of bronchi or lungs, Pneumocystis carinii
• CMV, TB, Toxoplasmosis, Herpes “chronic ulcers
• pneumonitis, esophagitis” , recurrent pneumonia
• *Neoplasms ????
• Lymphoma, Kaposi sarcoma, Cervics carcinoma.
• *CNS ????
• Aids dementia complex “ meningoencephalitis, peripheral neuropathy, cortical atrophy, dementia, memory loss & psychiatric dysfunction”
• CLASSIFICATION CCORDING TO CLINICAL MANIFESTATONS & CD4 COUNT
• Mosul university- College of dentistry-oral & maxillofacial surgery department
• TREATMENT
• CD4 lymphocyte count ???? predict the progression to AIDS ???? the key to managing HIV infection.
• The aim of therapy is reduction of the viral load to undetectable levels.
• Combination antiretroviral drugs should be used to prevent the development of resistance & achieve maximum response.
• 3 drugs should be used (at least 2 different classes)
• -Zidovudine
• -Viracept
• -Viramune