
Infertility
Dr.Nadia Mudher Al-Hilli
FICOG
Department of Obs&Gyn
College of Medicine
University of babylon

Objectives
• Know the definition of infertility
• Understand what could cause infertility
• Learn how to assess a couple with infertility
• Know the treatment options available for infertility
• Infertility: failure to conceive within one year of
unprotected regular sexual intercourse.
• Primary in couples that have never conceived
together, or secondary in couples that have
previously conceived together (although either
partner may have conceived in a different
relationship, which requires further elucidation)
• Infertility affects about 15 % of couples.
• Male & female factors each account for 30% of cases
• Male & female factors combined cause 20%
• The remaining 20% of cases the cause is unknown
( unexplained)
Natural conception
• A healthy couple having frequent intercourse have an 18–
20% chance of conceiving in a single menstrual cycle.
• a cumulative increase in pregnancy rates over time. Within
6 months 70% of couples will have conceived, after 12
months 80% and after 24 months 90%.
• The most important factor affecting fertility is female age,
which is related to a decline in the quality and quantity of
eggs, fertility tends to fall sharply over the age of 36, with
a further dip after the age of 40.
• Male age is also an important; semen quality fall in men
over the age of 50, while frequency of intercourse tends to
fall in men over the age of 40.
Factors that reduce the chance of spontaneous
conception:
• age of the female >35 years.
• Duration of infertility more than 3 years.
• Low coital frequency.
• No previous pregnancy.
• Smoking.
• Body mass index out side the range 19-29 kg/m2 in
women.
• Low number of motile healthy sperms.
• Drugs : NSAIDs, chemotherapy.
Causes of infertility
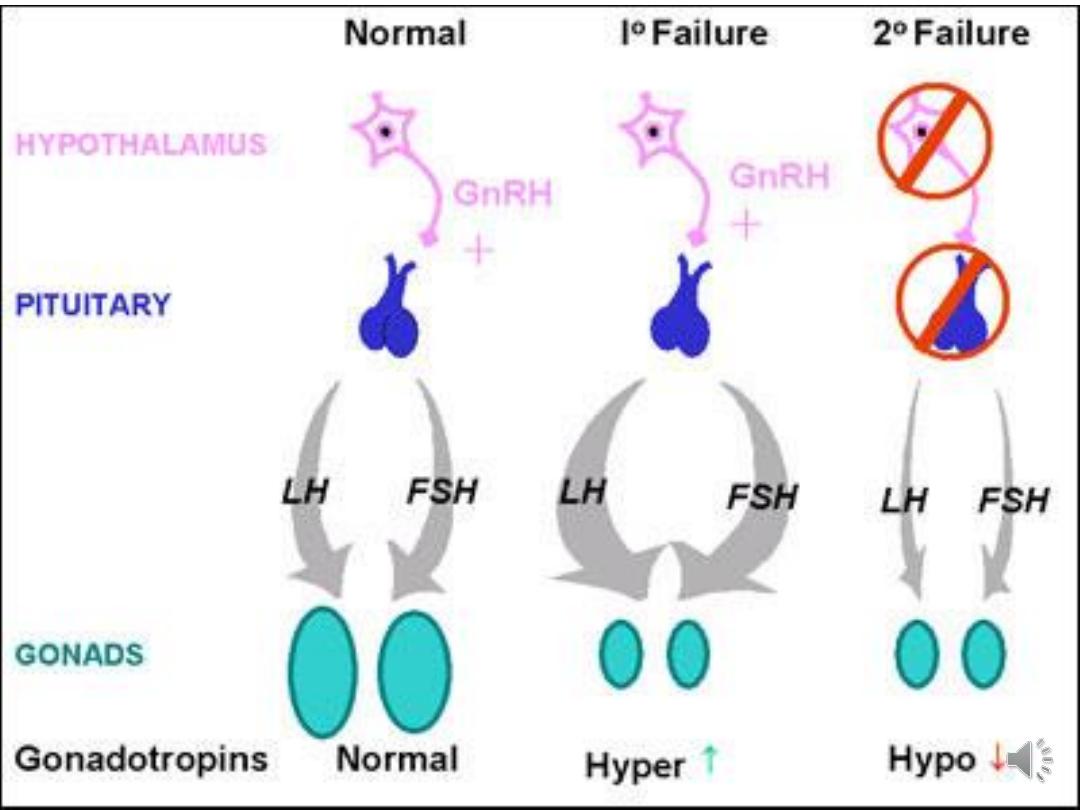
Ovulatory disorders: defect in the hypothalamus,
pituitary or the ovary.
WHO Classification:
Group
I
:
hypothalamic
pituitary
failure
(Hypogonadotrophic hypogonadism): conditions
cause failure of pituitary gland to produce
gonadotrophins & Factors that affect the pulsatile
release of GnRH.
• Group II : Ovulation Dysfunction: polycystic ovary
syndrome (PCOS)
• Women with PCOS who suffer from
oligomenorrhoea due to anovolution may require
treatment.
• hormonal treatments taken by women to regulate
their periods or help hirsutism may be incompatible
with getting pregnant
• Group III : Hypergonadotrophic hypogonadism:
Premature ovarian failure when the ovaries fail
before the age of 40 years.
• Endocrine disorders: hypo & hyperthyroidim &
hyperprolactiemia
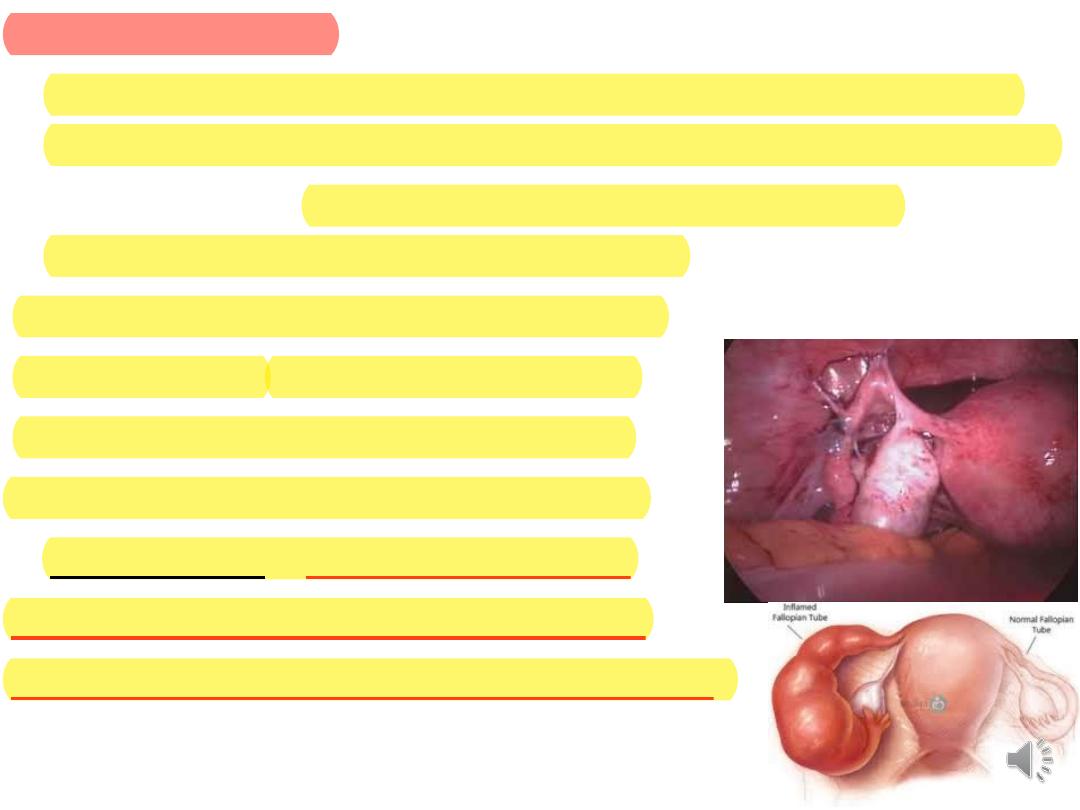
Tubal dysfunction:
• Normal tubal function requires both patency & a healthy
anatomy and physiology for gamete and embryo transport.
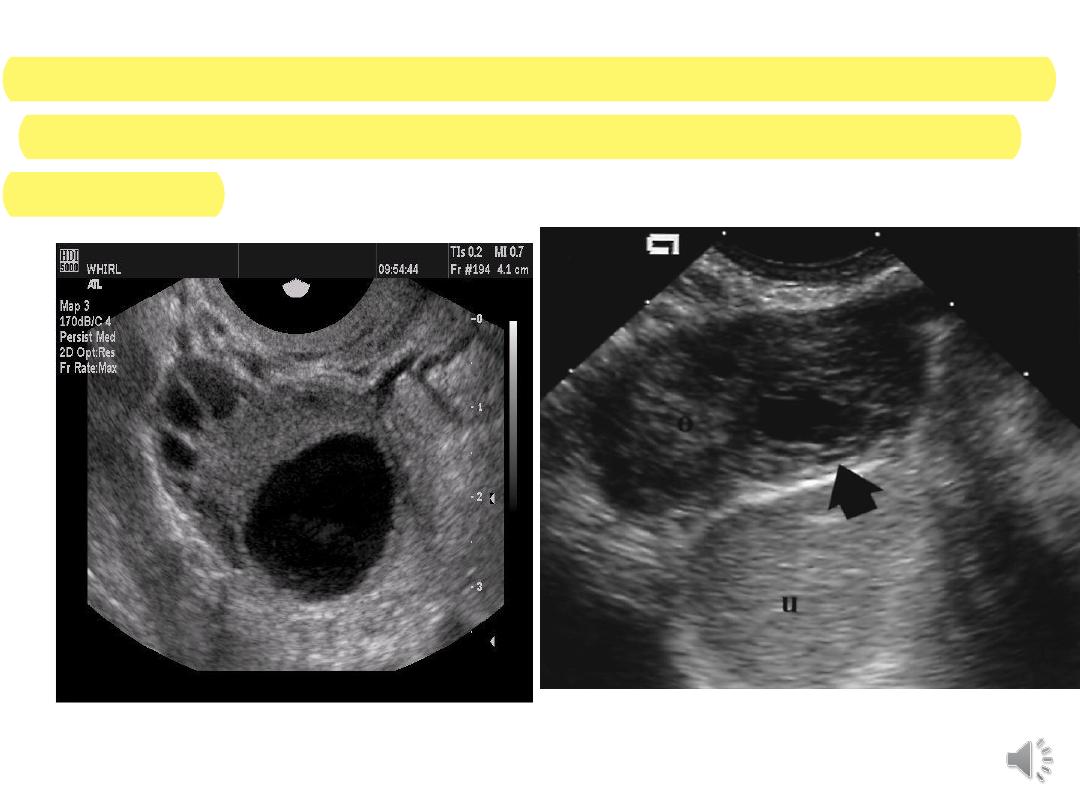
• Tubal damage: blockage is usually associated with
inflammatory processes in the pelvis
e.g, pelvic infection, endometriosis or
pelvic surgery. Chlamydial infections
in particular can produce significant
degrees of tubal damage, resulting in
a hydrosalpinx – a blocked Fallopian
tube, with a thickened wall, flattened
epithelial mucosa and peritubal adhesions
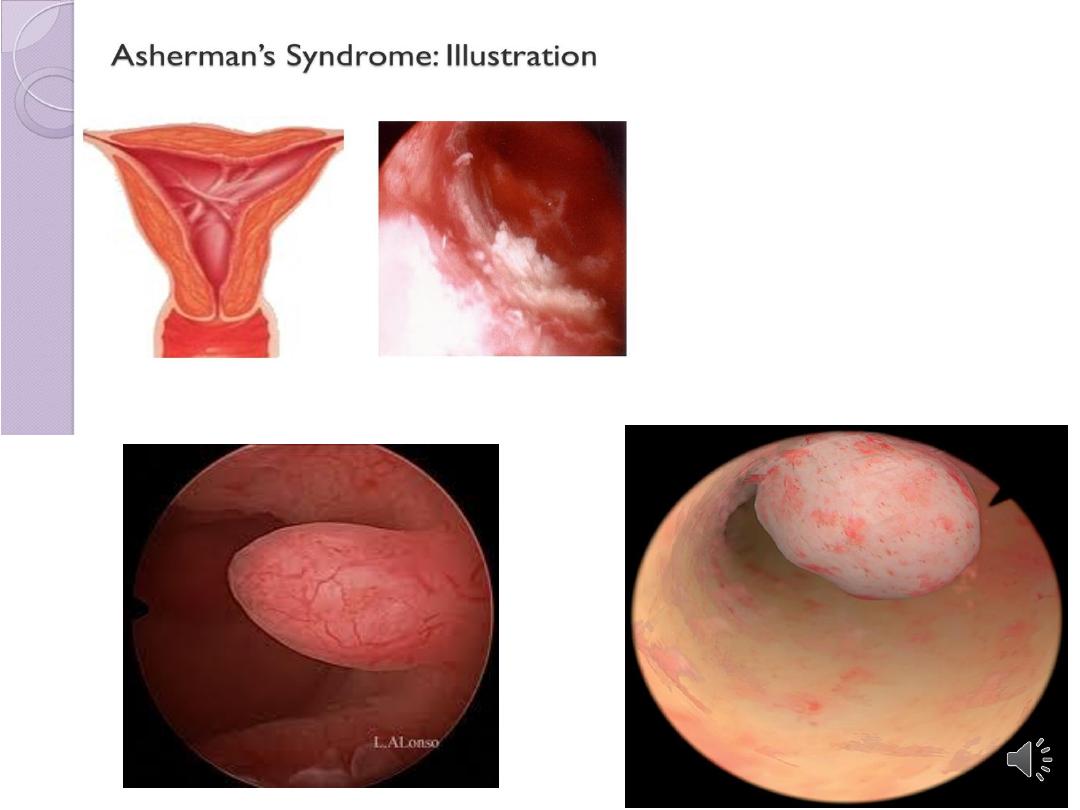
• Uterine problems (Disorders of implantation):
• intramural fibroids larger than 5 cm may effect
fertility
• defects related to endometrial development or the
production of growth & adhesion molecules or
submucous fibroid, or endometrial polyps.

Male factor:
• Disorders of spermatogenesis.
• Impaired sperm transport.
• Ejaculatory dysfunction.
• Immunological & infective factors.

Management:
• History & examination:
• medical & surgical history. Drug history, life style
coital frequency & any difficulties of coitus.
• menstrual cycle
• cervical smear, body weight & blood pressure.
• Examination of both partners is essential to ensure
normal reproductive organs.
Investigations:
• assessment of ovulation, Fallopian tube patency,
uterine cavity & seminal fluid analysis.
• Early follicular phase (day 2-5 of menstrual cycle)
measurement of FSH, LH & estradiole to assess
ovarian function.
• Mid-luteal progesterone level to confirm ovulation.

Marker of ovarian reserve :
Ovarian reserve declines after the age of 35 in an
average healthy woman, or at an earlier age due to
genetic predisposition, surgery or following exposure
to toxins, such as chemotherapy.
• anti-Müllerian hormone (AMH) is produced by
the granulosa cells. It reflect the size of follicular
pool. Need to be measured in pt with advanced
age or conditions affecting follicle number
• Antral Follicle count: measured by TV US, (<4
predicting low response, >16 high response).
Serial follicle tracking by transvaginal ultrasound
(TV US) in the midcycle can be used to confirm
ovulation.
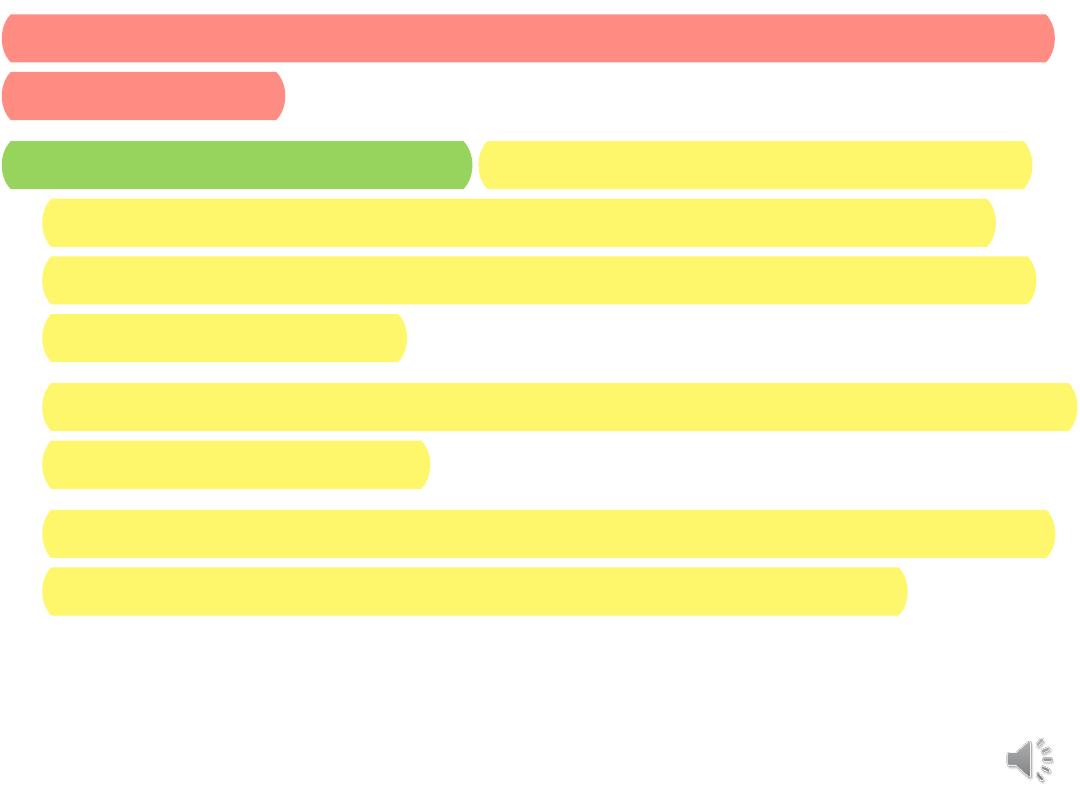
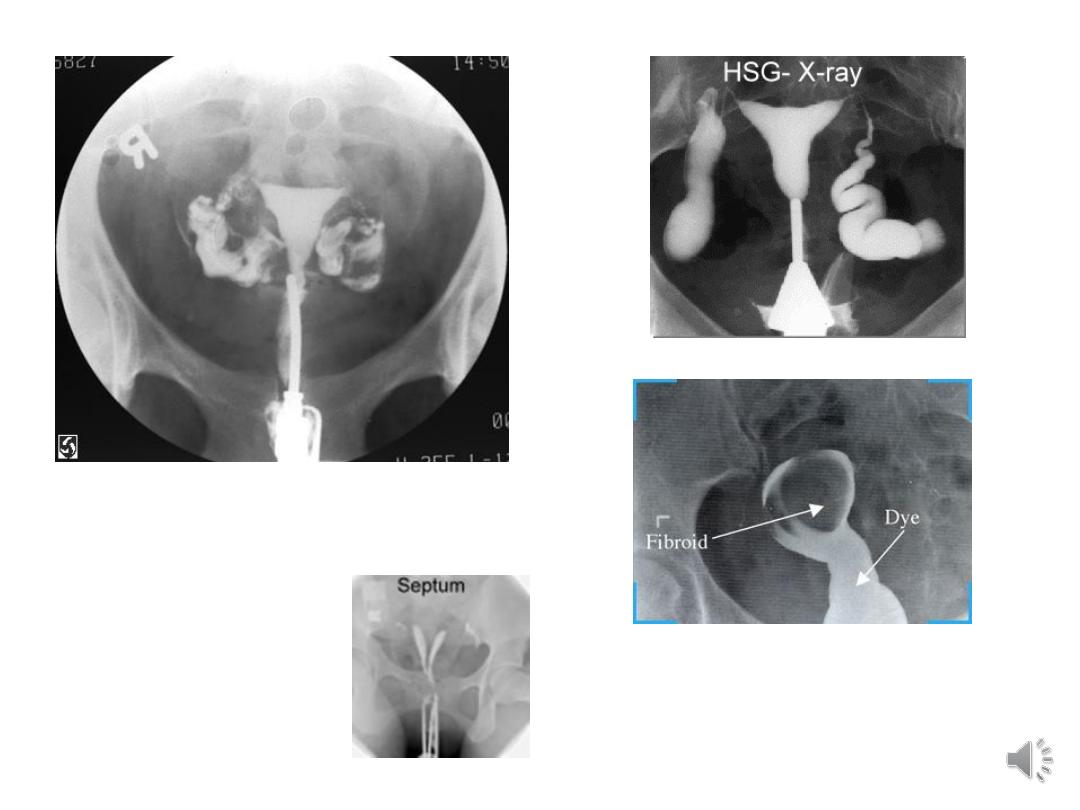
Assessment of tubal patency: in addition to assessing
uterine cavity
• Hysterosalpingogram: offered for women who are
not known to have comorbidities (such as pelvic
inflammatory disease, previous ectopic pregnancy
or endometriosis)
o When the dye flows freely into the abdominal cavity
it confirms patency.
o If the dye spill appear to be loculated or no spillage,
peritubal adhesion or obstruction are likely.

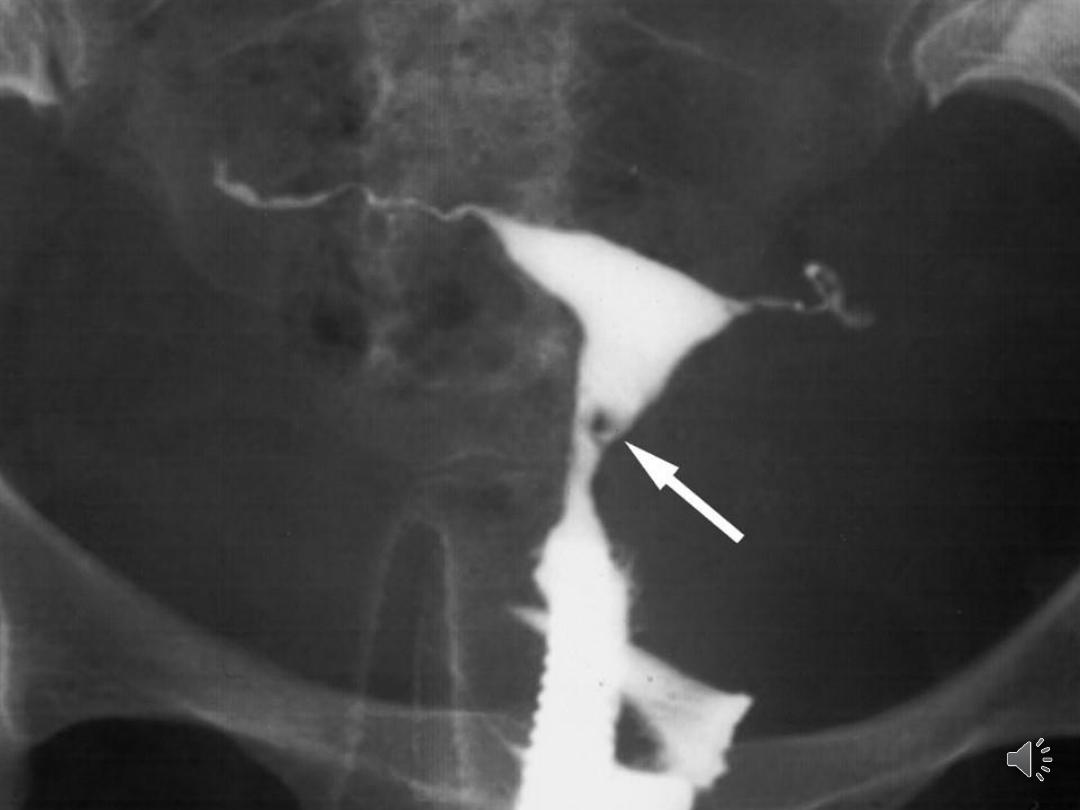
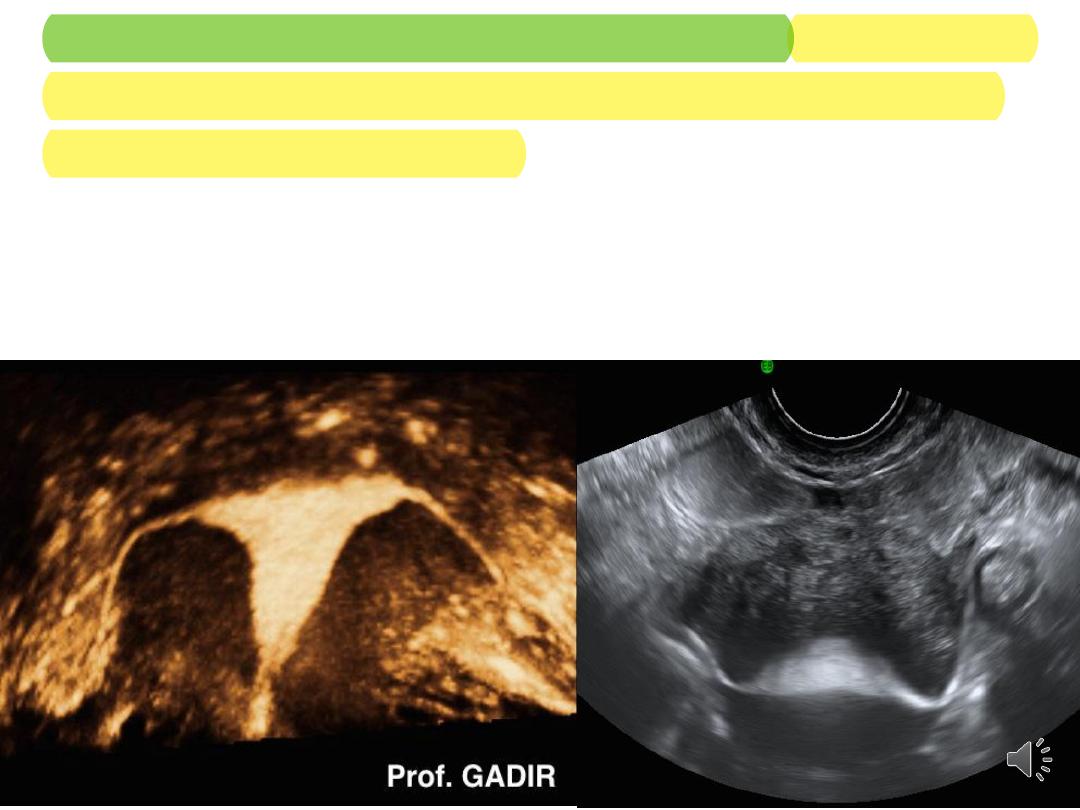
• Hysterocontrast sonography (HyCoSy) involves the
use of US to image the uterus & fallopian tube &
avoid exposure to X-ray.
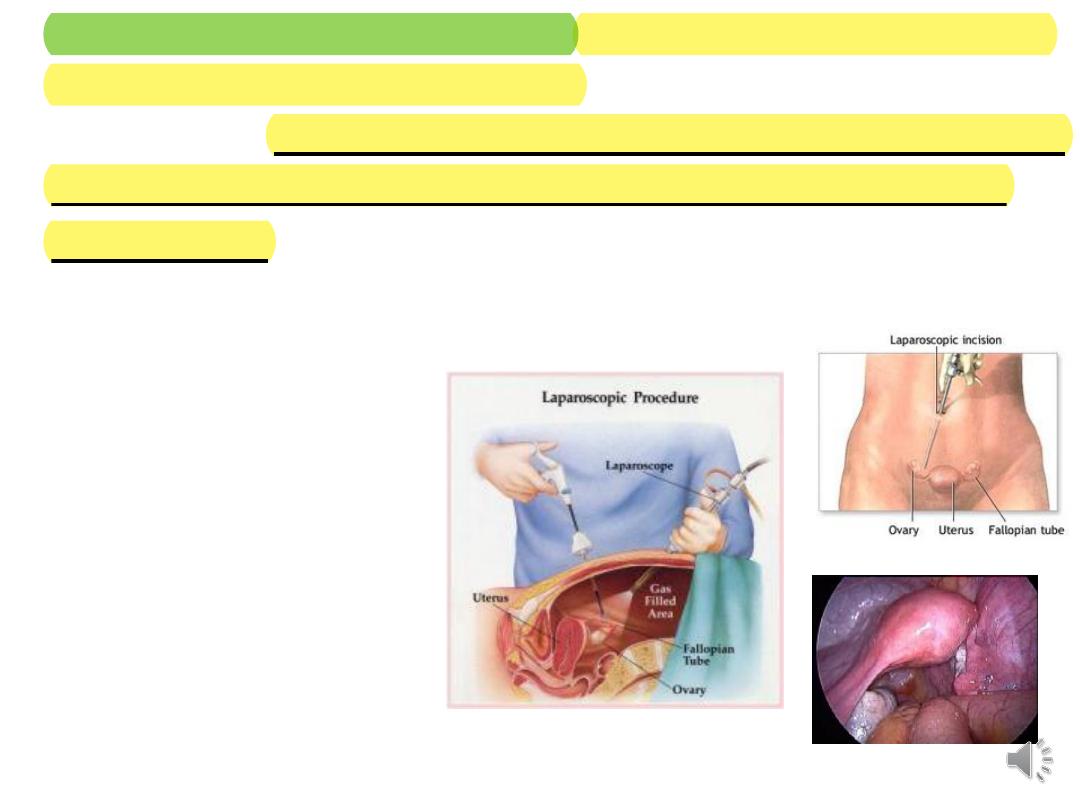
• Laparoscopy & dye intubation: offered for women who are
thought to have co-morbidities. necessitate general
anaesthesia. Tubal patency is tested by installing methylene
blue through the cervix & observing spillage of dye from
fimbrial end.
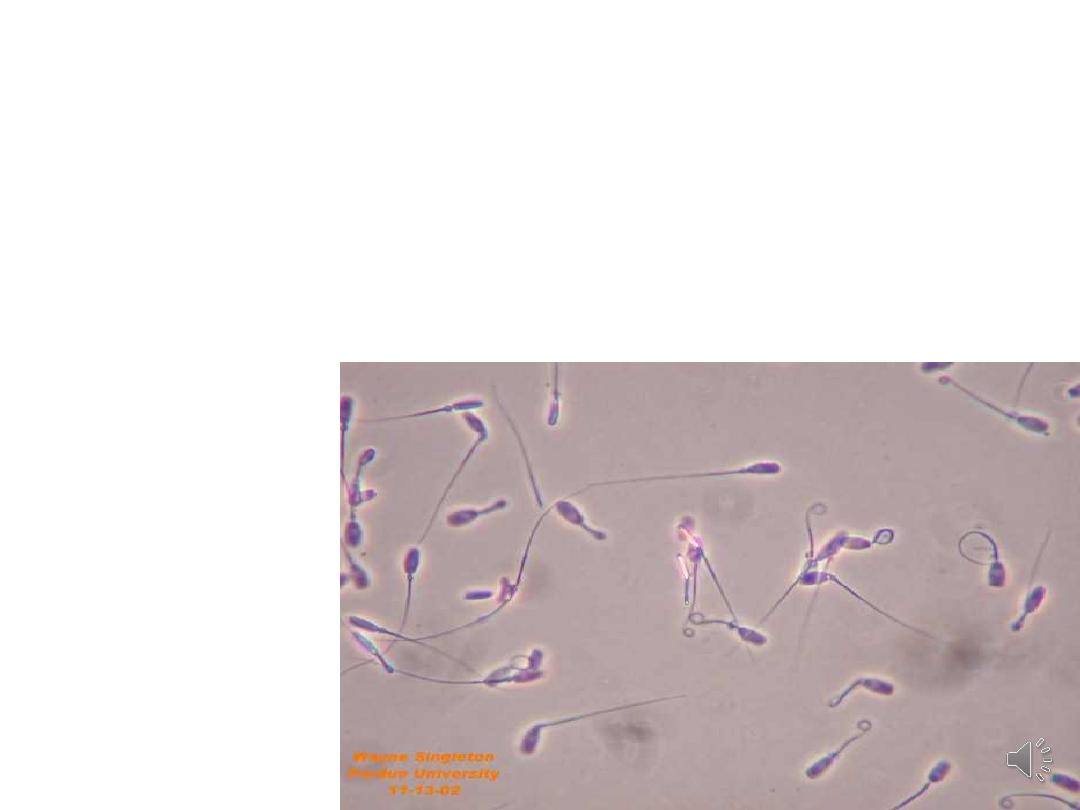
• Semen analysis: after 3 days of sexual abstinence.
• The potential of sperm to fertilize is indicated by its
progressive motility, morphology & agglutination.

• In men with very low sperm counts, an
endocrine profile (LH, FSH, testosterone &
prolactin is indicated.
Treatment:
• Ovulatory disorders:
• Hypothalamic disorder: optimize patient weight &
avoid stressful lifestyle.
If hyperprolactinaemia: dopaminergic agonists (e.g
bromocriptin, cabergolin).
If PCOS: …
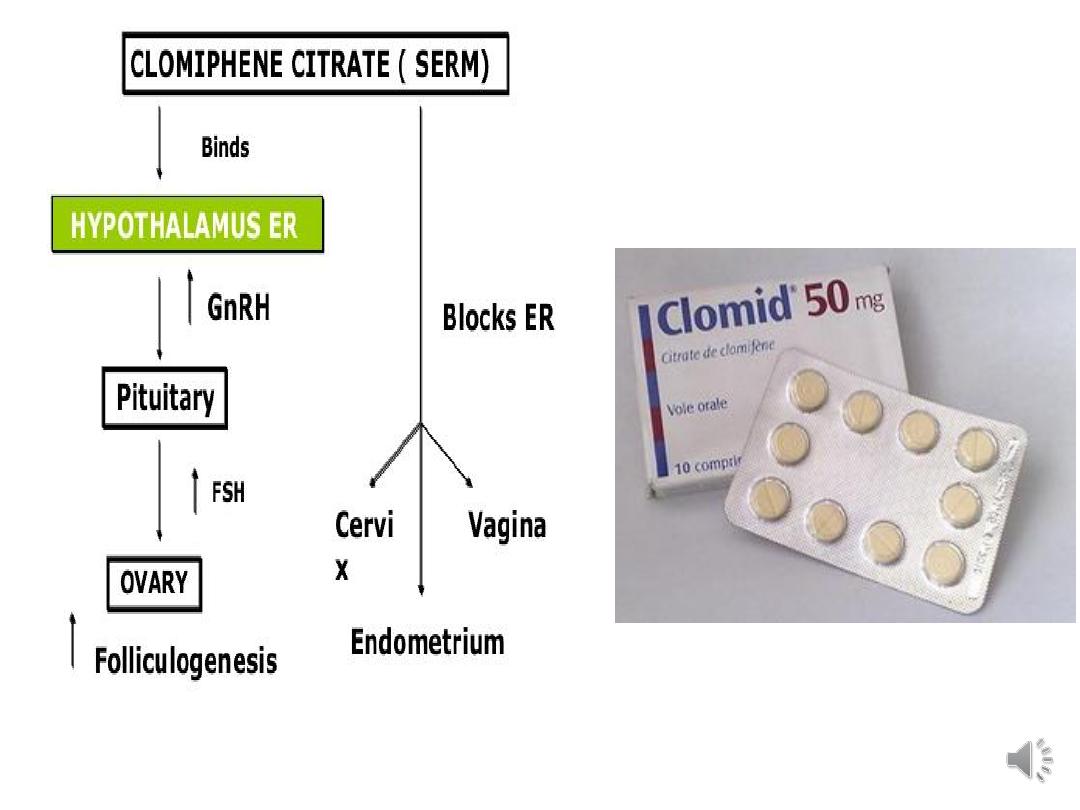
Ovulation induction:
• Clomiphene citrate: acts by increasing
gonadotrophin release from the pituitary.
• Response monitored by ultrasound.to avoid
multiple pregnancy.
• Adverse anti-oestrogenic effects of clomiphene
citrate include thickening of cervical mucus & hot
flushes, others include abdominal distension &
pain, nausea, vomiting, breast tenderness &
reversible hair loss.

• aromatase inhibitors : letrozole is nowadays used
for OI as first line espetially for patients with PCOS.
It inhibit aromatization of testosterone to estradiole
& decrease level of estrogen decrease negative
feedback on pituitary thus increaseing FSH
secretion.
• Gonadotrophins (FSH): are given by daily
injection from the beginning of the cycle.
monitored by US assessment of the number &
size of follicles.
• Human menopausal gonadotrophin, urinary
follicle-stimulating hormone and recombinant
follicle-stimulating hormone are equally effective
in achieving pregnancy
• Ovulation is triggered by injection of human
chorionic gonadotrophin (hCG which binds to LH
receptors) when 1-3 follicles are 18 mm in diameter.
• If more than three follicles are present, the couples
are asked to avoid sexual intercourse & hCG is
withheld.

Tubal disease:
• Treatment aims to restore normal anatomy.
• The success depends on severity, location of
damage & skills of the surgeon.
• In-vitro fertilization is an alternative to surgery.
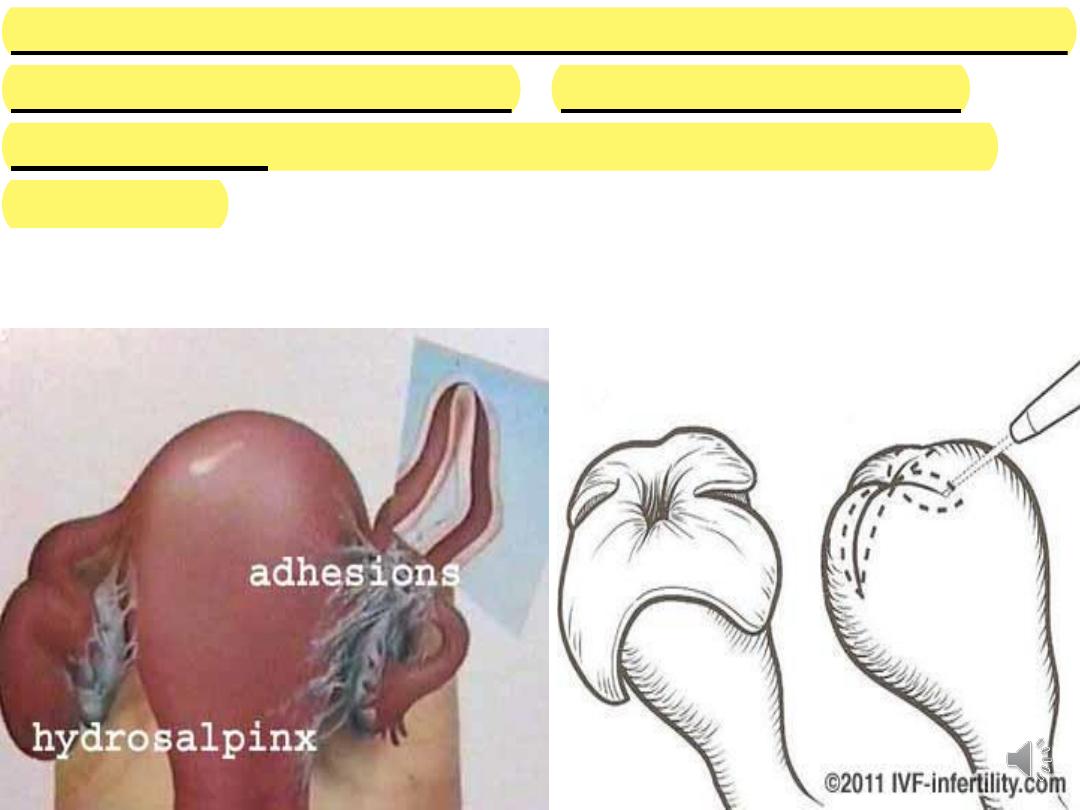
Peri-tubal & periovarian adhesions can be removed by
laparoscopic adhesiolysis. If fimbria are involved,
fimbrioplasty to remove fimbrial adhesions can be
successful.
• Reversal of sterilization produce good conception
rate as the mucosal damage is limited & the woman
has proven fertility.
• In case of hydrosalpinges, better to remove the
affected Fallopian tube prior to IVF as they affect
implantation adversely.