
بسم هللا الرحمن الرحيم
a.c. 19/02/2020 1440 هجري

Hospital-acquired
pneumonia

OBJECTIVES
• To know the epidemiology ,etiology,
pathogenesis ,clinical presentation,
investigation ,diagnosis ,treatment
,complication ,prognosis

Hospital-acquired pneumonia
Hospital-acquired or
nosocomial pneumonia
is a new episode of
pneumonia occurring at
least 2 days after
admission to hospital
It is the second most
common hospital-
acquired infection (HAI)
and the leading cause
of HAI-associated death.

Classification of HAP
Ventilator-associated
pneumonia’ (VAP)
Pneumonia occurred patients
in intensive care units,
especially when
mechanically ventilated;
Healthcare-associated
pneumonia (HCAP)
pneumonia in a person
who has spentat least 2
days in hospital within the
last 90 days,
has attended a
haemodialysis unit,
received intravenous
antibiotics .
been resident in a nursing
home or other long-term
care facility

Factors predisposing to hospital-acquired
pneumonia
Reduced host defences against bacteria
• Reduced immune defences
(e.g.corticosteroid treatment, diabetes,
malignancy)
• Reduced cough reflex (e.g. post-operative)
• Disordered mucociliary clearance (e.g.
anaesthetic agents)
• Bulbar or vocal cord palsy
Aspiration of nasopharyngeal or gastric
secretions
• Immobility or reduced conscious level
• Vomiting, dysphagia (N.B. stroke disease),
achalasia or severe reflux
• Nasogastric intubation
Bacteria introduced into lower
respiratory tract
• Endotracheal
intubation/tracheostomy
• Infected
ventilators/nebulisers/bron-
choscopes
• Dental or sinus infection
Bacteraemia
• Abdominal sepsis
• IV cannula infection
• Infected emboli

Microbiology
The early-onset HAP
(occurring within 4–5
days of admission) are
similar to those involved
in CAP.
Late onset HAP
Gram-negative bacteria
(e.g. Escherichia,
Pseudomonas, Klebsiella
species and
Acinetobacterbaumannii),
Staph. aureus (including
the meticillinresistant
type (MRSA)) and anaerobes

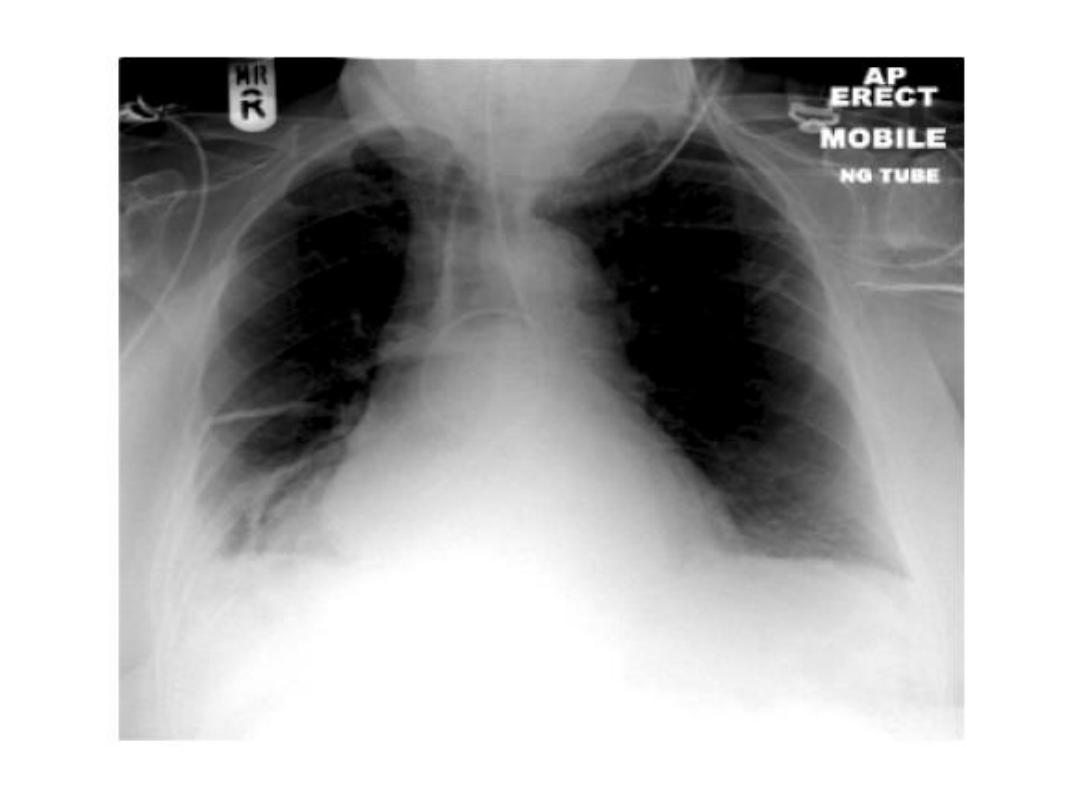
Clinical features
The hospitalised or ventilated patient
purulent sputum (or endotracheal secretions),
new radiological infiltrates,
unexplained increase in oxygen requirement,
a core temperature of more than 38.3°C,
a leucocytosis or leucopenia.
differential diagnosis
• Venous thromboembolism .
• ARDS .
• pulmonary oedema.
• Pulmonary haemorrhage.
• drug toxicity.

Investigations
• microbiological confirmation .
• the full blood count (FBC).
• urea and electrolytes (U&E),
• Erythrocyte sedimentation rate (ESR) and C-
reactive protein (CRP).
• arterial blood gas.
• chest X-ray.

Management
• adequate oxygenation,
• Appropriate fluid balance
• antibiotics.

Treatment
In early-onset HAP,
1-If not received
antibiotics
treated with co-amoxiclav
or
cefuroxime.
2- Received antibiotics
piperacillin/tazobactam
or a third generation
Cephalosporin..
In late-onset HAP,
the antibiotics must cover
the
1-Gram-negative bacteria
2-Staph. aureus
(including MRSA)
3- anaerobes.

Prevention
the mortality from HAP is approximately 30%,
Good hygie regard to handwashing and any
equipment used.
The risk of aspiration should be minimised,
ventilator associated pneumonia by limiting use
of proton pump inhibitors.
decontaminate the upper airway, by Oral
antiseptic (chlorhexidine 2%)
selective decontamination of the digestive tract
.

Suppurative pneumonia, aspiration
pneumonia and pulmonary abscess
These conditions are considered together, as
their aetiology and clinical features overlap

Suppurative pneumonia is characterised by
destruction of the lung parenchyma by the
inflammatory process .
Microabscess
formation is a characteristic
histological feature.
Pulmonary abscess’ is usually taken to refer
to lesions in which there is a large localised
collection of pus, or a cavity lined by chronic
inflammatory tissue, from which pus has
escaped by rupture into a bronchus.

Risk
Inhalation
septic material during operations on the nose, mouth or throat
under general anaesthesia,
vomitus during anaesthesia coma, particularly if oral hygiene is
poor.
bulbar palsy
vocal cord palsy,
stroke,
achalasia
oesophageal reflux,
alcoholism.
local bronchial obstruction
from a neoplasm or foreign
body.
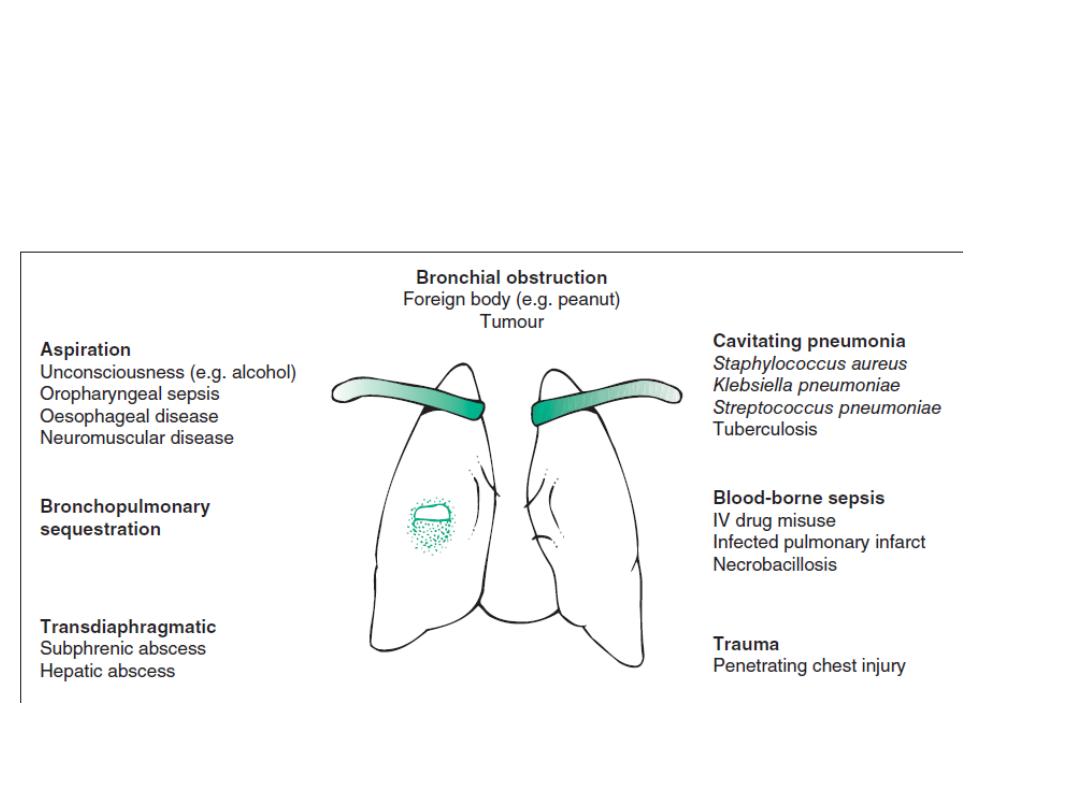
Aetiology of lung abscess

Microbilogy
mixture of anaerobes and aerobes from flora in the
mouth and upper respiratory tract.
in a previously healthy lung,
•
Staph. aureus
•
Klebsiella pneumoniae
.
pulmonary infarct or a collapsed
• Strep. pneumoniae, Staph. aureus, Strep. pyogenes,
H. influenzae and, in some cases, anaerobic bacteria
.
In many cases,
no pathogen can be isolated,
particularly when antibiotics have been given
.

Clinical features of suppurative
pneumonia
Symptoms
•
Cough
with large amounts of sputum, sometimes fetid and blood-
stained
•
Pleural pain
common
•
Sudden expectoration of copious amounts
of foul sputum if abscess
ruptures into a bronchus
Clinical signs
•
High remittent pyrexia
• Profound systemic upset
• Digital clubbing may develop quickly
(10–14 days)
•
Consolidation
on chest examination; signs of cavitation rarely found
•
Pleural rub
common
• Rapid deterioration in general health, with marked
weight loss
if not
adequately treated

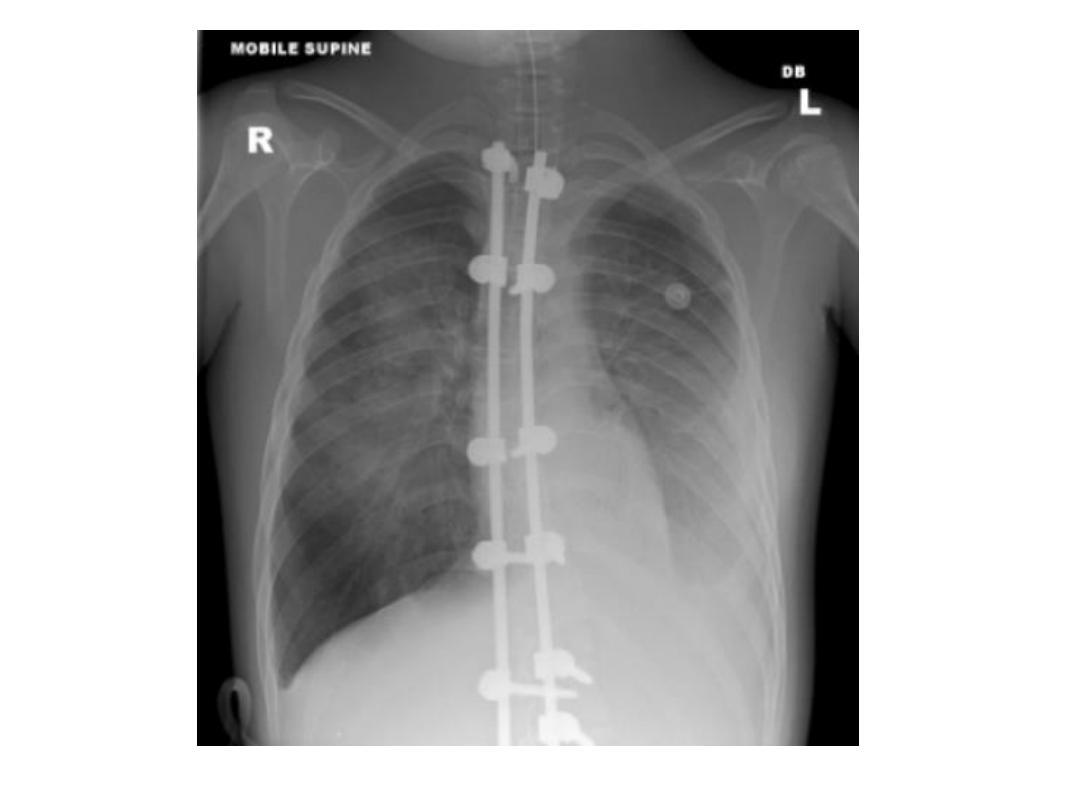
Investigations
Radiological features
Abscesses are characterised by cavitation and
fluid level.
Occasionally, a preexisting emphysematous
bulla becomes infected and appears as a
cavity containing an air–fluid level

Managment
Intravenousco-amoxiclav 1.2 g 3 times daily.
Metronidazole 400 mg 3 times daily If an anaerobic bacterial infection is
suspected (e.g. from fetor of the sputum), oral
CA-MRSA is usually susceptible to a variety of oral non-β-lactam antibiotics,
such
as trimethoprim/sulfamethoxazole,
clindamycin, others
Parenteral therapy with
vancomycin
or daptomycin and to metronidazole,
or clindamycin and third-generation cephalosporins.
Prolonged treatment for 4–6 weeks may be required in some patients
with lung abscess.
Physiotherapy

Prognosis
In most patients, there is a good response to
treatment and, although residual fibrosis and
bronchiectasis
Surgery
may be required.

Pneumonia in the
immunocompromised patient
Patients immunocompromised by drugs or
disease are at high risk of pulmonary infection.
The majority of cases are caused by the same
pathogens that cause pneumonia
Patients with more profound immunosuppression,
unusual organisms or those normally considered to
be of low virulence or non-pathogenic may become
‘opportunistic’pathogens

Clinical features
fever,
cough
breathlessness,

Diagnosis
Invasive investigations, such as
Bronchoscopy.
BAL.
transbronchial biopsy.
surgical lung biopsy.

Management
Broad-spectrum antibiotic
a third-generation cephalosporin or
aquinolone,
plus an antistaphylococcal antibiotic,
Or
an antipseudomonal penicillin plus an
aminoglycoside.

Respiratory infection in old age
Increased risk of and from respiratory
infection.
Predisposing factors: .
Atypical presentation .
Mortality
Influenza
TB

THANK YOU
• To know the epidemiology ,etiology,
pathogenesis ,clinical presentation,
investigation ,diagnosis ,treatment
,complication ,prognosis