Dr. BASIM AUDIB
Professor of Medicine
F.I.C.M.S,F.R.C.P (Edenbera)
SCE Diabetes and Endocrine (London)
Consultant of Medicine
Diabetes mellitus (DM) is a group of diseases
characterized by high levels of blood glucose
resulting from defects in insulin production, insulin
action, or both.
The term diabetes mellitus describes a metabolic
disorder of multiple aetiology characterized by
chronic hyperglycaemia with disturbances of
carbohydrate, fat and protein metabolism resulting
from defects in insulin secretion, insulin action, or
both.
The effects of diabetes mellitus include long–term
damage, dysfunction and failure of various organs.
Diabetes mellitus may present with characteristic
symptoms such as thirst, polyuria, blurring of vision,
and weight loss.
In its most severe forms, ketoacidosis (in type 1) or a
non–ketotic hyperosmolar state (in type 2) may
develop and lead to stupor, coma and, in absence of
effective treatment, death.
Often symptoms are not severe, or may be absent,
and consequently hyperglycaemia sufficient to cause
pathological and functional changes may be present
for a long time before the diagnosis is made.
The long–term effects of diabetes mellitus
include progressive development of the specific
complications of retinopathy with potential
blindness, nephropathy that may lead to chronic
kidney disease, and/or neuropathy with risk of
foot ulcers, amputation, Charcot joints, and
features of autonomic dysfunction, including
sexual dysfunction.
People with diabetes are at increased risk of
cardiovascular, peripheral vascular and
cerebrovascular disease.
The development of diabetes is projected to reach
pandemic proportions over the next10-20 years.
International Diabetes Federation (IDF) data indicate
that by the year 2025, the number of people affected
will reach 333 million (90% of these people will have
Type 2 diabetes).
In most Western societies, the overall prevalence has
reached 4-6%, and is as high as 10-12% among 60-
70-year-old people.
The annual health costs caused by diabetes and its
complications account for around 6-12% of all
health-care expenditure.
Normal insulin metabolism
◦
Produced by the cells in the
islets of Langherans of the
pancreas
8
Normal insulin metabolism
◦
Promotes glucose transport from
the bloodstream across the cell
membrane to the cytoplasm of the
cell
9
Normal insulin metabolism
◦
Insulin after a meal:
Stimulates storage of glucose as
glycogen
Inhibits gluconeogenesis
10
Normal insulin metabolism
◦
Insulin after a meal:
Enhances fat deposition in
adipose tissue
Increases protein synthesis
Type 1 Diabetes Mellitus
Type 2 Diabetes Mellitus
Gestational Diabetes
Other types:
LADA (latent autoimmune diabetes of adult)
MODY (
maturity-onset diabetes of youth)
Secondary Diabetes Mellitus
Was previously called insulin-dependent diabetes mellitus
(IDDM) or juvenile-onset diabetes.
Type 1 diabetes develops when the body’s immune system
destroys pancreatic beta cells, the only cells in the body
that make the hormone insulin that regulates blood
glucose.
This form of diabetes usually strikes children and young
adults, although disease onset can occur at any age.
Type 1 diabetes may account for 5% to 10% of all
diagnosed cases of diabetes.
Risk factors for type 1 diabetes may include autoimmune,
genetic, and environmental factors.
13
Progressive destruction of pancreatic
cells
Autoantibodies cause a reduction of 80%
to 90% of normal cell function before
manifestations occur
14
Causes:
◦
Genetic predisposition
Related to human leukocyte
antigens (HLAs) , HLA DR4 < HLA
DR3
◦
Exposure to a virus : mumps,
Coxackie B4, cytomeg., Epst.-Barr
15
Manifestations develop when the pancreas
can no longer produce insulin
◦
Rapid onset of symptoms
◦
Present at ER with ketoacidosis
in about 25% of cases
16
Weight loss
Polydipsia
Polyuria
Polyphagia
17
Diabetic ketoacidosis (DKA)
- 25 % of newly diagnosed type 1
◦
Occurs in the absence of exogenous
insulin
◦
Life-threatening condition
◦
Lethally if untreated
Was previously called non-insulin-dependent
diabetes mellitus (NIDDM) or adult-onset diabetes.
Type 2 diabetes may account for about 90% to 95% of
all diagnosed cases of diabetes.
It usually begins as insulin resistance, a disorder in
which the cells do not use insulin properly. As the
need for insulin rises, the pancreas gradually loses its
ability to produce insulin.
Type 2 diabetes is associated with older age, obesity,
family history of diabetes, history of gestational
diabetes, impaired glucose metabolism, physical
inactivity.
Type 2 diabetes is increasingly being diagnosed in
children and adolescents.
19
Accounts for 90% -95% of patients with
diabetes
Usually occurs in people over 40 years of age
80-90% of patients are overweight
20
Pancreas continues to produce
some
endogenous insulin
Insulin produced is either insufficient or
poorly utilized by the tissues
21
Insulin resistance
◦
Body tissues do not respond to
insulin
◦
Results in hyperglycemia
22
Gradual onset
Person may go many years with undetected
hyperglycemia
Marked hyperglycemia (500 to 1000 mg/dl)
A form of glucose intolerance that is diagnosed
in some women during pregnancy.
During pregnancy, gestational diabetes requires
treatment to normalize maternal blood glucose
levels to avoid complications in the infant.
After pregnancy, 5% to 10% of women with
gestational diabetes are found to have type 2
diabetes.
Women who have had gestational diabetes have a
20% to 50% chance of developing diabetes in the
next 5-10 years.
Other specific types of diabetes result from
specific genetic conditions (such as maturity-
onset diabetes of youth), surgery, drugs,
malnutrition, infections, and other illnesses.
Such types of diabetes may account for 1% to
5% of all diagnosed cases of diabetes.

Latent Autoimmune Diabetes in Adults (LADA)
) which is diagnosed in individuals
who are older than the usual age of onset of
type 1 diabetes.
Alternate terms that have been used for
"LADA" include Late-onset Autoimmune
Diabetes of Adulthood.
Often, patients with LADA are mistakenly
thought to have
, based on
their age at the time of diagnosis.
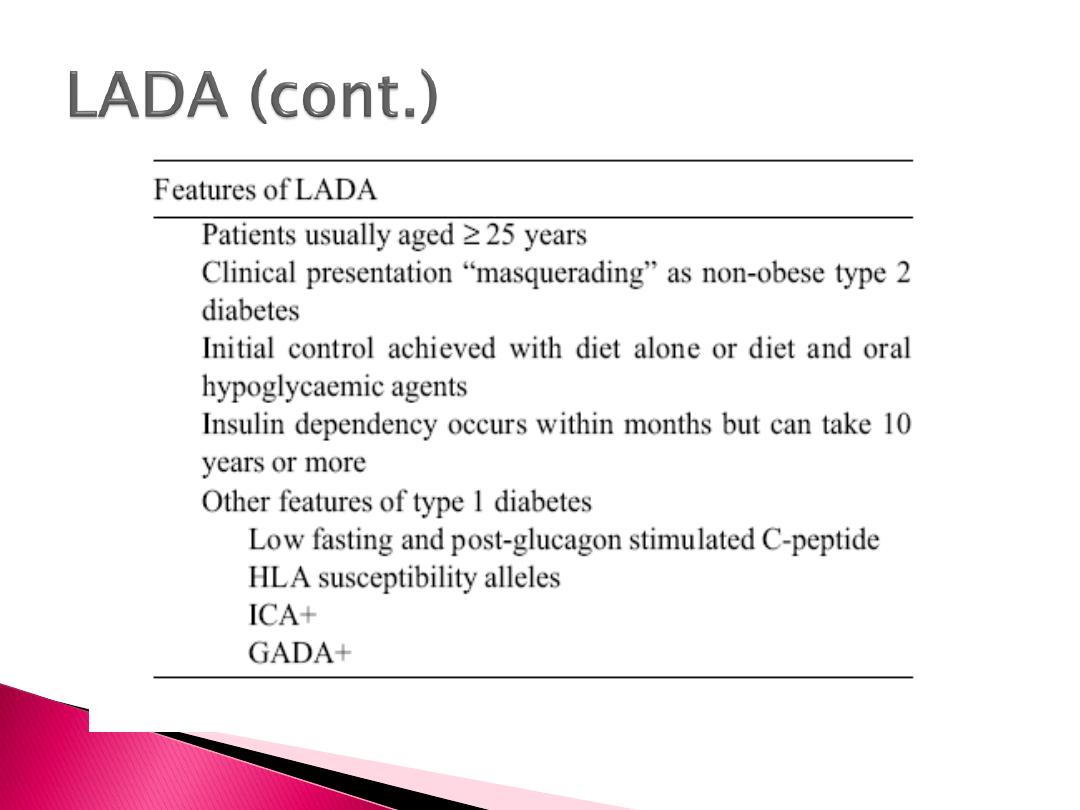
About 80% of adults apparently with recently
diagnosed Type 2 diabetes but with GAD
auto-antibodies (i.e. LADA) progress to
insulin requirement within 6 years.

MODY – Maturity Onset Diabetes of the Young
MODY is an autosomal dominant mode of
inheritance.
Originally, diagnosis of MODY was based on
presence of non-ketotic hyperglycemia in
adolescents or young adults in conjunction with a
family history of diabetes.
However, genetic testing has shown that MODY
can occur at any age and that a family history of
diabetes is not always obvious.
Type
Mutation
% of total MODY
MODY 1 HNF-4
α
5-10%
MODY 2 Glucokinase 30-70%
MODY 3 HNF-1
α
30-70%
MODY 4 IPF less than 1%
MODY 5 HNF-1β

Secondary causes of Diabetes mellitus include:
Acromegaly,
Cushing syndrome,
Thyrotoxicosis,
Pheochromocytoma
Chronic pancreatitis,
Cancer
Drug induced hyperglycemia:
◦
Atypical Antipsychotics - Alter receptor binding characteristics, leading to
increased insulin resistance.
◦
Beta-blockers - Inhibit insulin secretion.
◦
Calcium Channel Blockers - Inhibits secretion of insulin
◦
Corticosteroids - Cause peripheral insulin resistance and gluconeogensis.
◦
Fluoroquinolones - Inhibits insulin secretion by blocking ATP sensitive
potassium channels.
◦
Naicin - They cause increased insulin resistance due to increased free fatty
acid mobilization.
◦
Phenothiazines - Inhibit insulin secretion.
◦
Thiazide Diuretics - Inhibit insulin secretion due to hypokalemia. They
also cause increased insulin resistance due to increased free fatty acid
mobilization.

Thank You