
Body Fluid
Body Water Content
Total body water is a function not only of age and body mass, but
also of sex and the relative amount of body fat. Because of their
low body fat and low bone mass, infants are 73% or more water.
After infancy total body water declines throughout life,
accounting for only about 45% of body mass in old age. A
healthy young man is about 60% water; a healthy young woman
about 50%. This difference between the sexes reflects the fact
that females have relatively more body fat and relatively less
skeletal muscle than males. Of all body tissues, adipose tissue is
least hydrated (containing up to 20% water); even bone contains
more water than does fat. By contrast, skeletal muscle is about
75% water. Thus, people with greater muscle mass have
proportionately more body water.

Fluid Compartments
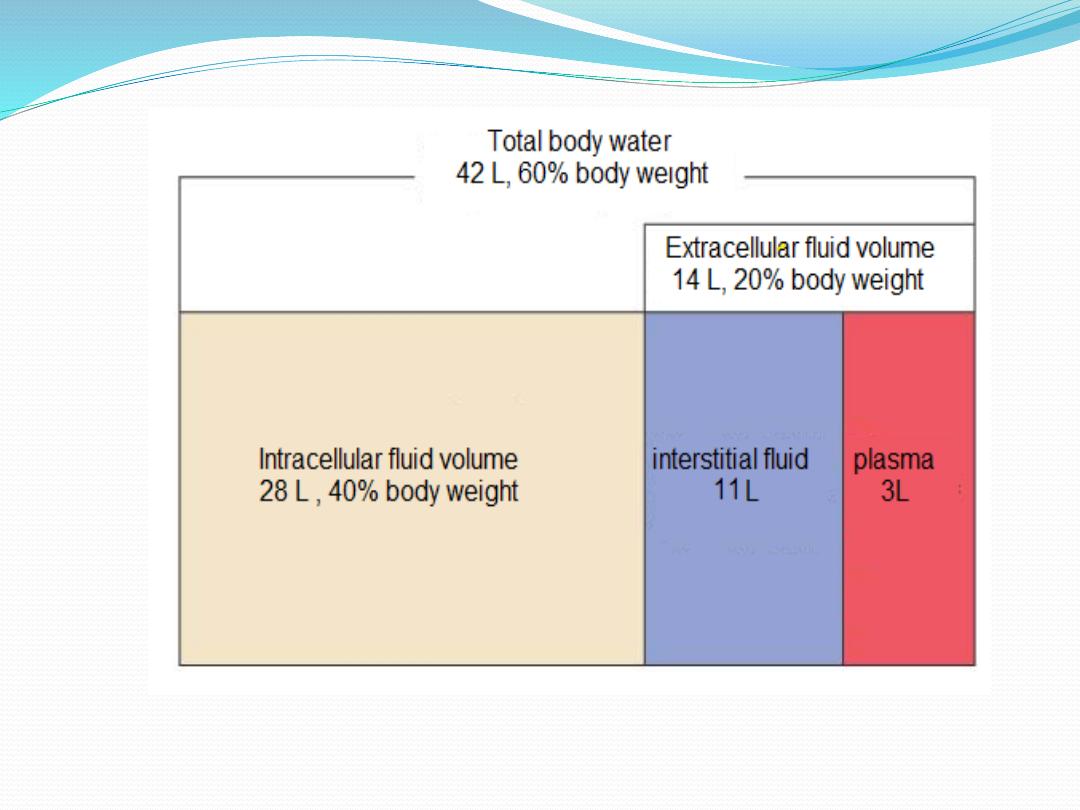
In the average 70-kilogram adult human, the total body
water is about 60% of the body weight, or about 42 liters. A
little less than two-thirds (about 28 L of the 42 L) by
volume is in the intracellular fluid (ICF) compartment,
which actually consists of trillions of tiny individual
“compartments”: the cells. The remaining one-third (14 L)
or so of body water is outside cells, in the extracellular fluid
(ECF) compartment. The ECF constitutes the body’s
“internal environment” referred to by Claude Bernard and
is the external environment of each cell.

The ECF compartment is divisible into two
subcompartments:
(1) plasma, the fluid portion of
blood, and (2) interstitial fluid (IF), the fluid in the
microscopic spaces between tissue cells. There are
numerous other examples of ECF that are distinct from
both plasma and interstitial fluid—lymph,
cerebrospinal fluid, humors of the eye, synovial fluid,
serous fluid, secretions of the gastrointestinal tract—
but most of these are similar to IF and are usually
considered part of it.

Ionic Composition of Plasma and Interstitial Fluid
The extracellular fluid, including the plasma and the
interstitial fluid, contains large amounts of sodium and
chloride ions, reasonably large amounts of bicarbonate
ions, but only small quantities of potassium, calcium,
magnesium, phosphate, and organic acid ions. Because the
plasma and interstitial fluid are separated only by highly
permeable capillary membranes, their ionic composition is
similar. The most important difference between these two
compartments is the higher concentration of protein in the
plasma.

Because of the
Donnan effect
, the concentration of
positively charged ions (cations) is slightly greater
(about 2 %) in the plasma than in the interstitial fluid.
The plasma proteins have a net negative charge and,
therefore, tend to attract cations, such as sodium and
potassium ions, thus holding extra amounts of these
cations in the plasma along with the plasma proteins.
Conversely, negatively charged ions (anions) tend to
have a slightly higher concentration in the interstitial
fluid compared with the plasma.
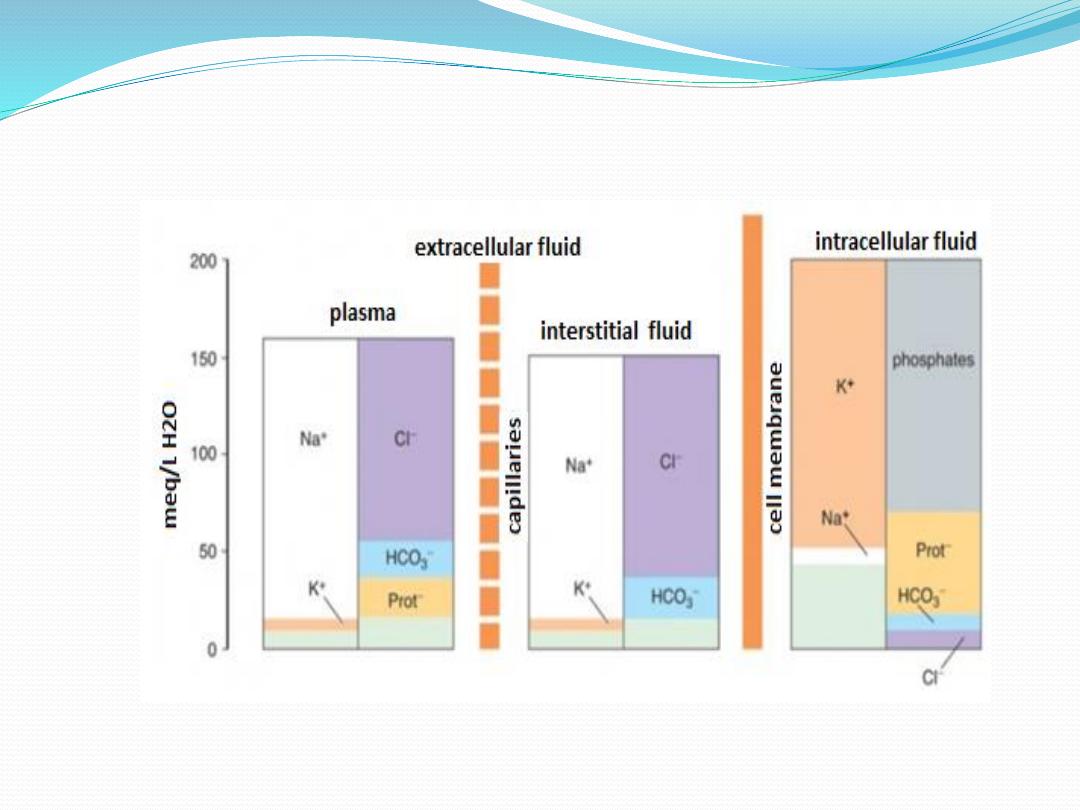
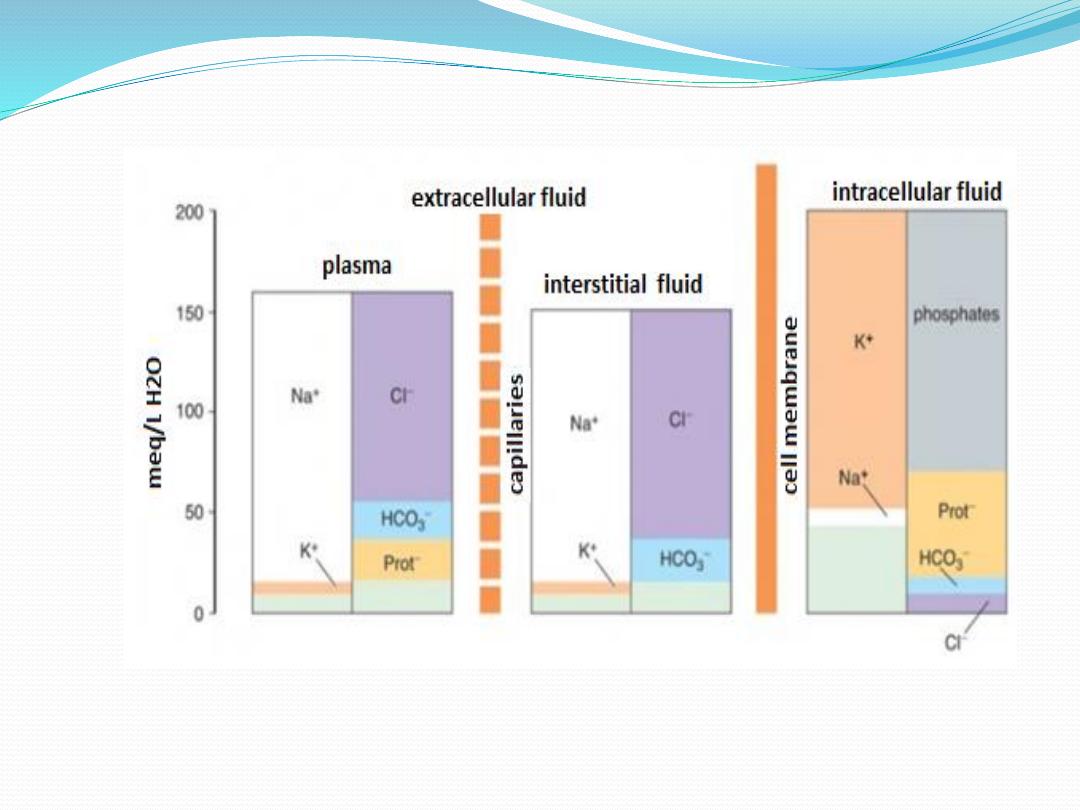
Composition of body fluid cmopartents.

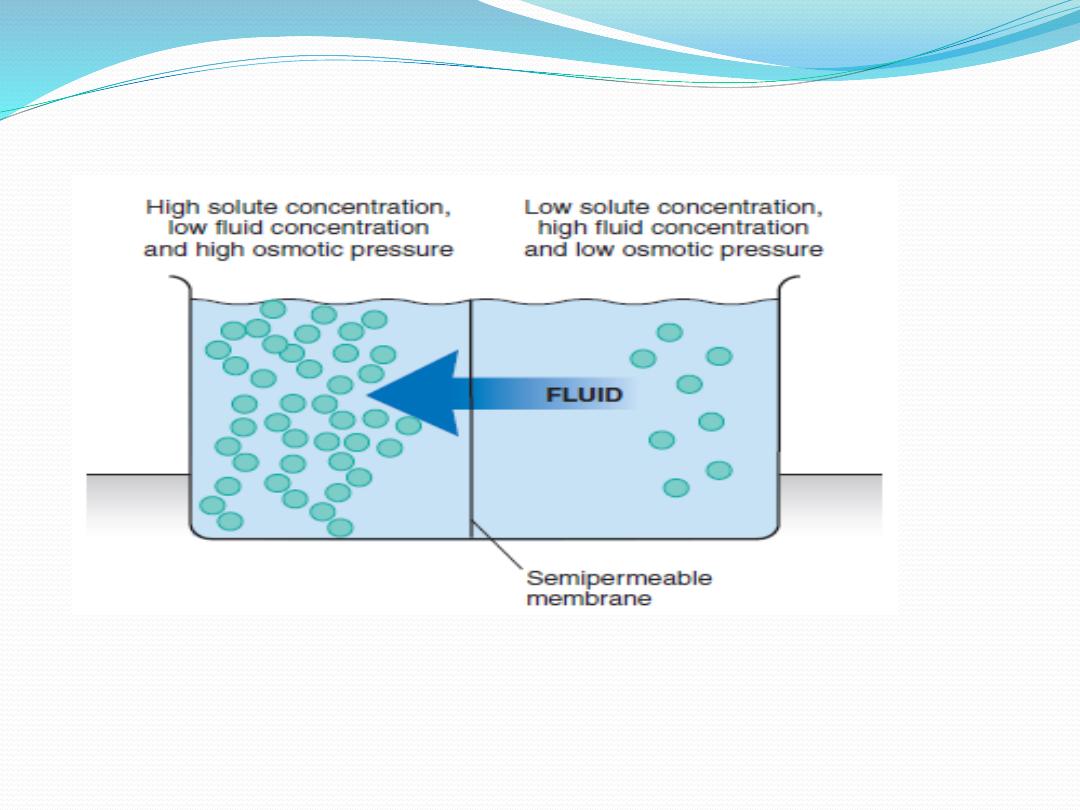
Osmosis
Osmosis
is
the
diffusion
of
water
across
a
semipermeable or selectively permeable membrane.
Water diffuses from a region of higher water
concentration
to
a
region
of
lower
water
concentration. The concentration of water in a
solution is determined by the concentration of solute.
The greater the solute concentration is, the lower the
water concentration will be.

Effective osmole
If a solute doesn't easily cross a membrane, then it is
an "effective" osmole for that compartment. In other
words, it creates an osmotic force for water. For
example, plasma proteins do not easily cross the
capillary membrane and thus serve as effective
osmoles for the vascular compartment. Sodium does
not easily penetrate the cell membrane, but it does
cross the capillary membrane, thus it is an effective
osmole for the extracellular compartment.

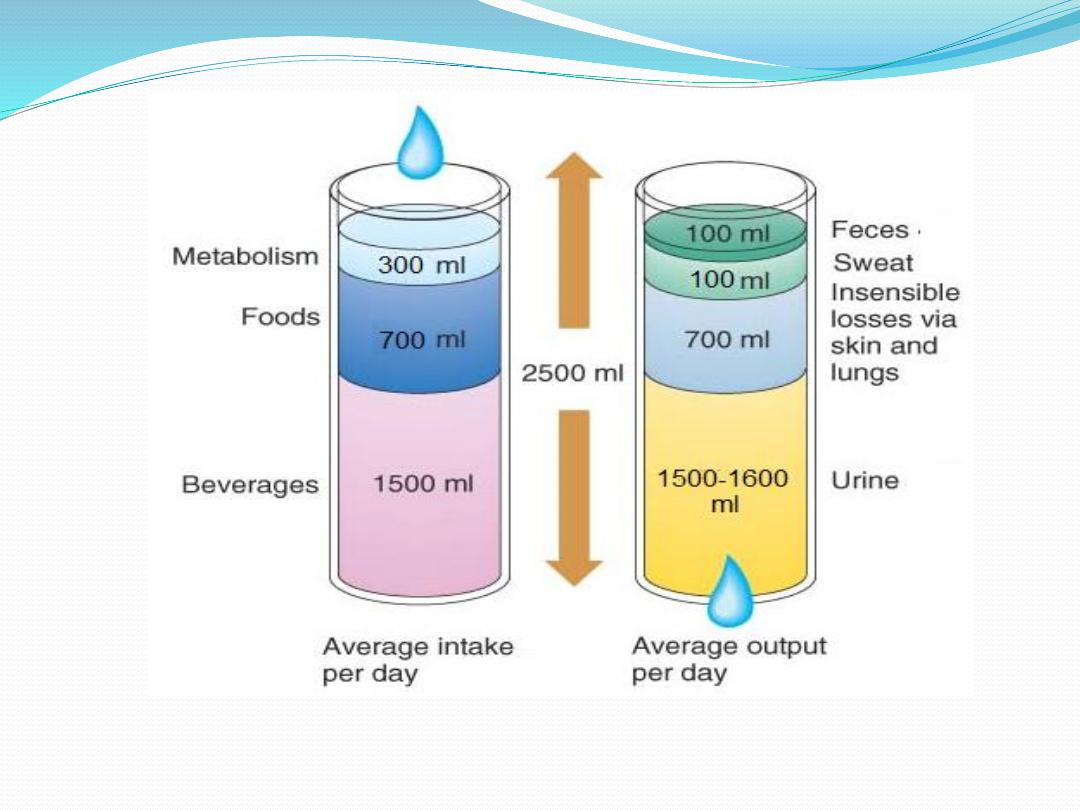
Water Balance
For the body to remain properly hydrated, water intake
must equal water output.
1.Water intake varies widely from person to person and is
strongly influenced by habit,but it is typically about
2500
m
l a day in adults. Most water enters the body through
it is ingested in the form of liquids or water in the food,
which together normally add about
2200 ml/day
to the
body fluids.
it is synthesized in the body as a result of oxidation of
carbohydrates, adding about 300 ml/day. This provides a
total water intake of about
2500 ml/day .
2. Water output occurs by several routes
insensible water loss , by evaporation from the respiratory
tract and diffusion through the skin, which together
account for about 700 ml/day of water loss under normal
conditions. When the cornified layer of the skin becomes
damaged, as occurs with extensive burns, the rate of
evaporation can increase as much as 10-fold, to 3 to 5 L/day.
For this reason, burn victims must be given large amounts
of fluid, usually intravenously, to balance fluid loss.
fluid loss in sweat, the amount of water lost by sweating is
highly variable, depending on physical activity and
environmental temperature.
The volume of sweat normally is about 100 ml/day, but
in very hot weather or during heavy exercise, water
loss in sweat occasionally increases to 1 to 2 L/hour.
water loss in feces, only a small amount of water (100
ml/day) normally is lost in the feces. This can increase
to several liters a day in people with severe diarrhea.
water loss by the kidneys, this is equal to 1.5-1.6 L/day.
The total water loss from the body will be about 2500
ml/day which is equal total water intake

Tonicity and intravenous fluid
Intravenous (IVF) fluid therapy is a common practice
today. It is an efficient and effective method of supplying
fluids directly into the ECF compartment, specifically the
venous system. An IVF effect on body fluid movement
depends in part on its tonicity, or concentration. This term
is sometimes used interchangeably with osmolarity,
although they are subtly different. Osmolarity is the
number of osmols or moles of solute per liter of solvent
plus solute. Tonicity is the relative osmolality of a solution.
Broadly, IV fluids are ordered for the following purposes:
1. to supply fluids when clients are unable to take in an
adequate volume of fluids by mouth. Example:
patients who are vomiting, patients with altered level
of consciousness, patients with disabilities or patients
under certain conditions cannot take in fluids orally.
2.to provide salts needed to maintain electrolyte
balance.
3.to provide glucose (dextrose), the main fuel for
metablism.
4.to provide water-solube vitamins and medications.
5. to promote a life line for rapidly needed medications
Common Type of Intravenous Solutions
Depending on its tonicity (the ability of the solute to cause
water movement from one compartment to another), the
intravenous solutions divided into:
1.Isotonic Solutions
The fact that it is isotonic means that the concentration of
solutes such as Na and Cl are equal in the intravenous
solutions and in the body's cells, so the water in the
solution is not attracted to osmose across the cell wall and
into the cell. This means the fluid will stay in the blood
vessels and support an increase in blood volume, resolving
the hypovolaemia.
Examples of isotonic fluids are
normal Saline Solution( 0.9% NaCl),
5% dextrose in water,
Ringer's solution( contains Na, K, Ca, Cl ),
Lactated Ringer's Solution (contains Na, K, Ca, Cl &
Lactate).
However, 5% dextrose in water is an isotonic fluid on initial
administration, but when glucose is metabolized, it
produces free water. This water may expand both the ICF &
ECF fluid volume, thus, acts as a hypotonic solution.
Furthermore, 5% dextrose in water when given in large
amounts may cause hyperglycemia.

2.hypotonic solution
A hypotonic solution would have a lower concentration of
solutes than the body cells, so fluid would leave the
circulation and enter the cells, causing swelling of the
tissues and cells. Examples of hypotonic fluids
0.45% NaCl (half strength normal saline),
0.33% NaCl ( one third strength normal saline)
2.5% Dextrose in water.
Hypotonic fluids are used to provide free water and treat
cellular dehydration,it also desirable to aid the kidneys in
elimination of solute via urine output.

3.hypertonic solution
A hypertonic solution would have a higher concentration of
solutes than the body cells, so fluid would leave the cells and
enter the blood circulation. This would be a good choice if the
patient was oedematous, but it could result in fluid overload and
cellular shrinkage. Examples of hypertonic fluids are
D5NSS (5% Dextrose in normal saline solution),
D5 in 0.45% NaCl ( 5% Dextrose in half strength normal saline)
, D5LR (5% Dextrose in Lactated Ringer's Solution),
D10W ( 10% Dextrose in water),
D50W50 (50% Dextrose in 50 ml of water).
Hypertonic solution draws fluids from the ICF causing cells to
shrink and ECF to expand. Therefore, its given to patients with
hyponatremias (Na deficits) with edema.

4.Nutrient Solution
Nutrient solutions contain some form of carbohydrates and
water. Water is supplied for fluid requirements and CHO for
calories and energy requirement. Nutrient solutions are useful in
preventing dehydration. However, it is a wrong notion to say that
dextrose increases weight, or promotes normal growth in
children or promotes wound healing or healing disorders. The
calories it provide are not for such purposes but mainly for
prevention of dehydration and ketosis. Common Nutrient
Solutions are:
D5W (5% Dextrose in water).
3.3% Glucose in 0.3% NaCl (Glucose in saline).
5% Dextrose in 0.45% NaCl (Dextrose in half strength saline).

5.Alkalyzing Solution
Alkalyzing solutions are administered to counteract or
prevent metabolic acidosis. Example....Lactated
Ringer's Solution.
6.Acidifying Solution
Acidifying slutions are administerd to counteract or
prevent metabolic alkalosis. Example... 0.9% NaCl
&/or D5NSS.
Primary causes of peripheral edema
1. Increased capillary hydrostatic pressure
, primary cause include:
Marked increase in blood flow, vasodilation in a given vascular bed.
Increasing venous pressure, venous obstruction or heart failure.
Elevated blood volume , heart failure.
2. Increased interstitial oncotic pressure the primary cause is thyroid
dysfunction (elevated mucopolysaccharides in the interstitium).These
act as osmotic agents resulting in fluid accumulation and a non-pitting
edema.
3.Decreased vascular oncotic pressure,
causes can include the
following:
Liver failure
Nephrotic syndrome

الحكمه
في
مخافه
هللا
النجاه
في قول الصدق
االمان في طلب العلم
الصحه
في اعطاء
الصدقه
طول العمر في صله الرحم
القوه في الصبر
دخول
الجنه
في بر الوالدين

4.Increased capillary permeability
, circulating agents,
e.g., tumor necrosis factor alpha (TNF-alpha),
bradykinin, histamine, cytokines related to burn
trauma, etc., increase fluid (and possibly protein)
filtration resulting in edema.
5.Lymphatic obstruction/removal (lymphedema),
causes can include
Filarial ( W. bancrofti-elephantitis).
Bacterial lymphangitis (streptococci).
Trauma.
Surgery.
Tumor.
Measurement of Fluid Volumes in the Different
Body Fluid Compartments
The Indicator-Dilution Principle
To measure the volume of a body compartment, a tracer substance
introduced into the compartment, allowing it to disperse evenly
throughout the compartment's fluid. Then the concentration of the
tracer in the compartment is measured, the volume of the
compartment can be calculated by using the following relationship:
Where A is the volume of compartment , A amount of tracer
introduced, and C is the concentration of tracer in the compartment.
For example, 300 mg of a dye is injected intravenously;
at equilibrium, the concentration in the blood is 0.05
mg/mL.
This is called the volume of distribution (VOD).

Properties of the tracer and compartment measured
Tracers are generally introduced into the vascular
compartment, and they distribute throughout body water
until they reach a barrier they cannot penetrate. The two
major barriers encountered are capillary membranes and
cell membranes. Ideal tracers should be
well distributed within that compartment, and
not rapidly metabolized or removed from that
compartment. Thus, tracer characteristics for the
measurement of the various compartments are as follows:
•
Plasma
: tracer not permeable to capillary
membranes, e.g., Evans blue dye (T-1824) and
125
I-
albumin.
•
ECF
: tracer permeable to capillary membranes but
not cell membranes, e.g.,
22
Na,
125
I-iothalamate,
thiosulfate, inulin, mannitol, sodium, and sucrose.
•
Total body water
: tracer permeable to capillary and
cell membranes, e.g., radioactive water (tritium, 3H
2
O)
or heavy water (deuterium, 2H
2
O), antipyrine, and
urea.
Blood Volume versus Plasma Volume
Blood volume represents the plasma volume plus the
volume of RB Cs, which is usually expressed as hematocrit
(fractional concentration of RB Cs). The following formula
can be utilized to convert plasma volume to blood volume:
For example, if the hematocrit is 50% (0.50) and plasma
volume= 3 L, then:

PHOSPHATE BALANCE
A normal plasma concentration of inorganic phosphate is
about 1 mmol/L. Phosphate plays a variety of roles in the
body: It is an important constituent of bone; it plays a
critical role in cell metabolism, structure, and regulation
(as organic phosphates); and it is a pH buffer. Phosphate is
mainly unbound in the plasma and freely filtered by the
glomeruli. About
60 to 70%
of filtered phosphate is actively
reabsorbed in the proximal convoluted tubule and another
15%
is reabsorbed by the proximal straight tubule via a
Na+-phosphate cotransporter in the luminal plasma
membrane. The remaining portions of the nephron and
collecting ducts reabsorb little, if any, phosphate. The
proximal
tubule
is
the
major
site
of
phosphate
reabsorption.

Only about
5 to 20%
of filtered phosphate is usually
excreted. Phosphate in the urine is an important pH buffer
and contributes to titratable acid excretion. Phosphate
reabsorption is Tm limited and the amounts of phosphate
filtered usually exceed the maximum reabsorptive capacity
of the tubules for phosphate. If more phosphate is ingested
and absorbed by the intestine, plasma [phosphate] rises,
more phosphate is filtered, and the filtered load exceeds
the Tm leading to increase phosphate excretion. While in
cases of phosphate depletion, the kidneys filter less
phosphate and the tubules reabsorb a larger percentage of
the filtered phosphate. Thus, the kidneys participate in
regulating the plasma phosphateof by an “overflow” type
mechanism.

When there is an excess phosphate in the body, they
automatically increase phosphate excretion, and when there is
low phosphate in the body, they automatically decrease
phosphate excretion Phosphate reabsorption in the proximal
tubule is controlled by a variety of factors. PTH can play a
significant role in regulating phosphate concentration through
two effects:
(1) PTH promotes bone resorption, thereby dumping large
amounts of phosphate ions into the extracellular fluid from the
bone salts, and
(2) PTH decreases the transport maximum for phosphate by the
renal tubules, so that a greater proportion of the tubular
phosphate is lost in the urine. Thus, whenever plasma PTH is
increased, tubular phosphate reabsorption is decreased and more
phosphate is excreted