


Myofunctional appliances




Myofunctional Appliances (MFA)
They are removable or fixed (cemented) appliances that mostly alter the posture of the mandible (designed to correct class II malocclusion, primarily by forwards posturing of the mandible in a growing child) and transmit the forces created by the resulting stretch dental and skeletal tissues to produce movement of the teeth and growth modification to the jaws and lower facial third.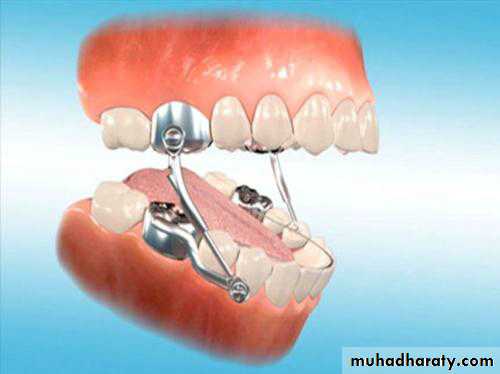
Clinical use of functional appliances
The ideal case for treatment with a functional appliance should have the following clinical features:•Increased overjet and class II buccal segment relationship;
•Mild to moderate skeletal class II base;
•Average to reduced lower face height;
•Proclined maxillary incisors;
•Retroclined mandibular incisors; and
• Active growth (Favourable growth pattern).
Advantages and disadvantages of MFA
It produce dentoalveolar and favourable growth of the jaw. The appliance must be worn for long hours.
Reduce treatment time and severity
Critical treatment time.
Needs well cooperative patient.
Needs fixed appliance after finishing
Theories on how functional appliances work
Functional appliances effect their changes by posturing the mandible forwards. This postural correction is fundamental to the appliances’ mode of action and influences four principal regions:• Orofacial soft tissues; • Muscles of mastication;
• Dentition and occlusion; • Facial skeleton.
Clinical effects of functional appliances
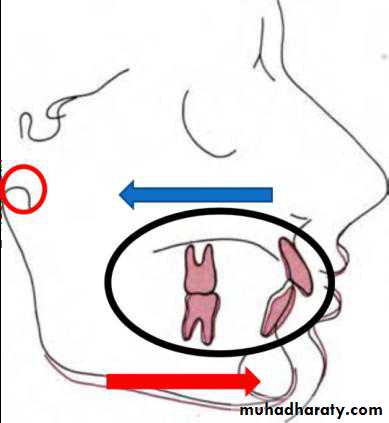
Numerous types and designs of functional appliance have been described, each with its own treatment philosophy. In essence, all of these appliances have similar effects, with the most significant being dentoalveolar change:• Retroclination of maxillary incisors;
• Proclination of mandibular incisors;
• Distal tipping of the maxillary dentition;
• Mesial eruption of the mandibular buccal dentition;
• Restraint of forwards maxillary development; and
• Forwards movement of the mandible due to small additional growth at the condyle and remodelling of the glenoid fossa.
The treatment results depend on the following:
1) Amount of forceThe force magnitude should be high or at least (400- 600 gm) per each side to make sure that only skeletal and no dental movements takes place. Such high forces produce hyalinization of the bony socket which prevents tooth and thus only orthopaedic movement is seen.
2) Duration of force
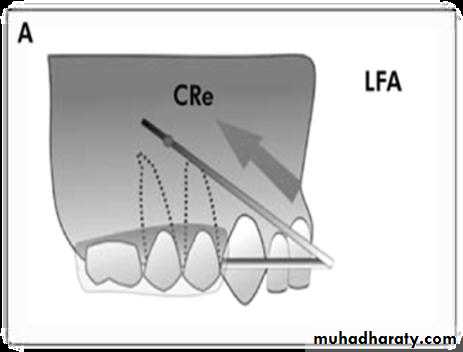
According to most authors, intrmittent forces produce skeletal changes whereas continuous forces produce dental movement. MFA should be worn for about 12- 14 hr/day to bring about the desired effect. Increasing the duration beyond the optimum range increases the dental effects. An intermittent heavy force is less harmful to the teeth and periodontium than a continuous heavy force.3) Direction of force: The direction of force application should be such as to maximize the skeletal effect. A favourable skeletal effect is seen when a force is directed postero-superiorly through the center of resistance of maxilla.

4) Age of the patient
MFAs are most effective during the late mixed dentition period as it takes the advantages of prepubertal growth spurt. However, treatment should be maintained till growth is complete as these appliances change only the expression of growth rather than the underlying growth pattern.5) Time of force application
There is evidence that there is an increase in the release of growth hormones more during the evening and night and is associated with the sleep onset. Therefore, it is advisable for the child to wear the appliance in the evening and throughout the night. Generally the child is more likely to wear it at night .Functional appliances should be used when the patient is growing. As girls complete their growth slightly earlier than boys, MFAs can be used a little latter in males.
Types of MyoFunctional Appliances
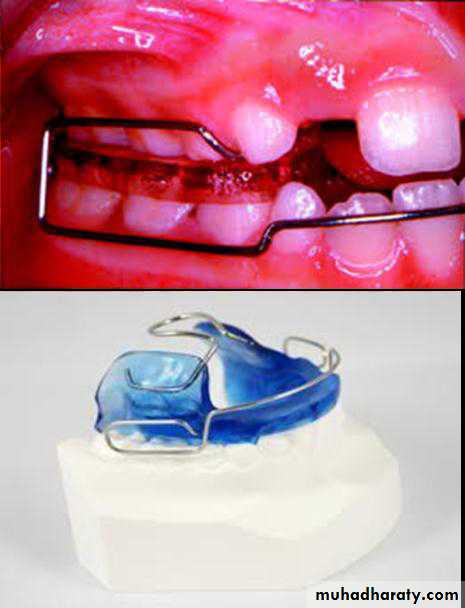
1)Oral screenThe appliance is the oldest type of functional appliances. Is a thin shield of acrylic which lies in the buccal sulcus. It is worn at night. In its passive form it transmits the forces of the circumoral musculature uniformly to the teeth.
Indications:
• As a retainer ( passive)
• Discourage thump sucking
C) The active oral screen has been used for overjet reduction in cases where there is sufficient incisors spacing to allow OJ reduction.
2) Andresen Activator (Monoblock)
It is a tooth born removable appliance consist of upper and lower appliances sealed together and holded the lower jaw in forward position to guide tooth eruption into a more desirable bite while helping the upper and lower jaws grow in proportion with each other.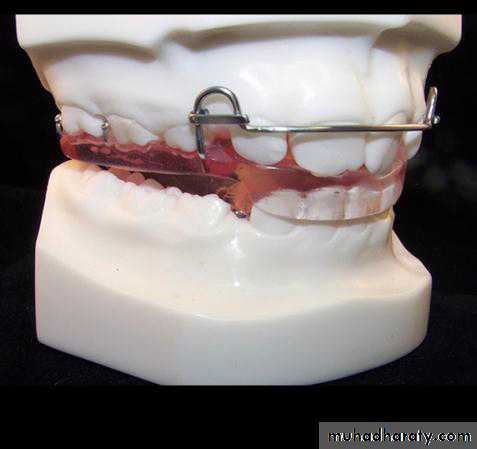
It was based upon the hypothesis of stimulating increased muscle activity in the mandibular elevator and retractor muscles to act directly on the dentition through the appliance and unload the condyle to allow remodelling and growth. patient cooperation in wearing this appliance is essential for successful improvement.
Mainly used in cases with Cl.II div.1 with mandibular deficiency.
Bite registration
Symmetrical position of the mandible. The bite should be opened 2mm beyond the free way space.
If the overjet is 10 mm or less, this will generally mean the postured bite can be taken with the incisors in an edge-to-edge relationship. If greater than 10 mm, it is unlikely that full overjet reduction can be achieved with a single appliance. Rather, the appliance may need reactivating, either by adjusting it so the mandible is postured further forwards or by fabricating a second appliance once the overjet has been partially reduced.
Trimming of acrylic (appliance adjustment)
The interdental acrylic in the buccal segments has been trimmed to make a series of inclined planes which guide the eruption of the upper molars and premolars buccaly and distally. While the lower buccal segment will be guided mesially and buccaly (forward movement of the lower jaw). The distal movement is intended to help correct the Class II buccal segment relationship.3) Bionator
It is best described as cut-down activator. The reduced bulk of the appliance making it more comfortable to the patient (increased wearing) and ensure normal oral function. The appliance also has the ability to reposition the mandible and modify dental eruption. Developed 1rst by Balter. It is indicated for: Class II and III malocclusion.
It is a tooth born appliance. A palatal coffin spring was incorporated into the appliance and designed to sit away from the palate, stimulating the tongue to adopt a more anterior position and helping to stabilize the bionator in the oral cavity. Buccal wire shields were also incorporated to hold the cheeks away from the buccal segments and allow passive expansion of the dental arches.
Activators combined with headgear
Functional appliance wear can encourage a clockwise rotational effect on the dentition and dental bases, which can lead to an increase in the lower face height and greater vertical rather than sagittal change in chin position. To prevent this and optimize skeletal correction in the anteroposterior dimension, headgear can be attached to the appliance. These are: The Teuscher appliance
The Van Beek appliance
The Dynamax appliance

4) Frankle appliance
It is a tissue born functional appliance, also it has some contact with the teeth (bite blocks). Much of the appliance is located in the vestibule.Frankle appliance originally called the function regulator (FR). Frankel was an advocate of the functional matrix theory of growth, which states that there is no direct genetic influence on the size, shape or position of the skeletal tissues. Rather, bony growth is driven by form and function of the surrounding soft tissues.
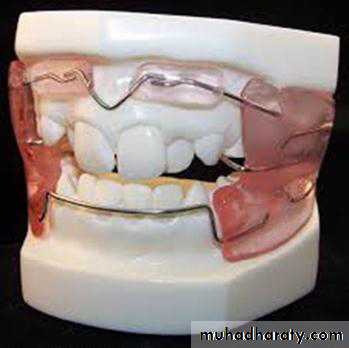
It looks very different as having acrylic shields in the buccal sulci and little or no acrylic lingually. Heavy wires and buccal shields are intended to cause passive expansion of the arches by holding the cheeks and lips away from the teeth, so disturbing the muscle balance and also to enlarge the alveolar process by stretching the periosteum in the depth of the vestibule (in theory),
as well as encouraging forwards posture of the mandible. The treatment philosophy is based upon full-time wear, but the bulk and fragility of the appliance can make compliance difficult.
There are different types of Frankle appliances according to the type of malocclusion:
(1)FR I is for treatment of Class II div.1 (OJ less than 7mm) malocclusion and incorporate lip pads labial to the lower incisors to allow forward development of the mandibular alveolar process.(2) FR II is for treatment of Class II div.2, so it has in addition a palatal wire to procline the upper incisors.
(3) FR III is for treatment of Class III malocclusion having acrylic shields labial to the upper incisors which together with a palatal arch to procline them and a lower labial bow which retroclines the lower incisors.
(4) FR IV is for open bite cases.
5) The twin block appliance
The unique feature of this appliance is that its constructed in two parts as separate upper and lower appliances. Forward mandibular posturing is achieved by incorporating buccal blocks with interlocking inclined planes (The inclined planes of these blocks are set at approximately 70°with the height greater than 5 mm vertically to ensure that the patient occludes with the lower block in front of the upper and not on it. It is a tooth born appliance.Twin block appliance is most comfortable and aesthetic of all functional appliances. The patient can eat and speak normally (movement of the jaws is not restricted).

The twin block also carries a number of other advantages:
• Upper arch expansion can be achieved by incorporating a midline expansion screw.• Headgear can be easily attached to the upper appliance in cases with maxillary protrusion.
• Fixed appliances can be placed to start alignment of the labial segments without compromising retention of a twin block; and
• This appliance is robust and relatively easy to fabricate.
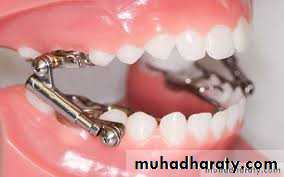
6) Herbst appliance (bite-jumper)
Its a tooth born appliance. It can be either fixed (cemented or bonded) or removable appliance. The maxillary and mandibular arches are splinted with frameworks that is usually are cemented or bonded but can be removable, and connected with a pin- and- tube device that hold the mandible forward. It is now one of the most widely used functional appliances for class II correction. The original design used bands on the first molars and premolars. For better anchorage and robustness, Pancherz now recommends using cobalt-chromium cast splints for the super-structure.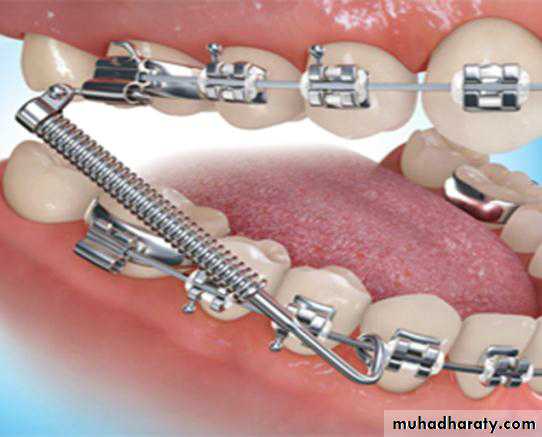
The fixed nature of this appliance means that effective compliance is not usually an issue and overjet reduction in 6–8 months is commonly achieved.
This appliance encourage the lower jaw to grow in a forward direction by positioning it forward and holding it there. It also has the ability to push the upper molars backwards.
End of treatment with functional appliance and retention
Once the overjet is corrected and due to the tendency of the original growth pattern to re-establish itself following treatment; wear of the appliance should be continued on a part-time basis to retain the sagittal correction and allow occlusal settling (to close the transient lateral open bite that happen at the end of treatment). This can include part-time wear of a cut-down functional appliance or a removable appliance with an inclined anterior bite plane.7) Exra Oral Devices
A)HeadgearHeadgears are the most common among all the orthopaedic appliances. They are ideally indicated in patient with excessive horizontal growth of the maxilla with or without vertical changes along with some protrusion of the upper teeth. Reasonably good mandibular dental and skeletal morphology. They are most effective in the prepubertal period.
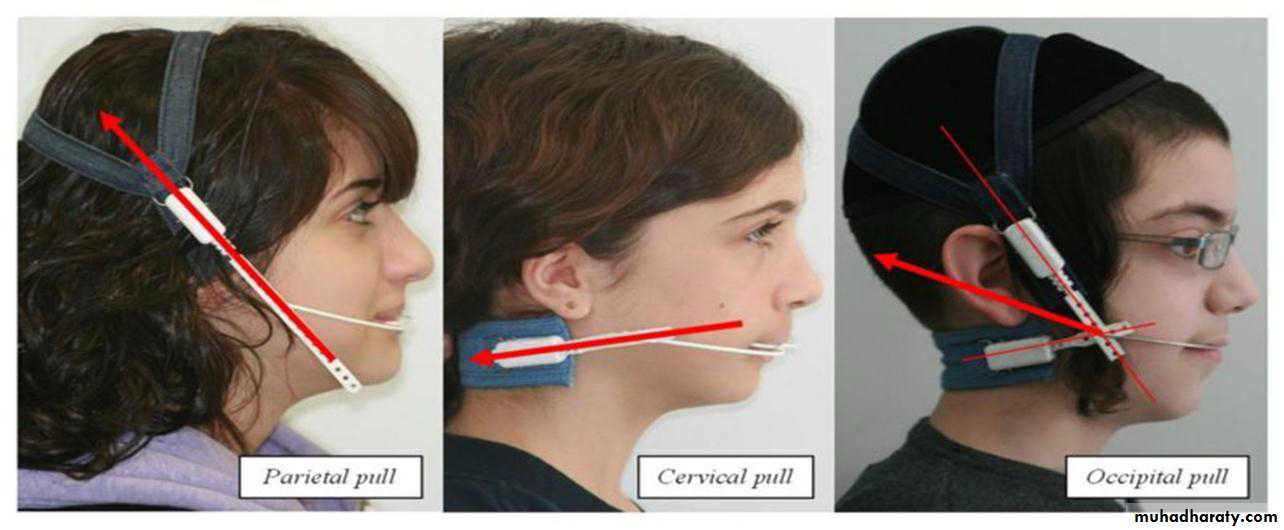
Headgears can also be used to distalize the maxillary dentition along with the maxilla. They are an important adjunct to maintain anchorage.
Components:
1-Force delivering unit (face bow, J hook).
2- Force generating unit
3- Anchor unit (head cap, neck strap).
b) Face mask (Delare mask)
Class III malocclusion is usually a result of a combination of maxillary deficiency and mandibular excess. Growth modification for class III problems is the reverse of class II, i.e.treatment involves restriction of mandibular growth along with downward and forward maxillary growth by heavy extra oral elastics attached to hooks on a rigid frameworks. When headgear applies a distal force to the maxilla, compression of the maxillary sutures can inhibit forward maxillary growth.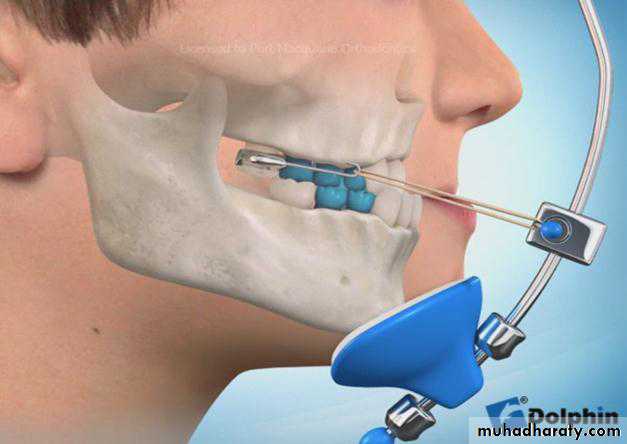
Likewise, pulling the maxilla forward, opening or seperation of the sutures should stimulate forward growth of the maxilla. Headgears which cause forward pull on the maxilla are, therefore, called reverse pull headgear. It gain anchorage from chin and forehead. This appliance is indicated for patient with mild to moderate skeletal Class III malocclusion, mainly due to maxillary retrusion.
Force= 450 gml side
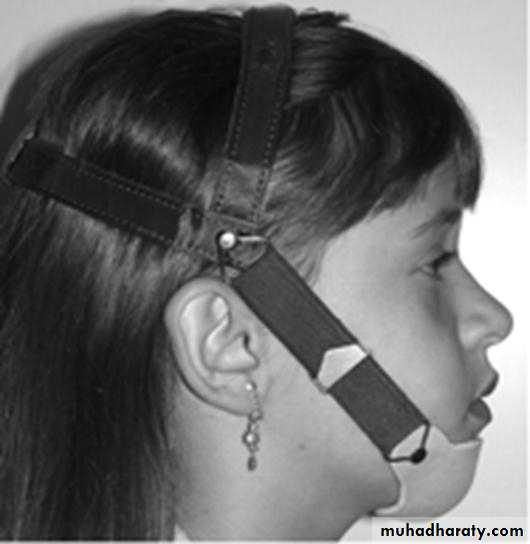
c) Chin capIt is used in Class III malocclusion. The appliance utilizes a head cap, which is firmly fitted/seated on the postero-superior aspects of the cranium as anchorage and has attachments for the placement and activation of the chin cap.
The effects of the chin cap:
Redirection of the mandibular growth in a downward
and backward direction.
Remodeling of the mandible and a decrease in the
mandibular plane angle.
Lingual tipping of the mandibular incisors.
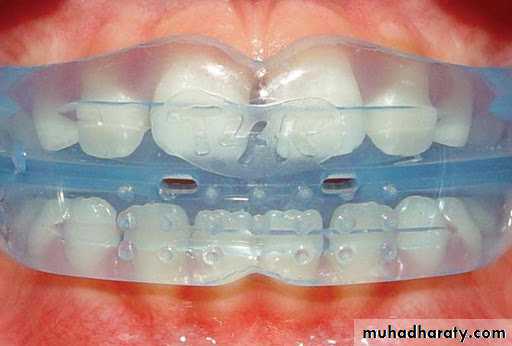
Myofunctional Trainers Appliance System
Pre-orthodontic trainers or the myofunctional trainers are new types of prefabricated removable functional appliances which according to the manufacturer‘s claims, train and exercise the orofacial muscles into their correct position and bring about a state of equilibrium between the forces delivered onto the dento-alveolar system.
Myofunctional Trainers Appliance System
They have possibility to reeducate masticatory and facial muscles, improve the position of tongue and more actively than any other known functional appliance helping in alignment of the teeth and stimulating proper growth and development of the craniofacial system.In 1992, the Pre-Orthodontic Trainer for Kids™ (T4K®) was introduced by Myofunctional Research Company, Australia, followed by other appliances of The Trainer System™. It consists of various appliances for different age groups, each available in single size.
They consist of phase I and phase II appliances wherein phase I appliances are made of silicone and phase II appliances are made up of harder material like polyurethane

Mechanism of Action of Trainer Appliances
The effects of Trainer system appliances produces sagittal effect similar to that achieved with other functional appliances designed to stimulate mandibular growth by leading the mandible forward into the edgetoedge position. Leading the mandible in anterior position, stretches muscular fibers of mandible protractors (masseter, medial pterigoid and lateral pterigoid muscles). During the period of 10-12 hours of using the Trainer appliance (during sleep) muscles remain stretched; the diameter of blood vessels is reduced hindering sufficient blood flow and decreasing oxygenation and metabolism.These conditions cause muscular fatigue due to the accumulation of lactic acid in muscles. When the appliance is removed, protruding muscles become hypercontractible moving the mandible forward and backward. Subsequent muscular hypercontractibility after several hours of stretching muscle fibers leads to increased blood flow and removal of accumulated lactic acid.
At the same time, increase in blood flow in muscles brings more undifferentiated cells with the ability to differentiate into myoblasts causing production of new muscle fibers in protractors. The increase in muscle fibers and trained muscles in further treatment allow keeping the mandible in anterior position without having muscle fatigue.
Another effect of the Trainer reported in the literature is the stimulation of transversal development of dental arches ,the intercanine, interpremolar and intermolar distance of dental arches. The mechanism of this effect is similar to the Fränkel function regulator.
Trainer system appliances are used in accordance with indications and patient’s age, including :
Infant Trainer intended for use in children 2-5 years old,
Trainer for children with mixed dentition (T4KTM),Trainer for adolescents/adults (T4ATM),
Trainer the Brackets (T4BTM),
Trainer for class II malocclusion (T4CIITM),
Trainer for class III malocclusion (i3),
Trainer Lingua and Myobrace.