• Specific disorders
:
bacterial pneumonia :
The major purpose
of CXR in patients with suspected chest infection is to establish
whether or not pneumonia is present.
• Diagnosing the responsible infectious agent is rarely possible on
radiological grounds.
• The basic radiological feature of pneumonia is one or more areas
of consolidation, varying from a small, ill defined opacity to a large
opacity involving the whole of one or more lobes .
• Consolidation may be accompanied by loss of volume of the
affected lobe , a feature that is particularly common in children.
• Cavitation may occur within the consolidated areas. Cavitation is a
particular feature of infections with staphylococci, Gram negative
and anaerobic bacteria and tuberculosis.
• The differentiation between pneumonia and pulmonary oedema
or pulmonary infarction may, at times, be difficult or impossible
radiographically.
• A common infecting organism in community-acquired lobar pneumonia is
Streptococcus pneumoniae (pneumococcal
pneumonia).
• In pneumococcal pneumonia, there is usually 1- dense consolidation of a
considerable portion of one lobe, 2- usually without loss of volume. 3-
There may be an associated pleural effusion.
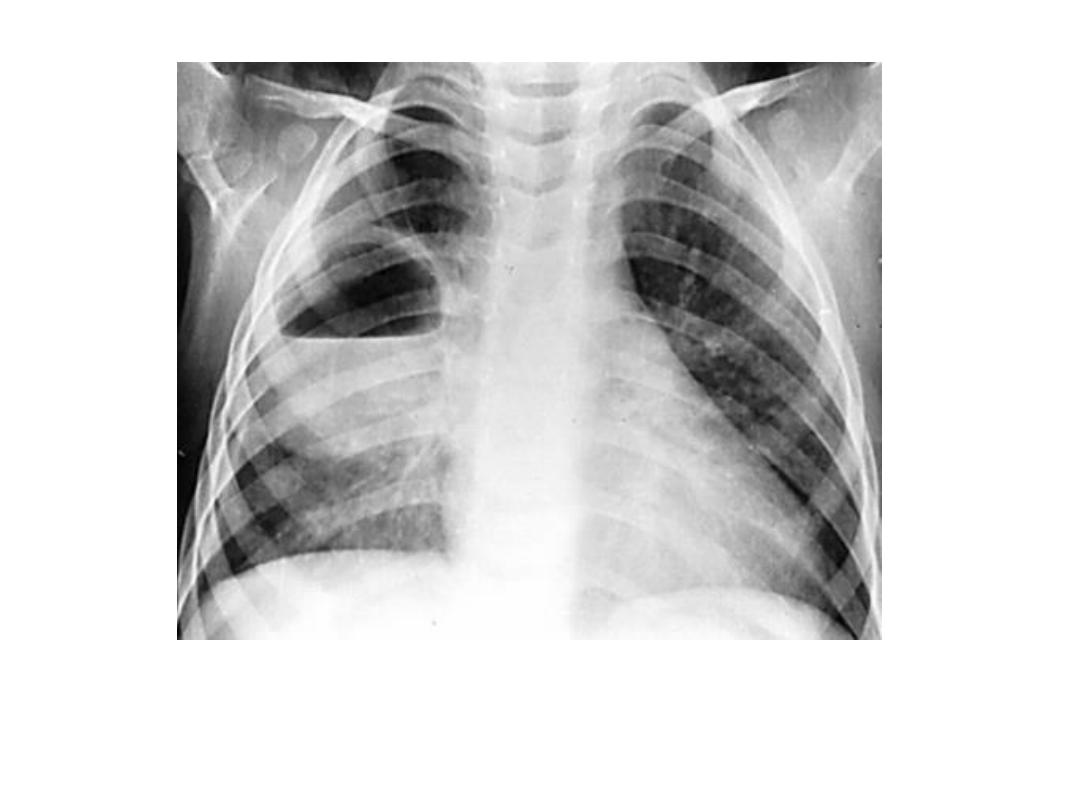
• When the consolidation is patchy, involving one or more lobes, it is
commonly referred to as bronchopneumonia, The most frequent causes of
community acquired bronchopneumonia are
Staphylococcus aureus,
various Gram-negative and anaerobic bacteria and
Mycoplasma
pneumoniae.
• Pneumonia may be secondary to obstruction of a major bronchus,
carcinoma being a common cause of obstruction.
• Bronchial obstruction should always be considered in any patient presenting
with consolidation of one lobe, or of two lobes supplied by a common
bronchus (e.g. the right middle and lower lobes), particularly if there is
associated loss of volume.
• Viral and Mycoplasma pneumonia
:
Viral pneumonia and pneumonia due to
Mycoplasma pneumoniae
may produce 1- widespread ill-defined
consolidation and 2- loss of clarity of the vascular markings , which on
occasion may resemble pulmonary oedema. 3- Alternatively, only a
localized area of consolidation may be seen. 4- Pleural effusions are rare. 5-
The radiological abnormality may persist for many weeks after clinical
recovery.
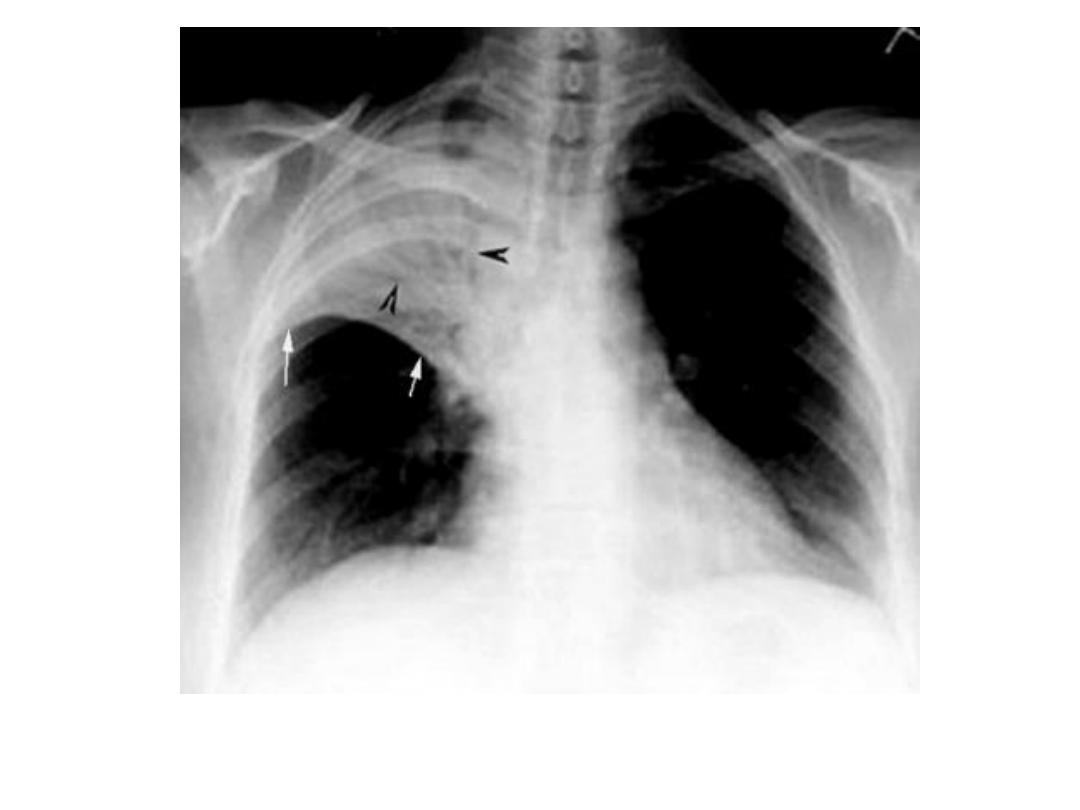
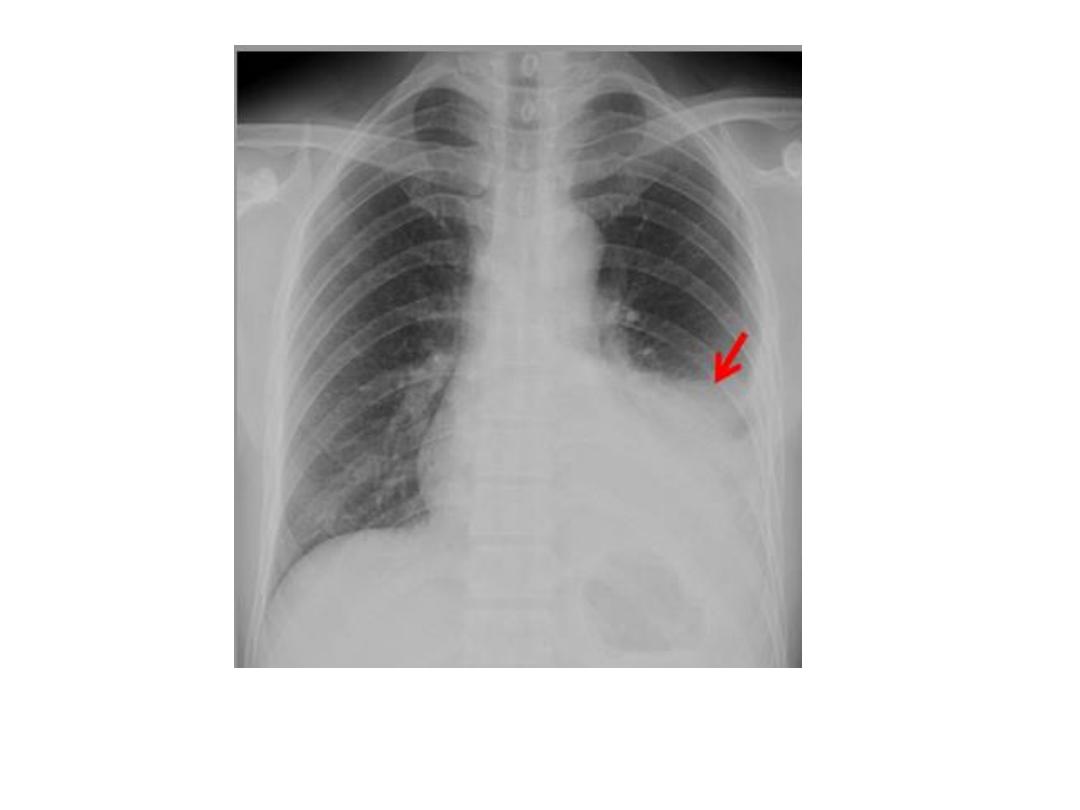
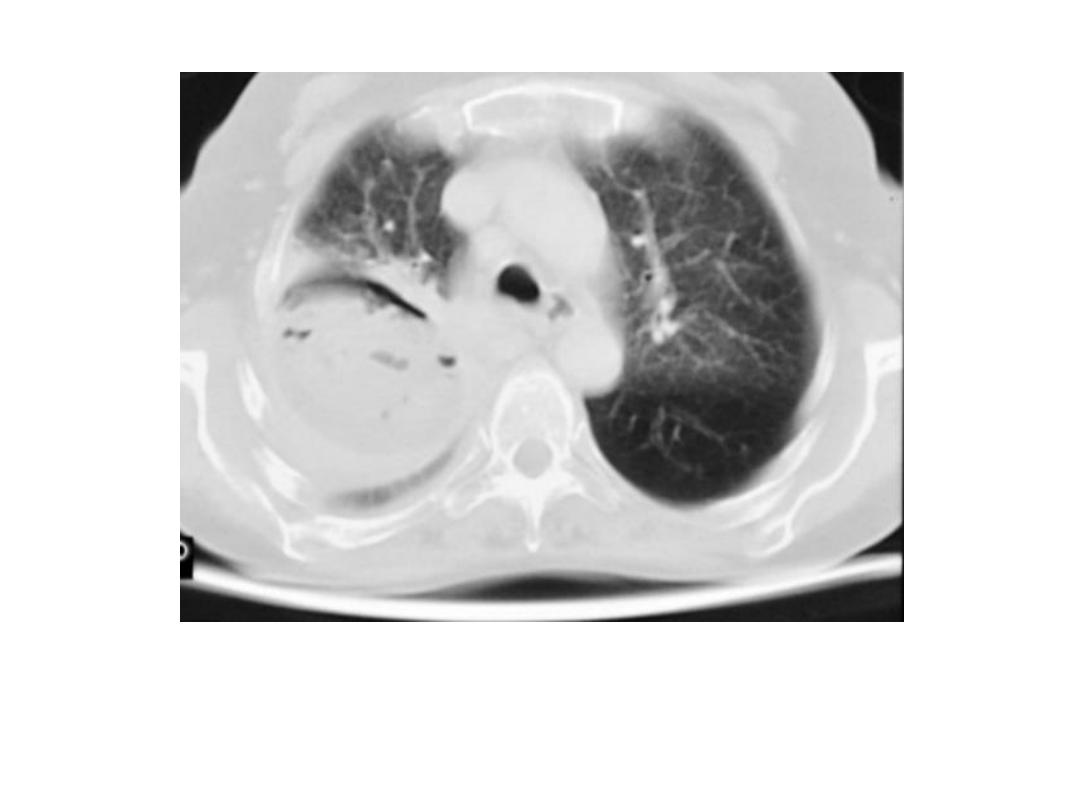
• Lung abscess : A lung abscess is a localized suppurative lesion of the lung
parenchyma.
• The most frequent causes are:
1- Aspiration of food or secretions: Such abscesses are usually in the apical
(superior) segments of the lower lobes or in the posterior segments of
the upper lobes.
2- Infection beyond an obstructing lesion in the bronchus.
3- Infected emboli, particularly in drug addicts.
• A lung abscess is usually seen as a spherical opacity containing a central
lucency due to air within the cavity, An air–fluid level may be present.
• Pulmonary TB : Pulmonary tuberculosis is usually divided into primary
and postprimary forms.
• Primary tuberculosis is the result of the first infection with
Mycobacterium tuberculosis and usually occurs in
childhood.
• Postprimary tuberculosis, the usual form in adults, is believed to be re-
infection, the patient having developed relative immunity following the
primary infection.
• Tuberculosis (and atypical mycobacterial infections) is seen commonly in
patients with acquired immune deficiency syndrome (AIDS).
• Primary TB : In primary tuberculosis, A- an area of consolidation, known as the Ghon
focus, develops in the periphery of the lung usually in the mid or upper zones.
Usually, the pulmonary opacity is small, but it may occasionally involve most of the
lobe.
• B- The consolidation is often accompanied by visibly enlarged hilar or mediastinal
lymph nodes , This combination of pulmonary consolidation and lymphadenopathy is
known as the
primary complex.
• C-In most cases, whether treated or not, the primary complex heals and often
calcifies, A calcified primary complex often remains visible throughout life.
• D-Spread of primary tuberculous infection may occur via two routes:
• 1 The bronchial tree, leading to tuberculous bronchopneumonia: This appears
radiologically as patchy or lobar consolidation; it often involves more than one lobe,
may be bilateral and frequently cavitates.
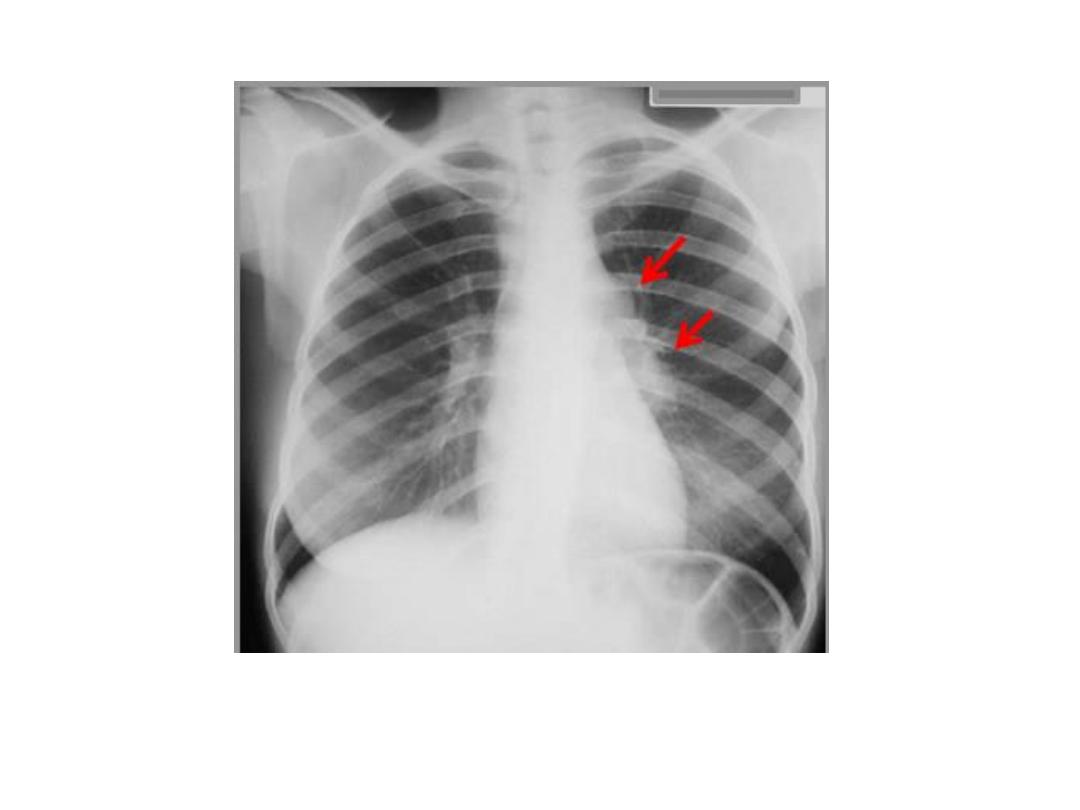
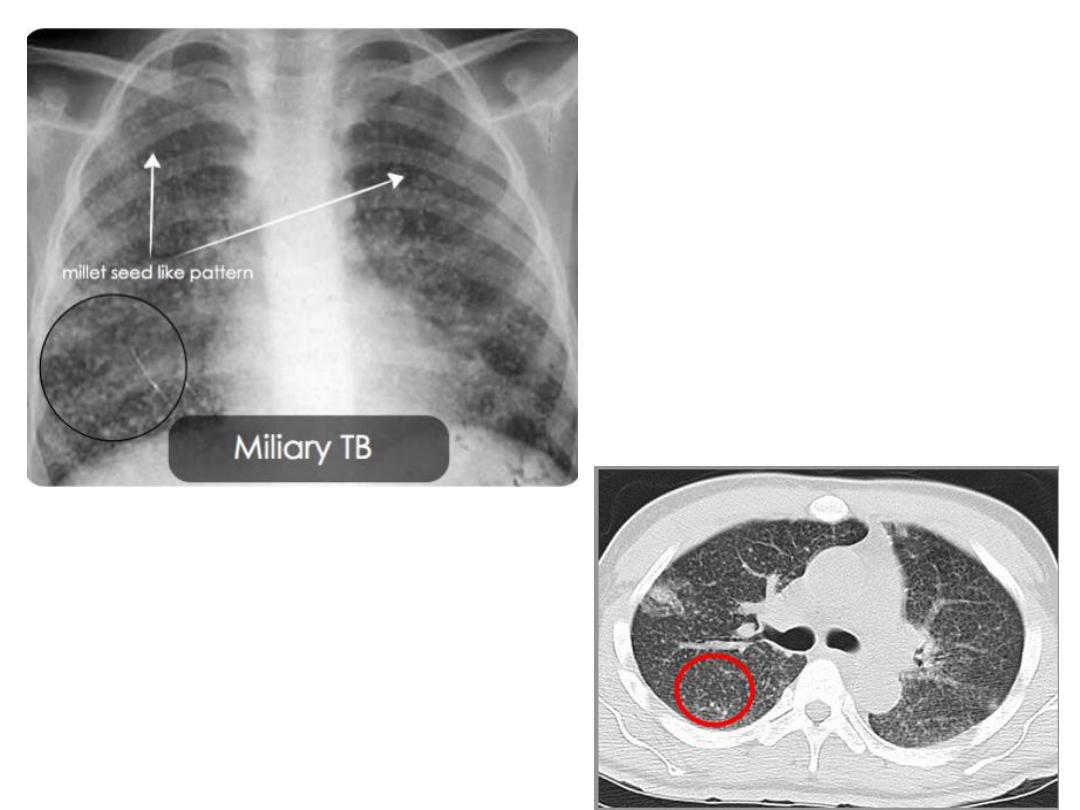
• 2 The blood stream, resulting in
miliary tuberculosis :
in which there are
innumerable small nodules in the lungs, all much the same size and fairly evenly
distributed.
• Usually, the nodules are well defined but in severe cases they become relatively
confluent so that the individual nodules are difficult to appreciate.
• A pleural effusion may be present.
• It is important to note that the chest film may be normal in the early stages of miliary
tuberculosis.
• Primary tuberculosis may present with a pleural effusion.
• Occasionally the primary complex is also visible, butmore often the effusion is the only
visible abnormality.
• Post primary TB : Postprimary tuberculosis usually presents with cough,
haemoptysis, weight loss, night sweats or malaise. Occasionally, the disease is
discovered on a routine chest film. Postprimary tuberculosis is usually confined
to the apical and posterior segments of the upper lobes and the apical
segments of the lower lobes, though may present as a lower or middle lobe
bronchopneumonia.
• The initial lesions are multiple small areas of consolidation , and are often
bilateral.
• Pleural effusions are frequent and may be the only radiographic abnormality.
• The predominant or sole feature, particularly in non-Caucasians, may be
mediastinal and/or hilar lymphadenopathy .
• If the infection progresses, any areas of consolidation may enlarge and
frequently undergo cavitation.
• Cavities are seen as rounded air-spaces (translucencies) completely surrounded
by pulmonary opacification .
• As with the primary form, postprimary tuberculosis may spread to give
widespread bronchopneumonia or miliary tuberculosis.
• The infection may undergo partial or complete healing at any stage.
• Healing occurs by fibrosis, often with calcification, but both fibrosis and
calcification may be seen in the presence of continuing activity.
• Pleural effusions often leave permanent pleural thickening which may, on
occasion, calcify.
• Tuberculoma : The term tuberculoma refers to a tuberculous granuloma in the
form of a spherical mass, usually less than a centimetre or two in diameter, and
mostly much smaller.
• The edge is usually sharply defined and the lesions are often partly calcified.
• CT may be needed to demonstrate the calcification.
• Tuberculomas are almost invariably inactive even though viable tubercle bacilli
may be present deep within the lesions.
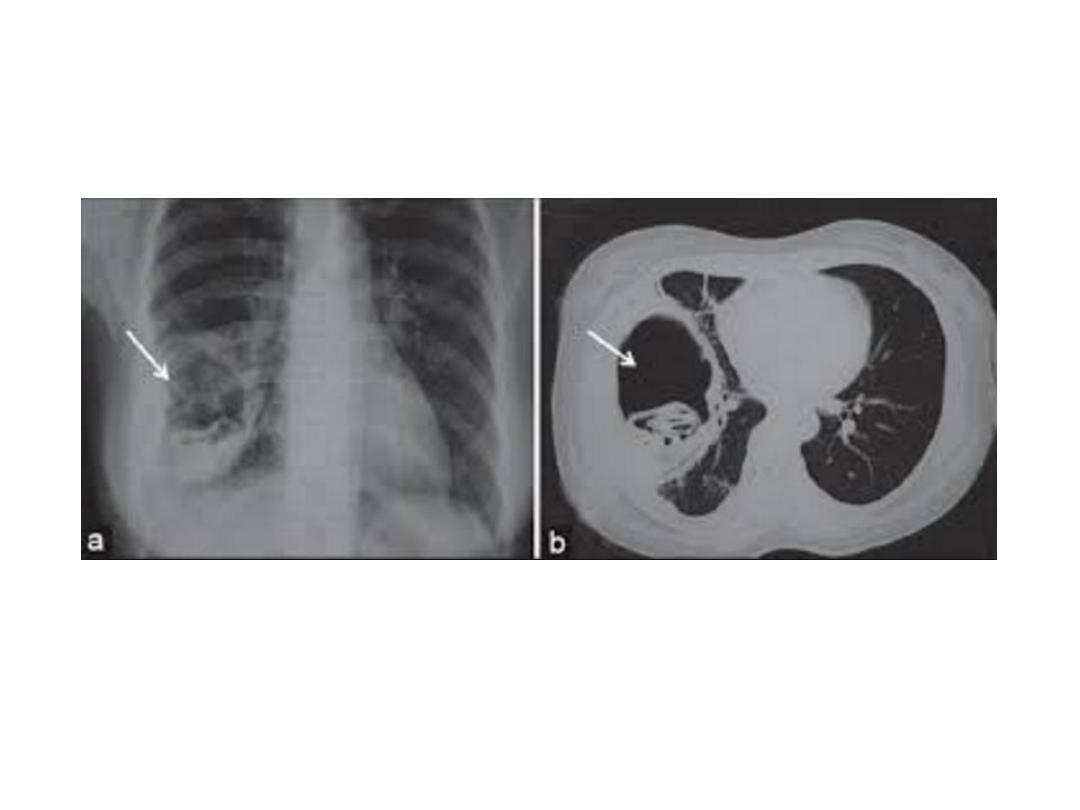
• Mycetoma : The fungus
Aspergillus fumigatus may colonize old tuberculous
cavities to produce a ball of fungus (mycetoma) lying free within the cavity .
• Air is seen between the mycetoma and the wall of the cavity. Cavities
containing mycetomas are usually surrounded by other evidence of old
tuberculous infection, particularly fibrosis and calcification of the adjacent lung.
• CT often allows a specific diagnosis of mycetoma to be made.
• Is the TB is active ? Valuable diagnostic signs of activity are:
1- development of new lesions on serial films
2- demonstration of cavities.
• Lack of change over a period of years is useful evidence against activity, but the
progression on serial chest films may be subtle, even with active disease.
• Many routine chest films in asymptomatic patients show evidence of previous
tuberculosis.
•
In a few, the diagnosis of active disease is readily apparent by the presence of cavities or by
comparison with previous films.
•
In the remainder it can be a considerable problem to decide which patients to investigate further
and which to accept as having old inactive disease.
•
The better defined the opacities and the greater the degree of calcification, the less the likelihood of
activity. The presence of ill-defined opacities, even if partially calcified, is suggestive of active
disease.
•
However, the decision is often largely based on the clinical findings and the results of sputum
examination for tubercle bacilli.
•
It is important to realize that there is no way of excluding activity radiologically unless serial films
show no change in the appearances over a prolonged period of time.
•
Fungal and parasitic diseases : When fungi are inhaled they may produce lung infection.
•
The radiological appearances vary with the particular fungus, but two broad divisions can be made:
•
1 Infection of an otherwise normal patient. Organisms such as histoplasmosis, coccidioidomycosis
and blastomycosis , produce lung lesions that are very similar and often identical to tuberculosis.
•
Cavitation is a particular feature.
•
Healing by fibrosis and calcification is frequent.
•
2 Infection in an immunocompromised host. With impaired immunity, fungi such as
Candida
albicans and Aspergillus fumigatus,
may cause widespread pneumonia.
•
It is not possible to predict the infecting organism from the chest film , although recognized signs on
HRCT include multiple nodularities with surrounding ground glass appearances.
•
Aspergillus fumigatus
affects the lung in three ways: (i) it
may colonize a pre-existing cavity forming
a fungus ball (mycetoma) ; (ii) it may infect the lung in an immunocompromised patient causing
severe pneumonia ; or (iii) it may be responsible for allergic bronchopulmonary aspergillosis.
•
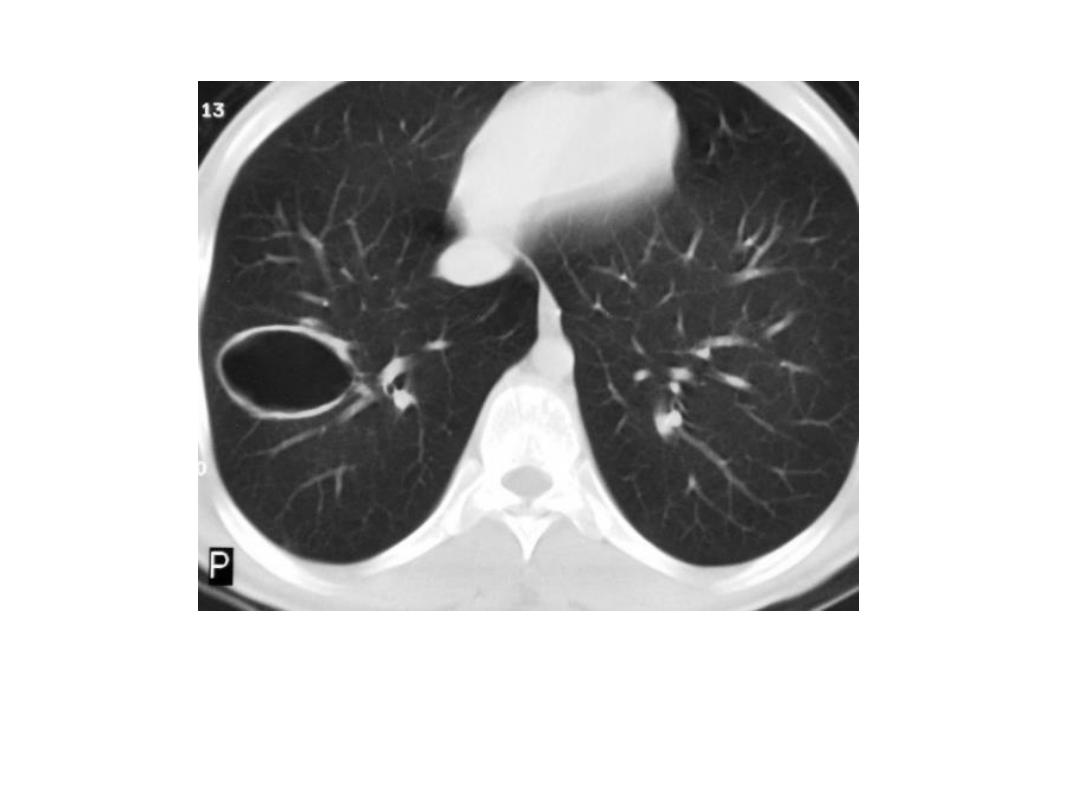
Hydatid disease : Pulmonary infection with
Echinococcus granulosus may
result in cysts in the
lung or pleural cavity.
•
These cysts may be solitary or multiple and are seen as spherical opacities with very well-
defined borders. Hydatid cysts occasionally rupture to produce complex cavities.
•
Pneumonia in the immunocompromised host : Pneumonia in these patients may be due to
the usual pathogens, but often it is due to opportunistic fungi, tuberculosis or
Pneumocystis
carinii.
•
Pneumonia in immunocompromised patients usually causes widespread non-specific
pulmonary opacification. It may not even be possible to say whether the opacification is due to
infection or to such conditions as pulmonary oedema, pulmonary haemorrhage or neoplastic
disease.
•
The predilection of people with AIDS to develop
P. carinii
pneumonia means that widespread,
uniformly distributed pulmonary opacification in a patient with AIDS is usually due to this
organism.
•
Sarcoidosis : The radiological manifestations are largely confined to the chest. The features on
CXR and CT are:
1- Hilar and paratracheal lymphadenopathy : When hilar lymphadenopathy is present it is
almost invariably bilateral and is usually symmetrical .
Mediastinal adenopathy is common and the nodes are large enough to be visible on a CXR in
about half the patients. Mediastinal lymphadenopathy is most readily recognized in the right
paratracheal region.
•
On chest CT , the widespread distribution of the mediastinal lymphadenopathy is readily
apparent. Unlike lymphoma, the lymph node enlargement is never predominant in the
anterior mediastinum.
2-Reticulonodular opacities in the lungs. The pattern varies from uniform small nodular
opacities, which may clear on steroid therapy, to coarse reticular opacities maximal in the mid
and upper zones, which represent pulmonary fibrosis , at this stage the pulmonary disease is
often irreversible.
•
The majority of patients with sarcoidosis of the chest have lymphadenopathy only, which
clears without treatment and does not progress to pulmonary involvement.
•
Many are discovered on a routine CXR and have no symptoms.
•
Approximately 10% of patients with sarcoidosis develop a significant degree of lung
involvement; some have visibly enlarged lymph nodes at this stage. Often the lymph nodes get
smaller and may return to normal, even though the lung fibrosis persists.
•
Diffuse interstitial pulmonary fibrosis : The known causes of diffuse interstitial pulmonary
fibrosis include: extrinsic allergic alveolitis, collagen vascular diseases (notably rheumatoid
arthritis), drug-induced fibrosis, pneumoconiosis and sarcoidosis. However, a substantial
proportion of cases are idiopathic in origin.
•
Several names are given to the most common idiopathic form of diffuse interstitial fibrosis,
notably usual interstitial pneumonia (UIP), idiopathic pulmonary fibrosis (IPF) and idiopathic or
cryptogenic fibrosing alveolitis (CFA).
•
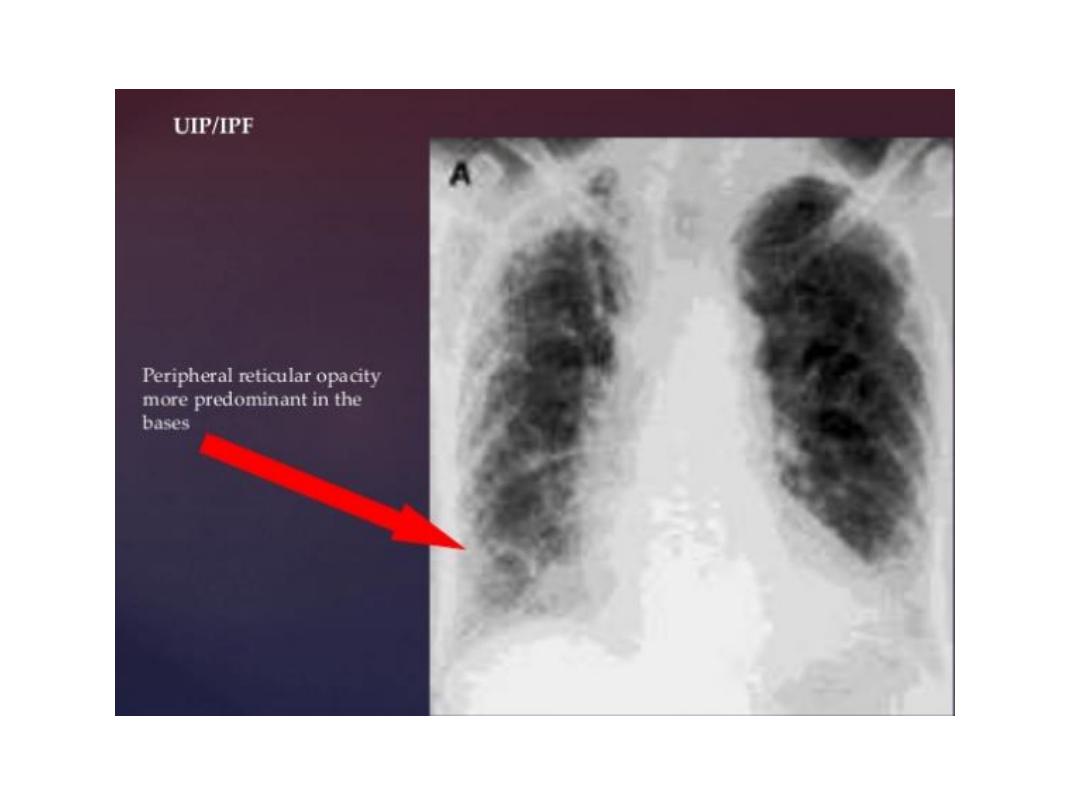
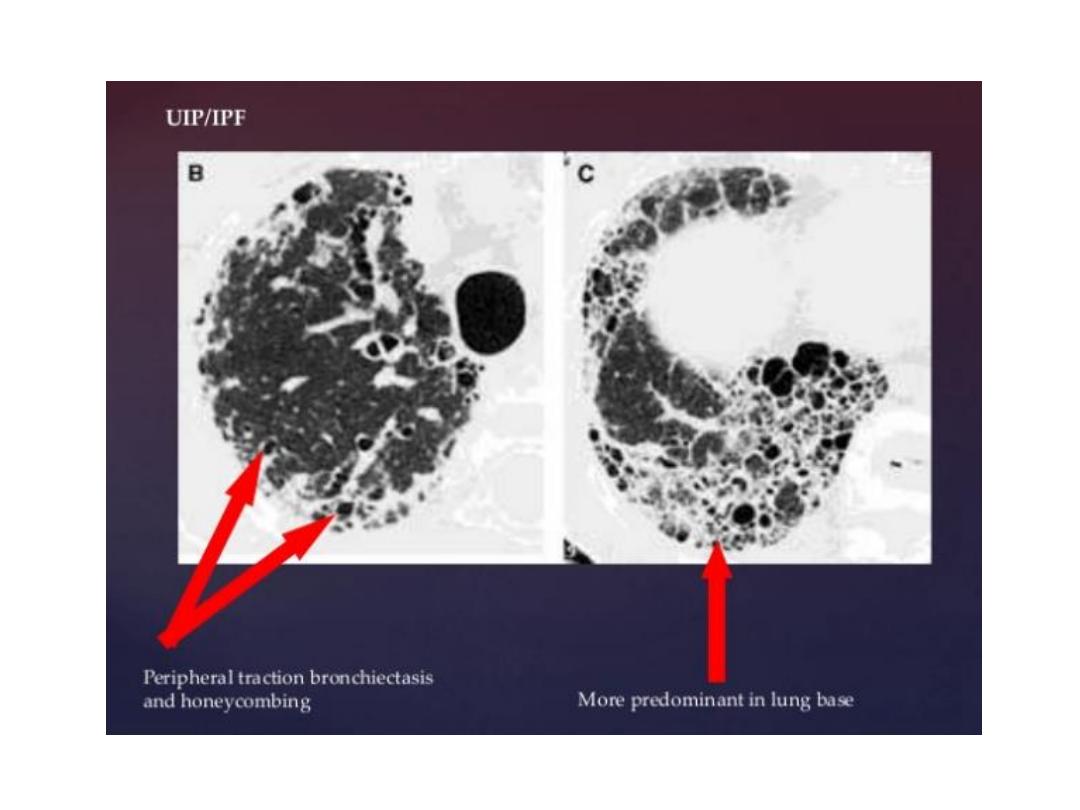
Usual interstitial pneumonia (cryptogenic fibrosing alveolitis, idiopathic pulmonary fibrosis)
: In UIP there is thickening of the alveolar walls with fibrosis and desquamation. As the disease
progresses, the alveolar walls break down and small, rounded air-spaces develop. At this stage,
the appearances are known by the descriptive term ‘honeycomb lung’. It causes a restrictive
ventilation defect with severe reduction in gas transfer across the alveolar walls. The imaging
features are:
1- Hazy shadowing at the lung bases leading to a lack of clarity of the vessel outlines. Later, ill-
defined nodules with connecting lines become discernible, which may contain circular
lucencies (honeycomb lung)
2- Decreased lung volume, often marked .
3- Eventually, the heart and pulmonary arteries enlarge due to increasingly severe pulmonary
hypertension.
•
These signs are seen on both CXRs and HRCT. HRCT is more sensitive for detecting the changes,
particularly areas of ground glass shadowing and honeycombing, and demonstrates the
distribution and severity of disease.
• Determining the cause of diffuse pulmonary fibrosis : The distribution of pulmonary
opacities may give a clue to its aetiology.
• In UIP, the lung opacification is often maximal at the bases and at the lung periphery,
although it may be fairly uniformly distributed in advanced cases. Scleroderma and
rheumatoid arthritis give an identical picture.
• The combination of pulmonary fibrosis with certain other signs may lead to a specific
diagnosis:
• Substantial past or present hilar/mediastinal adenopathy suggests sarcoidosis .
• Coexistent conglomerate masses in the mid and upper zones are virtually diagnostic
of silicosis or coal miners’ pneumoconiosis.
• Coexistent bilateral pleural thickening and calcification are highly suggestive of
asbestosis.
• Past or present pleural effusions are highly suggestive of rheumatoid arthritis.
• Radiation pneumonitis : Radiation pneumonitis may occur following radiotherapy
for intrathoracic neoplasms and breast carcinoma .
• The response of the lung to radiation varies from patient to patient.
• 1- Initially, there is no radiological change, 2- but within a few weeks ill-defined,
small opacities, indistinguishable from infective consolidation, are seen within the
radiation field. 3- If the inflammatory change goes on to fibrosis, there is dense,
coarse opacification that may be sharply demarcated from the normal lung in a
geometric fashion, conforming to the field of radiation but ignoring the lobar
boundaries of the lung. 4- There is loss of volume in the fibrosed areas. 5- Extensive
pleural thickening is also sometimes seen.
• Collagen vascular diseases : This group of diseases includes rheumatoid arthritis,
systemic lupus erythematosus, polyarteritis nodosa, systemic sclerosis,
dermatomyositis and Wegener’s granulomatosis.
• Various radiological signs occur.
• Rheumatoid lung: 1-The most common finding in the chest is pleural effusion.
2- Pulmonary fibrosis, indistinguishable from that seen in idiopathic pulmonary
fibrosis, is another important feature.
• An interesting sign of pulmonary involvement in rheumatoid arthritis is the
development of rounded granulomas in the periphery of the lung, histologically
similar to the subcutaneous nodules seen in this disease. These spherical nodules,
which may be single or multiple, rarely exceed 3 cm in size. Eventually, many
cavitate and then go on to resolve.
• Systemic lupus erythematosus: 1-The CXR is usually normal. 2-The commonest
abnormalities are pleural effusion and cardiac enlargement due to pericardial
• effusion. 3- Patchy consolidation in the lungs is occasionally seen.
• Scleroderma and dermatomyositis : 1- The cardinal feature is basal
reticulonodular opacities from pulmonary fibrosis, similar to that seen in idiopathic
pulmonary fibrosis. 2- Pleural effusion is rare. 3-Widening of the oesophagus is a
feature of scleroderma that may be visible on the CXR.
• Wegener’s granulomatosis : the lungs may show one or more well-defined
consolidations or masses, usually in the mid zones, which may cavitate, These
lesions are often difficult to distinguish from bronchogenic carcinoma, when single,
or metastases, when multiple, on radiographic grounds alone.
• Pneumoconiosis :The pneumoconioses consist of a group of conditions caused by
the inhalation of a variety of dusts related to people’s work.
• Coal workers’ pneumoconiosis : Coal workers’ pneumoconiosis is now very
uncommon, following the introduction of preventative measures.
• Simple pneumoconiosis is due to dust retention in the lungs with minor fibrosis. It
does not give rise to symptoms, but radiologically it causes many small nodules
similar in appearance to miliary tuberculosis. For reasons that are not entirely clear,
progressive massive fibrosis may supervene.
• Progressive massive fibrosis causes homogeneous, rounded opacities in the upper
halves of the lungs. The opacities may be unilateral or bilateral and there is usually
nodular opacification in the rest of the lungs.
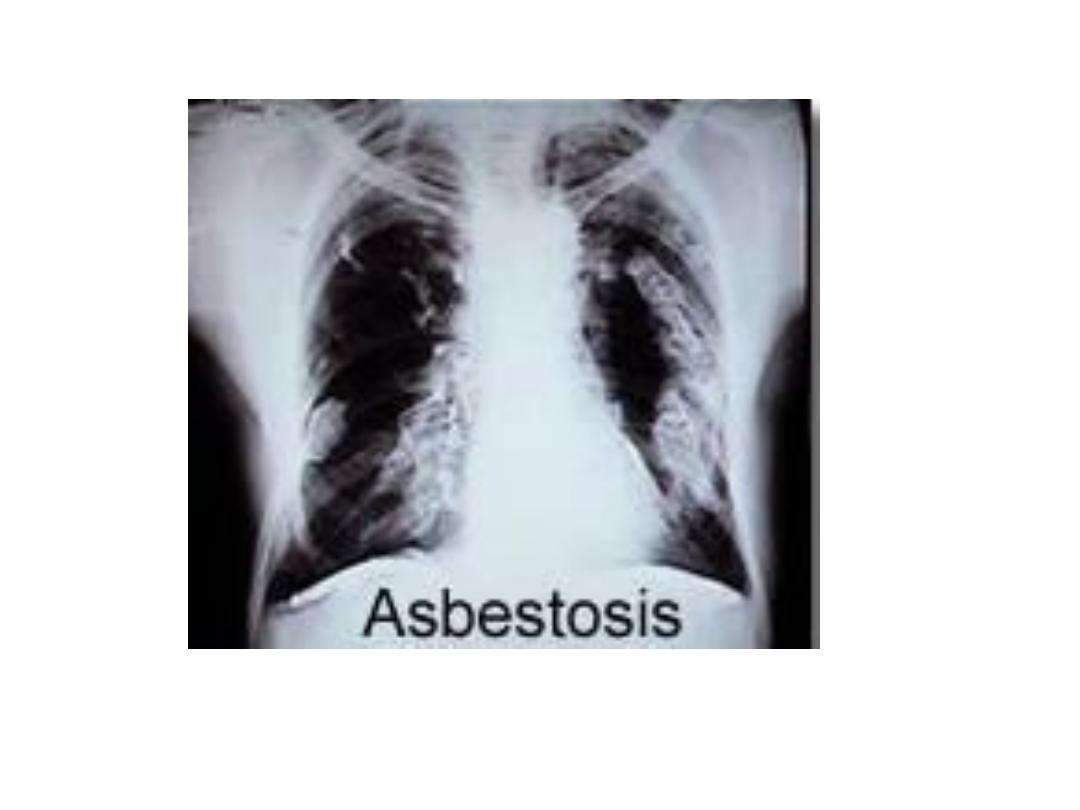
• Asbestos-related disease: Inhalation of asbestos fibers may lead to:
•
Pleural plaques. Localized plaques of pleural thickening,
some of which are
calcified, are seen along the lateral chest wall and diaphragm. The plaques in
themselves are harmless, but they are a useful pointer to previous asbestos
Exposure.
•
Diffuse pleural thickening, which may encase one or
both lungs, and cause
restrictive reduction in pulmonary function.
•
Pulmonary fibrosis. Unlike the pleural plaques, which
may be seen following minor
exposure to asbestos, pulmonary fibrosis (asbestosis) only follows significant
exposure. Pulmonary fibrosis in asbestosis is symmetrically bilateral and maximal at
the bases, similar to UIP.
•
Development of malignant neoplasms. Malignant mesothelioma
and bronchial
carcinoma are both seen with far higher frequency in asbestos-exposed patients
than in the general population.
Lobar pneumonia

Bronchopneumonia
Lung abscess
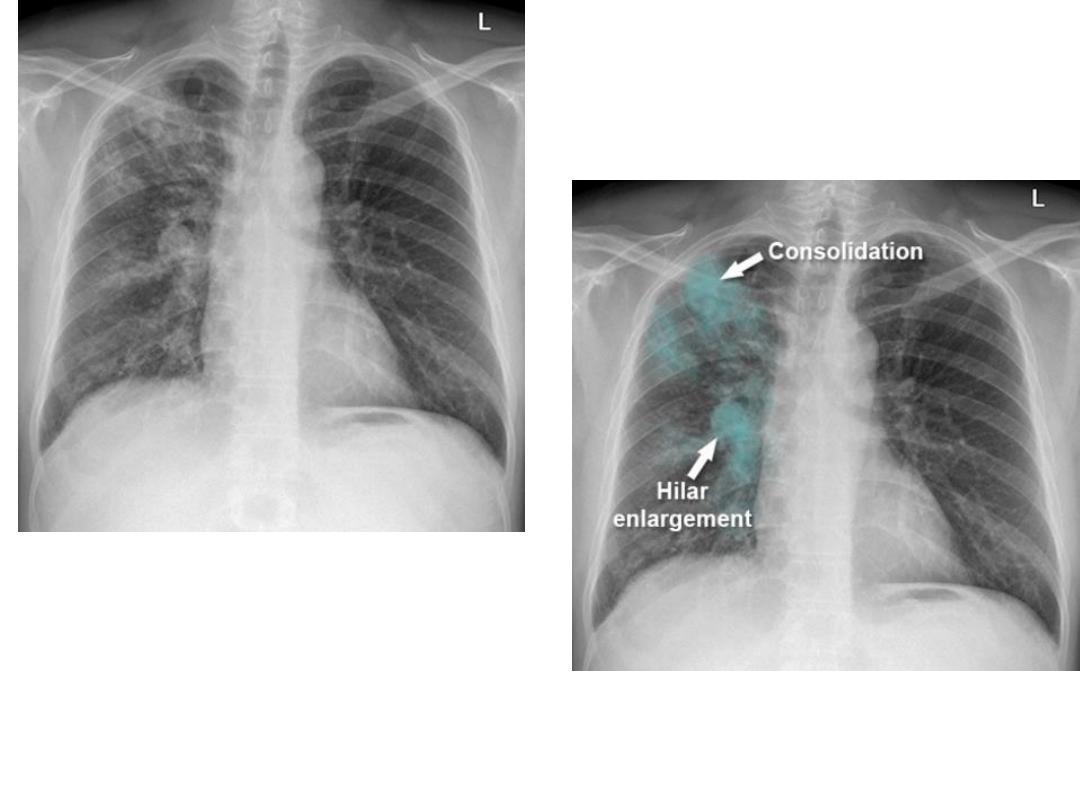
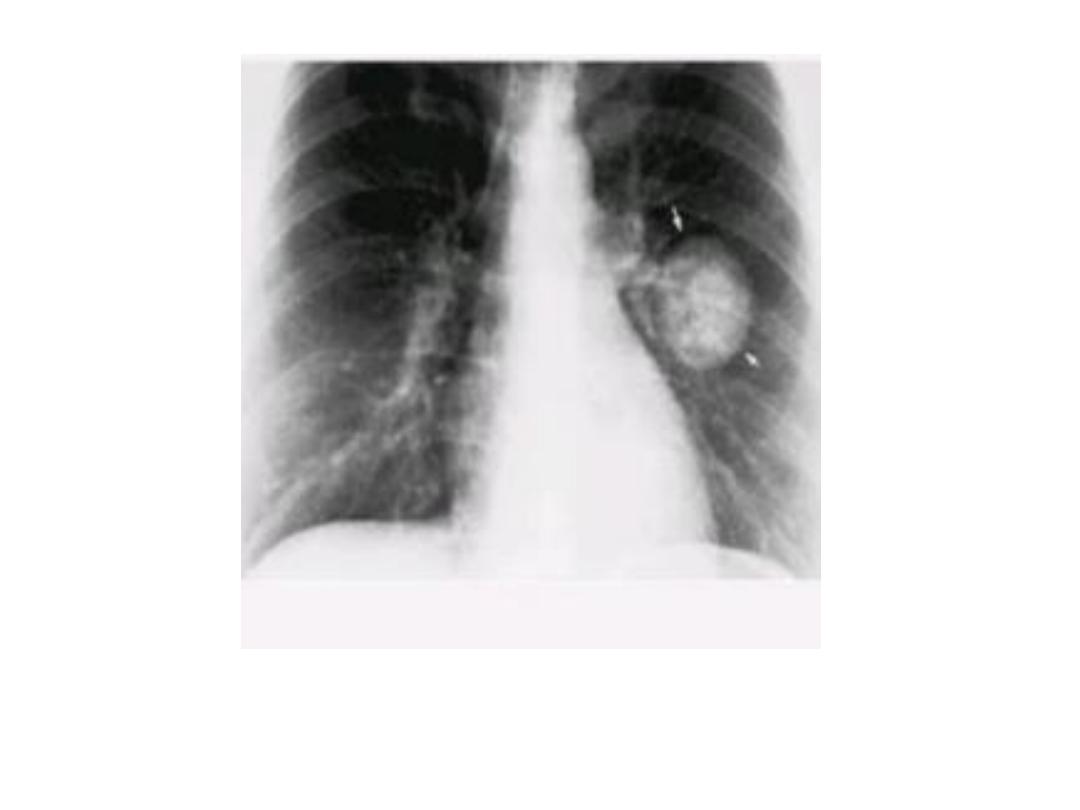
Primary TB
Unilateral Hilar and med. In primary TB
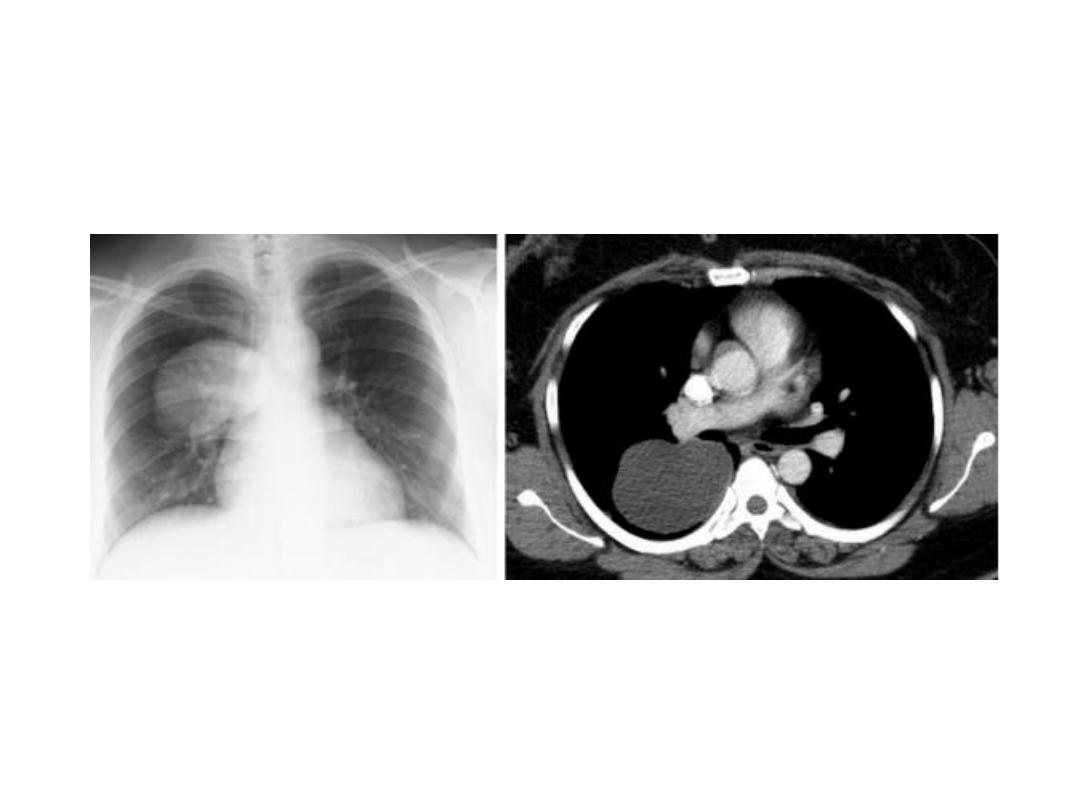
Pleural effusion in primary TB
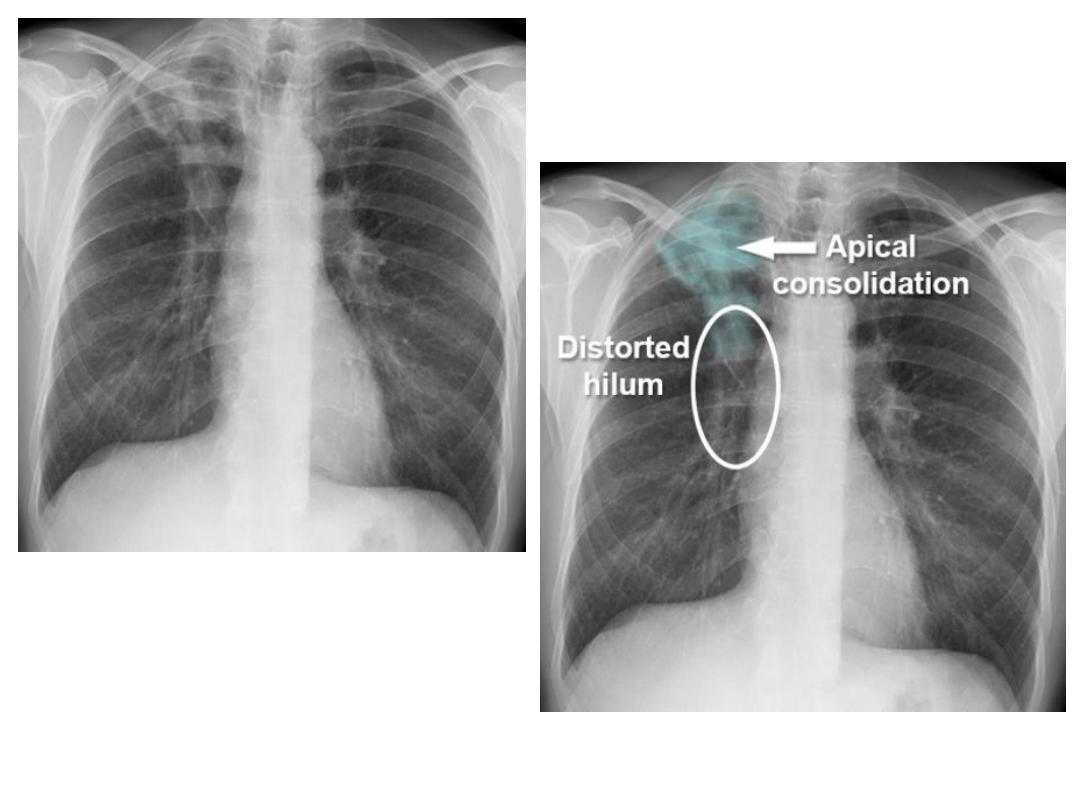
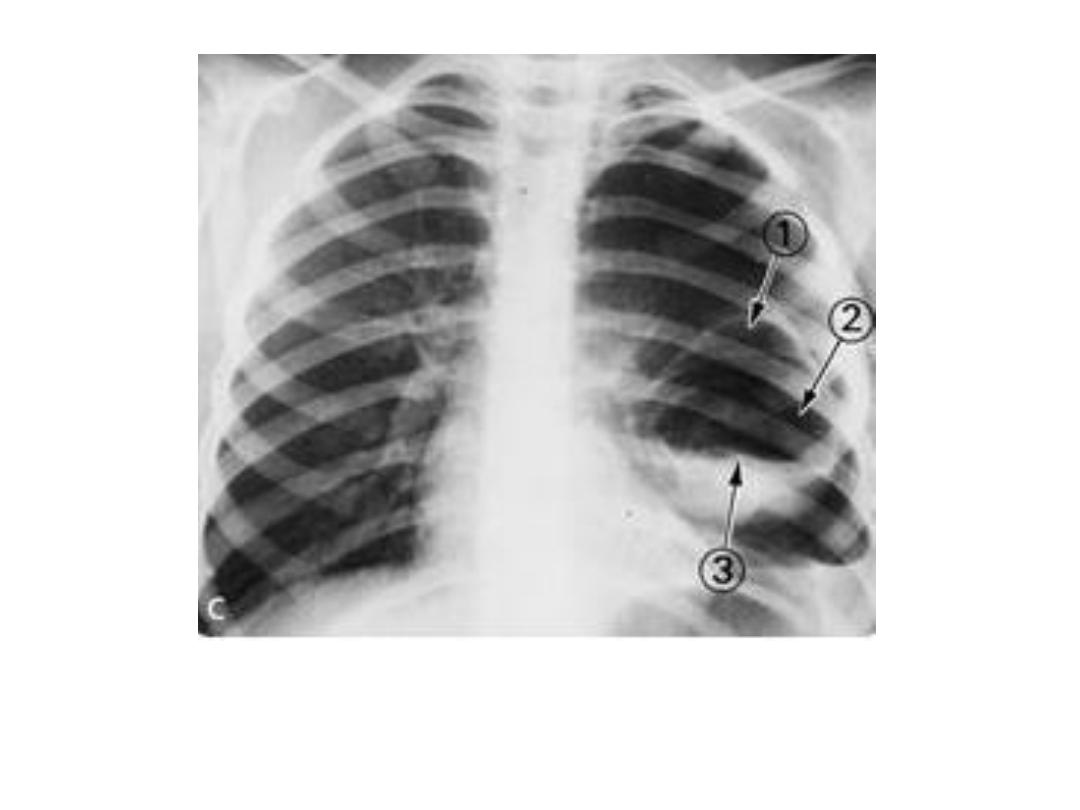
Post primary TB
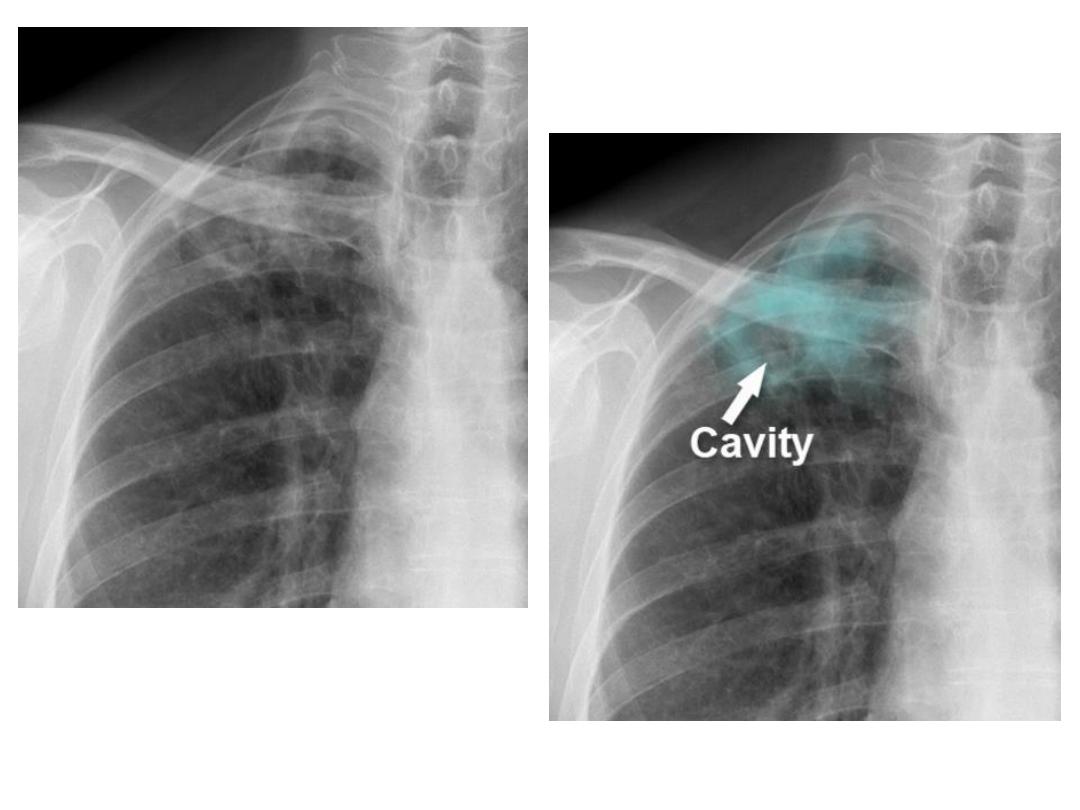
Same prev. patient 4 m
later develop cavity
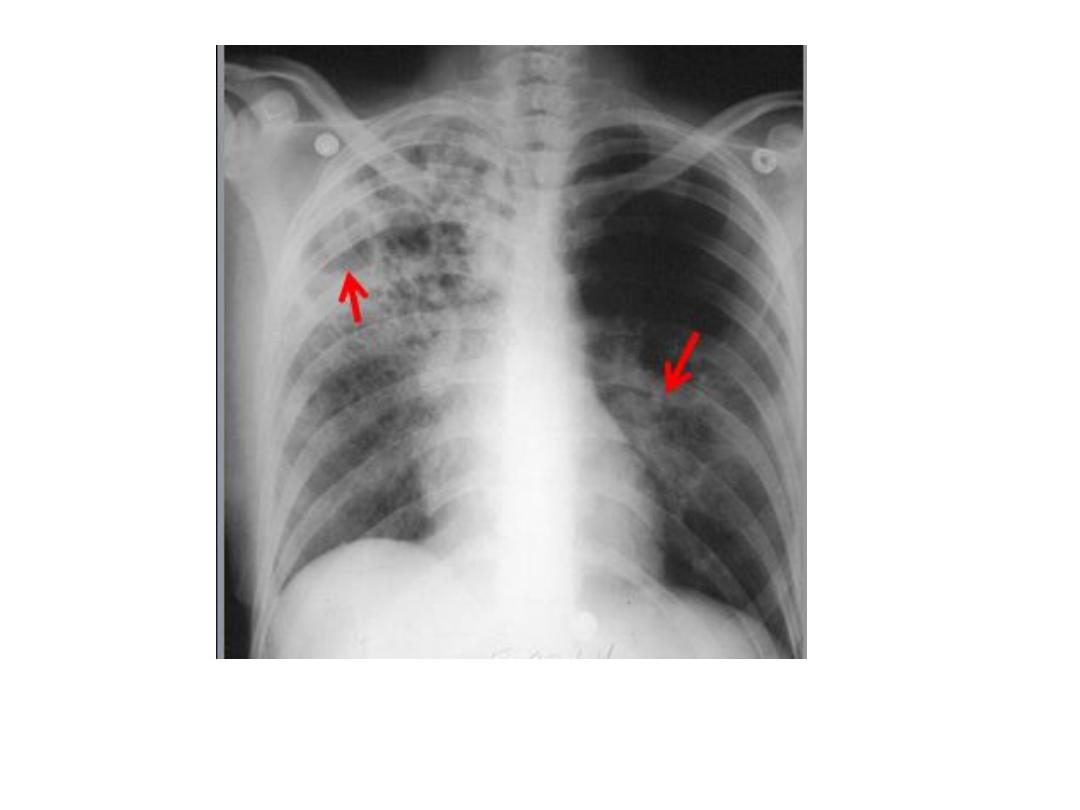
RUL TB cavitary lesion with transbronchial spread to
left LL

mycetoma
Tuberculoma
Intact HC

Multiple HCs
Lung HC, double arc or cumbo sign when air
track between peri and endocyst forming arch
above air fluid level
HC crescent sign: air enter between
ecto and pericyst
HC whirl sign: floating detached
membrane in the cavity + pl
effusion

HC water lily sign : irregular
air fluid level
HC Empty cyst sign : complete evacuation
of HC membrane
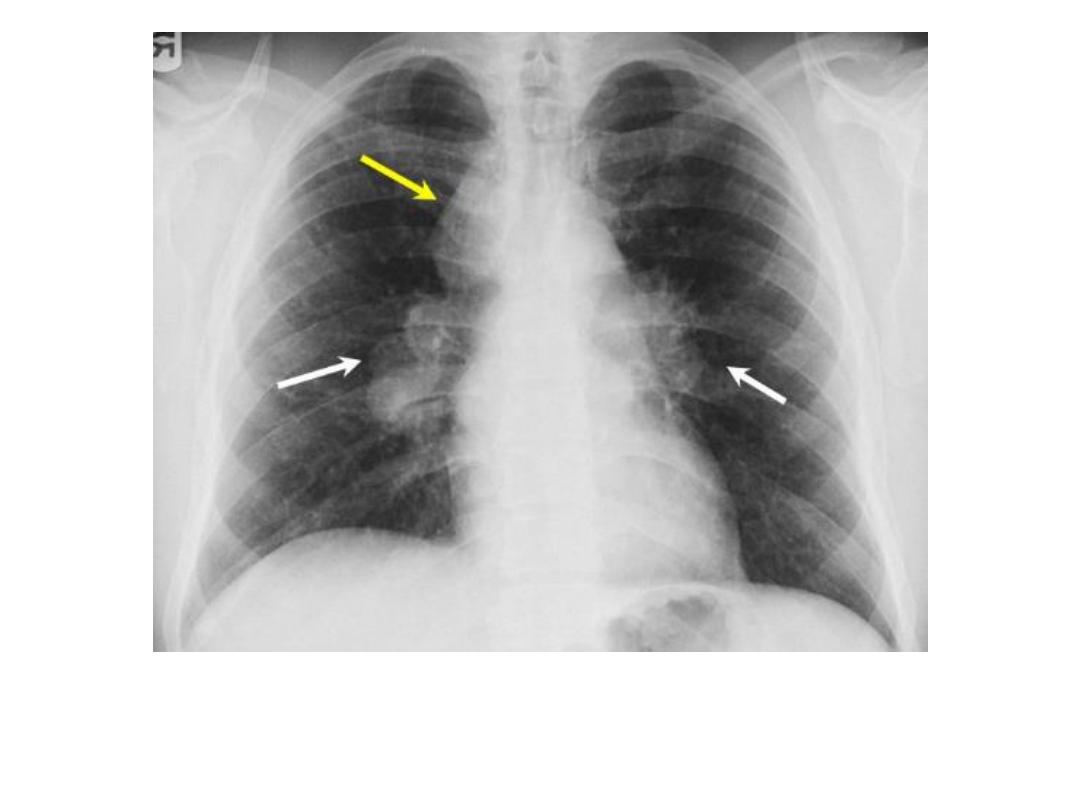
Sarcoidosis : hilar and rt.
Para tracheal LNs

Pulmonary infiltrate in
sarcoidosis

Radiation pneumonitis

Rheumatoid arthritis Caplan
syndrome lung nodules

Malignant mesothelioma

THANK YOU