ﺑ
ﺳ
م
ﷲ
ا
ﻟ
ر
ﺣ
ﻣ
ن
ا
ﻟ
ر
ﺣ
ﯾ
م
CRANIAL NERVES
DISORDERS
Cranial Nerves
I- OLFACTORY
II- OPTIC
III- OCULOMOTOR
IV- TROCHLEAR
V- TRIGEMINAL
VI- ABDUCENS
VII- FACIAL
VIII- VESTIBULOCOCHLEAR
IX- GLOSSOPHARYNGEAL
X- VAGUS
XI- ACCESSORY
XII- HYPOGLOSSAL
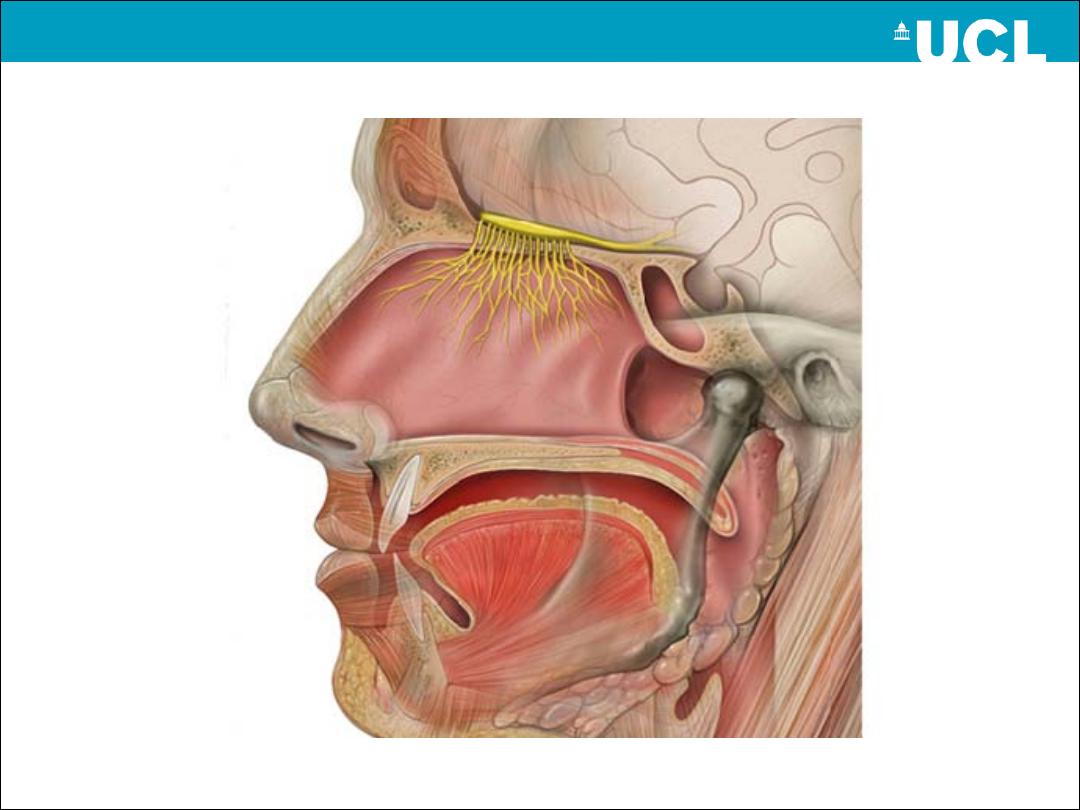
OLFACTORY nerve
-fibers enter the cranium through the cribriform plate to form the olfactory
tract.
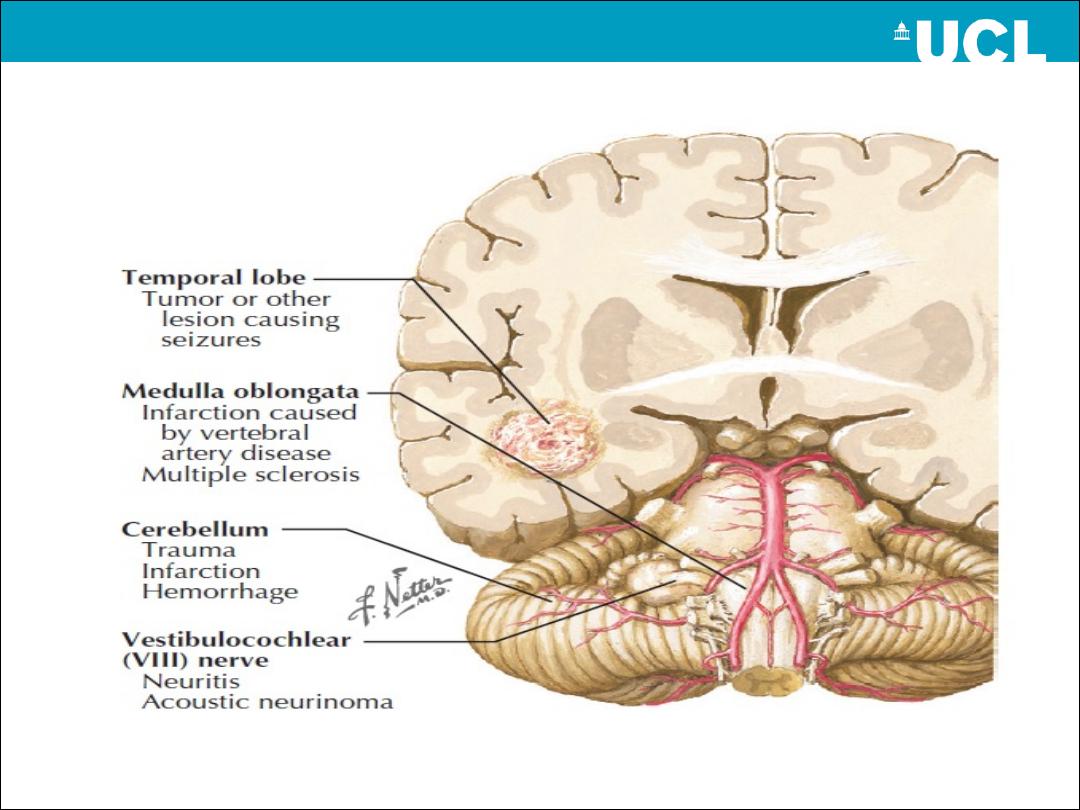
Cortical olfactory area is in the temporal lobe.
causes of anosmia:
A-nasal obstruction by infective or allergic oedema of the nasal mucosa.
B-degenerative including aging, Parkinson's and Huntington's diseases.
C-head injury
D- anterior fossa tumor
Optic
Discussed in the introduction
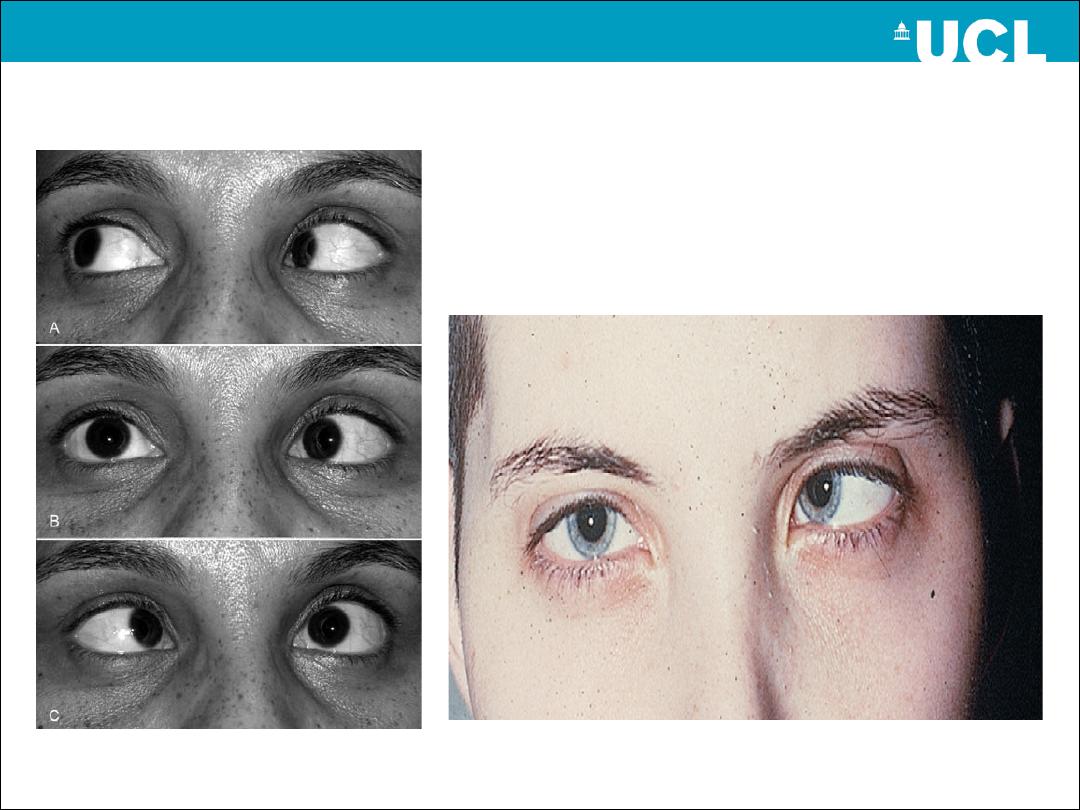
The oculomotor (III)
-The nerve innervates the superior, medial and inferior recti, the
inferior oblique and levator palpebrae superioris muscles.
-parasympathetic fibres arising from the Edinger-Westphal
nucleus, the nerve indirectly supplies the sphincter muscles of
the iris, causing constriction of the pupil.
-it passes in relation to the
posterior communicating artery
and
enters the dura surrounding the
cavernous sinus
.
-
III palsy= squint + complete ptosis + dilated pupil
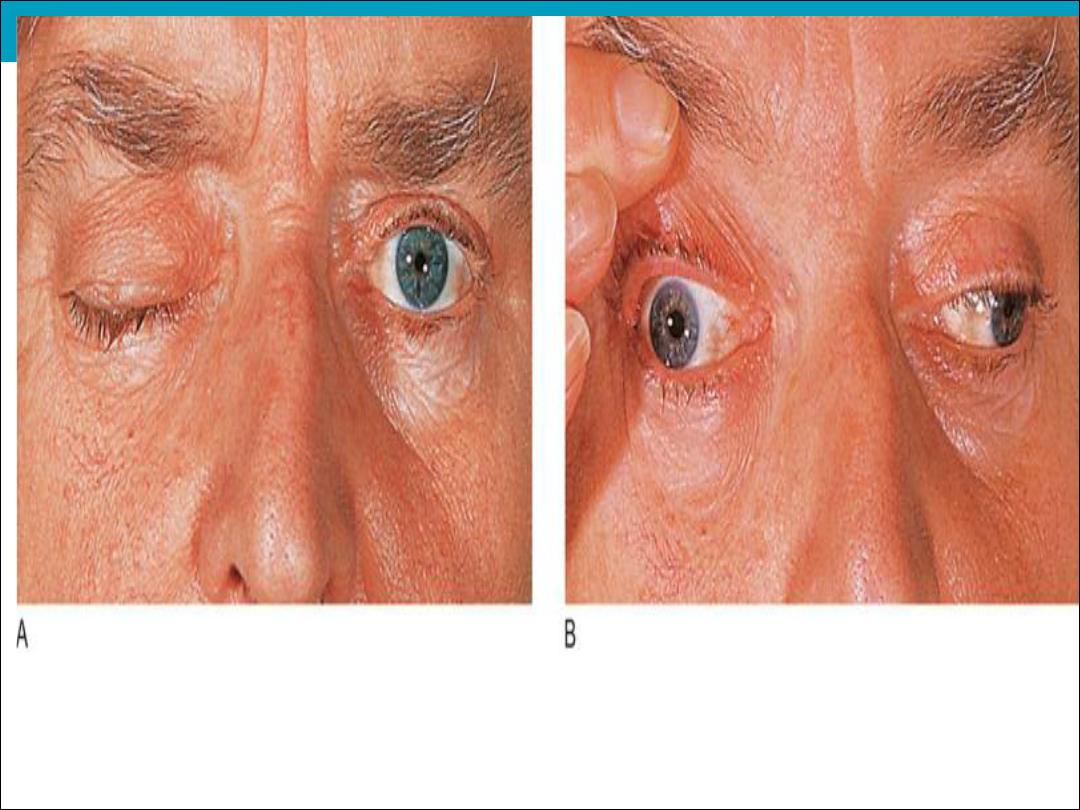
nerve palsy
rd
Medical 3
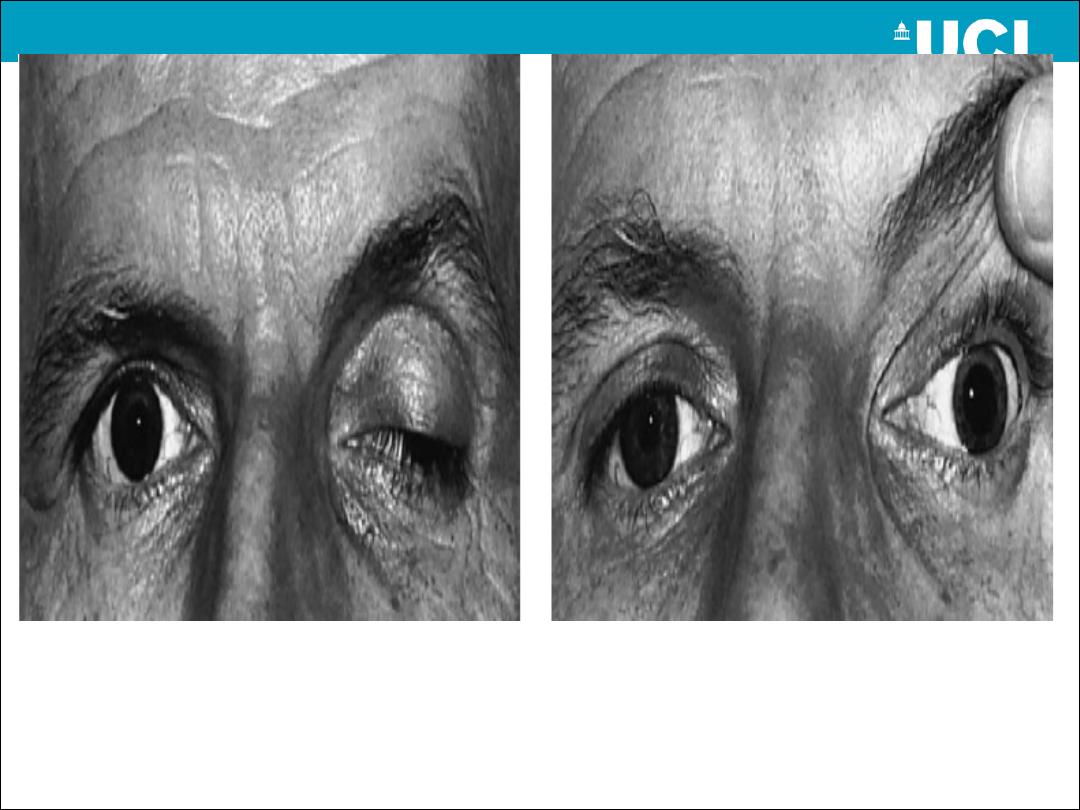
nerve
rd
Surgical 3
palsy
Trochlear (IV)
-innervate sup. Oblique muscle. Causes are
(1) Trauma
(2) Idiopathic
(3) Ischemic
(4) Congenital
(5) Tumor
-Vertical diplopia is most clear in down gaze.
ABDUCENS (VI)
Innervates the lateral rectus muscle.
-causes are
(1) Idiopathic
(2) Tumor
(3) Trauma
(4) Ischemia
(5) Raised ICP as a false localizing sign
- VI palsy produces horizontal diplopia maximal to
the direction of weakness.
CN VI palsy
Trigeminal nerve palsy
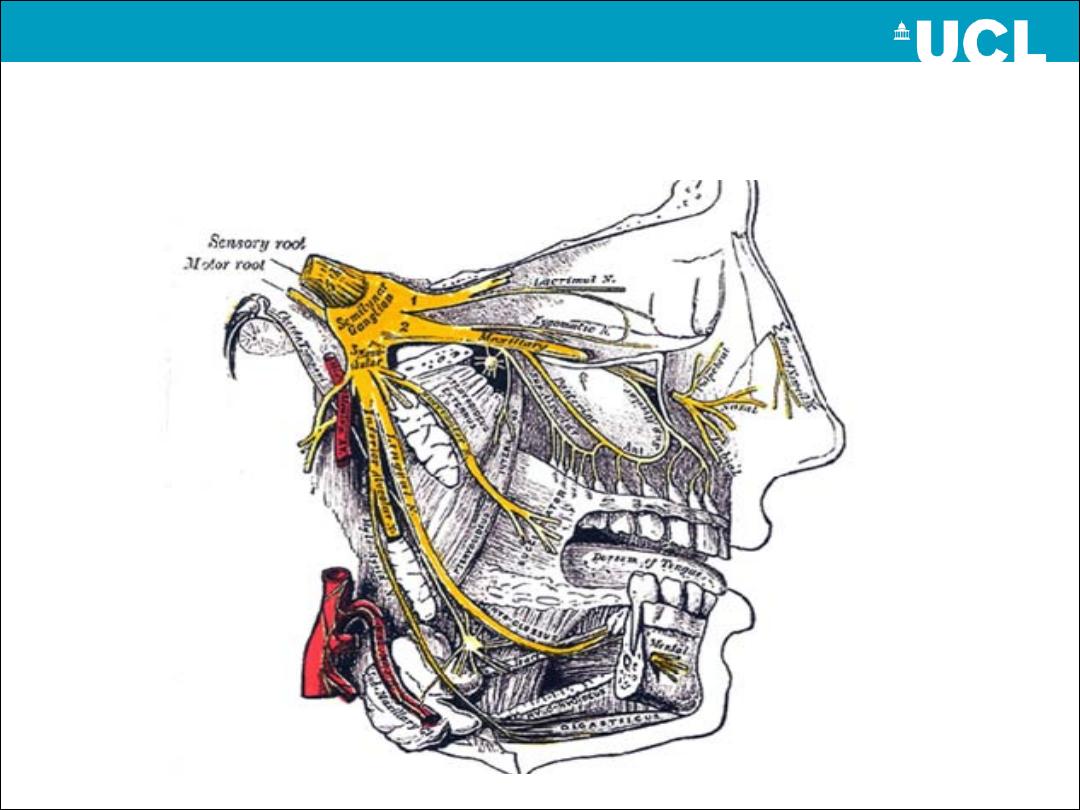
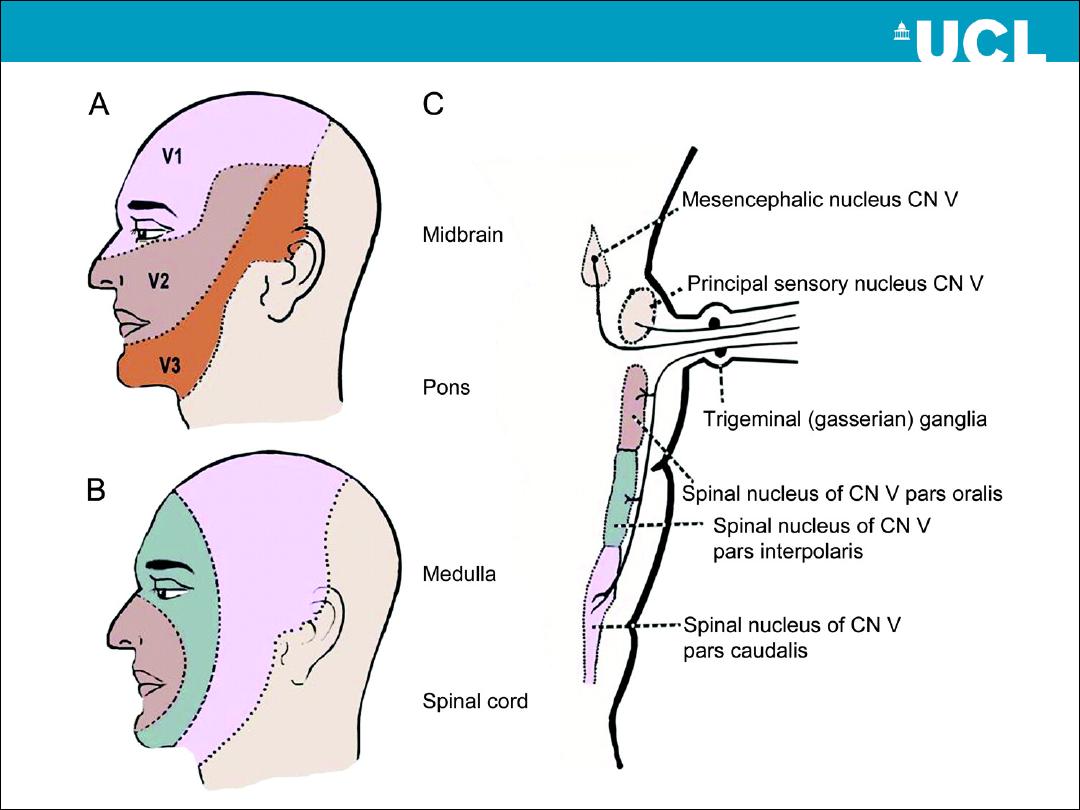
CN V disorders
Lesions lead to loss of sensation in the face and
weakness in muscles of mastication
causes:
1-tumors(acoustic neuroma)
2-Sjogren”s disease
3-trauma
4-idiopathic
5-herpes zoster (usually ophthalmic division)
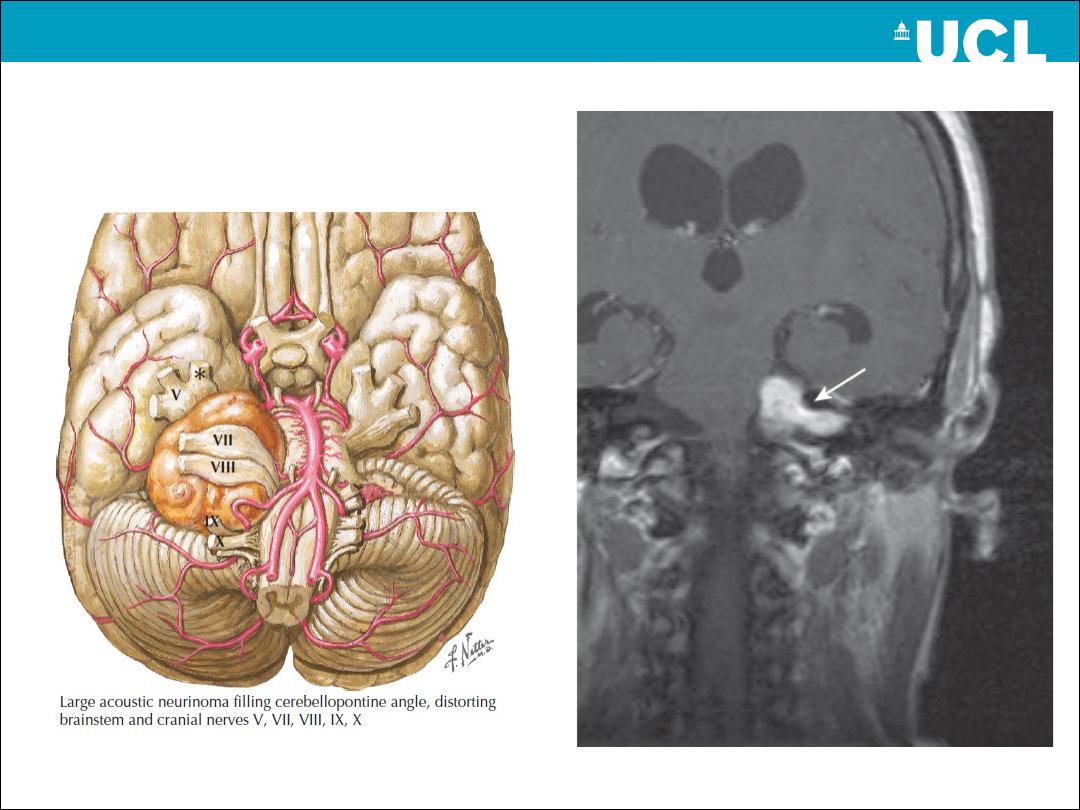
Acoustic Neur(in)oma
Left V palsy

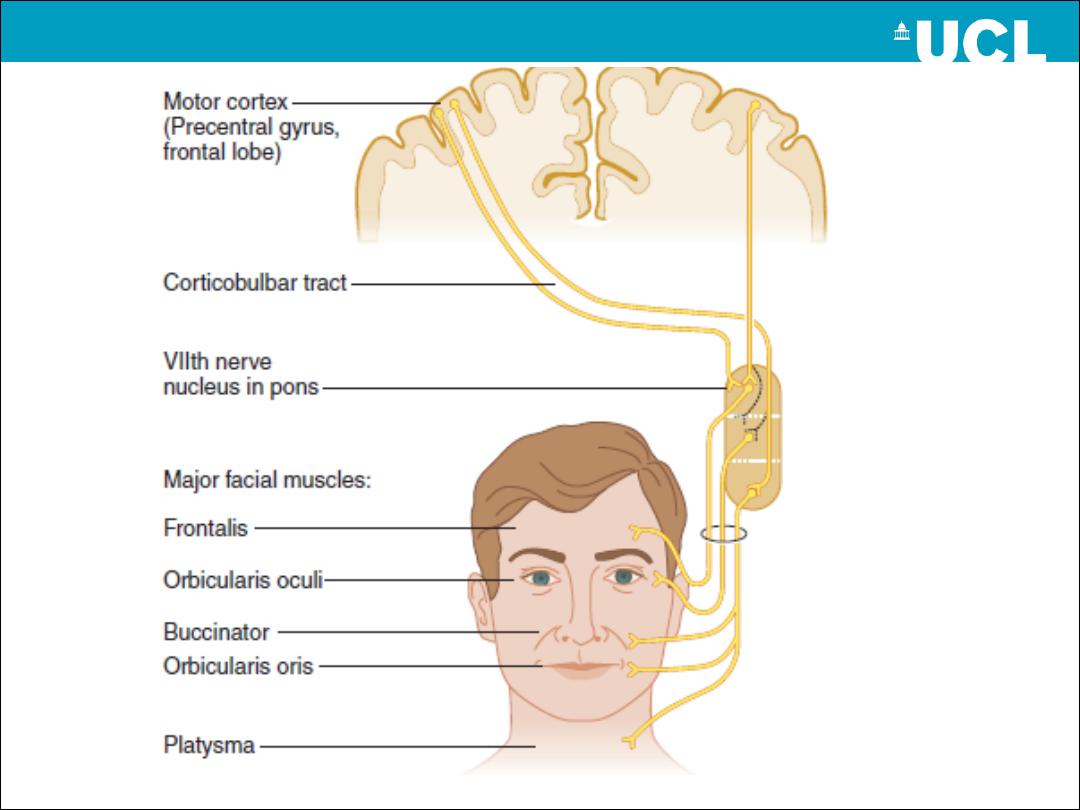
Facial (VII) nerve
Mediates
Sensory function: somatic sensation from external auditory meatus; taste
(anterior 2/3 of tongue, )
Motor function to muscles of facial expression
parasympathetic function( GVE) to the lacrimal, submandibular and
sublingual salivary glands (via nervus intermedius).
-
it is emerging from the lateral pontomedullary junction in close
association
with the VIII nerve
; together they enter the internal
acoustic meatus.
-exiting the skull via the
stylomastoid foramen
.
-Passing through
the parotid gland
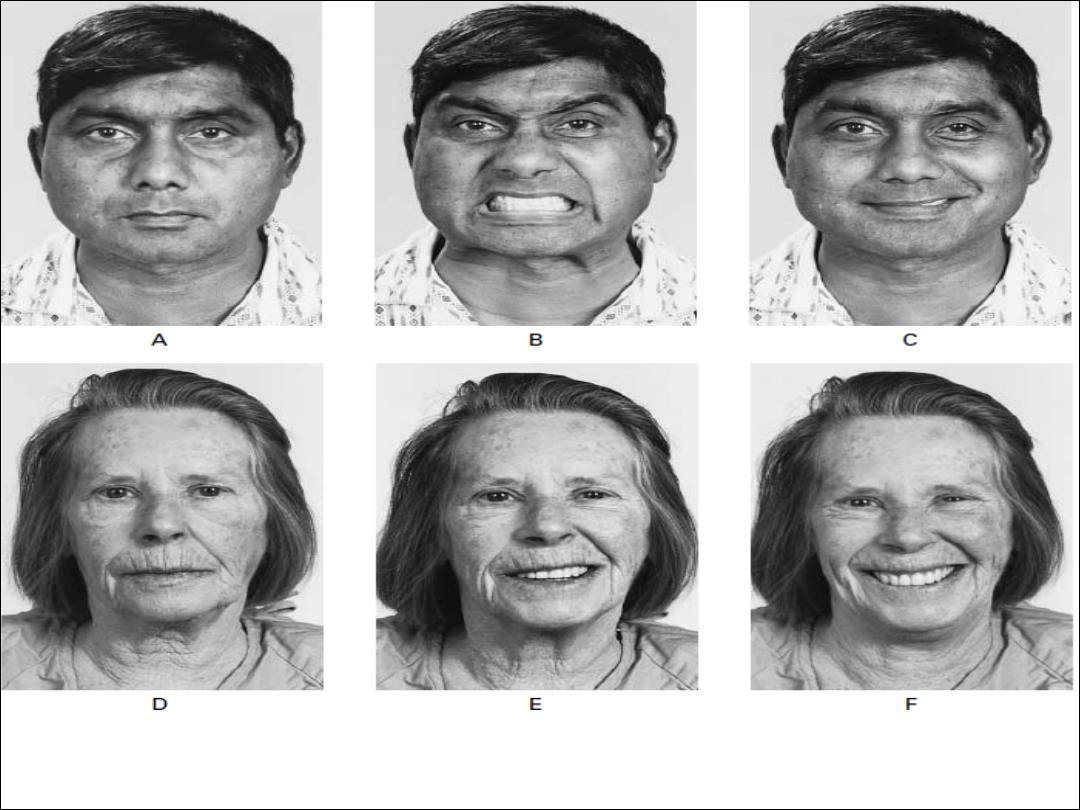
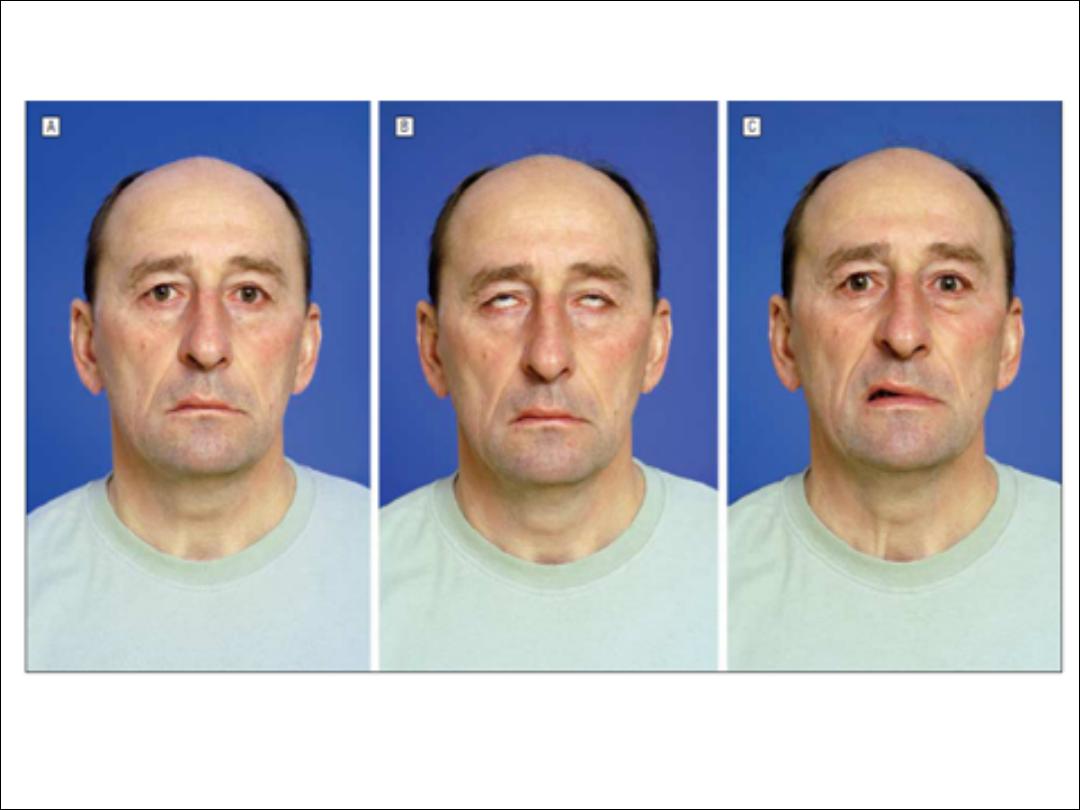
CN VII disorders
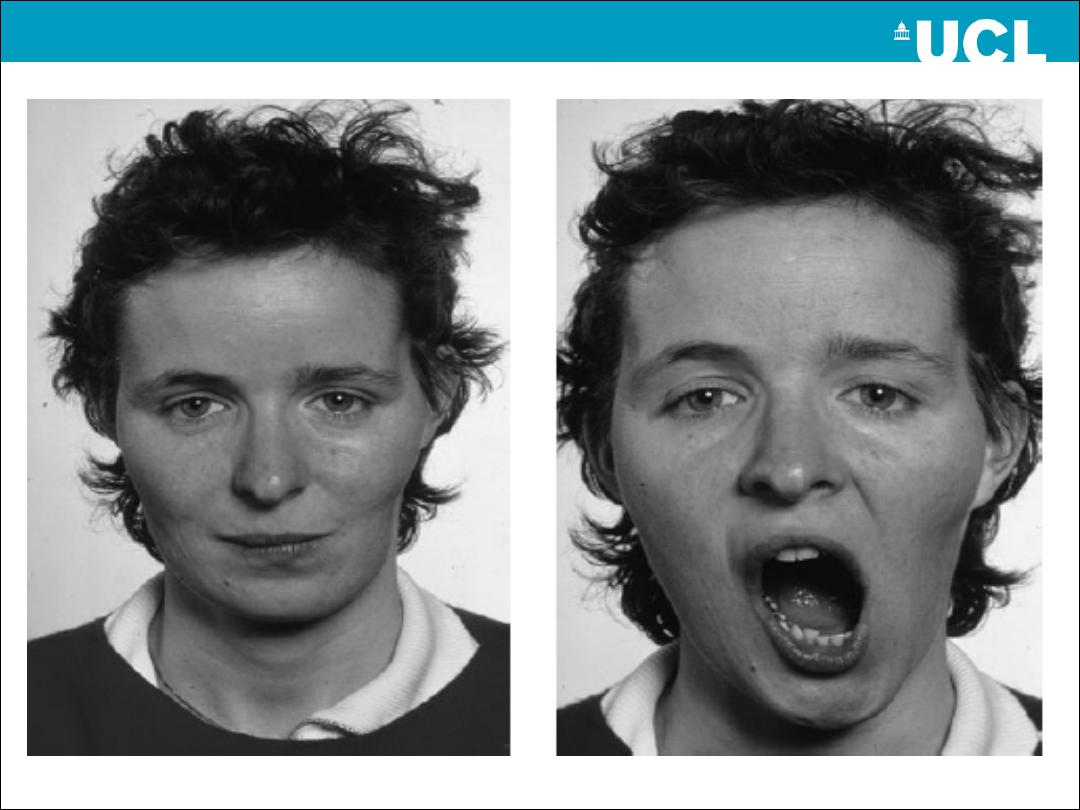
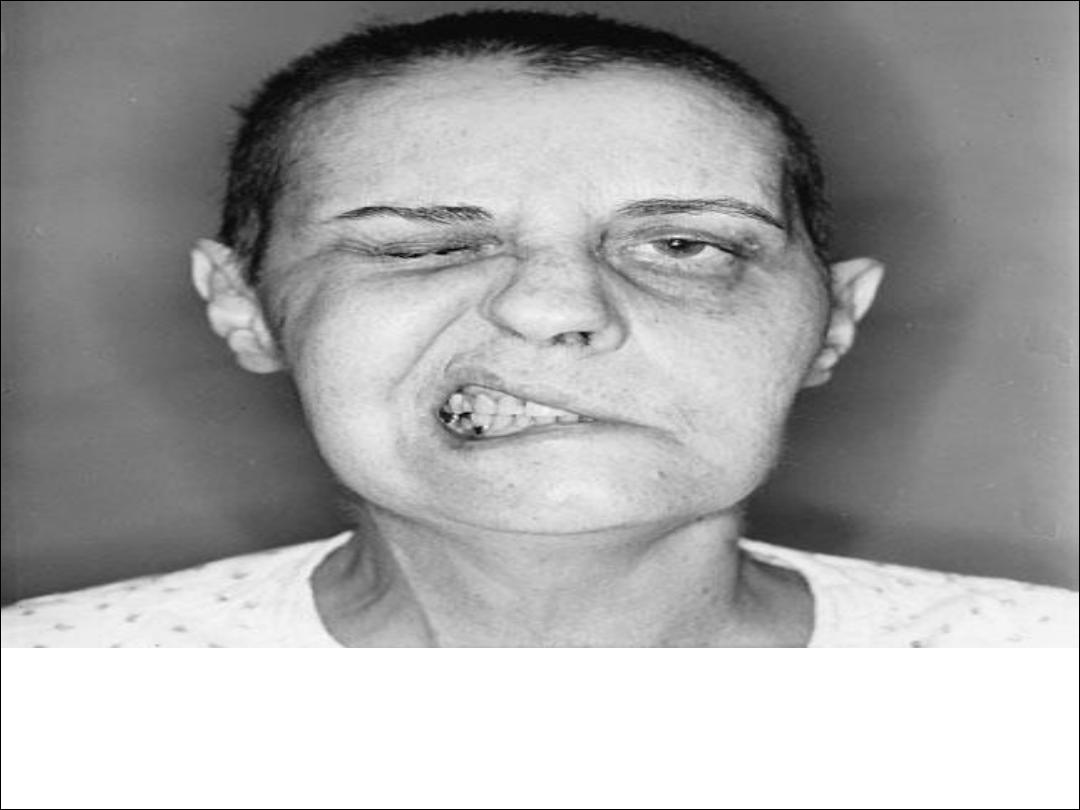
-In a unilateral lower motor neurone VII nerve lesion, there is weakness
of both upper and lower facial muscles.
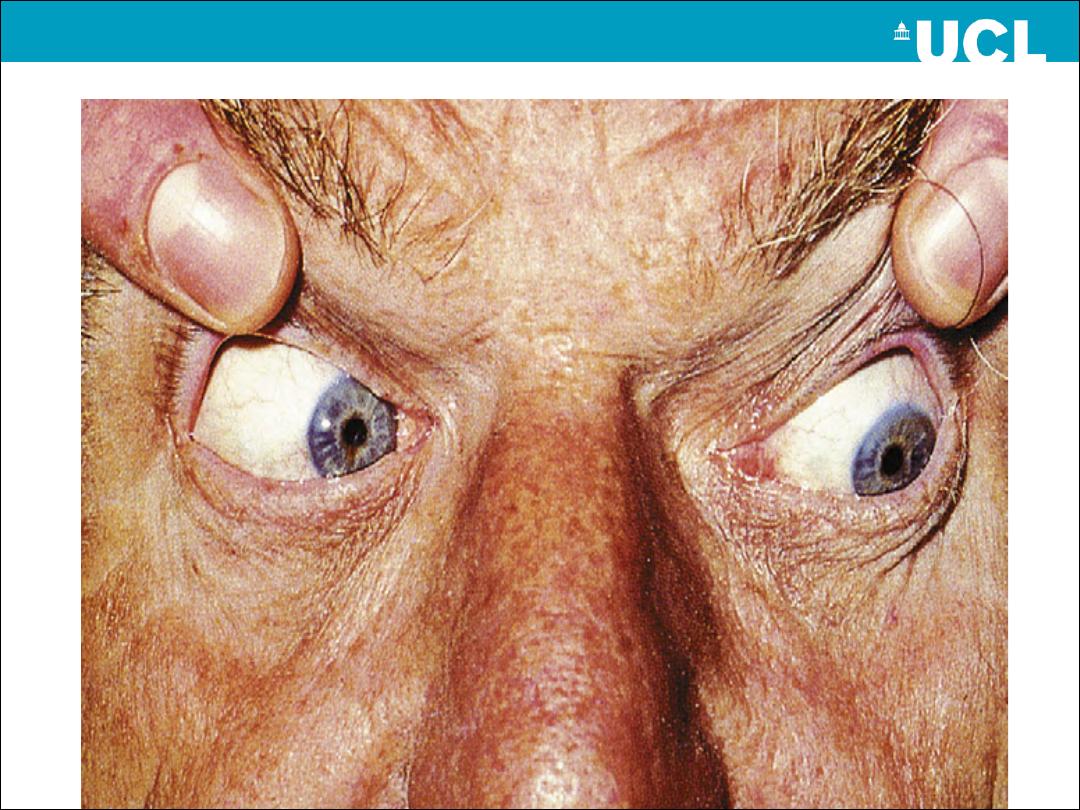
-Bell's phenomenon occurs when the patient is unable to close the eye.
As he or she tries, the eyeball rolls upwards, exposing the conjunctiva
below the cornea.
-In unilateral VII nerve upper motor neurone lesions, weakness (facial
paresis) is marked in the lower facial muscles with relative sparing of
the upper face. This is because there is bilateral cortical innervation of
the upper facial muscles. While the nasolabial fold may be flattened
and the corner of the mouth drooping, eye closure is usually well
preserved.
Bell’s palsy
•
The commonest cause of LMN palsy.
• The cause of this condition is not certain, although there is some evidence to
suggest inflammation due to reactivation of herpes simplex virus within the
nerve ganglion in many cases.
• The lesion is usually proximal enough to have effects on taste and hearing.
• After some aching around the ear, the facial weakness develops quite
quickly within 24 hours.
• The cornea may be vulnerable to infection because of impaired eye closure.
• Mx: steroid+ antiviral + eye protection
LMN V Palsy
em
Emotional and voluntary UMN facial
weakness
Bilateral V palsy + Bell”s
phenomenon
Causes of CN VII palsy
LMN palsy
1-Bell’s palsy
2-diabetes
3- herpes zoster (Ramsay –
Hunt syndrome)
4- cerebello-pontine angle
tumors (acoustic neuroma)
5-parotid tumor or injury.
UMN palsy
1-stroke
2-multiple sclerosis
3-cerebral tumor
4-trauma
5-encephalitis
Vestibulocochlear nerve
consists of two functional divisions:
• Auditory nerve (cochlear)
• Vestibular nerve
Pure
special visceral afferent nerve
Exits the brainstem at cerebellopontine (CP) angle
Disorders of VCN-A
Destructive ( negative symptoms): sensori-neural
hearing loss secondary to:
•Vascular
• inflammatory
•neoplastic aetiologies
•Meniere disease
Irritative (positive symptoms): tinnitus
Disorders of vestibular nerve
Lesions result in : vertigo, nystagmus and ataxia
Causes:
1-Vestibular neuropathy (diabetes, meningitis,
hypothyroidism)
2-Acute peripheral vestibulopathy
(vestibular neuritis)
3-Benign positional vertigo
4-Toxic vestibulopathy (drugs, alcohol)
5-Meniere disease (severity decrease with time, SNHL)
6-Otosclerosis
Glossopharyngeal nerve
Mediates:
Sensory function
(somatic: part of external auditory
, taste: from posterior 1/3 of tongue), taste sensation
from posterior 1/3 of tongue
Motor function
(: stylopharyngeus muscle)
Visceral efferent (parasympathetic)
( GVE: Otic
ganglia to parotid gland)
Nuclei: medulla
Exit foramen: jugular foramen
Vagus nerve
Mediates:
Sensory function
(GSA: infratentorial dura, posterior surface
of EAM, tympanic membrane; SVA: taste from epiglottis)
Motor function
(SVE: , palate, muscles of swallowing,
laryngeal muscles)
Visceral efferent (parasympathetic)
to viscera of the neck,
thocoabdominal viscera down to left colic flexure.
Nuclei: medulla
Exit foramen: jugular foramen
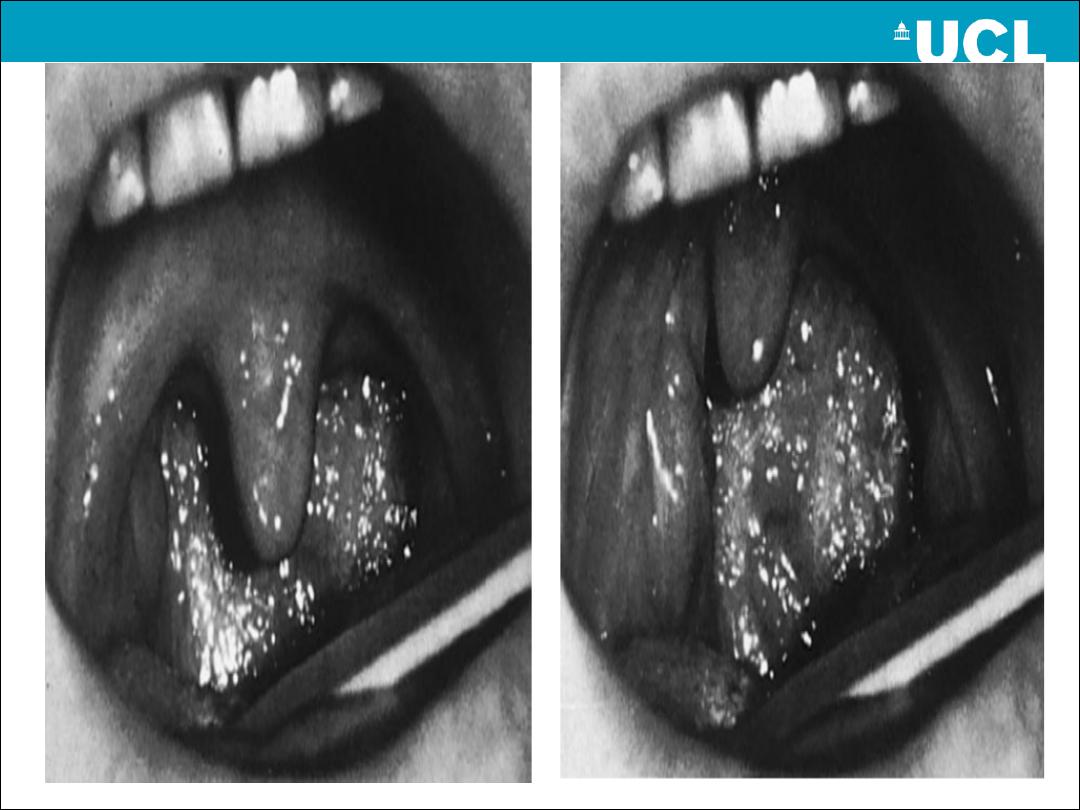
Disorders of GPN and VN
Bulbar and Pseudo bulbar palsy
- similarities and
differences, causes
Vascular
Inflammation
Tumors
Motor neuron disease
Myasthenia gravis
Accessory Nerve
Two parts:
cranial
( with CN X supplying the larynx; exit from
jugular foramen), and
spinal
(from C1-C6, enter the skull via
the foramen magnem to exit again via jugular foramen)
Mediates
Pure Motor function
to the sternomastoid and trapezius
muscles
Most common cause is iatrogenic injury( neck surgery)
Injury results in weakness or paralysis of respective muscles
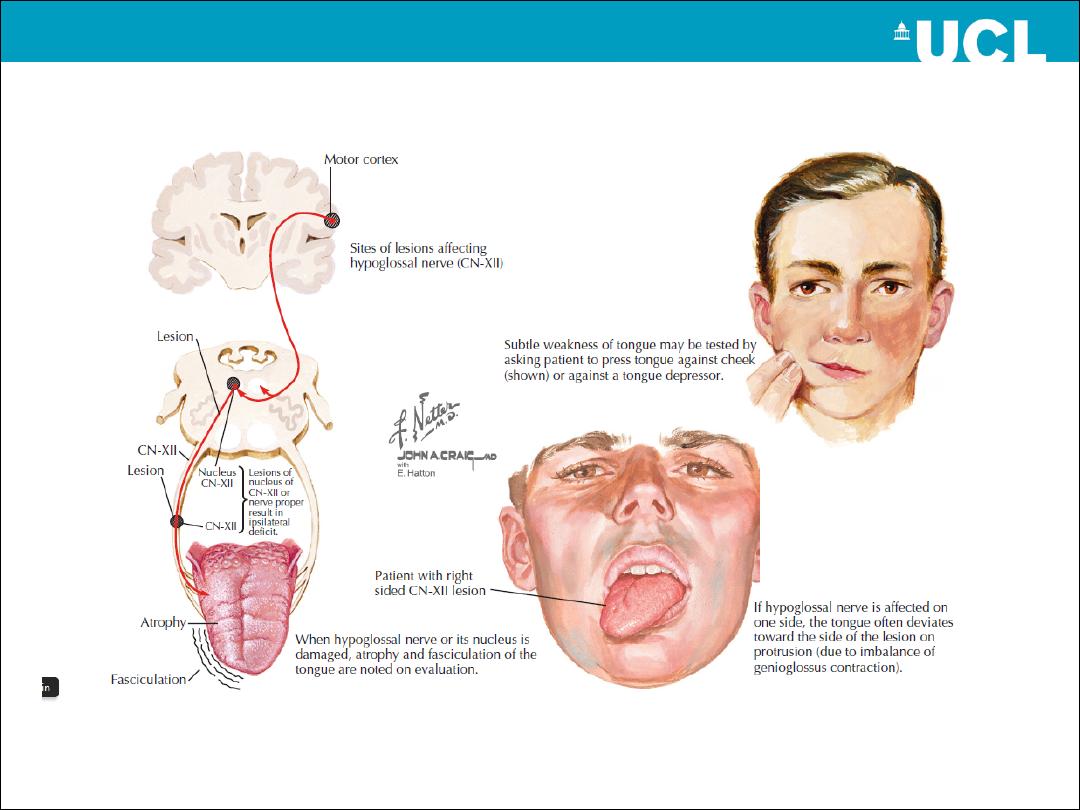
Hypoglassal nerve
Pure motor nerve
GSE to the extrinsic and intrinsic muscles of tongue
Nucleus: medulla
Exit foramen: hypoglossal canal
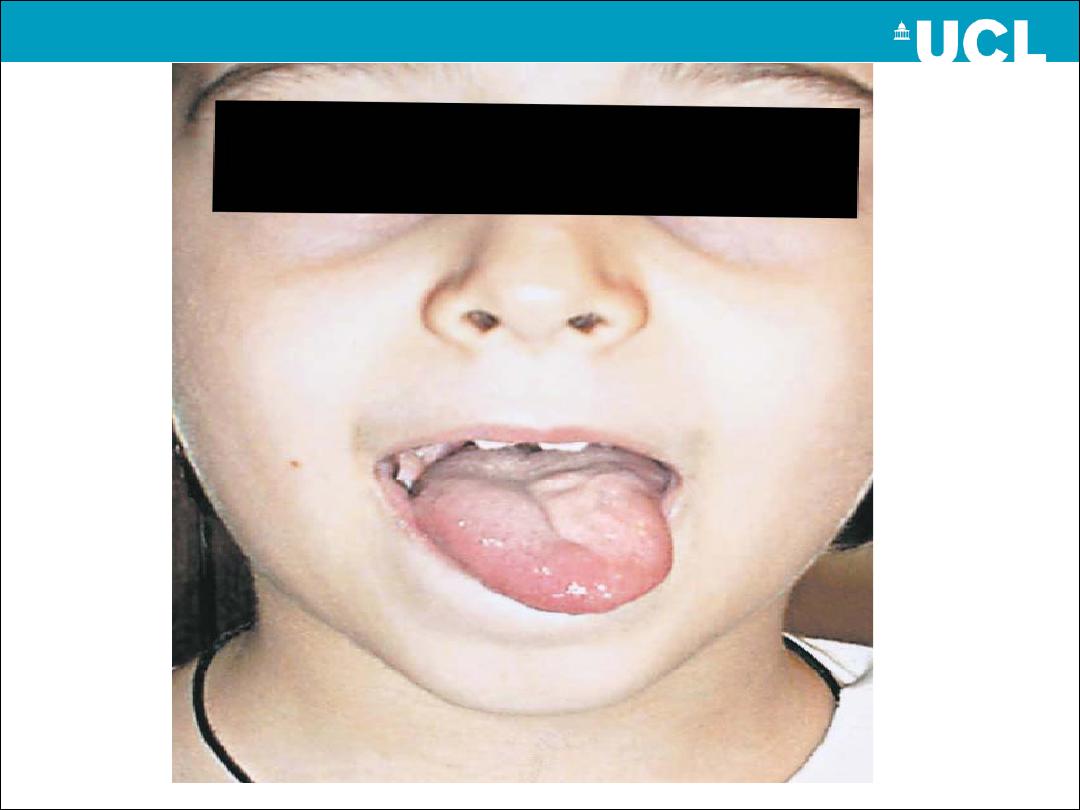
•Deviation of tongue will be
to the side of affected
hypoglossal nerve.
GOOD
LUCK