
1
The ankle & foot
د
.
ﻣ
ﮭ
ﻨ
ﺪ
ﻋ
ﻠ
ﻲ
Congenital deformities
novarus (idiopathic club foot)
Talipes equi
It is a common congenital deformity, the incidence ranging from 1-2/1000 of live birth,
boys are affected twice as often as girls & it is bilateral in 1/3 of the cases.
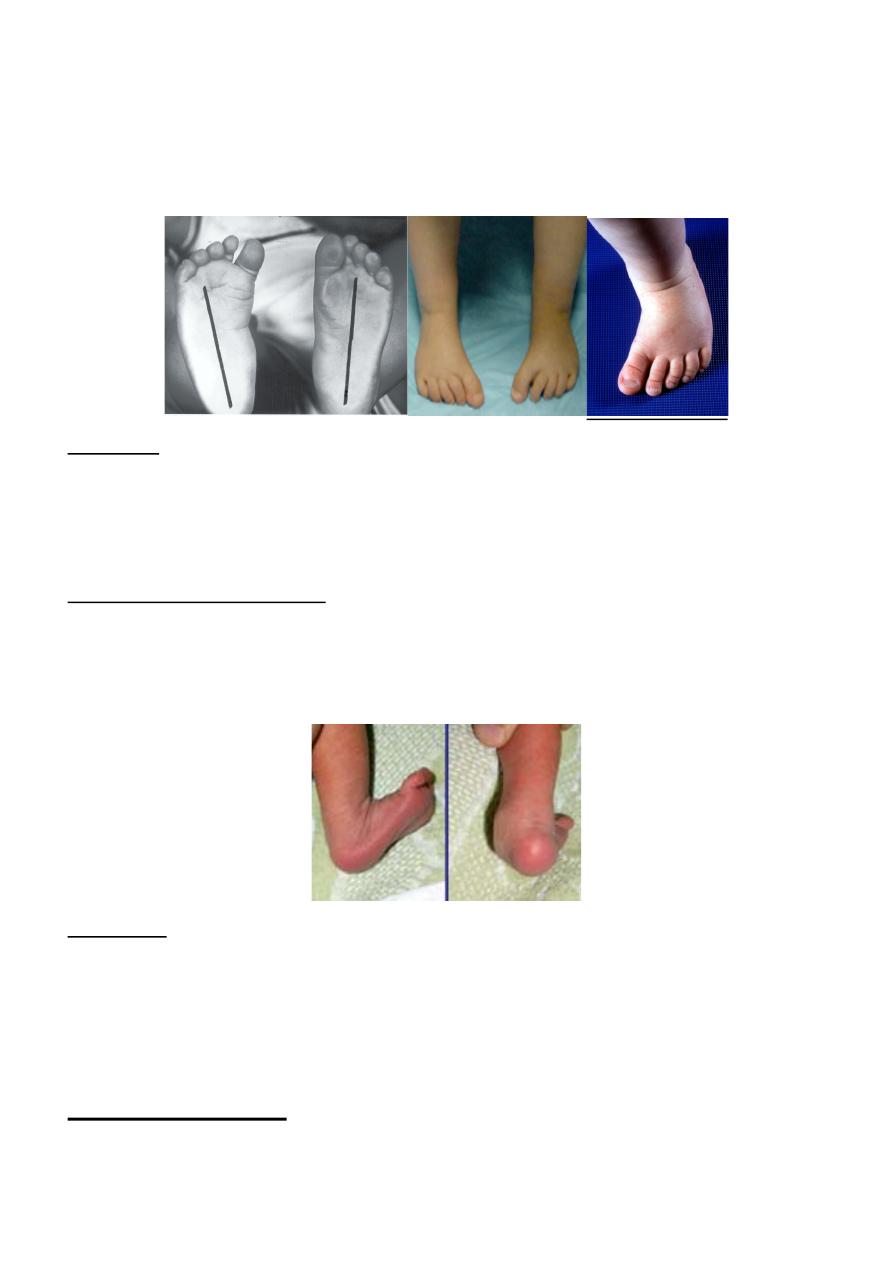
The term Talipes is derived from tali =talus =ankle bone, pes =foot, the equinovarus
mean the heel is in equines & the hind foot is in varus & the mid-foot & the forefoot
adducted & supinated.
The causes;
• Genetic disorder or a form of arrested development.
• Neuromuscular disorder & neural tube defect (myelomeningiocele & spinal dysraphism).
• Postural, caused by tight packaging in an overcrowded uterus.
Clinical features;
The ankle is in equinus, the heel is inverted & the forefoot is adducted & supinated, the
foot may have high medial arch. The heel is small & high. & deep creases appear
posteriorly & medially.
In the normal children the foot can be dorsiflexed & everted until the toes touch the front
of the leg. In club foot this is difficult.
Treatment;

2
The aim of treatment is to correct the deformity & hold it in the corrected position (i.e. to
Obtain& maintain plantigrade, supple foot that will function well).this can be achieved by
one of the following;
1. Conservative treatment by stretching & splintage.
2. Operative treatment.
Conservative treatment
This treatment is started in the 2
nd
or 3
rd
day of life & it consist of repeated manipulation
& stretching followed by an above knee POP cast to maintain the correction the
manipulation & casting is repeated every week until we obtain correction & slightly
overcorrection after that the correction is maintained by splint until the child is walking,
then the splint is used only at night until skeletal maturity.
Operative treatment
It is indicated for severe & rigid deformities, those who fail to respond to conservative
treatment& those who present after the age of 6 months.
This treatment is consist of elongation of the Achilles tendon & capsulotomies of the
ankle & subtalar joints, release of the shorten medial soft tissue & elongation of the long
flexors of the toes, then after obtaining the correction, it is held by casting for 3 months
then splintage until walking then night time splint until skeletal maturity.
For children with failed correction or relapse after treatment & those who present
between 5-10 yr, corrections is surgical & include soft tissue releases combined with
bone reshaping osteotomies.
For patients above the age of 10 yr the treatment is by triple arthrodesis
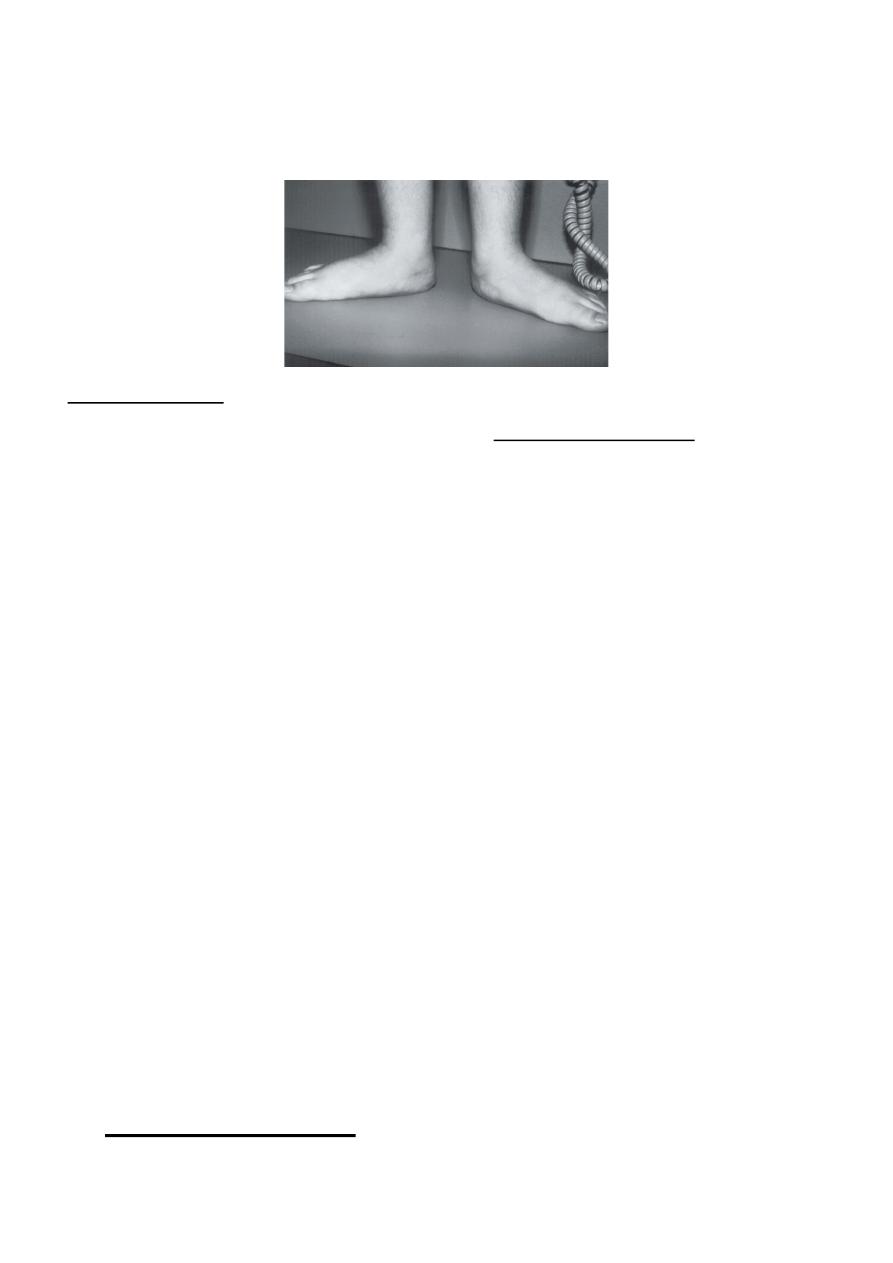
Metatarsus adductus (congenital forefoot adduction)
3
It is a common congenital anomaly; it could be unilateral or bilateral & may be associated
with developmental dysplasia of the hip (DDH). It is common in the first year of the life
& causes an in-toeing gait.
Treatment;
If it is passively corrected, it needs stretching & observation. If it is rigid then it need
serial manipulation & casting (more than 90% of the cases can be treated none
operatively). If these measures fail then surgery is indicated.
Congenital calcaneovalgus
It is a common deformity caused by abnormal intrauterine position, it present as acutely
dorsiflexed foot with deep crease in front of ankle joint, it can be corrected by passive
stretching. The deformity is usually bilateral & there is an association with (DDH).
Treatment;
it is often corrected spontaneously in the neonatal period, severe deformities
occasionally require serial manipulation & casting.
Flat-foot (pes planus)
4
It is a condition in which there is flattening of the medial longitudinal arch of the foot
usually with valgus of the hind foot.
Causes of flat-foot
; the causes of flat-foot differ according to the age group:
• In the neonate it is congenital & caused by congenital vertical talus.
• In children & adolescents, the flat-foot could be;
1. flexible flat-foot; it is common in toddlers & consider as a normal stage in
the development, it disappear spontaneously as the child grow , occasionally it
persist to the adult life, it may be associated ligamentous laxity or family history of
flat-feet. The deformity is flexible & can be corrected passively by dorsiflexing the
big toe (Jack test).
2. stiff or rigid flat-foot; in which the deformity can not be corrected
passively by dorsiflexing the big toe, it is usually due to underlying abnormality
like tarsal coalition, inflammatory joint disorder or neurological disorders.
3. Compensatory flat-foot; in which the flat-foot deformity occur to
compensate for some other postural deformities like tight tendo Achillis
compensated by everting the foot), external rotation deformity of the lower limb
(the body weight fall anteromedial to the ankle & the feet go into the valgus – the
Charlie Chaplin look) & the genovalgum knees.
• In adults; the flat-feet may be due to child hood flexible flat-feet, tarsal coalition,
disorders of tibialis posterior tendon, post traumatic deformity, degenerative
arthritis, inflammatory arthritis, neuromuscular disorder.
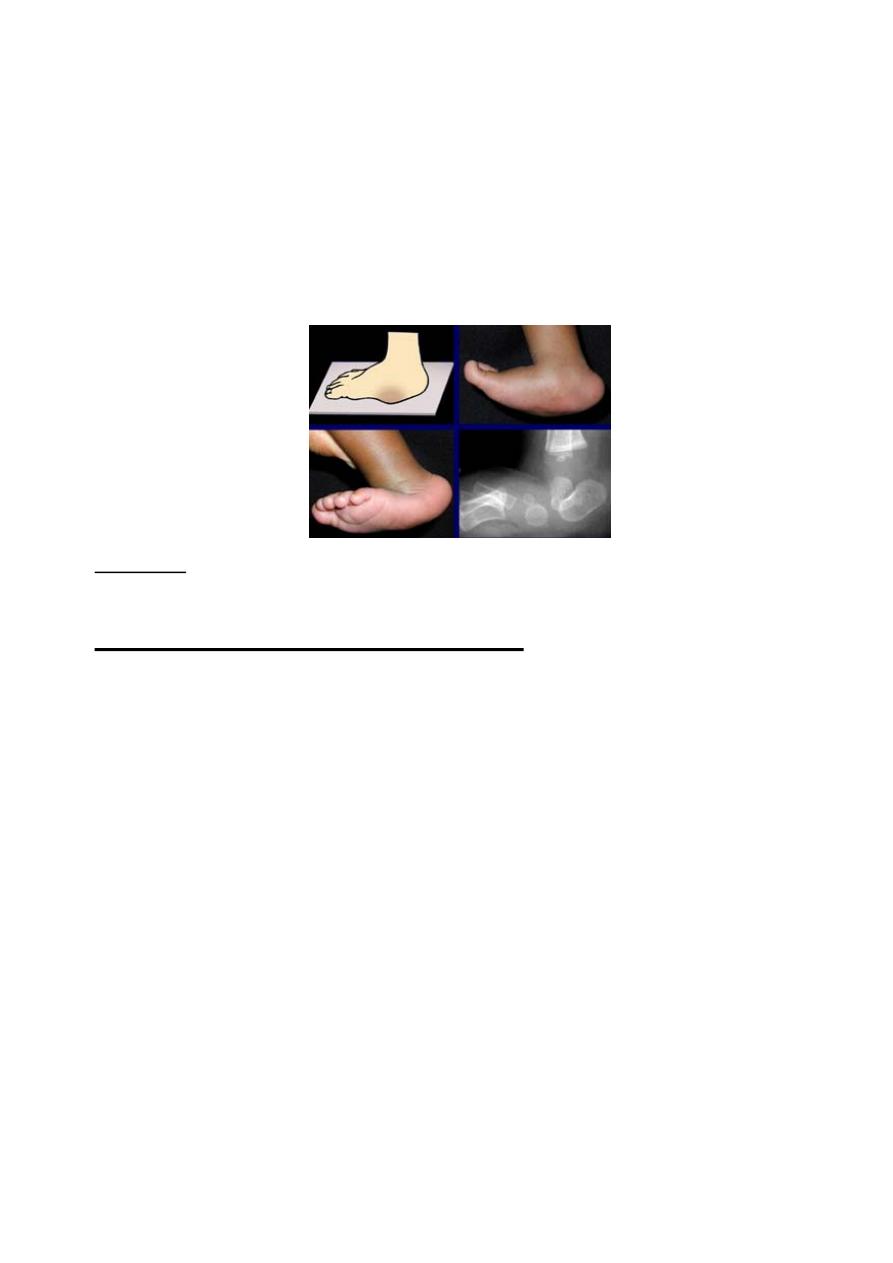
Congenital vertical talus
5
It is a rare deformity seen in infants, it usually affects both feet, on examination the
medial side of the foot is bulging into the sole of the foot leading to appearance of
rocker-bottom foot, the hind foot is in equinus & valgus, the forefoot is abducted,
pronated & dorsiflexed, the talus is vertical & pointed towered the sole with dorsal
dislocation of talonavicular joint, the deformity is rigid & passive correction is
impossible.
Treatment;
it operative by open reduction of the dislocated joints & release of
contracted soft tissues, the operation usually done before the age of 2 yr.
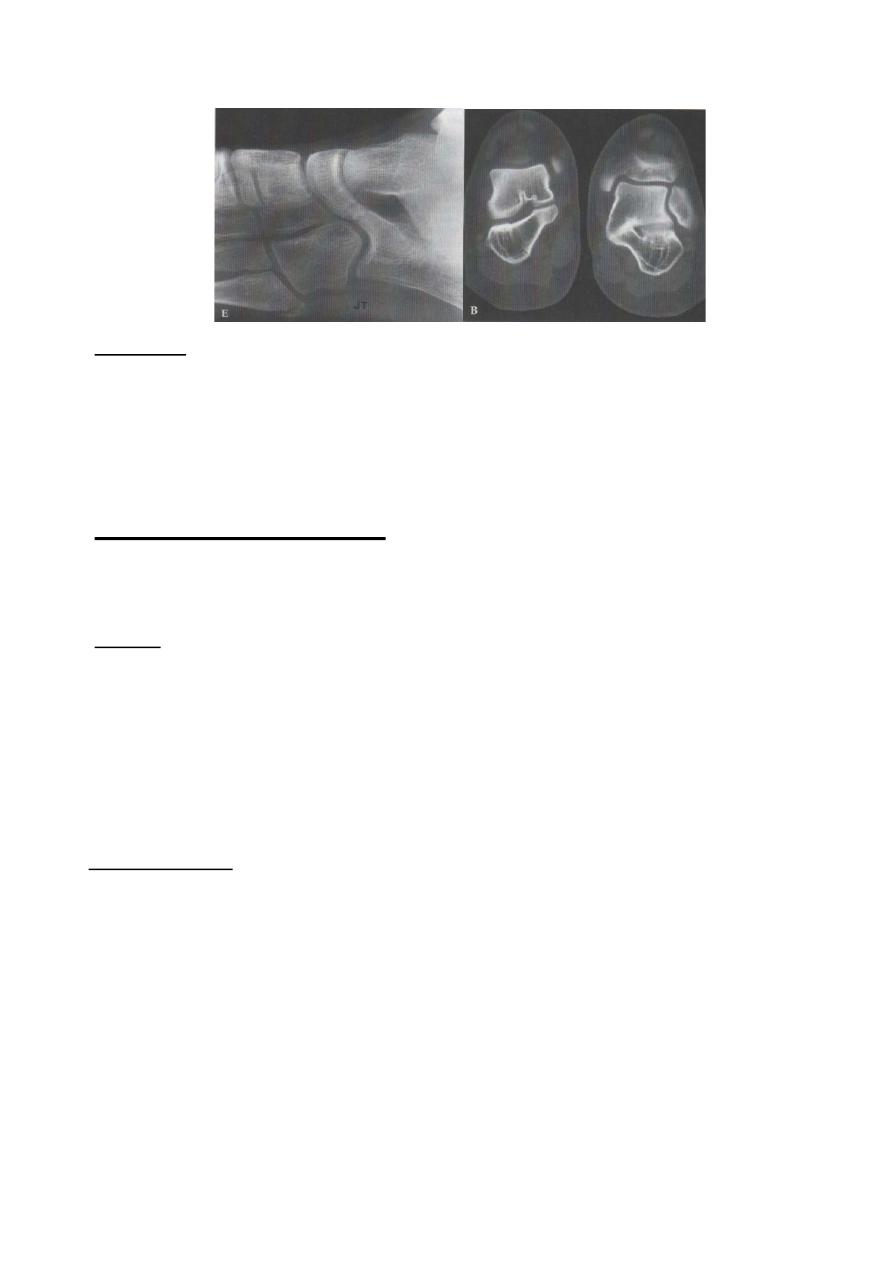
Peroneal spastic flat-foot (tarsal coalition)
This condition usually occur in adolescent where the foot at rest looks normal but after
walking & exercise it become painful with rigid flat-foot, it is caused by spasm of the
Peroneal & extensor muscles. The condition could be idiopathic or it may be
associated with tarsal coalition (partial or complete fusion between two or more of
tarsal bones).
The cause of the pain is either from stress # of these bony bars or from spasm of the
muscles.
X-ray & CT scan may show the abnormal coalitions.
6
Treatment;
The initial treatment is always conservative by resting the foot in a walking cast
followed by splint, if this fail then operative by excising the bony bare is indicated.
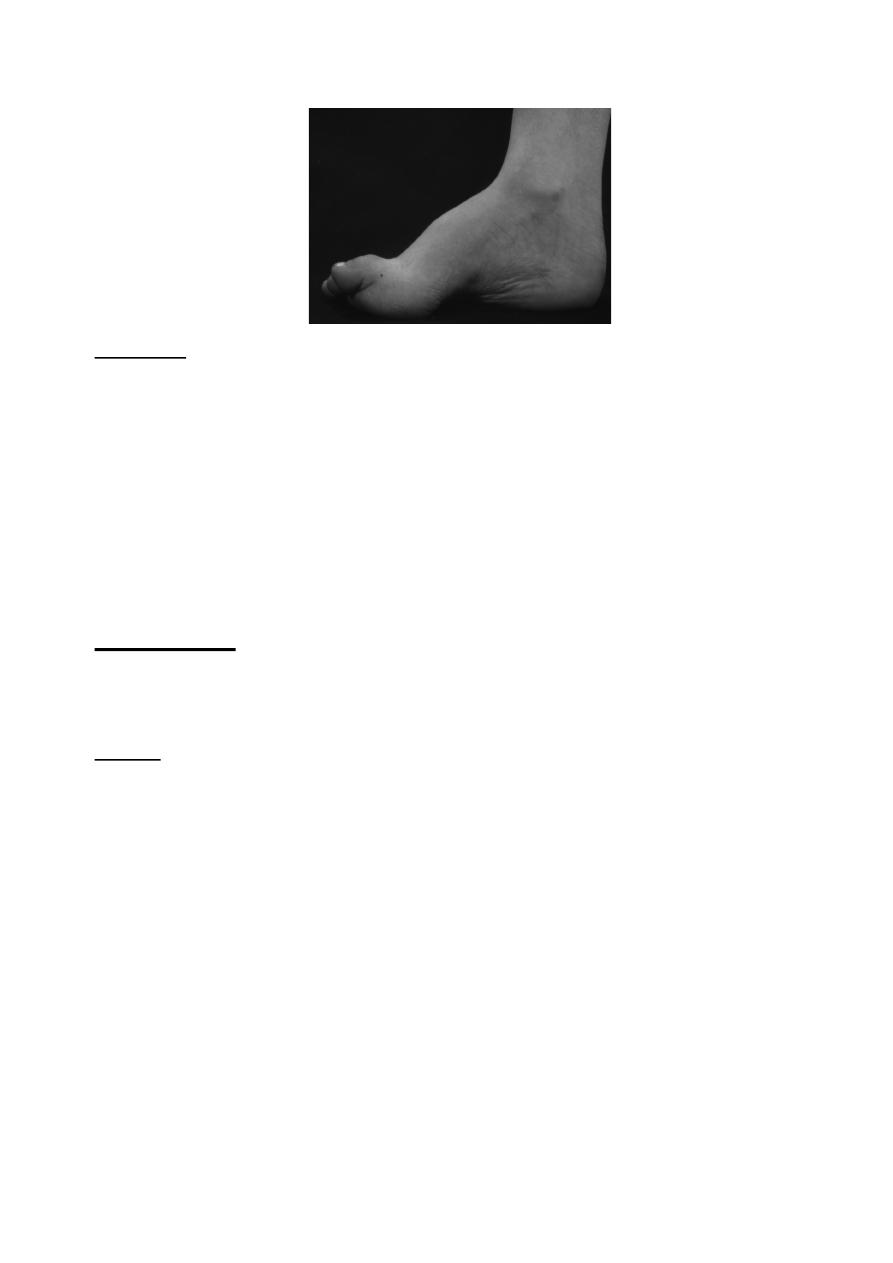
High-arched feet (pes cavus)
In this deformity the medial arch of the foot is higher than usual, with varus hind-foot
& clawing of the toes.
Causes;
1.
Congenital causes like arthrogryposis multiplex congeniti.
2.
Neuromuscular disorders like muscle dystrophies, peripheral neuropathies, spinal
cord disorders, (tethered cord, syringomelia), brain disorders (Friedreich's ataxia,
cerebral palsy).
3.
Trauma, burns, compartment syndrome.
Clinical features;
The medial arch is accentuated, the heel is inverted, and the toes are clawed with
callosities under the metatarsal heads (from friction with the shoes).
In early stages the deformity is flexible & can be corrected by pressure under the first
metatarsal head (pushing it up) this will correct the claw toe deformity & the high arch
deformity, later on the deformity will become stiff & rigid.
7
Treatment;
If the deformity is painless &mobile, no treatment is needed apart from shoe
modification.
If the deformity is painful but still mobile & the shoe wear modification fail to relive
the symptoms then the deformity can be corrected by soft tissue release & tendon
transfer.
For painful, stiff deformities, it needs corrective osteotomies & arthrodesis.
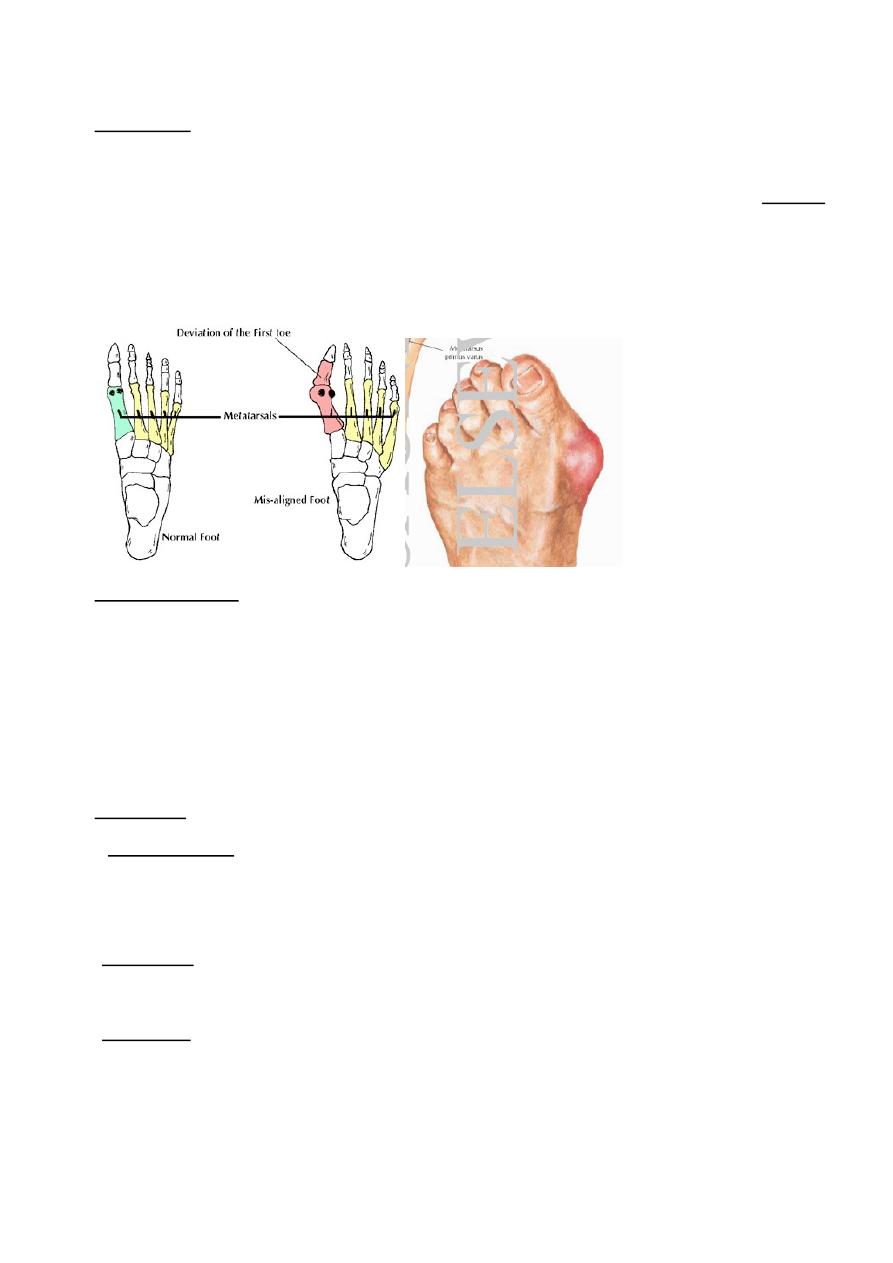
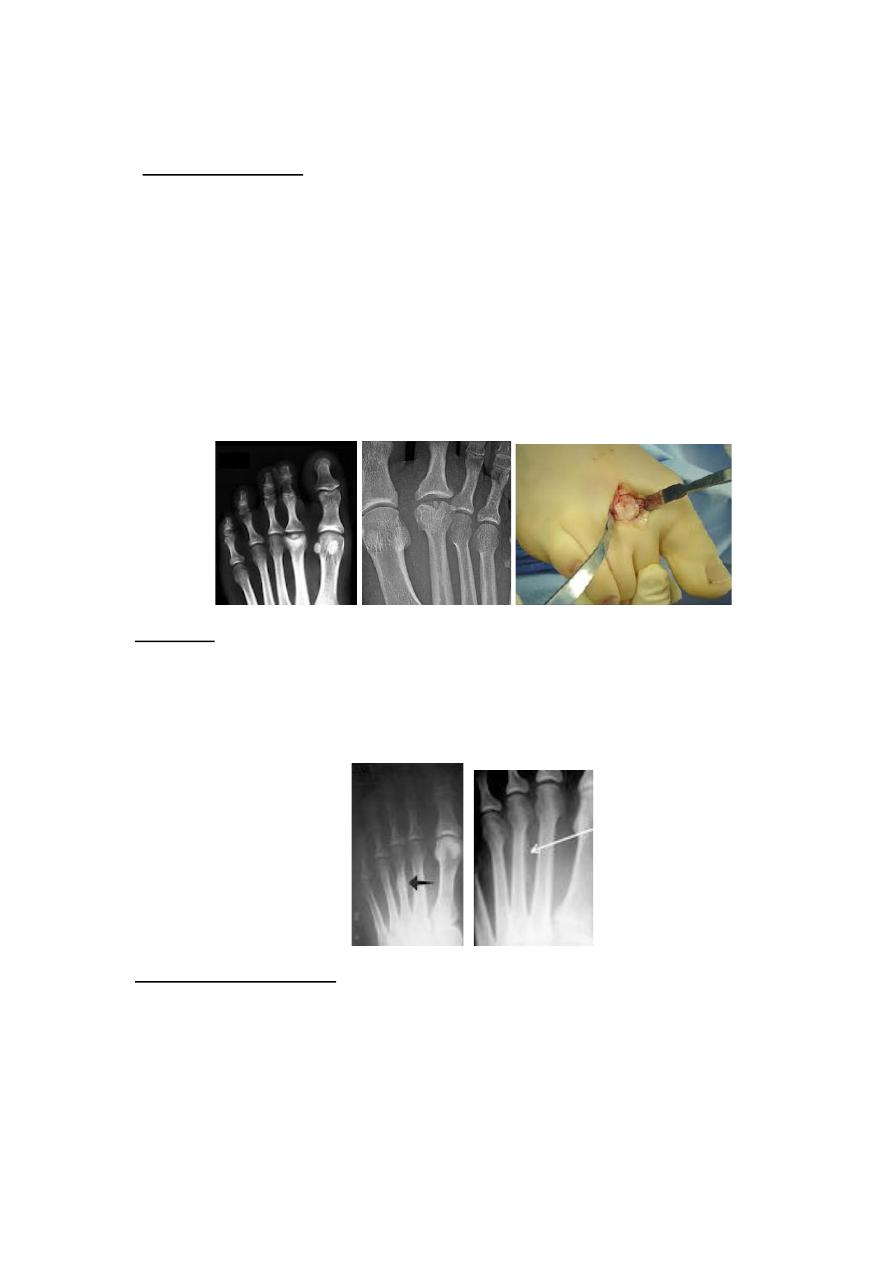
Hallux valgus
It is the commonest of the foot deformities, in which the big toe deviated into the
lateral side (valgus) with rotation.
Causes;
the primary abnormality is the varus angulation of the first metatarsal bone
(deviated to the medial side) called
metatarsus primus varus
, the causes of this are:
1. Congenital metatarsus primus varus, this type usually occurs in young
adolescent girls, usually with family history of Hallux valgus in her mother.
2. Loss of muscle tone in the forefoot in elderly women leading to splaying of
the forefoot.
3. Neuromuscular disorder associated with muscle imbalance.
4. Rheumatoid arthritis.
8
Pathology;
The deformity consist of
1. lateral deviation & rotation of the Hallux,
2. There is prominence on the medial side of the first metatarsal head called bunion
this is caused by; Subluxation of the first metatarsophalangeal joint. Overlying
bursa. Thickening of the skin & soft tissues.
3. In long-standing cases the metatarsophalangeal joint become osteoarthritic.
Clinical features;
The patient is usually a women aged between 50-70 yr & the deformity is usually
bilateral; a second group of patient is an adolescent usually with family history.
The patient present with deformity, sometime there is pain over the large bunion
On examination the Hallux is in valgus & rotated, the forefoot is widened; palpation
may reveal tenderness over the bunion or over the metatarsophalangeal joint.
Treatment;
if the deformity is asymptomatic then no treatment is required.
• In adolescent; the initial treatment is conservative by modification of the shoes, by
using wide toe box shoes to accommodate the deformity, if this fail then surgery is
required, the type of surgery will depend on the severity of the deformity.
• In adult; the treatment is the same as in adolescent except that if the
metatarsophalangeal joint is osteoarthritic then the treatment is by arthrodesis.
• In elderly; the treatment is usually conservative if this fail then surgery either in the
form of arthrodesis or Excisional arthroplasty (by excising the base of the proximal
phalanx of the big toe).
9
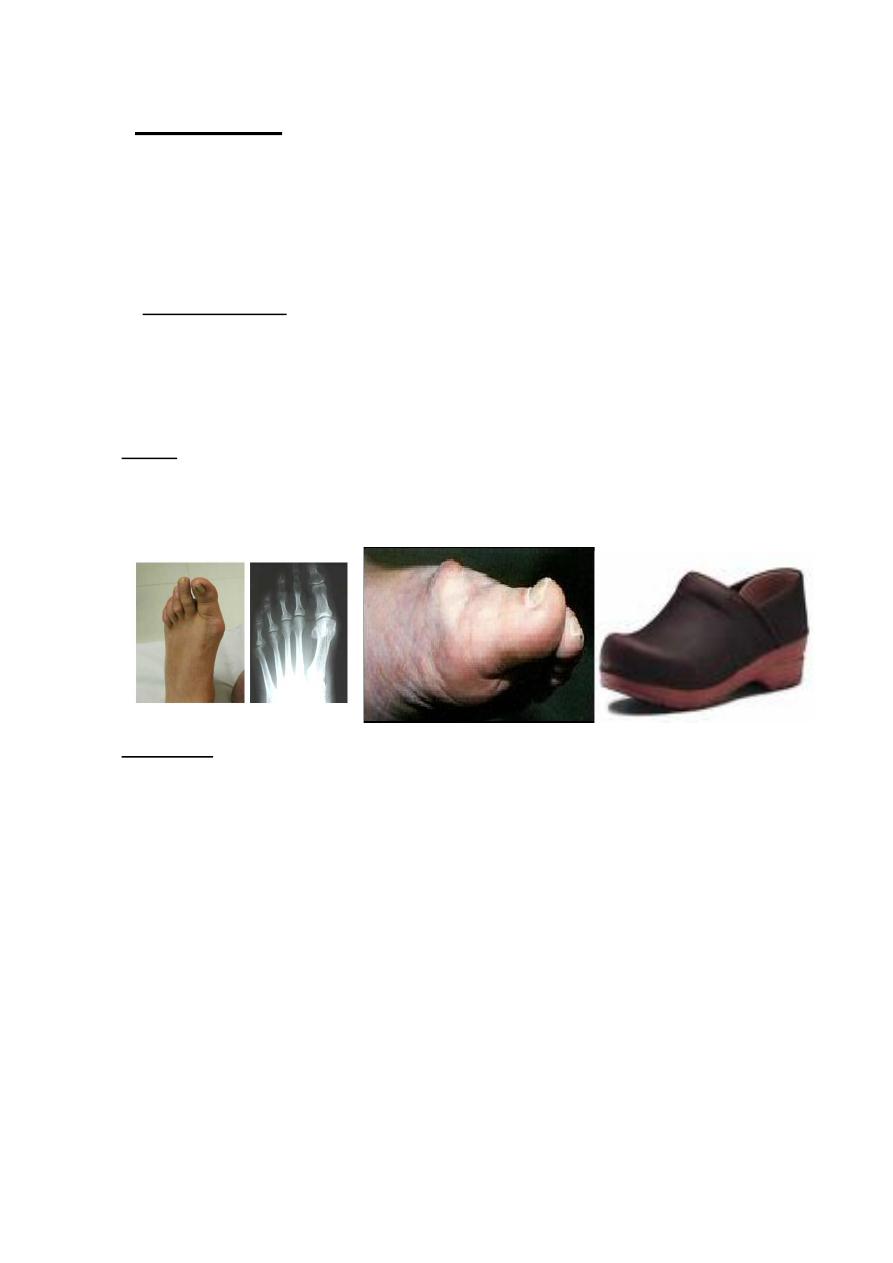
Hallux rigidus
It is a painful & stiff first metatarsophalangeal joint, due to osteoarthritis
secondary to;
(1) Trauma. (2) Osteochondritis dissecans of the metatarsophalangeal joint.
(3) Gout & pseudo gout.
Clinical features;
The patient has pain in the metatarsophalangeal joint on walking; the Hallux is
straight with callosity on the medial side of the distal phalanx, the joint feel
knobbly with tender dorsal bunion, the dorsiflexion is restricted & painful.
X-ray;
Show the signs of osteoarthritis with narrowing of joint space & large dorsal
osteophyte.
Treatment;
The initial treatment is conservative by using rocker-soled shoes which allow the
foot to roll without the necessity for dorsiflexing the metatarsophalangeal joint, if
this fail to relive the symptoms then surgery is indicated there are different types of
operations:
• Extension osteotomy of the proximal phalanx to mimic the dorsiflexion.
• Cheilectomy by removal the dorsal osteophyte & the dorsal part of the
metatarsal head to increase the dorsiflexion.
• Joint replacement using silastic prosthesis.
• Arthrodesis of the first metatarsophalangeal joint.
10
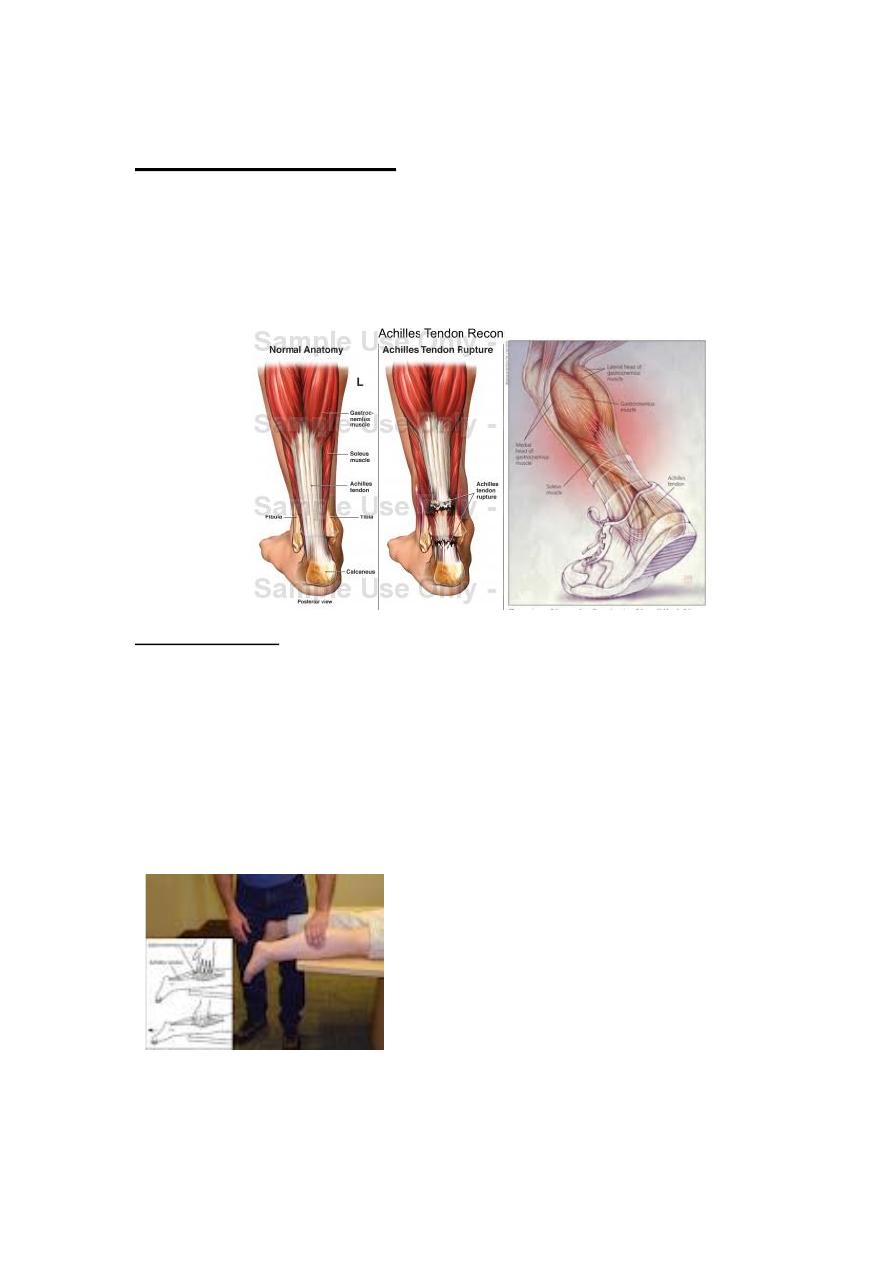
Rupture of tendo-Achillis
Spontaneous rupture occur when the tendon is degenerated & weakened,
consequently most patients are over 40 yr, the rupture occur while the patient
pushing off as in running or jumping, during this the calf muscles contract but the
contraction is resisted by body weight & the tendon ruptures.
Clinical features;
After jumping or running the patient feels as if has been struck above the heel &
he is unable to perform tiptoe (standing on tiptoe).
Soon after the tear a gap can be seen & felt 5 cm above the insertion of the
tendon, planter flexion of the foot is weak & Simmond's test is positive(with the
patient prone the calf is squeezed, if the tendon is intact, the foot is seen to
plantar-flexed but if the foot is ruptured the foot remains still.
11
Treatment;
If the tear is seen early then the ends of the tendon can be approximated by
planter flexion of the foot with plaster cast applied for 8 weeks followed by raised
heel shoe for another 6 weeks. Operative repair have little risk of rerupture
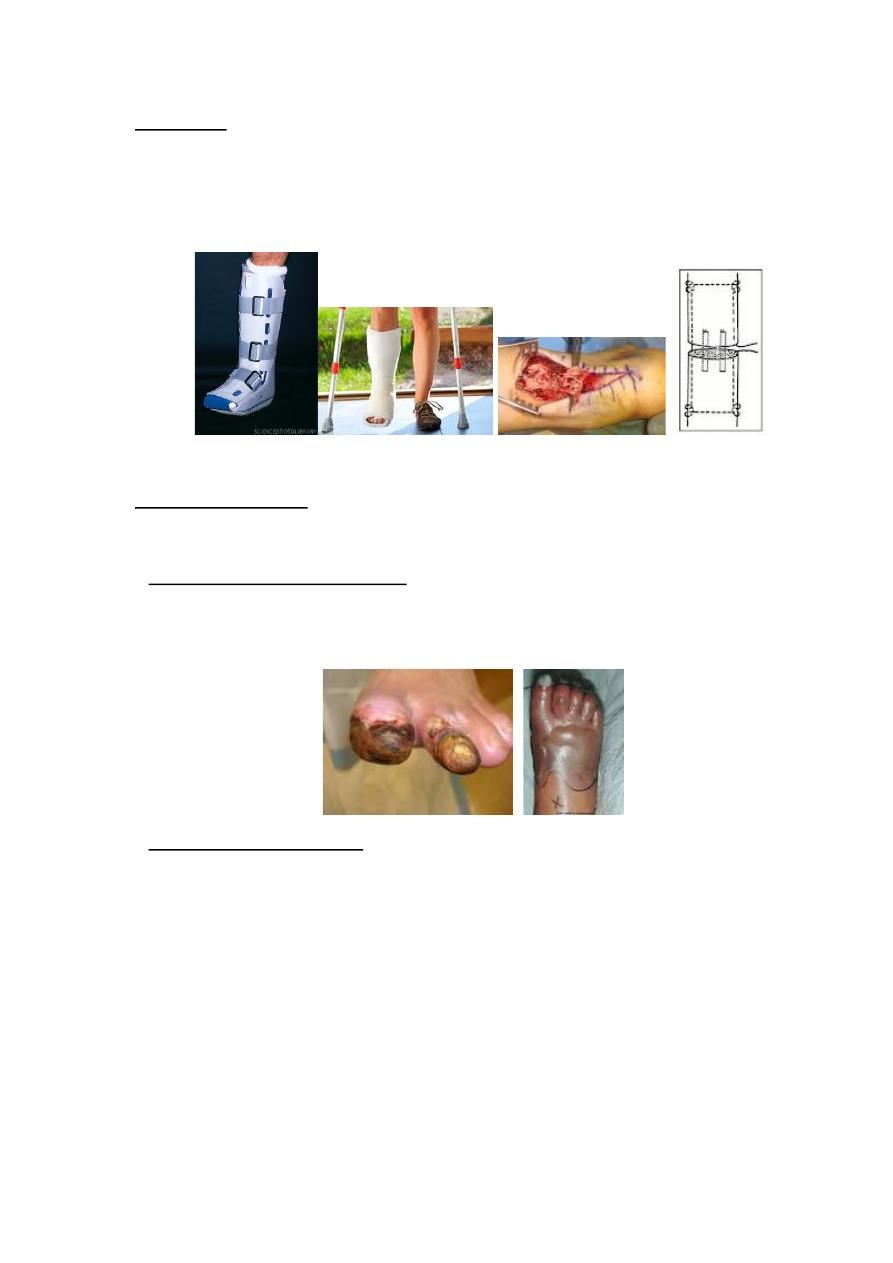
The diabetic foot
The foot disorders are common in diabetic patient & result from;
1. Peripheral vascular diseases commonly affecting the medium & small sized
vessels causing claudication, trophic changes, ulceration, dry gangrene from
obstruction of digital vessels & wet gangrene from proximal vascular occlusion.
2. Peripheral neuropathy loss of sensation lead to increase in risk of trauma &
burn, also cause hyperkeratotic skin from increase shoe pressure with subsequent
fissuring & ulceration, the neuropathy also affect the autonomic nervous system
(sweat gland in the skin) causing anhydrosis (dryness of the skin with fissuring),
the neuropathy may also affect the motor nerves leading to various deformities
which will increase the risk of ulceration & infection. The patient may develop
neuropathic joint (Charcot joint).
12
3. Diabetic osteopathy this consist of severe osteoporosis especially in foot with
stress #, other manifestation of osteopathy include cortical defect near the joint &
osteolysis.
4. Infection the diabetes will affect the white blood cell function (lazy leukocyte
syndrome) this together with local ischaemia & decrease sensation will increase
the risk of sepsis.
Treatment;
• Proper control of diabetes.
• Constant & careful attention to the skin & toe nail to prevent infection.
• Dry gangrene of the toe can be left to demarcate before amputation, wet
gangrene & infection may call for immediate amputation.
• Charcot joints causing instability may need splintage.
• Osteoporotic # should be immobilized only until pain subsides, movement is
important.
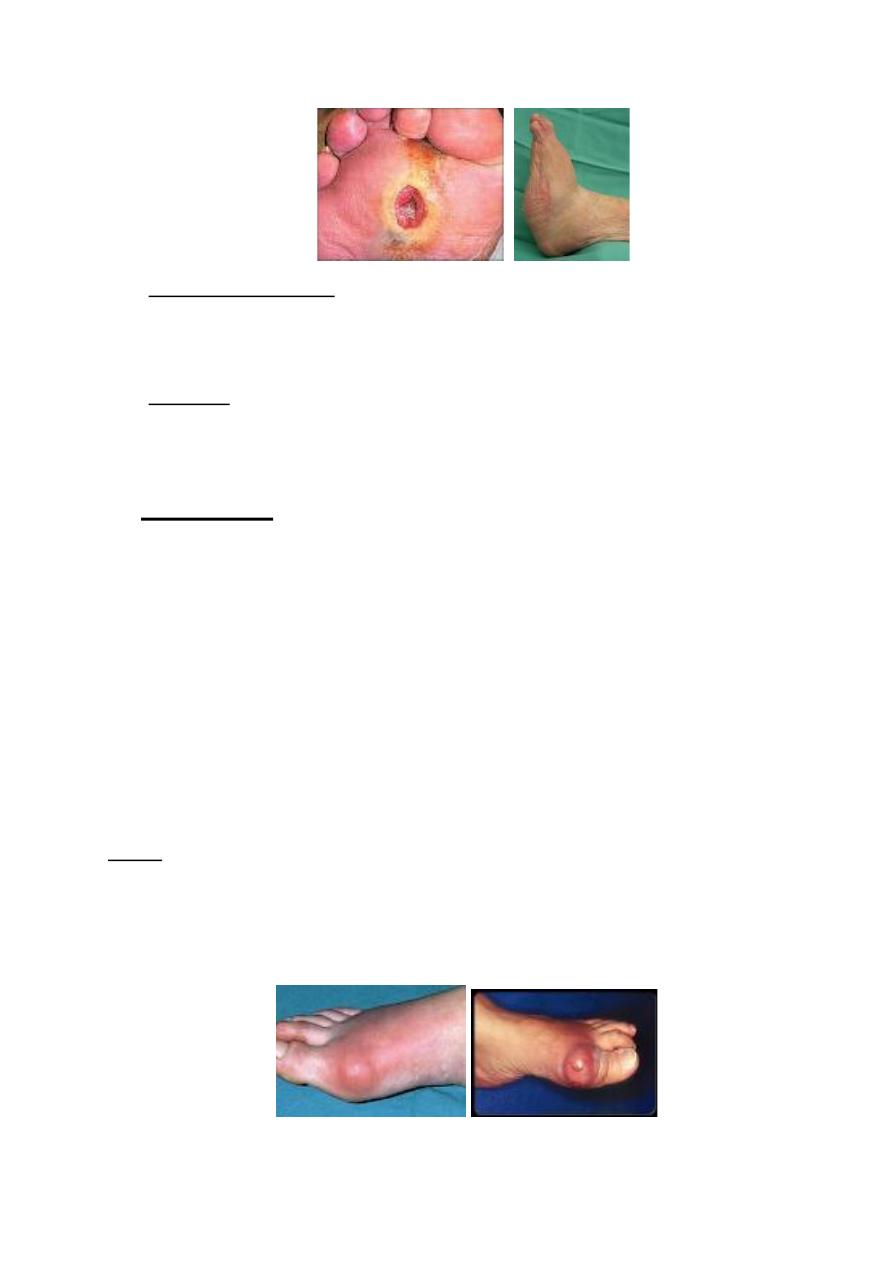
Gout
Gouty arthritis of the foot usually present as an acute inflammation of the
metatarsophalangeal joint of the big toe (podagra). The joint present with swelling,
redness, hotness & exquisite tenderness.
13
The condition closely resembles septic arthritis, but there is lake of systemic features
of infection (fever, tachycardia), the ESR & C-reactive protein are within normal &
serum uric acid level may be raised.
Treatment;
By NSAID will abort the acute attack, until the inflammation subsides the foot
should be rested & protected from injury.
Painful feet
This usually divided according to the site of pain into; heel pain, mid-foot pain &
forefoot pain.
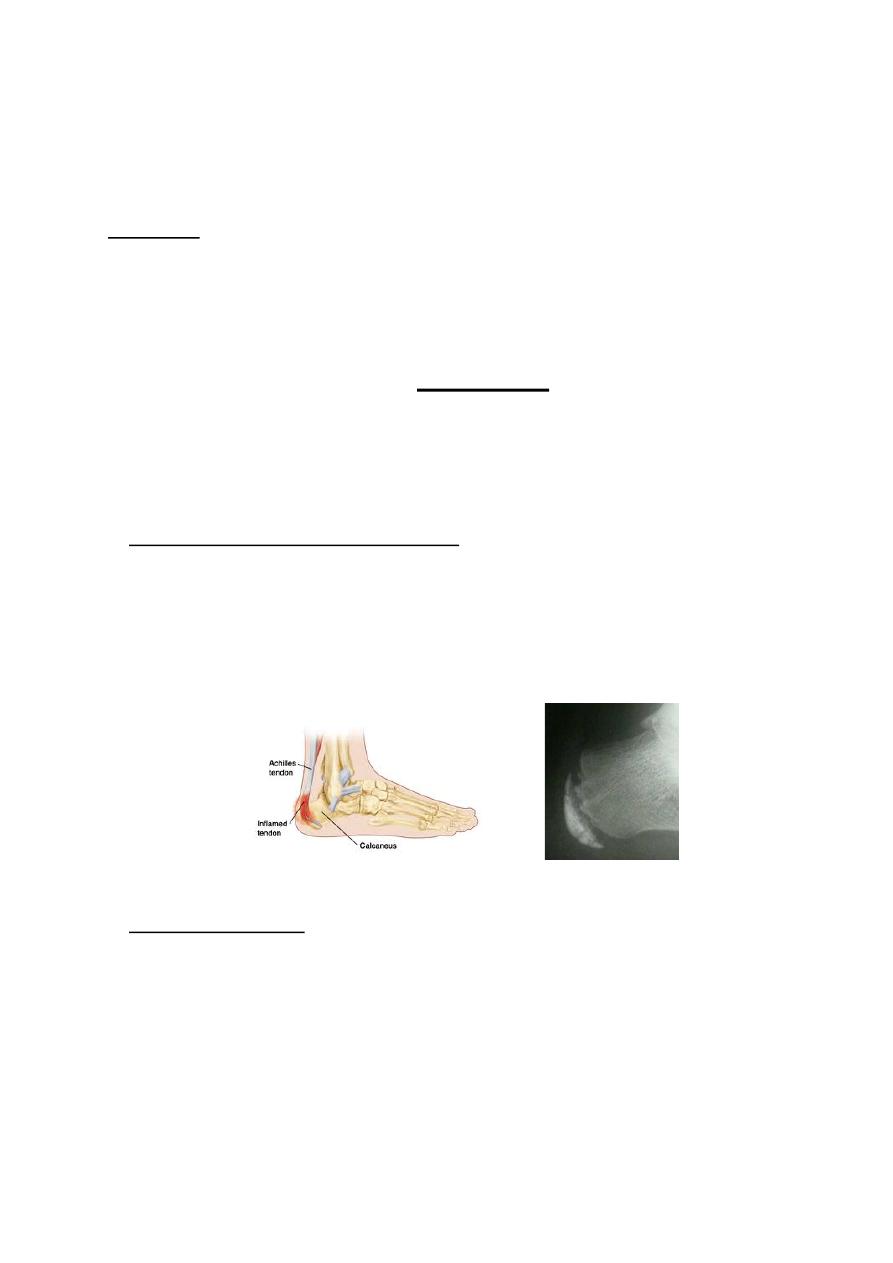
I. Posterior heel pain;
this is usually result from
;
• Traction apophysits (Sever's disease); it is a traction injury at the insertion of the
Achillis tendon to the calcaneum, it usually occur in boys of about 10 yr. the patient
present with pain, swelling & localized tenderness at the insertion of the Achillis
tendon. X-ray will show an increased density & fragmentation of the calcaneal
apophysis.
Treatment
; consist of raising the heel of the shoe & restriction of activities
• Calcaneal bursitis; this is caused by prominent posterolateral portion of the
calcaneum associated with shoe friction resulting in a retrocalcaneal bursitis. The
patient is a young woman complains of a painful bump on the back of the heel, the
symptoms worse in a cold weather & the disorder is sometime called winter heel.

14
Treatment;
conservative treatment by using open-back shoes & padding the heels,
operative treatment by removal of the bump.
II. Inferior heel pain;
this is usually result from;
•
Calcaneal bone lesions
;
any bone disorder in the calcaneum can present as a heel
pain (stress #, osteomyelitis, osteoid osteoma, cysts, Paget's disease); the x-ray
usually will provide the diagnosis.
• Planter fasciatis; it is characterized by sharp pain under the heel, usually the first
step after getting up from the bed or a period of inactivity is the worst but the pain
present through out the day, the patient is usually a men (30-60 yr), there is
tenderness along the distal edge of the heel contact area (the site of attachment of
planter fascia to the calcaneum).
X-ray;
may reveal a bony spur on the undersurface of the calcaneum.
Causes;
it may be associated with chronic stress as long period of standing or over
weight (policeman's heel) or it is associated with gout, Reiter's disease. Ankylosing
spondylitis as a part of enthesopathy.
Treatment;
by NSAID, heel pad or Cushing, local steroid injection, if these
measures failed then surgery is indicated.
15
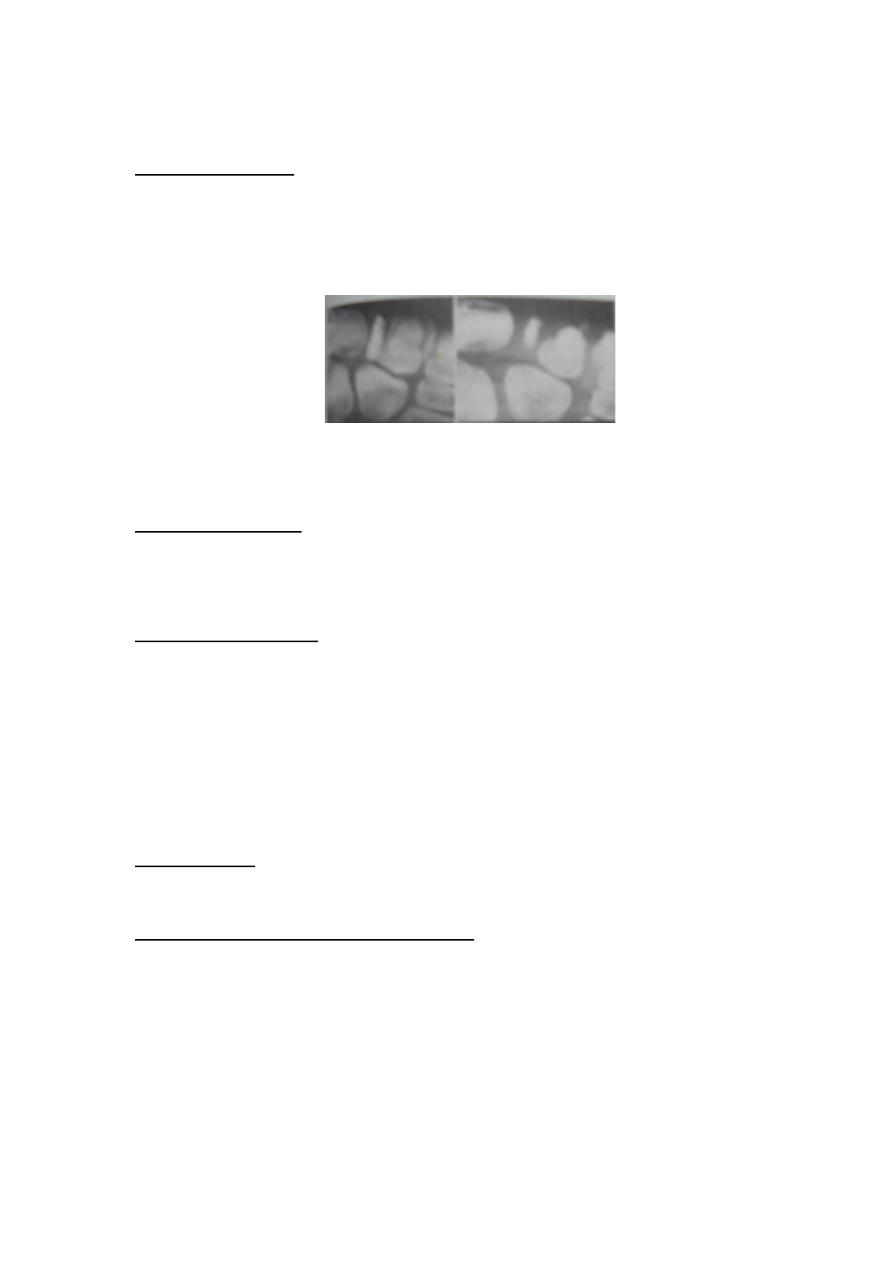
III. Painful mid-foot (painful tarsus);
this is usually result from ;
• Kohler's disease; it is crushing osteochondritis of the bony nucleus of the
navicular bone, it present in children under the age of 5 yr as a pain in mid-tarsal
region & limping with tender & thickening over the navicular bone. X-ray show
increase density & fragmentation of the navicular.
Treatment;
no treatment is needed as the condition resolve spontaneously, if
symptoms persist a short period of below knee cast.
• Brailsford's disease; this condition is similar to Kohler's disease but it occur in
middle aged women, the navicular become dense & alter in shape, later on
osteoarthritis of mid-tarsal joint may occur.
• Accessory navicular; in young adult pain over the medial aspect of the naviculum
may be due to congenital accessory navicular bone, the accessory bone may be
prominent under the skin & felt tender.
X-ray;
will show the type of this accessory segment that may need surgical
removal, otherwise simple adjustment of shoe wear can be helpful.
IV. Generalized pain in forefoot;
• Metatarsalgia; it is a generalized ache in the forefoot, it usually result from faulty
weight distribution or prolong & unaccustomed walking, climbing & standing.
• Pain in metatarsophalangeal joint; an inflammatory process in the
metatarsophalangeal joints as in rheumatoid arthritis may cause a generalized pain
in the forefoot & difficulty with shoe wear.
16
V. Localized pain in the forefoot;
this may be due to:
• Freiberg's disease; it is crushing type of osteochondritis of the second metatarsal
head rarely the third; it affects young adults, usually women. A bony lump (the
enlarge metatarsal head) is palpable & tender, the joint is irritable.
X-ray;
show the metatarsal head is wide, flat with thickening of the metatarsal neck
& increased joint space.
Treatment;
usually conservative by using a walking plaster to decrease pressure on
the metatarsal head, if this fail the operative treatment by Synovectomy &
trimming of the metatarsal head.
• Stress #; usually of the second or the third metatarsal, occur in the young adults
after unaccustomed activity. The affected shaft feels thick & tender, the x-ray
appearance is at first normal but later (after 2-3 weeks) it shows fusiform callus
around a fine transverse # line. Rest is all that is needed.
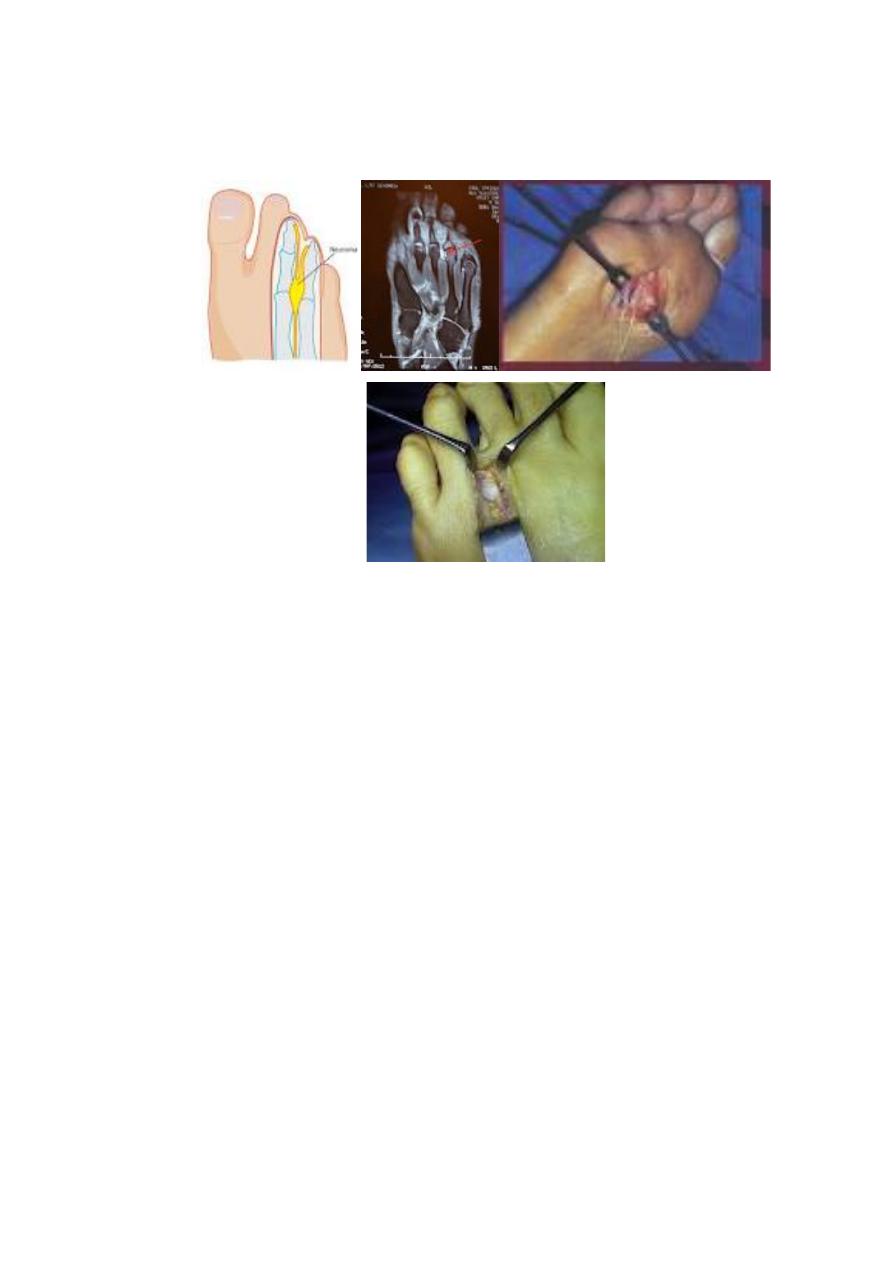
• Morton's Metatarsalgia; it is an entrapment neuropathy affecting one of the
interdigital nerves usually the third. The patient complains of pain in the forefoot,
radiating to toes. Tenderness is localized to one of the interdigital spaces-usually
the third & sensation may be diminished in the adjacent toes.
17
Treatment;
by using protective padding in the shoes, if this fail then surgical
excision of the neuroma.