BENIGN TUMORS OF
BONE

BENIGN TUMARS OF BONE
1-cystic lesions
2-fibrous lesions
3-cartilaginous lesions
4-benign (occasionally aggressive) bone tumors
5-bone forming tumors
6-miscellaneous bone tumors
Unicameral [simple bone]cyst
• Occurs in childhood, rare in adults, more in males
• Most in prox. Humerus or prox. Femur
• Two forms: - active
- inactive
• asymtomatic unless fracture is present
• Obliteration after healing of fracture
• X.Ray : lytic lesion
• Treatment: -curettage with or without bone graft.
-aspiration followed by instillation of . .
Methylprednisolone
- F.I.N

Pathological fracture :healing :remodling

Installation of prednisalone

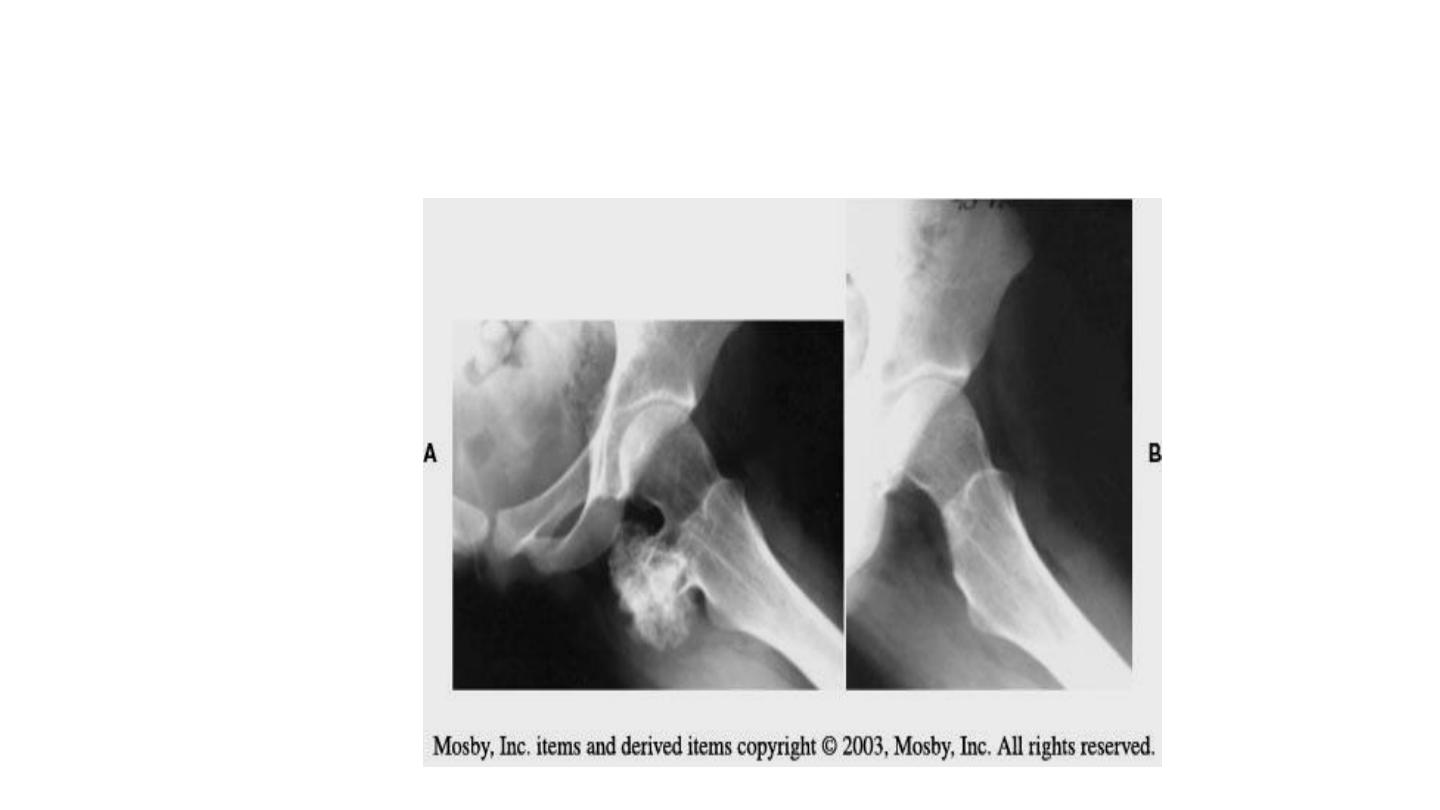
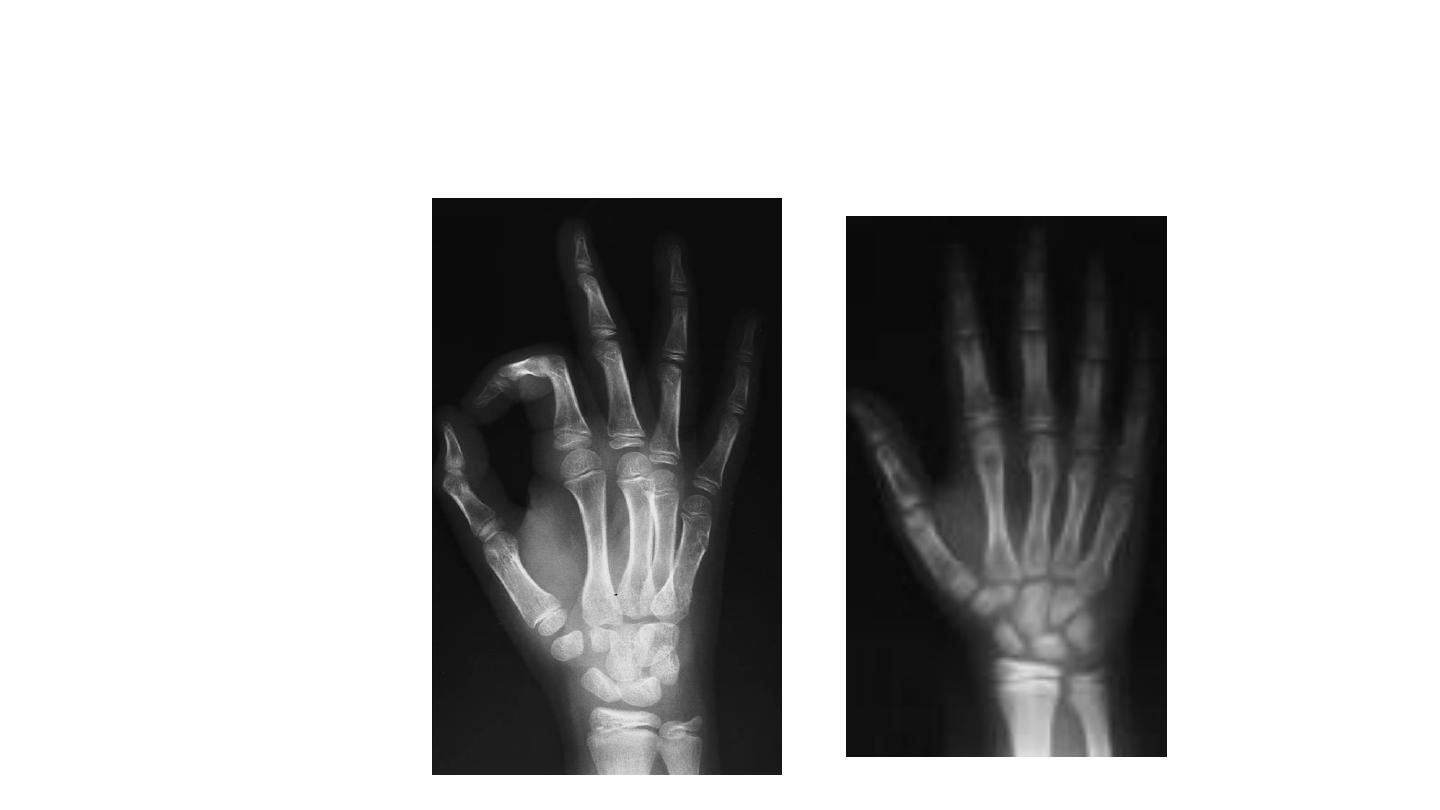
Aneurysmal bone cyst
• Occurs in any age, common in young adults
• X.Ray: lytic lesion have a honeycamb shape
• C.T: location & size – M.R.I: fluid levels
• Biopsy: to diff. Between G.C.T or Osteosarcoma
• Grow rapidly
• Treatment: curettage & bone grafting
• Recurrence approx. 25%
• Vertebral lesions treated surgically

Aneurysmal bone cyst of phalange
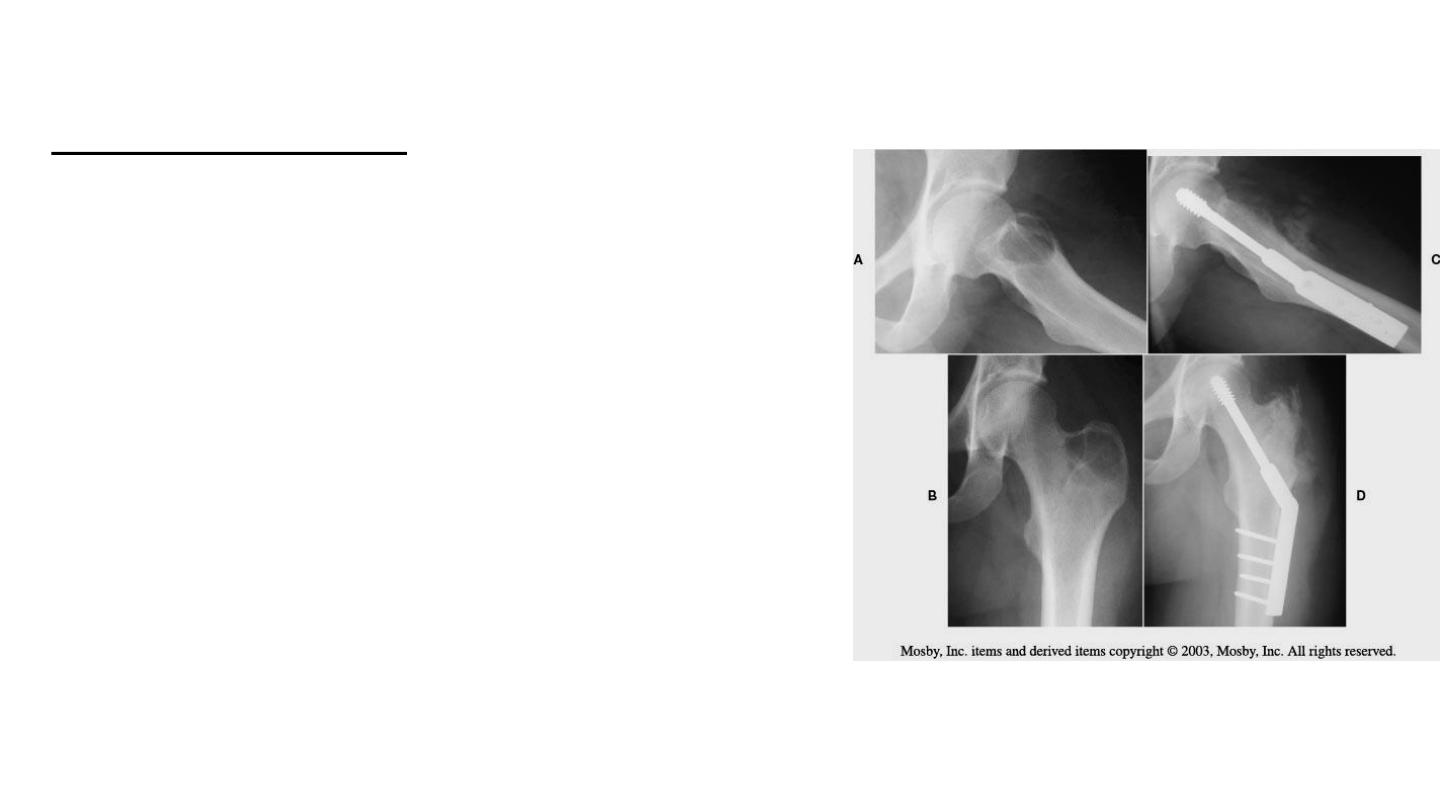
Fibrous lesions
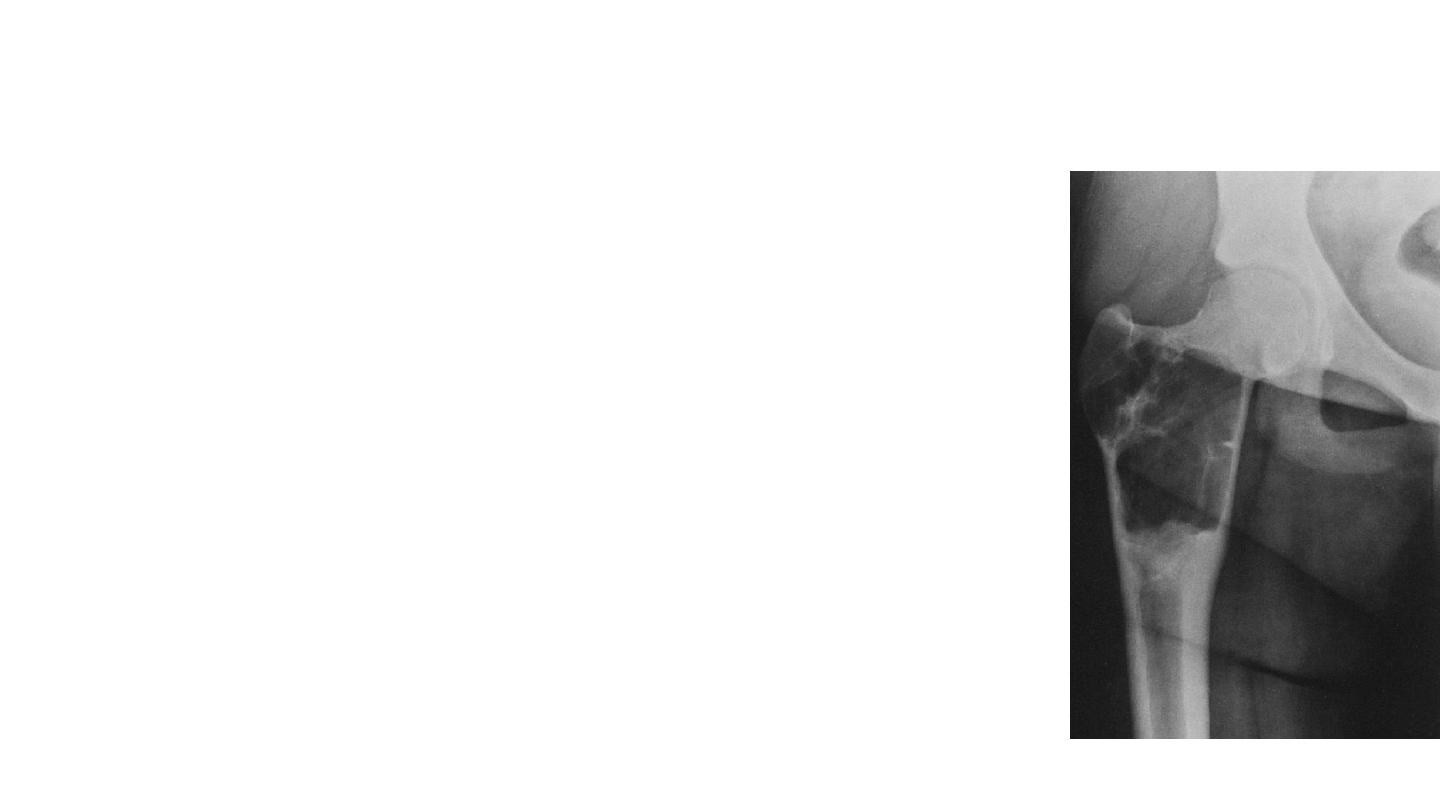
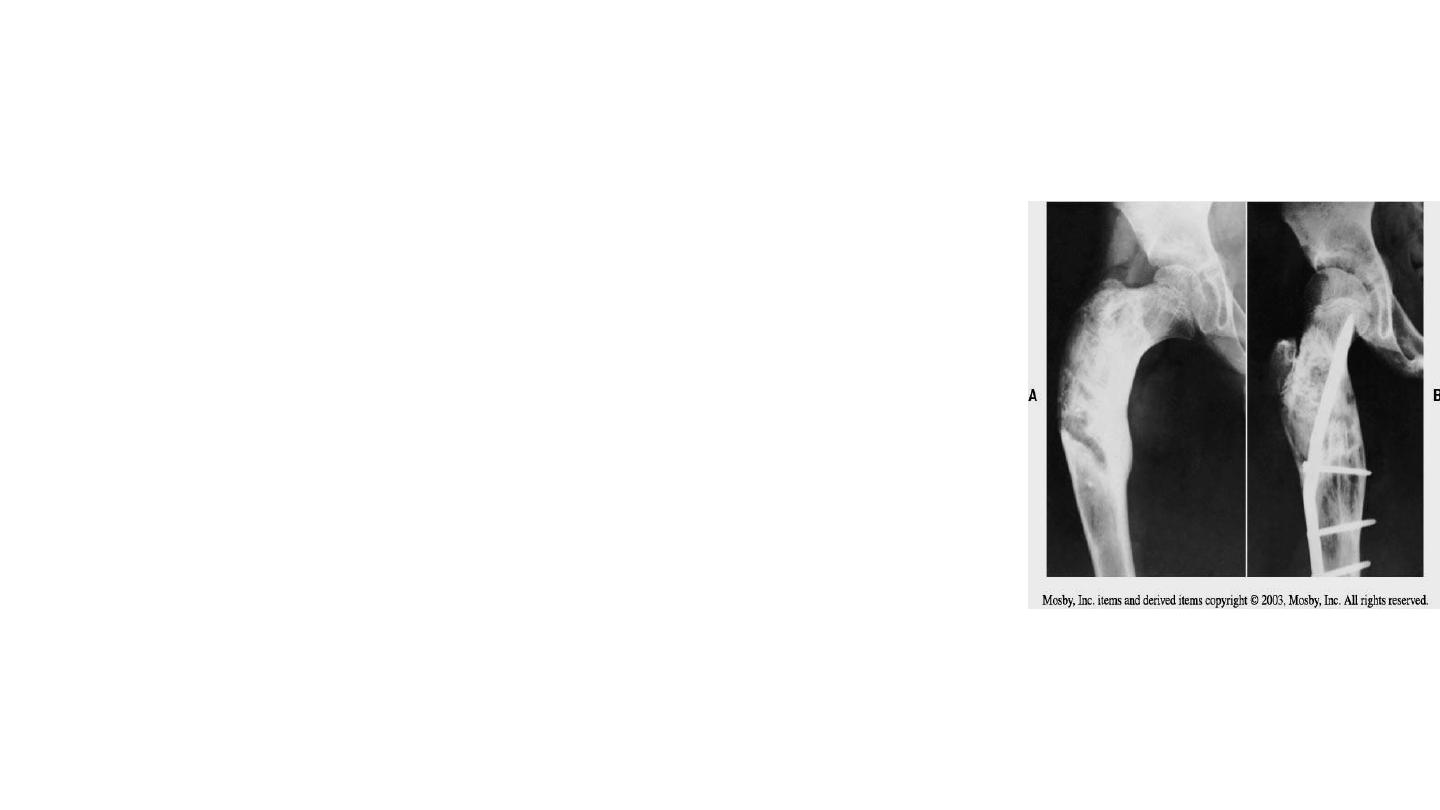
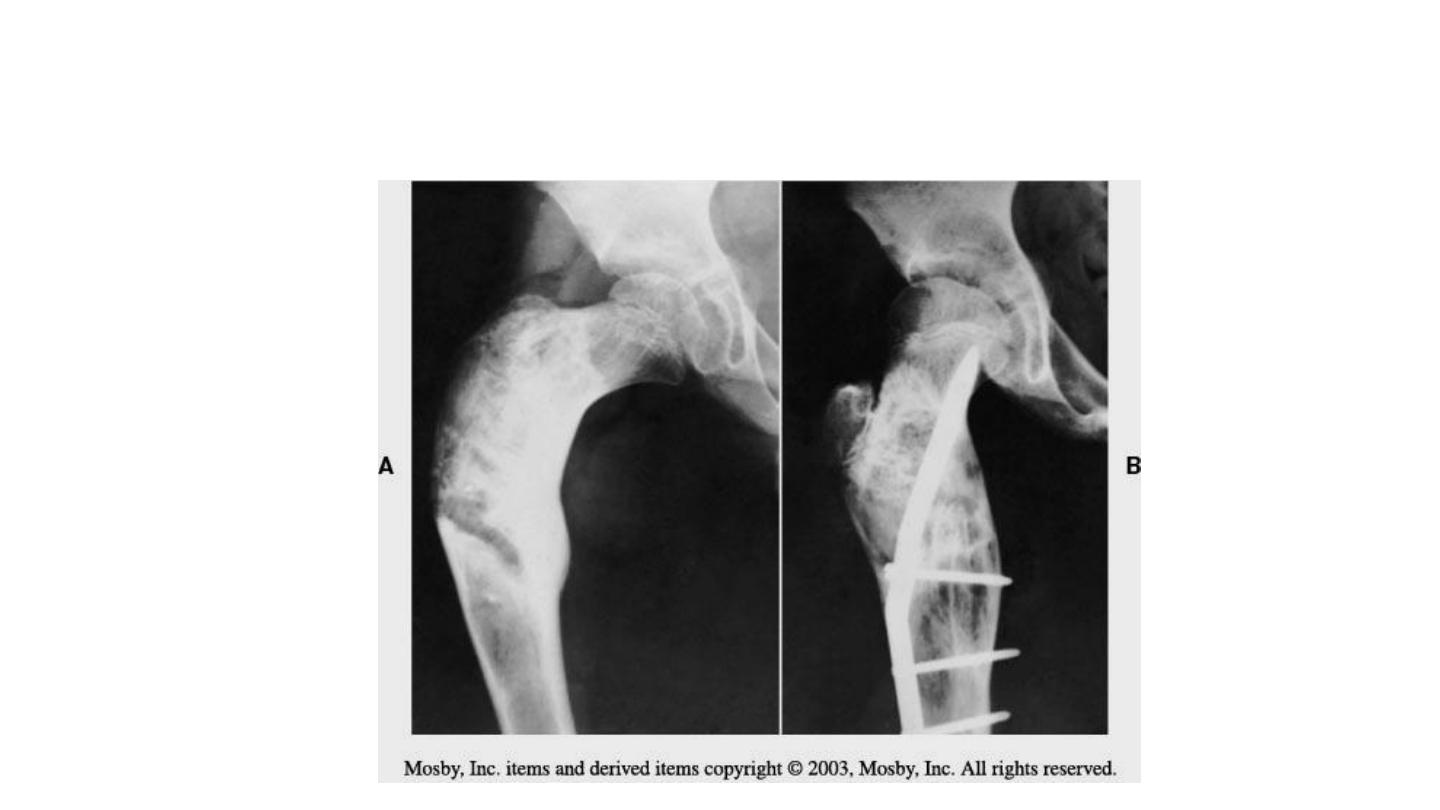
• fibrous dysplasia
- developmental anomaly of bone formation
- the hallmark is replacement of normal bone and
marrow by fibrous tissue and small woven bone
- occurs in any part of bone
- associated abnormalities : sexual precocity- thyroid
disease-abnormal skin pegmentation
- large lesion gives: pain, pathological fracture
- x.ray: fine & granular area [ ground glass ]
- classic sign: shepherd’s crook deformity in prox.
Femur
- biopsy is necessary
- malignant reported
- treatment: curettage & bone grafting
Fibrous dysplasia

• Osteochondroma- cartilage capped exostosis
-the most common of benign tumors; more in
males
-their growth usually stopped when skeletal
maturity is reacted
-clinically: mass or pain
-x-ray: 2 types; stalked & broad based .
Calcification within the cap
-the cap usually thin and thicker should be
studied (secondary chondrosarcoma)
-treatment: surgery in large lesions or produce
symptoms or roentgenographic features
suggest malignancy
-Recurrence is rare
-spontaneous disappearance has been reporteda
Osteochondroma of prox. femur
Cartilaginous tumors
• Multiple osteochondromatosis
-The most striking feature is the presence of
many exostosis
-caused by anomaly of skeletal development
-most regions involved are about the knees ,
ankles and scapula
-surgery indicated to remove painful mass,
improve joint motion and correct
deformity

Cartilaginous tumors
• Chondroma (including enchondroma and periosteal
chondroma)
-chondromas are less common than osteochondromas
-occur third & forth decades located centrally in small
bones of hands and feet
-asymptomatic and seen incidently or after path.
Fracture
-x-ray: low radiolucent appears as well circumscribed
with small foci of calcification
-signs of transformation to malignant tumor is; age > 30
, pain , increasing mass, cortical lysis
-treatment: curettage and bone grfting , periosteal
chondroma should be excised en bloc
After 6 mon… after curt. & bone graf.
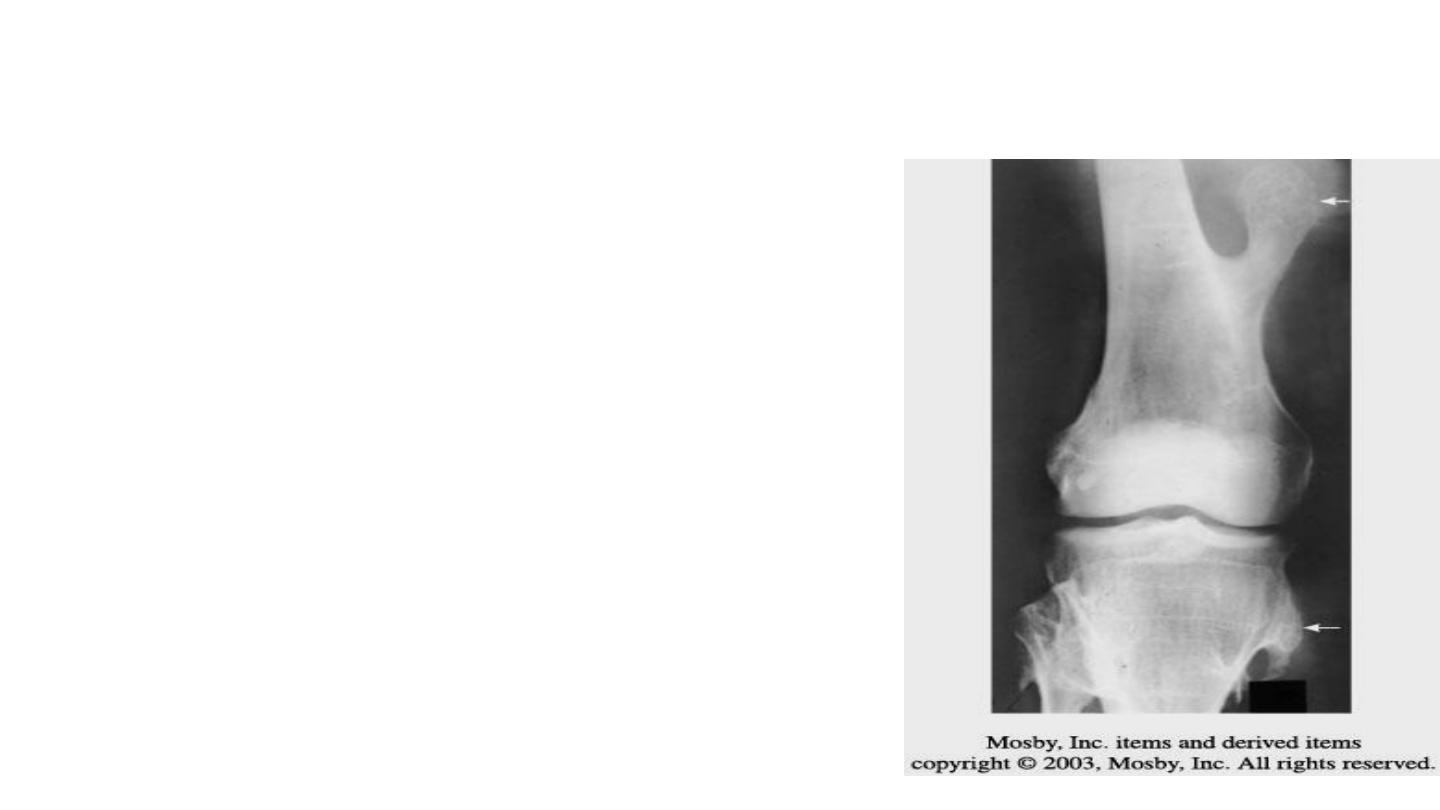
• Gaint cell tumor
-occur in mature long bones(dis. femur & prox. Tibia), in age 20-40
and rarely in adolescent
-located in epiphysis abut subchondral bone
-path. Fractures occur in 10-30%
-x-ray: purely lytic lesion and expands through cortex . Malignant
expands to soft tissues
-MRI; determine the extent of the lesion
-treatment: extended curettage with phenol or argon beam
arthroplasty or aethrodesis may be indicated
=radiation may be used for inoperable lesions(spine , pelvis)
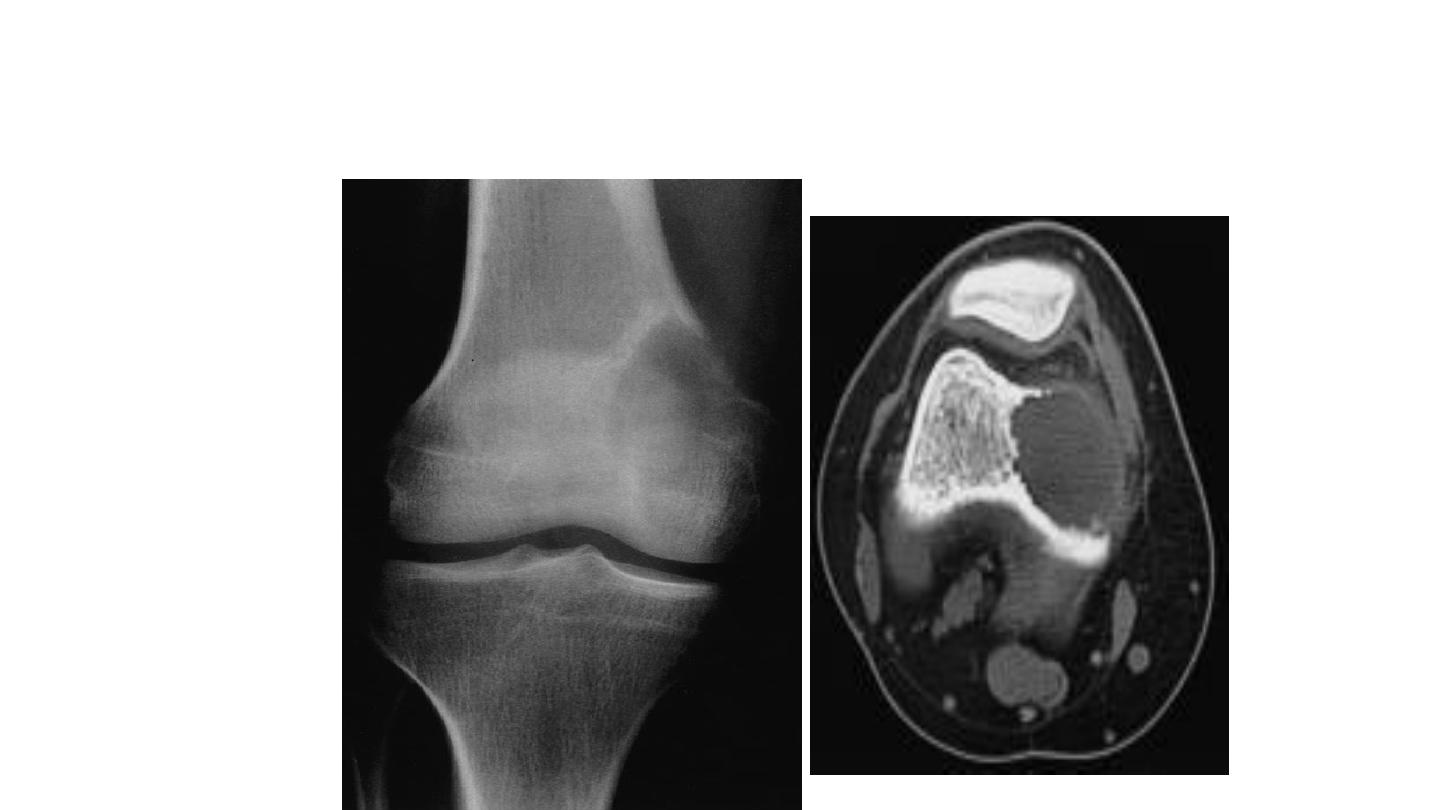
GCT of medial condyle
After curettage and bone cement
Benign(occasionally aggressive) bone tumors
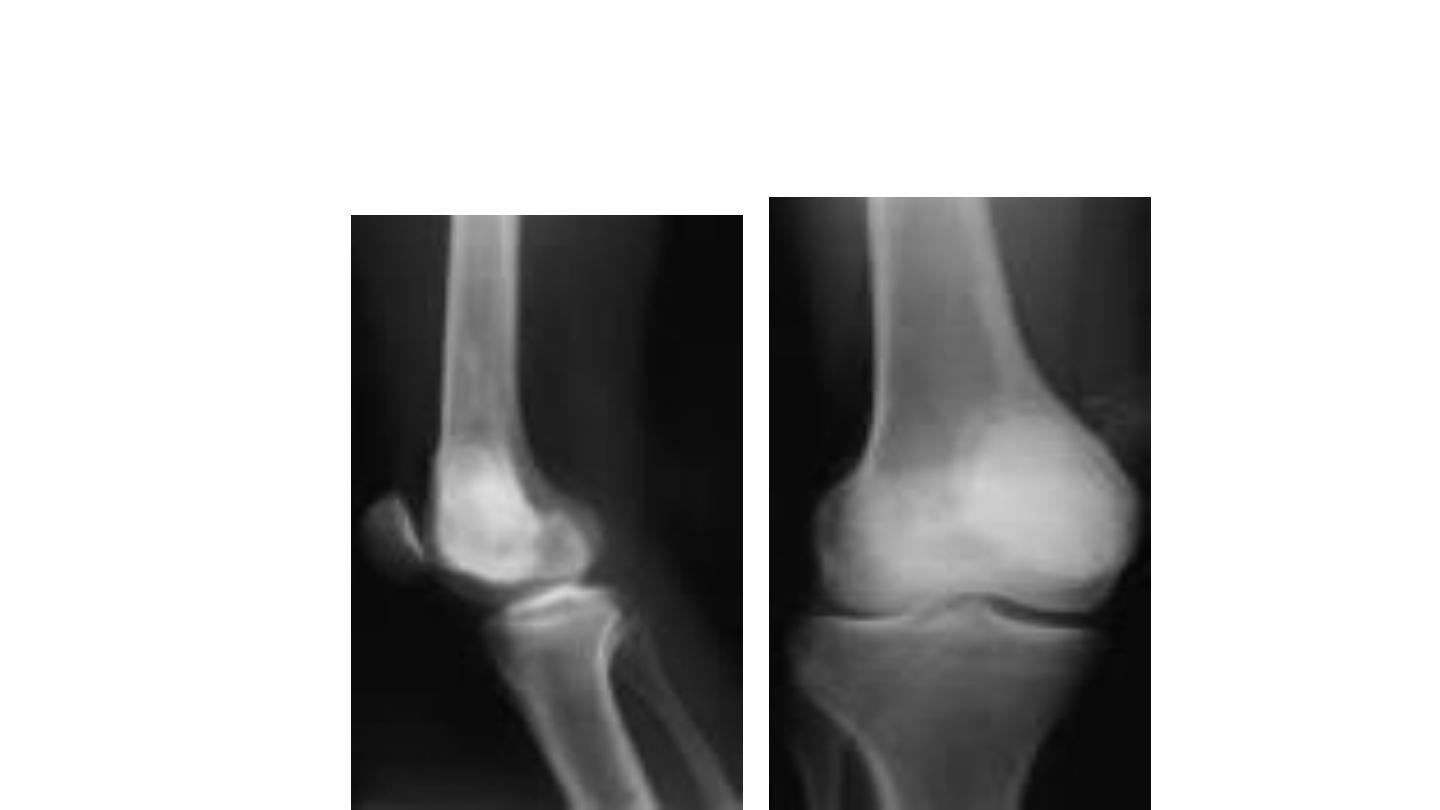
• Chondroblastoma
-rare, typically occur in patients ages, 10-
20y, more in males. Most common sites;
dis. Femur & prox. Tibia
-clinically ; pat. C\O progressive pain that
may mimic a chronic synovitis
-x-ray; well-circumscribed lytic lesion
centered in epiphysis of long bones
surrounding rim bone.
- treatment: extended curettage & bone
grafting or cement
Chondroblastoma in intracondyl notch
Bone-forming tumors
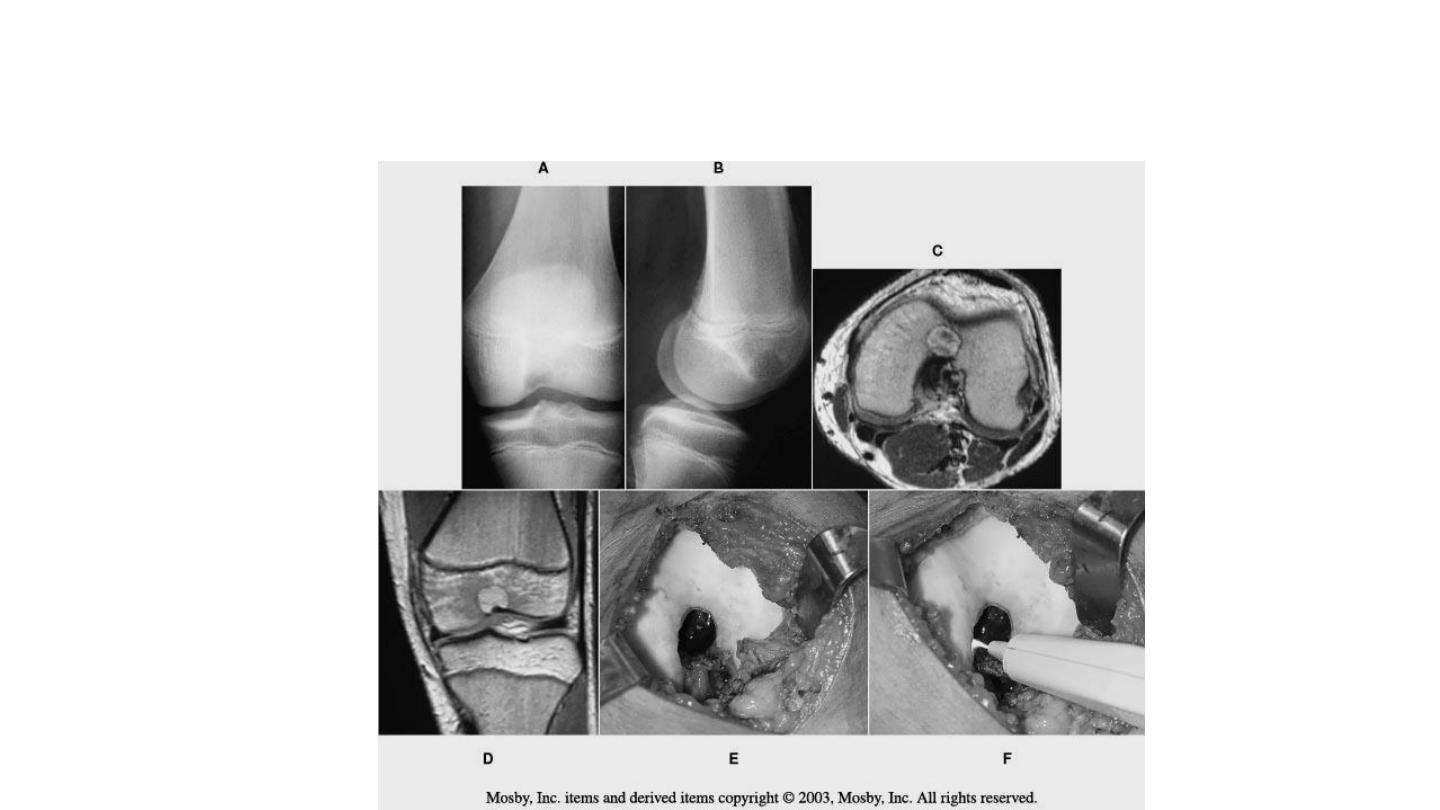
• Osteoid osteoma
-occur in first three decades, often in young
females
-any bone can be involved, 50% the femur
or tibia
-no malignant changes
-pain worse at night and relieved by aspirin
-x-ray: cortical sclerosis and multicentric
fuci . CT, to detect nidus
Treatment: block resection of the nidus
CT-guided percutaneous
resection
-spontaneous disappearance may occur
MALIGNANT BONE TUMORS
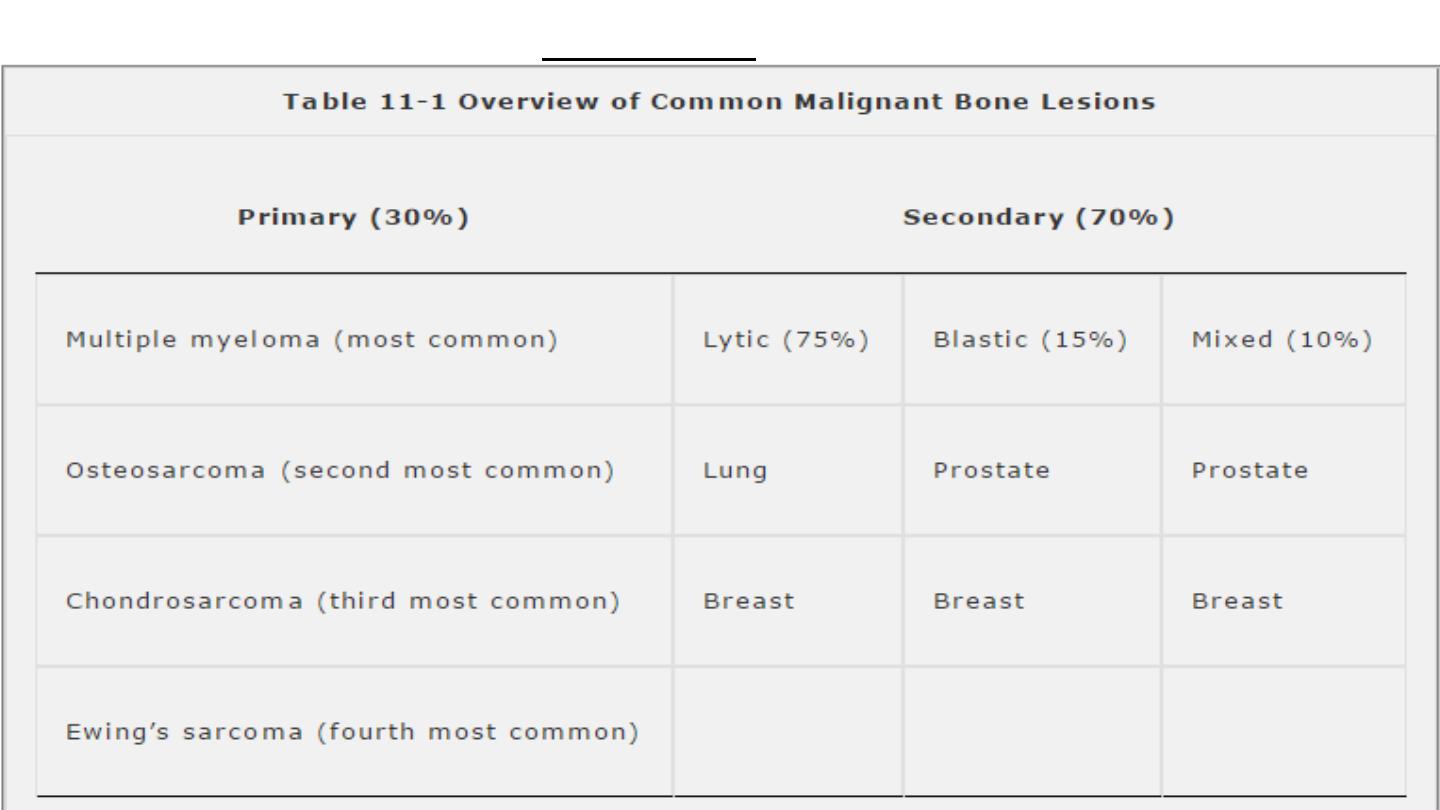
Occurence
Osteosarcoma
Malignant osteoid

Epidemiology
• 3 new cases /1 milion/ year
• 2nd. decade
• Metaphysis of long bones
1/2 in knee region
distal femur
proximal tibia
proximal humerus
Classification
• Primary
• High-grade
–Conventional high-grade (80 – 90%)
»Osteoblastic
»Chondroblastic
»Fibroblastic
• Low-grade
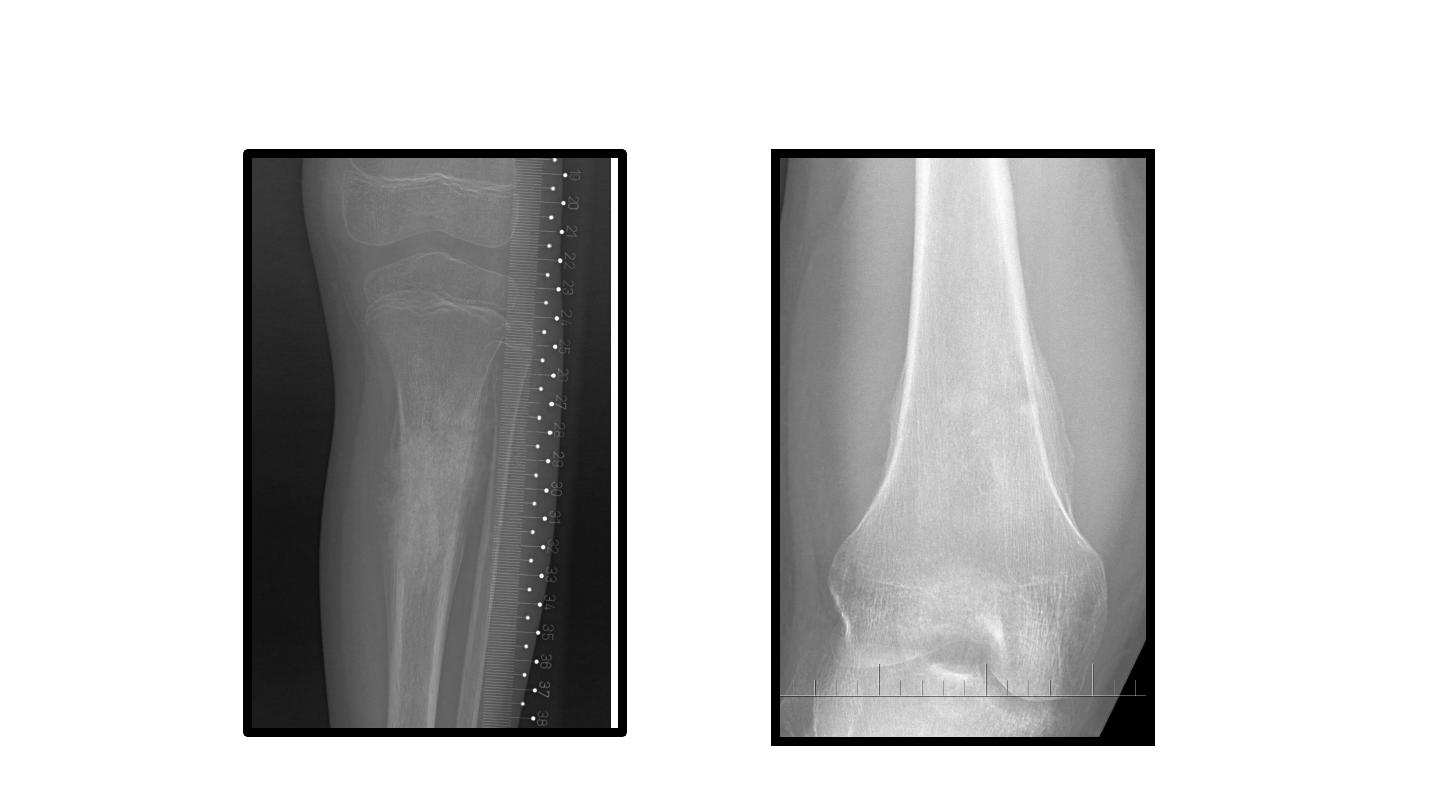
Secondary
- in Paget´s disease of bone
- post radiation

Symptoms
• pain
– during night, in rest
• swelling
• pathological fracture
• metastases in the time of diagnosis
in 10-25 % of patients

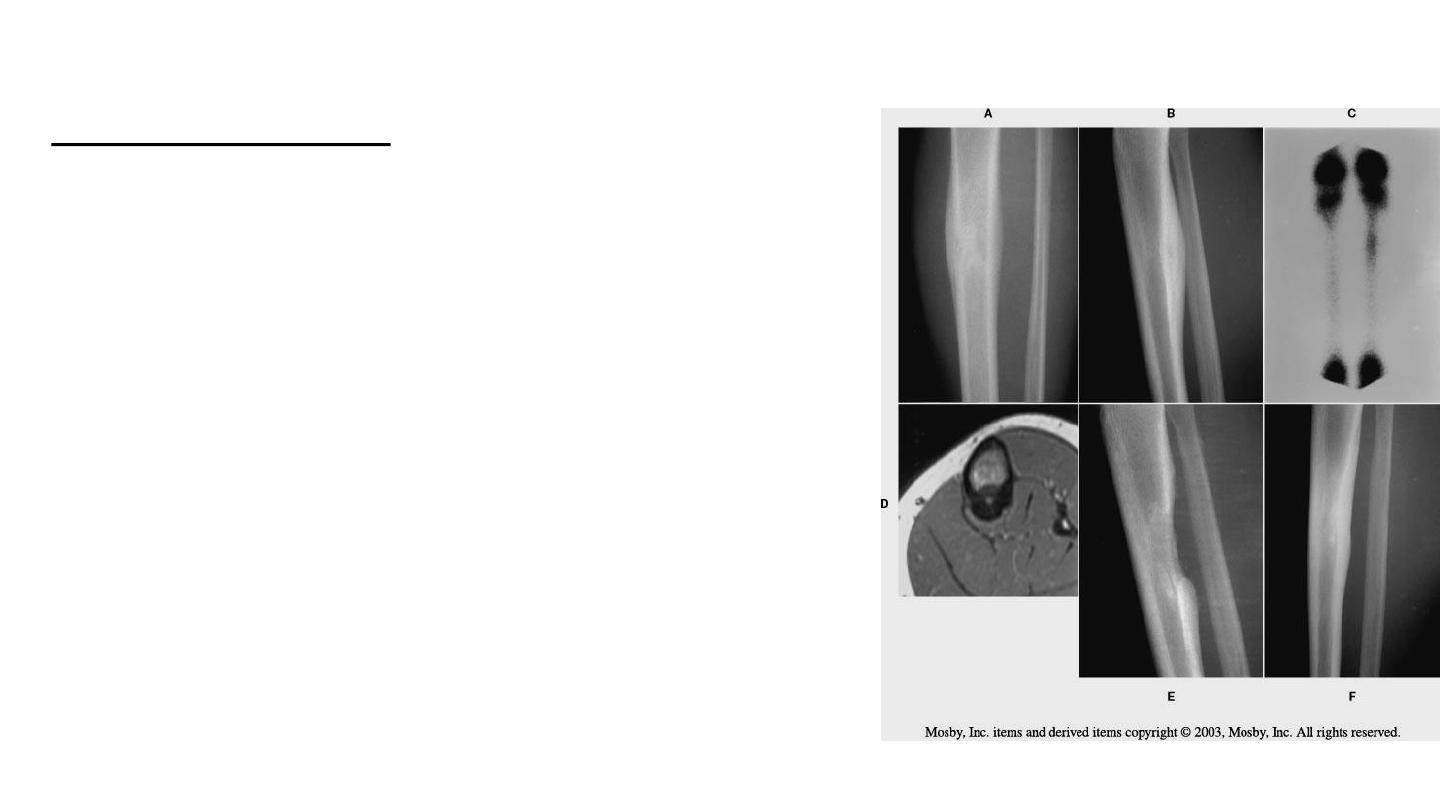
Diagnostics
• X-ray
• CT / MRI
• Scintigraphy
• Chest X- ray or spiral CT
• Ultrasonography
• Biopsy – excisional, needle

Conventional osteosarcoma

Therapy
• neodjuvant chemotherapy
• surgery – radical resection / amputation
• adjuvant chemotherapy
• Metastasectomy in lungs
• In low-grade OSA – only surgical treatment
• OSA is a radioresistant tumor

Prognostic factors
• Metastases
• Size of the tumor
• Axial localisation
• Radicality of surgery
• Response to chemotherapy

Chondrosarcoma

Epidemiology
• 10% of primary malignant bone tumors
• Age:
– primary: 40 – 60 years
– secondary: 25 – 45 years
• Localisation-
pelvis, proximal femur, proximal humerus

Etiology
• Secondary
– Multiple enchondromas (M.Ollier,
Maffucci sy
– Exostosis disease
cartilage over 2 cm
– Chondroblastoma, chondromyxoid fibroma …

Chondrosarcoma

Therapy
• Radical resection – wide resection, amputation
• Chemoresistant tumor
• Radioresistant tumor

Prognosis
• Prognostic factors:
–Radicality of surgery
–Size
–Histological grading
• Prognosis:
–Conventional low-grade 90% 10 years
–Conventional high-grade 20-40% 10 years
–Dediferenciated sarcoma 15% 5 years

Ewing sarcoma family
Group of high grade malignant round cells bone tumors
with neuroectodermal differentiation and specific
translocation.

Epidemiology
• One new case /1 mil./ 1 year
• 5-25 years
• In metaphysis of long bones with extension into diaphysis and
in flat bones (pelvis, scapulla)
Symptoms
• pain
• swelling
• Fever, redness,
• Leucocytosis, ESR elev.
• Biopsy- + identification of specific gene translocation
t(11,22)q(24,12)
Ewing sarcoma

Therapy
• Chemo and radio sensitive tumor
• Neoadjuvant chemotherapy
• Local therapy:
–Radiotherapy
–Wide resection
–Radiotherapy and wide resection

Prognosis
• Response to chemotherapy (systemic disease)
• 5-years survival in 60 % of patients
• Worse prognosis:
– metastases
– Size over 100cm
3
– Surgery not possible
– Axial localisation
– Local recurrence
– Some genetic variants