


Hernias
Dr. Muslim Kandel2019-20
1
Hernias
Lecture one
General features to all types of hernias
Definition
Hernia is a protrusion of the contents of a patient's abdomen (some abdominal organ, part
of his omentum , or his abdominal fat) through an abnormal opening or weak area in the
abdominal walls .
May be external ( through abdominal wall )or intraabdominal ( like hiatus hernia or
through band )The external abdominal hernia is the commonest
Review of Surgical Anatomy
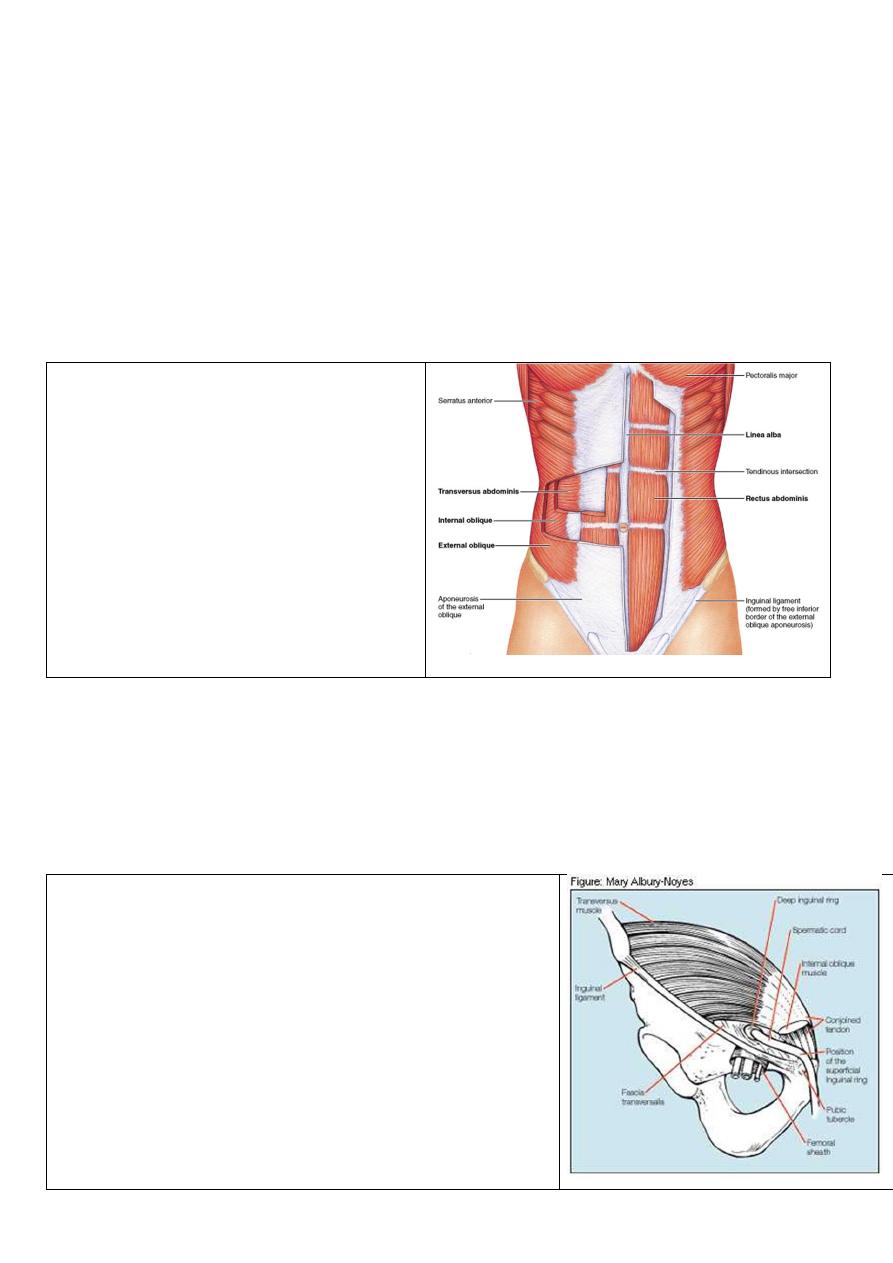
Anatomy of anterior &lateral abdominal wall
Its composed from following layers
1-skin & superfecial facia
2-Abd. Muscles
Tow paramedian
-Rectus abdominus .m
-Pyramidalis m
Three anterolateral flat m
-ext . Abd. Oblique m
- int. Abd. Oblique m
-transversus abd. m
3-facia transversalis ( strong layer )
4-pariatal layer of peritoneum ( form
sac of hernia)
There are weak points at abd wall
that’s more liable to form hernias are:-
1- umbilicus
- scar of umbilical cord in embryo , lies in middle of abd. wall
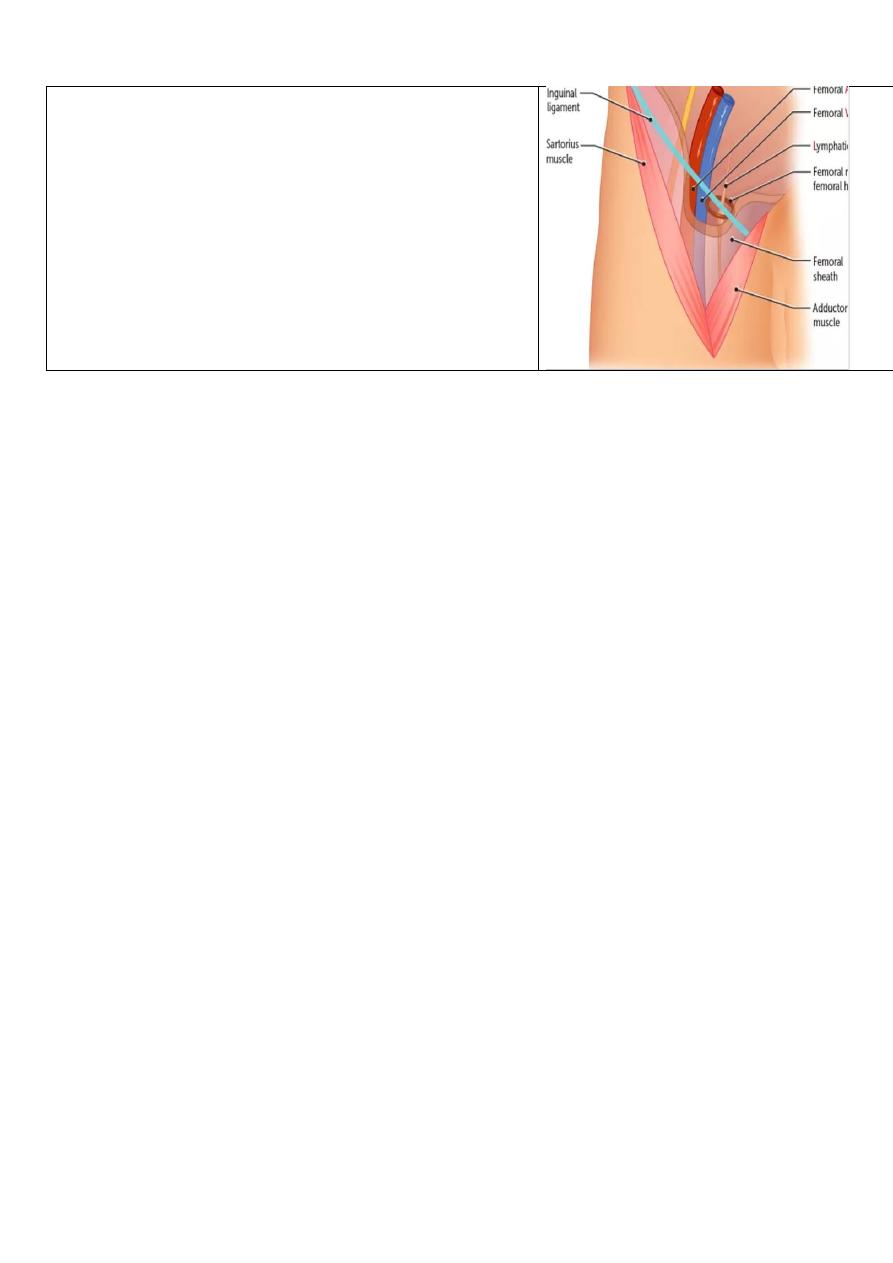
2-inguinal canal
Its oblique intramuscular passage in the lower part of ant. Abd. Wall transmit (
spermatic cord in male or round leg. In female ), lies just above med1\2 if ing.
Ligament about 4 cm length , start from
Deep inguinal ring – is a U-shaped condensation of the
transversalis fascia and it lies 1.25 cm above the inguinal
(Poupart ’ s) ligament, midway between the symphysis
pubis and the anterior superior iliac spine.
Superficial inguinal ring - is a triangular aperture in the
aponeurosis of the external oblique and lies 1.25 cm above
the pubic tubercle
Boundaries of canal:-
Ant. wall of canalext. oblique & fleshy int. oblique
Post.wall of canal facia transversalis
Roof lower arched fiber of int. oblique
Floor inguinal leg
Hernias
Dr. Muslim Kandel2019-20
2
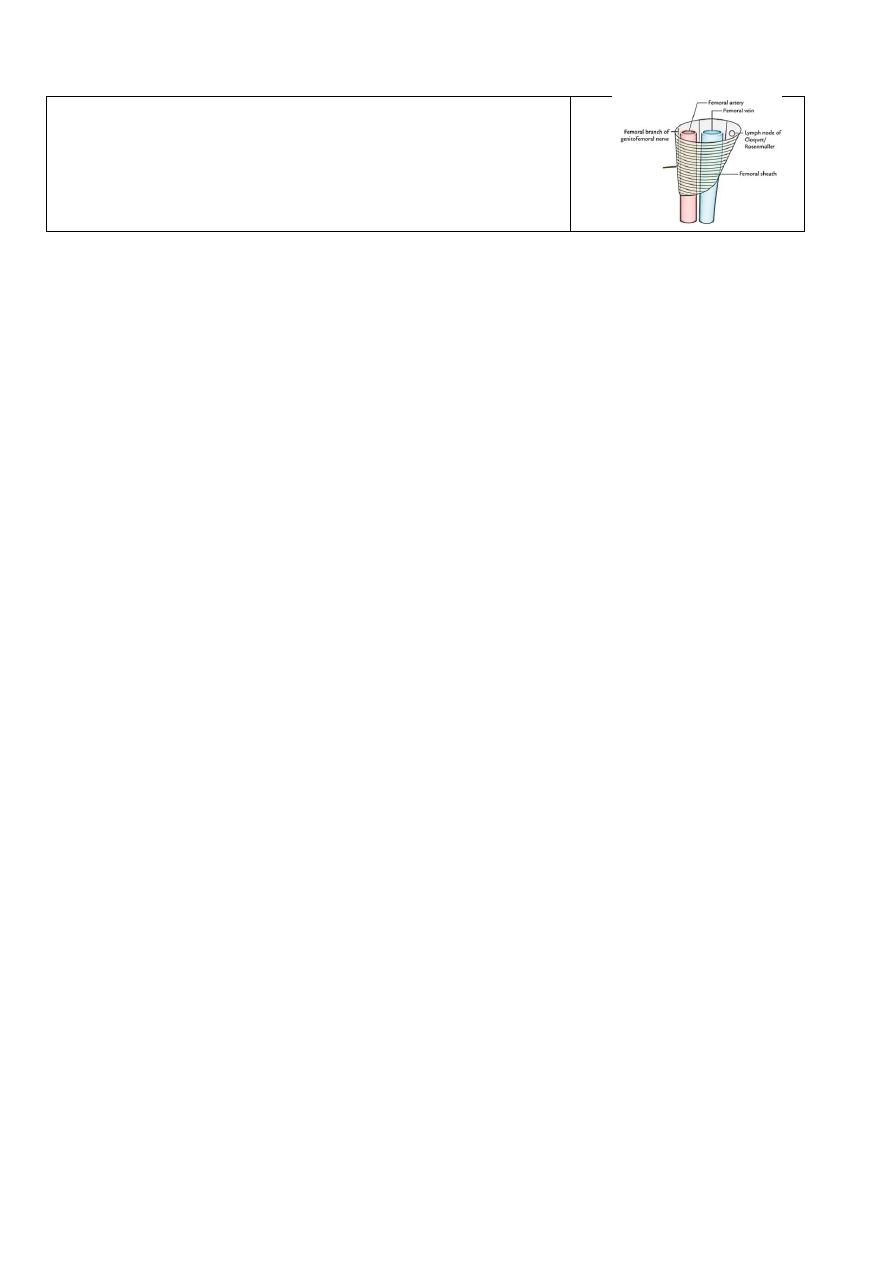
3-The femoral canal & sheath
is formed by a prolongation downward, of the abd.
fascia, behind the inguinal ligament transmit the
structures pass from abd. to L.Limbs
Its divided by two vertical partitions 3 compartments
--lateral contains the femoral artery
--the intermediate the femoral vein,
--the medial and smallest one is named the femoral
canal, and contains some lymphatic vessels
and a lymph gland embedded in a small amount of
areolar tissue
Other weak points in abd. wall
--Hiatus of esophagus. Foramen of Winslow they cause internal hernia .
--Between layers of abd. Wall (arcuate line)
--Iatrogenic :- Surgical incision –Colostomy incisional hernia
General features of Hernias
Aetiology of hernias
a- congenital
undescending testis usually associated with inguinal hernia , An indirect hernia
may occur in a congenital preformed sac — the remains of the processus vaginalis.
b- aquired
1- raises intra-abdominal pressure (ie. Whooping cough is a predisposing cause in
childhood , amongst smokers …)
2- Acquired collagen deficiency increasing an individual ’ s susceptibility to the
development of hernias
3—obesity and pregnancy due to :-
-- Stretching of the abdominal musculature because of an increase in contents,
-- Fat acts to separate muscle bundles and layers, weakens aponeurosis and favours the
appearance of paraumbilical, direct inguinal and hiatus hernias.
--A femoral hernia is rare in nulliparous women and men, but more common in
multiparous women owing to stretching of the pelvic ligaments.
4-after surgical operation(incisional hernia) wound is weakest area in abdominal
wall
Composition of a hernia .
1-The sac
The sac is a diverticulum of peritoneum consisting of mouth, neck, body and fundus.
The body of the sac varies greatly in size and thickness in childhood the sac is very thin.
In long-standing cases the wall of the sac may be comparatively thick.
2-The covering s are derived from the layers of the abdominal wall through which the sac
passes. In long-standing cases they become atrophied from stretching and so amalgamated
that they are indistinguishable from each other.
3-Contents
Commonly either omentum = omentocele (epiplocele);
Hernias
Dr. Muslim Kandel2019-20
3
Or intestine = enterocele. More commonly small bowel, but may be large intestine or
appendix; Sometimes a portion of the circumference of the intestine Richter ’ s hernia;
But other structures like ur. bladder, fallopian tube ….may be but rare
What's happen inside hernia?
Usually hernia is reducible either spontenously during supine position or reduce by
patent himself , but sometimes may become
1- Irreducible hernia ( especially when omentum ) .
2- Obstructed hernia (especially when bowel )
3-Strangulated hernia
especially when blood vessels that supply contents are blocked)
4-inflamed hernia
when the contents superadded by infection either from
- from inflammation of the contents of the sac (e.g. acute appendicitis or salpingitis)
-or from external causes (e.g. the trophic ulcers which develop in the dependent areas of
large umbilical or incisional hernias).
Pathology.
--In reducible hernia the content not adherent sac so reduce easy to abdominal cavity
-- The irreducible hernia due to adhesion of omentum inside sac or over crowded
of he contents so that difficult to reduce contant
-- Obstructed and strangulated hernia
if bowel inter sac may cause intestinal obstruction
Initially, only the venous return is impeded so the wall of the intestine becoming
congested and bright red with the transudation of serous fluid into the sac ,with time
congestion will increases The intestinal pressure increases distending the intestinal loop
gradually the arterial supply becomes more and more impaired.-, part of blood is
extravasated ( The fluid in the sac becomes blood stained, that sign of impaired blood
supply and beginning of gangrene ), Bacterial transudation occurs secondary to the
lowered intestine viability and the sac fluid becomes infected
--
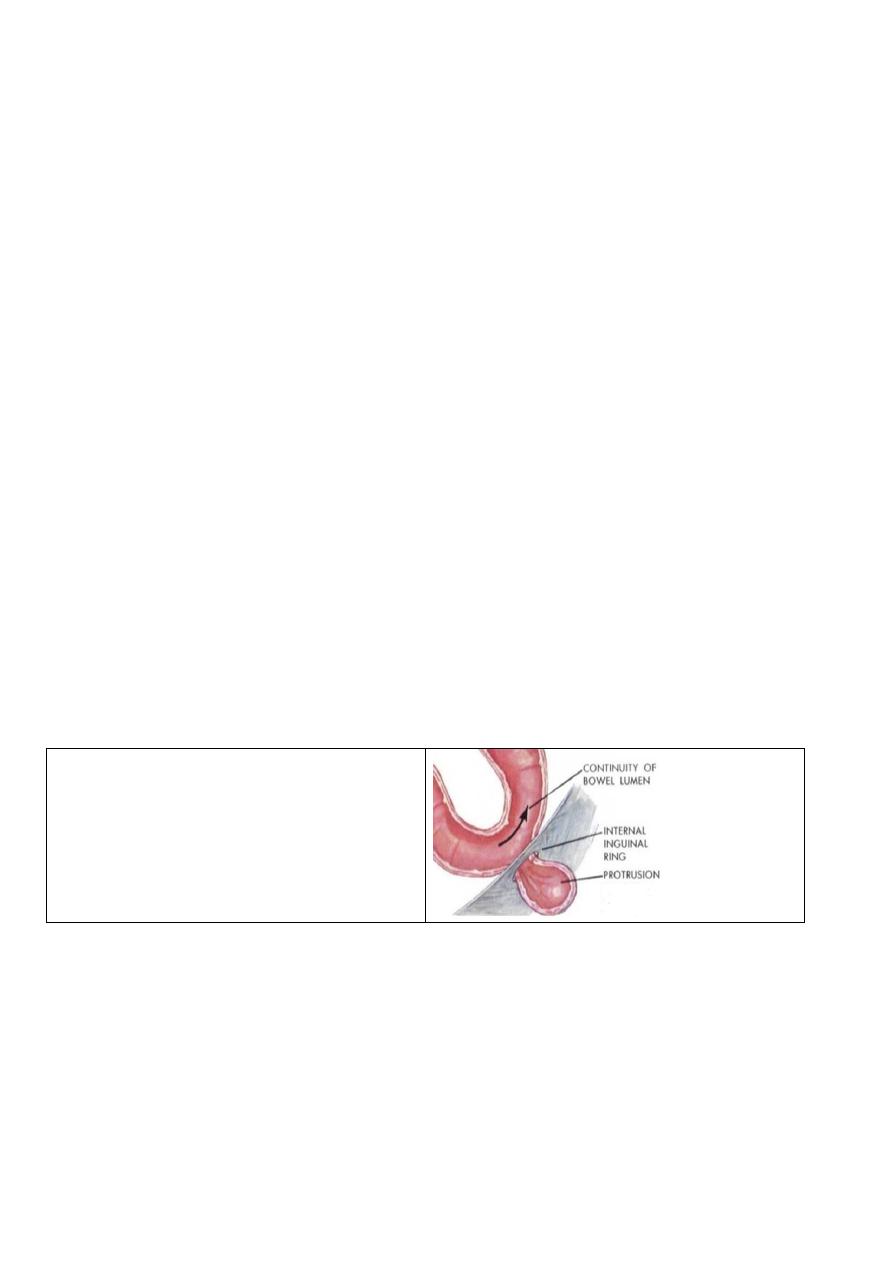
Richter ’ s hernia
-
is a hernia in which the sac contains only
a portion of the circumference of the
intestine (usually small intestine). It
usually complicates femoral and, rarely,
obturator hernias
Clinical features.
--in non obstructed
--cough impulse.
-- In large hernias there is a sensation of weight, and dragging on the mesentery may
produce epigastric pain.
-- In infants the swelling appears when the child cries.
--in obstructed
--signs of intestinal obstruction ,Sudden pain at first situated over the hernia is followed
by generalised abdominal pain, colicky in character and often located mainly at the
umbilicus. Nausea and subsequently vomiting ensue. The patient may complain of an
increase in hernia size.
Hernias
Dr. Muslim Kandel2019-20
4
--On examination, the hernia is tense, extremely tender and irreducible, and there is no
expansile cough impulse.
-- Spontaneous cessation of pain must be viewed with caution as this may be a sign of
perforation
common hernias
75% inguinal region 5 –20% incisional 10% umbilical and epigastric 5%femoral
Lecture two
types of abdominal wall hernias
Groin hernias (inguinal, femoral
)
1-Inguinal hernia
The indirect inguinal hernia, the most common form of groin hernia across all ages and
both genders
,
etiology behind the indirect inguinal hernia is believed to be a patent
processus vaginalis,
A- Indirect (oblique) inguinal hernia
It is most common in the young, whereas a direct hernia is most common in the old. In
the first decade of life inguinal hernia is more common on the right side in the male. males
are 20 times more commonly affected than females This is no doubt associated with the
later descent of the right testis and a higher incidence of failure of closure of the processus
vaginalis. In adult males, 65 per cent of inguinal hernias are indirect and 55 per cent are
right-sided. The hernia is bilateral in 12 per cent of cases .
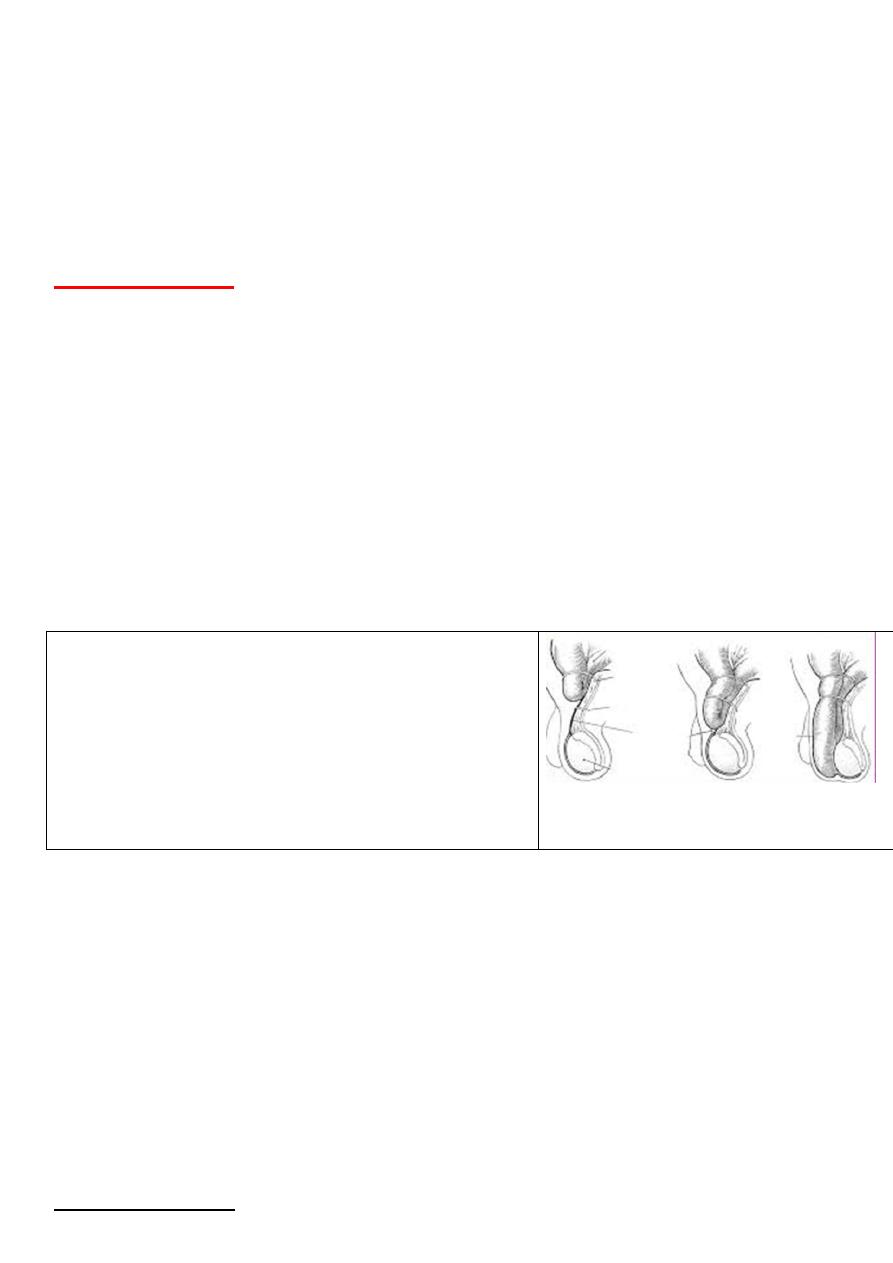
Three types of indirect inguinal hernia occur
1-Bubonocele
When the hernias limited to the inguinal canal
2- Funicular the processus vaginalis is closed just
above the epididymis the content of the sac can be felt
separately from the testis, which lies below the hernia
3-Complete (scrotal) — a complete inguinal hernia is
rarely present at birth but is commonly encountered in
infancy
Differential diagnosis
The presentation of inguinal hernia either groin mass or scrotal swelling
Groin mass
• an encysted hydrocele of the cord;
(move with pulling down of testis )
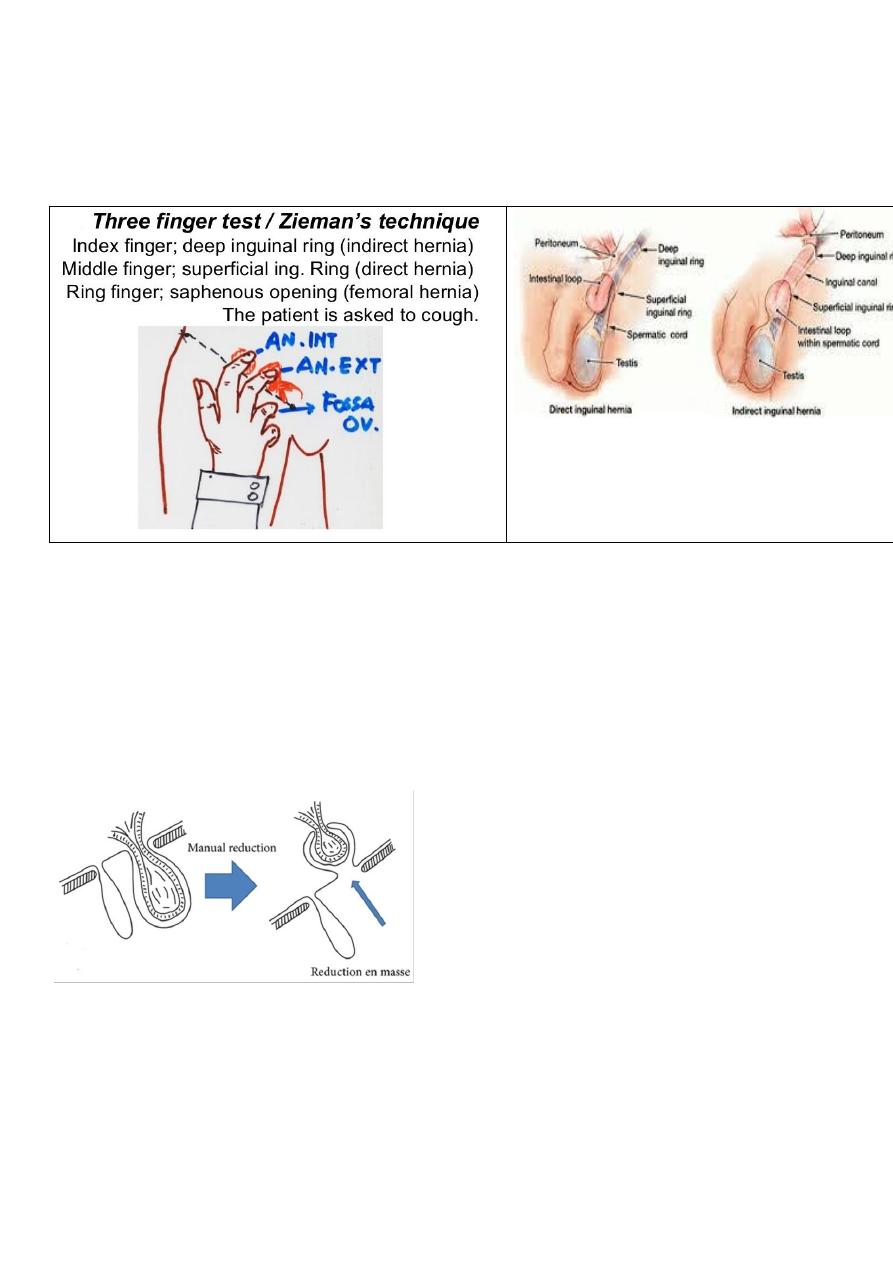
• a femoral hernia; ( 3 finger test Zeimen test
• an incompletely descended testis; ( empty testis )
• a lipoma of the cord
• LN.
Scrotal swelling
• hydrocele -- (can get above it. , trnslumination )
• spermatocele;
Treatment of indirect inguinal hernia
1) Operative treatment. Which is treatment of choice
A- Open technique which is traditional treatment . done under local, epidural or spinal,
as well as general, anesthesia
Hernias
Dr. Muslim Kandel2019-20
5
- in children until age 16years use herniotomy only . This is dissecting out and
opening the hernial sac, reducing any contents, and then transfixing the neck of the sac and
removing the remainder.
- in in adult Herniotomy and repair (herniorrhaphy).
suturing between inguinal lig & conjoin tendon by many methodes(Bassini, Darning , Shouldice
mesh inserted between inguinal lig & conjoin tendon (tension free)
laparoscopic repair
-
B
In the laparoscopic approach uses mesh to repair the hernia defect in a plane posterior to the defect
1-Totally Extraperitoneal(TEP)
an inflatable balloon is placed in the preperitoneal space, and the repair is done preperitoneal. More skill
required
.
2-Trans-abdominal Preperitoneal(TAPP)
*** whereas the open approaches repair the hernia anterior to the defect.
Complication of operation:-
1- recurrence it is often secondary to deep infection, undue tension on the repair, or tissue ischemia.
2-infection , stitch abscess &sinus
3 Postoperative groin pain, or neuralgia due to (nerve injury)
4- urine retention
5 Testicular swelling and atrophy (ischemic orchitis )thrombosiss of pampiniform plexus
6- Injury to the vas is a rare complication
7-secondary hydrocele
2- non operative
may be used when operation is contraindicated or when operation is refused
1-A truss. provides support for the herniated area, using a
pad and belt ,Used in old age or who unfit for operation.
2-gallow ’ s traction
only indicated in infants. The child is given analgesia and
placed in gallow ’ s traction In 75 % of cases reduction is
effected and there appears to be no danger of gangrenous
intestine being reduced
B-Direct inguinal hernia
In adult males, 35 % of inguinal hernias are direct. At presentation, 12 % of patients will
have a contralateral hernia , there is a four-fold increased risk of future development of
contralateral hernia.
--The sac passes through a weakness or defect of the transversalis fascia in the posterior
wall of the inguinal canal
-- Predisposing factors are :-
1-smoking,chr. Chest inf , prostate hypertrophy causes increase intraabd. pressure
2-occupations that involve straining and heavy lifting.
3-Damage to the ilioinguinal nerve (previous appendicectomy) due to resulting
weakness of the conjoined tendon.
Hernias
Dr. Muslim Kandel2019-20
6
Diffrentiate from indirect inguinal hernia
-- A direct inguinal hernia is always acquired.
-- Direct hernias do not often attain a large size or descend into the scrotum).
-- lies behind the spermatic cord.
--the neck of the sac is wide, direct inguinal hernias do not often strangulate.
-- 3 finger test (Zeimman test)
Treatment
same as indirect hernia
manual reduction of hernial content :
should be done softly with sedation , the vigorous manipulation (taxis) has no place in
modern surgery Its dangers include:
• contusion or rupture of the intestinal wall;
bowel contents go into peritoneum cause peritonitis
the sac may rupture at its neck and the contents are reduced, not into the peritoneal
cavity but extraperitoneally
• reduction-en-masse: ‘ The sac together with its contents is pushed forcibly back into the
abdomen; as the bowel will still be strangulated by the neck of the sac, the symptoms are in
Special forms of inguinal hernia
1- prevesical hernia.
The prevesical fat and a portion of the bladder that protrudes through a small oval defect
in the medial part of the conjoined muscle just above the pubic tubercle. It occurs
principally in elderly males and occasionally becomes strangulated.
Hernias
Dr. Muslim Kandel2019-20
7
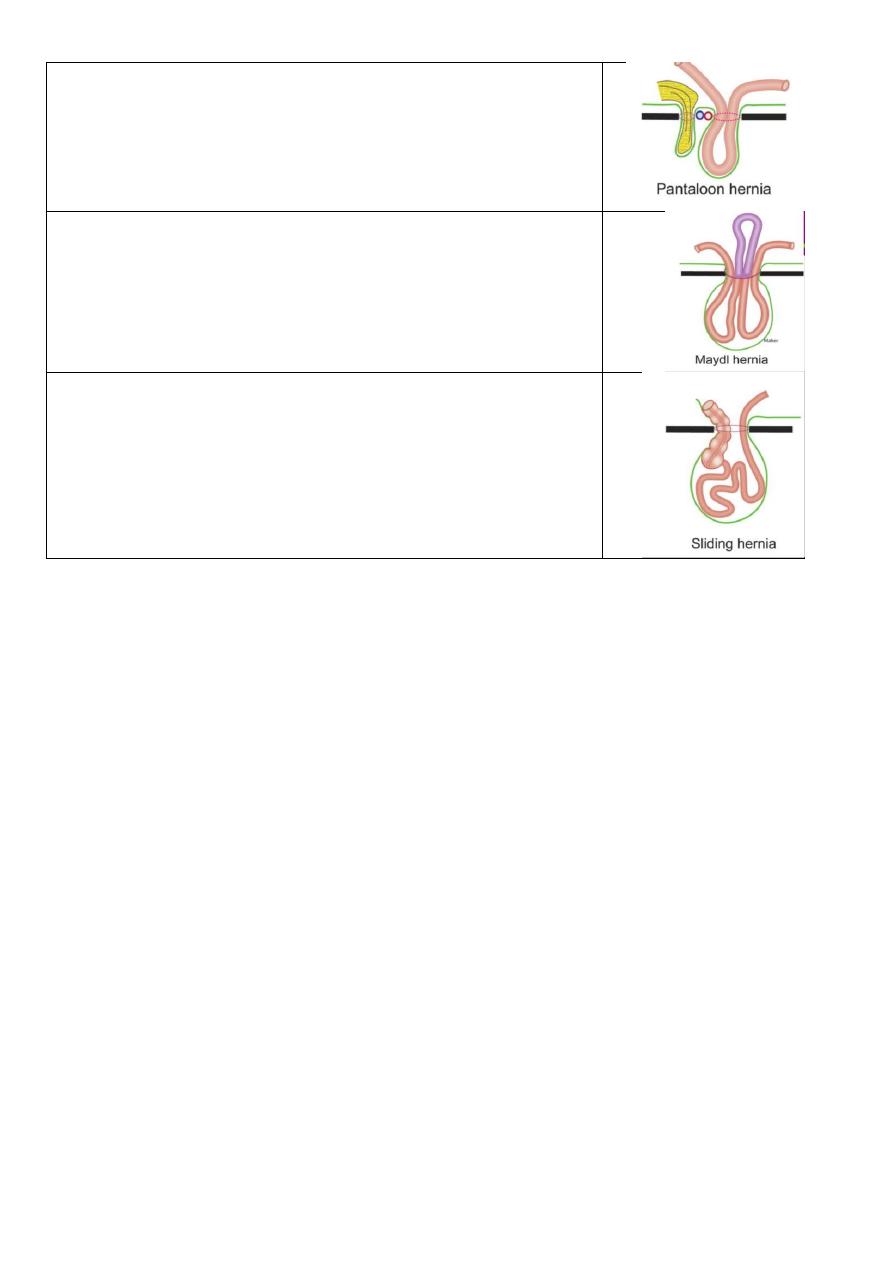
2-Dual (saddle bag; pantaloon) hernia. This type of hernia
consists of two sacs which straddle the inferior epigastric
artery, one sac being medial and the other lateral to this vessel.
The condition is not rare and is a cause of recurrence, one of the
sacs having been overlooked at the time of operation.
3- Maydl ’ s hernia (syn. hernia-in-W).
Maydl ’ s hernia is rare. The strangulated loop of the W lies
within the abdomen, thus local tenderness over the herniais not
marked
4-Sliding hernia
As a result of slipping of the posterior parietal peritoneum on
the underlying retroperitoneal structures, the sigmoid colon, the
caecum , portion of the bladder
Strangulated inguinal hernia
occurs at any time during life and in both sexes. Sometimes a hernia strangulates on the
first occasion that it descends; but commonly occur in:-
--Indirect inguinal hernias, the direct variety is less due to the wide neck of the sac.
-- in patients who have use a truss for a long time,
-- in those with a partially reducible or irreducible hernia.
Usually, the small intestine is involved in the strangulation; the next most frequent is the
omentum; sometimes both are involved. It is rare for the large intestine to become
strangulated in an inguinal hernia, even when the hernia is of the sliding variety.
Treatment of strangulated inguinal hernia
(The danger is in the delay not in the operation)
*preoperation = Vigorous resuscitation with intravenous fluids, nasogastric aspiration ,
antibiotics , catheterisation.
* operation= An incision is made over the most prominent part of the swelling.
- Devitalised omentum is excised after being securely ligated.
- gangrenous intestine is excised by localised resection with end to end anastomosis
- Viable intestine is returned to the peritoneal cavity.
- Doubtfully viable bowel , use warm moist back with 100% O2 for 5 min then re
check viability of bowel
if viable bowel returned back if devitelized excise .
-prosthetic mesh is best avoided
Hernias
Dr. Muslim Kandel2019-20
8
2-Femoral hernia
Femoral hernia is the third most common type of primary
hernia. It accounts for about 20 per cent of hernias in
women and 5 per cent in men.
Clinical features.
Femoral hernia is rare before puberty. Between 20 and 40 years of age the prevalence rises
and continues to old age. The right side is affected twice as often as the left, and in 20 per
cent of cases the condition is bilateral.
The femoral hernia often presents as a small bulge just below the medial groin crease. It is
often difficult to reduce on initial presentation
The symptoms to which a femoral hernia gives rise are less pronounced than those of an
inguinal hernia; may be unnoticed by the patient for years, perhaps until the day it
strangulates. Adherence of the greater omentum sometimes causes a dragging pain. Rarely,
a large sac is present.
Differential diagnosis.
1-An inguinal hernia ( 3 finger test Zeimman )
2-A saphena varix. (Associate with varicosity of long saphenous vein)
3- An enlarged femoral lymph node .(other enlarged lymph nodes to aid the diagnosis. )
4-Lipoma.
5-A femoral aneurysm ( pulsatile )
6-. A psoas abscess ( TB lumber vertebrate )
7-A distended psoas bursa. (The swelling diminishes when the hip is flexed and
osteoarthritis of the hip is present. )
Strangulated femoral hernia
A femoral hernia strangulates frequently and gangrene rapidly develops. This is
explained by the narrow, unyielding femoral ring. In 40 % of cases the obstructing
agent is not the lacunar ligament but the neck of the femoral sac itself.
A Richter ’ s hernia is a frequent occurrence
Treatment of a femoral hernia.
A truss is contraindicated , only open surgery. There are many approaches
-- the low operation below the inguinal ligament via a groin-crease incision,
-- the high operation vertical incision to deal with both femoral& inguinal hernias
In all cases the open sac reduce healthy contents to abdomen (herniotomy) then
herniorrhaphy by suturing inguinal ligament with iliopectenial fascia . or
insertion polypropylene mesh.
Hernias
Dr. Muslim Kandel2019-20
9
Lecture three
Umbilical hernias
1-
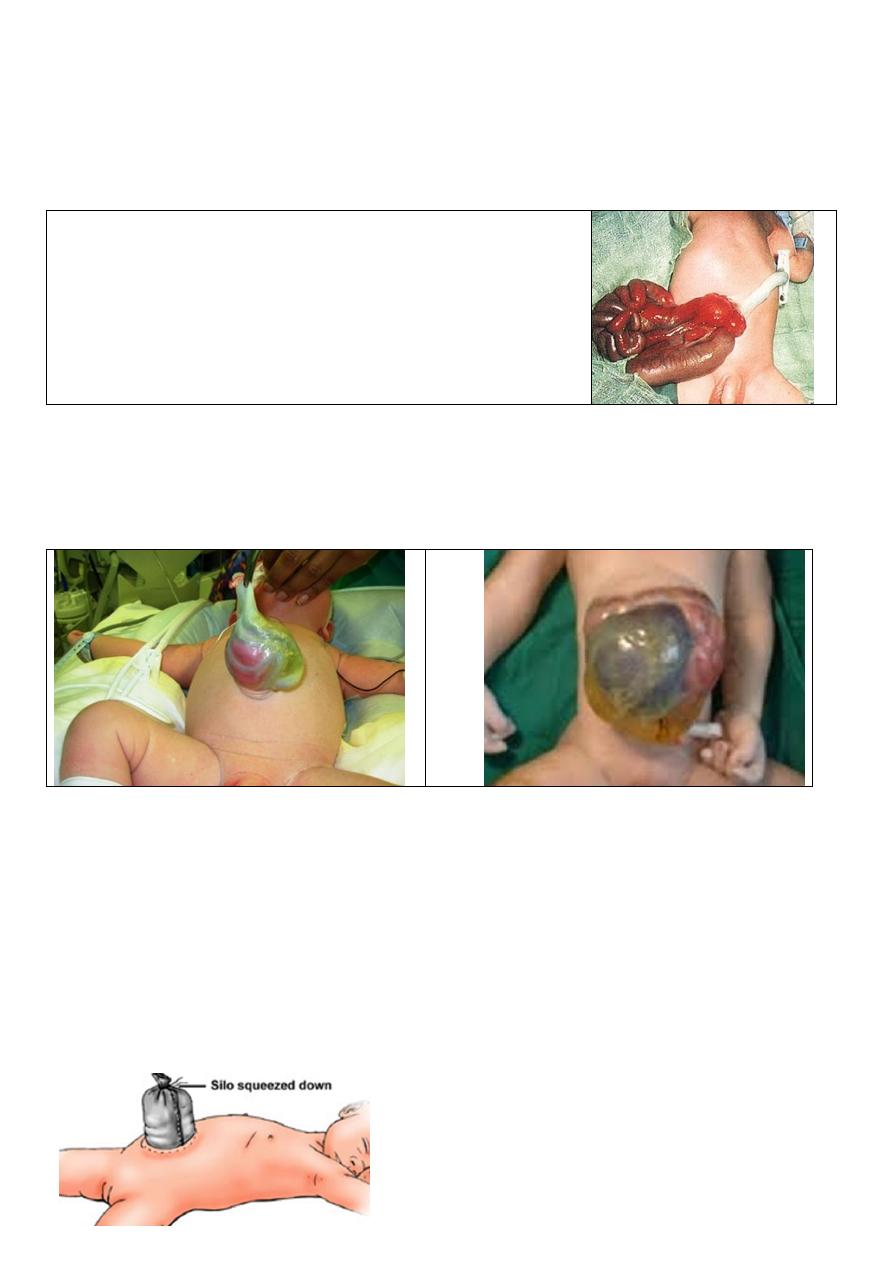
Exomphalos
(omphalocele and gastroschisis)
occurs once in every 6000 births; it is due to failure of all or part of the midgut to return to
the coelom during early foetal life.
gastroschisis :-when the sac ruptuered during labour or
after lead to appearance of bowel out of abdomen
Omphalocele When the sac remains unruptured, it is
semitranslucent and, although very thin, it consists of two
layers — an outer layer of amniotic membrane and an inner
layer of peritoneum.,
Omphaloceles may be divided into
Omphaloceles minor those with a fascial defect of less than 4cm
Omphaloceles major those with a fascial defect of greater than 4 cm.
In large defects the liver, spleen, stomach, pancreas, colon or bladder may be seen
through the membrane. The intestine lies freely mobile within the intact sac without
evidence of adhesions or inflammation.
Omphaloceles minor Omphaloceles major
Treatment
-- Small defects may be closed primarily soon after birth
-- Large defects, the difficulty is disproportion between the size of the abdominal cavity
and the volume of the sac contents.
a- Operative therapy many operatios :- skin flap closure, staged closure ( silo), and
primary closure
b-Nonoperative therapy:- is appropriate for premature infants with a gigantic intact sac or
associated anomalies make survival of a major operation unlikely. The intact sac is painted
daily with a desiccating antiseptic solution and, if successful, an eschar forms over the sac.
Eventually granulisation grows in from the periphery and the subsequent ventral hernia can
be repaired later.
Hernias
Dr. Muslim Kandel2019-20
10
2-Congenital umbilical hernias
a- Umbilical hernia of infants and children
This is a hernia through a weak umbilicus which may partially result from failure of the
round ligament (obliterated umbilical vein) to cross the umbilical ring and partially from
absence of the Richet fascia.
-- Both sexes seem to be equally affected, although
--the incidence in black infants eight times higher than in white infants.
--The hernia is often symptomless but increases in size on crying
Obstruction or strangulation below the age of 3 years is extremely uncommon
Treatment.
Conservative treatment is indicated under the age of 2 years. 95 per cent of hernias will
disappear spontaneously. herniorrhaphy is indicate If the hernia persists at 2 years of age d
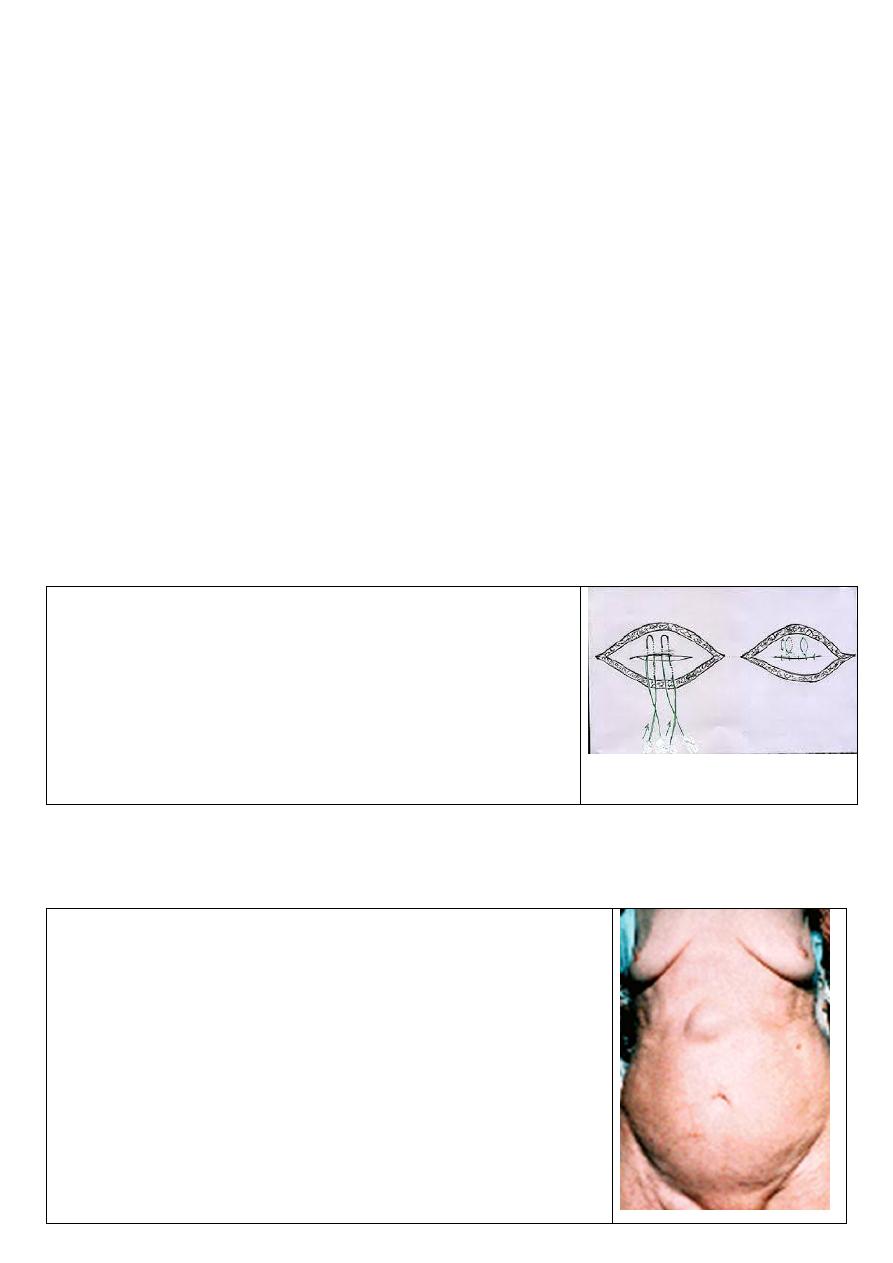
b- Paraumbilical hernia (supraumbilical or infraumbilical hernia)
In adults the hernia does not occur through the umbilical scar. It is a protrusion through
the linea alba just above or sometimes just below the umbilicus
-- Paraumbilical hernias can become very large..
-- Women are affected five times more frequently than men.
-- common in overweight women specially after pregnency, of 35 and 50 years.
Treatment.
1-- If the defect is small, a primary herniorrhaphy can be performed.
2 - If the defect is large, the repair is:-The classic primary
repair is ( Mayo s operation). The aponeurosis on both sides
overlap of 5 or 7.5 cm. Interrupted mattress sutures are then
inserted into the aponeurosis,
3- In the case of very large primary para-umbilical hernias
(fascial defect > 4 cm) or for recurrent paraumbilical hernias,
the use of prosthetic material (polypropylene mesh) is
recommended.
- Additional lipectomy if large fatty abdomen.
Epigastric hernia
(fatty hernia of the linea alba)
An epigastric hernia occurs through the linea alba anywhere between the xiphoid process
and the umbilicus, usually midway between these structures. Such a hernia commences as
a protrusion of extraperitoneal fat through the linea alba
. More than one hernia may be present and the commonest cause
of ‘ recurrence ’ is failure to identify a second defect at the time
of original repair. A swelling the size of a pea consists of a
protrusion of extraperitoneal fat only (fatty hernia of the linea
alba).
The mouth of the hernia is rarely large enough to permit a
portion of hollow viscus to enter it;
The patients are often manual workers between 30 and45 years
of age. Usually Symptomless
Treatment
legating the pedicle, the small opening in the linea alba is closed
by nonabsorbable sutures in adults and with absorbable sutures
in children.
Hernias
Dr. Muslim Kandel2019-20
11
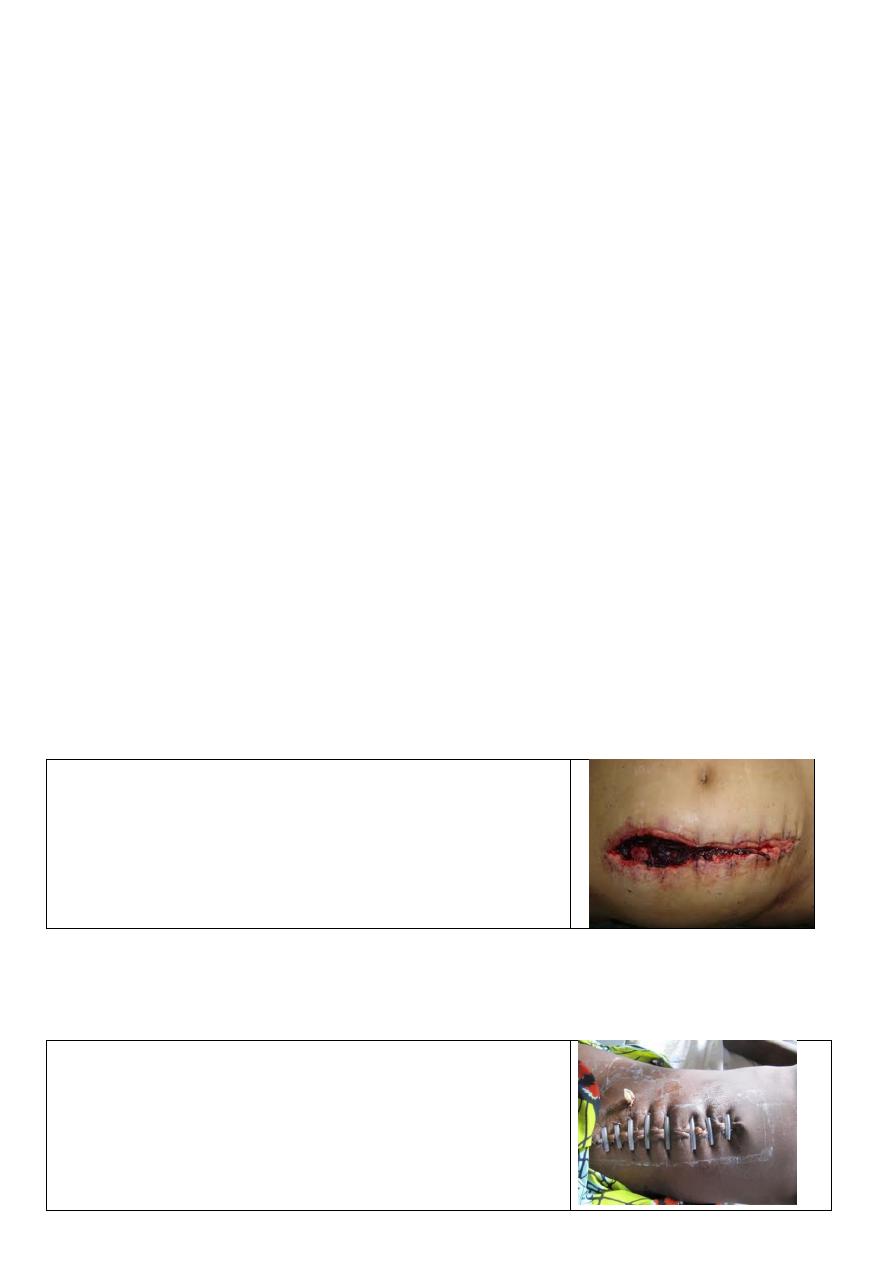
Burst abdomen (wound dehiscence)
The disruption of the all layers of wound, mostly between the 6th and 8th day after operation In 1—2
per cent of cases
Factors
1- surgeon causes ( Technique of wound closure).
• inappropriate suture material —catgut leads to a higher incidence of bursts than the use
of nonabsorbable, so should never be used;
• method of closure —interrupted suturing has a low incidence. than contenous
• tight sutures , may act as cutter when the patient is conscious and coughing.
• drainage directly through a wound leads to a higher incidence of ‘ bursts ’ than
employing drainage through a separate (stab) incision.
• Midline and vertical incisions have a tendency to burst which is higher than those which
are transverse.
2- operation causes .
• Infected case; causes wound infection
• Operations on the pancreas, with leakage of enzymes,
• Coughing; vomiting;. At the completion of an operation any violent coughing set off by
the removal of an endotracheal tube and suction of the laryngopharynx strains the sutures;
• vomiting and distension (e.g. due to ileus) in the early postoperative period.
• Over-vigorous postoperative ventilation in sedated patients can lead to wound disruption.
3- patient causes .
Obesity, jaundice, malignant disease, hypoproteinaemia and anaemia are all factors
conducive to disruption of a laparotomy wound; abdominal wounds in pregnancy are
notorious for a high risk of disruption; steroids delay wound healing.
Clinical features
• A serosanguinous (pink) discharge from the wound before fully disruption in 50 % of
cases. It is the most pathognomonic sign of impending wound disruption.
Patients often ‘ felt something give way ’ .
• If skin sutures have been removed, omentum or coils of
intestine may be forced through the wound and will be
found lying on the skin.
• Pain and shock are often absent
• there may be symptoms and signs of intestinal
obstruction.
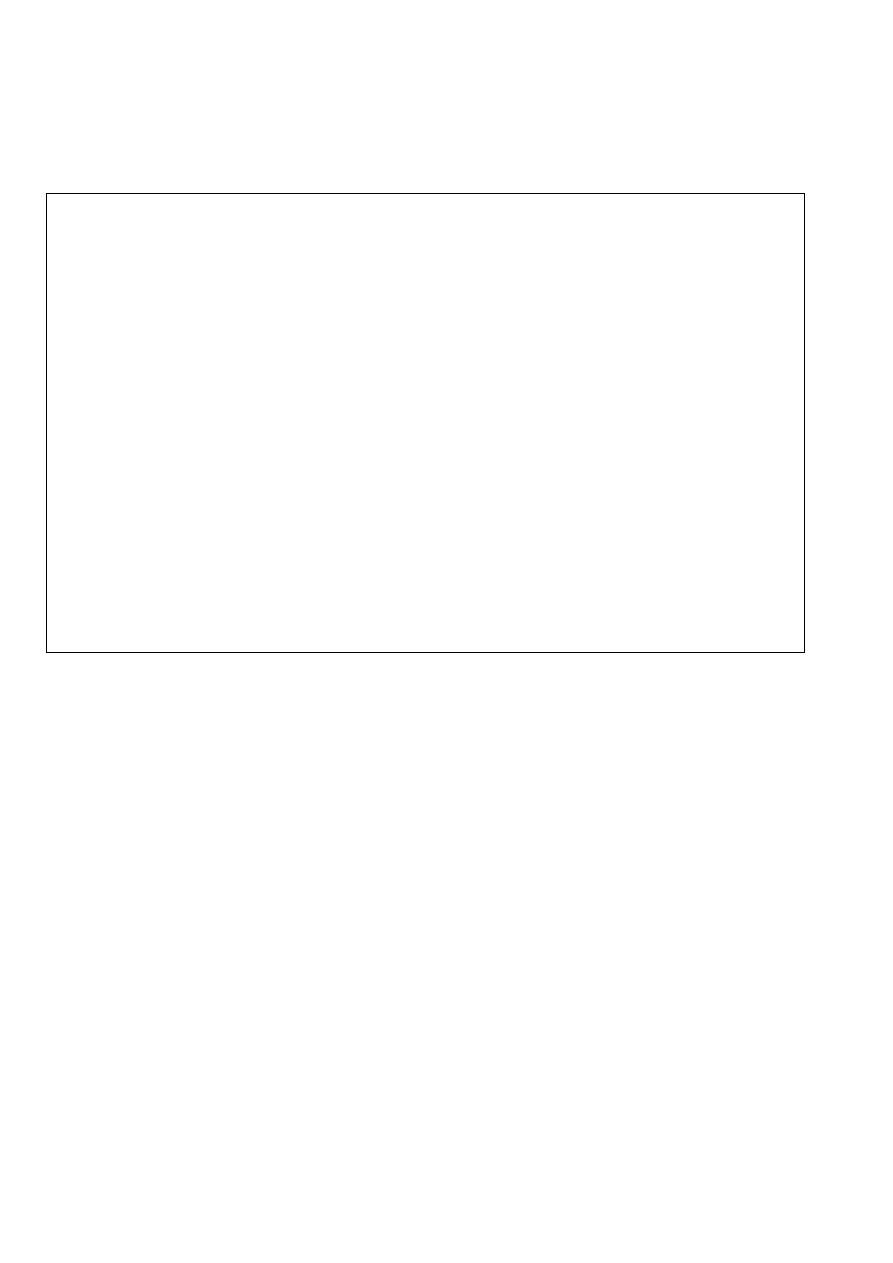
Treatment
An emergency operation is required to replace the bowel, relieve any obstruction then resuture the
wound.
--While awaiting operation, reassure the patient and cover the wound with a sterile towel.
-- nasogastric tube and intravenous fluid therapy commenced
.
operation.
--Each protruding coil of intestine is washed gently with saline
solution and returned to the abdominal cavity.
--close of The abdominal wall by (tension suture ) all layers are
approximated by through and through sutures of monofilament nylon,
each passed through a soft rubber or plastic tuber collar
.

Hernias
Dr. Muslim Kandel2019-20
12
--The abdominal wall may be supported by strips of adhesive plaster encircling the anterior two-thirds of
the circumference of the trunk.
-- Antibiotic therapy should be started., peritonitis rarely supervenes
A second dehiscence rarely occurs.
Incisional hernia (postoperative hernia)
Incisional hernia occurs due to disruption of deep layers of abdominal wall with intact skin and
subcutaneous tissues most often in :-
-obese individuals,
-a persistent postoperative cough
-postoperative abdominal distension
Causes : same as wound dehiscence , due to patients , operation and surgeon causes
Clinical features
An incisional hernia usually starts as a symptomless , may occur through a small portion of the scar,
often the lower end. More frequently there is a diffuse bulging of the whole length of the incision. usually
increases in size more and more of its become irreducible.
- Sometimes the skin overlying it is so thin and atrophic that normal peristalsis can be seen in the
underlying intestine.
- Attacks of partial intestinal obstruction are common and strangulation is liable to occur at the neck of a
small sac or in a loculus of a large one.
Treatment
Palliative. An abdominal belt is sometimes satisfactory, especially in cases of a hernia through an upper
abdominal incision.
Operative
1- Simple clossuer .
The layers are repaired usually with nonabsorbable sutures, sometime need tension-relaxing incisions
2-Complex apposition .
These consist of various procedures (Mayo, ‘ Keel ’ , Kattel , da Silva)
3-Plastic mesh ..
these techniques are now the method of choice for all
-- if above the umbilicus, A mesh is then inserted between the posterior rectus sheath and the muscle
--If below the umbilicus, the mesh is placed in the preperitoneal space.
Careful haemostasis and meticulous asepsis are essential , then put suction drainage (. Redivac).
Postoperative treatment.
NG and intravenous fluids are employed, and nothing by mouth allowed until the bowels have
functioned( bowel sound +ve)
Early ambulation and gentle physical exercise are to be encouraged. The patient should not resume
strenuous exercise for several weeks.
High recurrence rate of the hernia in between 30 and 50% except where mesh techniques have been
employed in specialist centers, where recurrence rates may be as low as 10 %
Rare external hernias
1-Divarication of the recti abdominis
Divarication of the recti abdominis is seen principally in elderly multiparous patients. When the patient strains, a
gap can be seen between the recti abdominis through which the abdominal contents bulge
2-Tearing of the inferior epigastric artery
occurs in elderly women, athletic, muscular men, or pregnant women, causes haematoma is usually at the level of
the arcuate line,
3- Interparietal hernia ( interstitial hernia).
An interparietal hernia has a hernial sac which passes between the layers of the anterior abdominal wall
Preperitoneal (20 %) Intermuscular (60 %) Inguinosuperficial (20 %)
4 - Lumbar hernia. 5 -Obturator hernia.6 -Gluteal and sciatic hernias.
Hernias
Dr. Muslim Kandel2019-20
13
Lecture four
other abdominal wall problems
Umbilicus
Diseases of the umbilicus
• Inflammation
Infection of the stump of the umbilical cord (omphalitis)
Umbilical granuloma ( Chronic infection of the umbilical stump)
Pilonidal sinus (a sinus containing a sheath of hairs)
• Fistula
Faecal Patent vitellointestinal duct
Neoplastic ulceration from the transverse colon
Tuberculous peritonitis
Urinary= Patent urachus
• Neoplasms
Benign Adenoma (raspberry tumour) , Endometrioma
Malignant
Primary
Secondary ( Stomach, Colon, including the rectum , Ovary and uterus
Breast)
• Hernia
• Umbilical calculus
Inflammation of the umbilicus
A) Acute infection of the umbilical cord (Omphalitis).
Usually occur at the third or fourth day post delivery the stump in over 50 per cent of
babies born in maternity hospitals. The chief prophylaxis is strict asepsis during cutting of
the cord and the use of 0.1 per cent chlorhexidine, locally, for a few days
management
-- antibiotic therapy usually localises the inflammation.
--warm moist dressings, the crusts separate, giving exit to pus.
complications
1-- Abscess of the abdominal wall. the infection is liable to spread along the hypogastric
arteries or umbilical vein , If gentle pressure is exerted above or below the umbilicus , and
a bead of pus exudes,
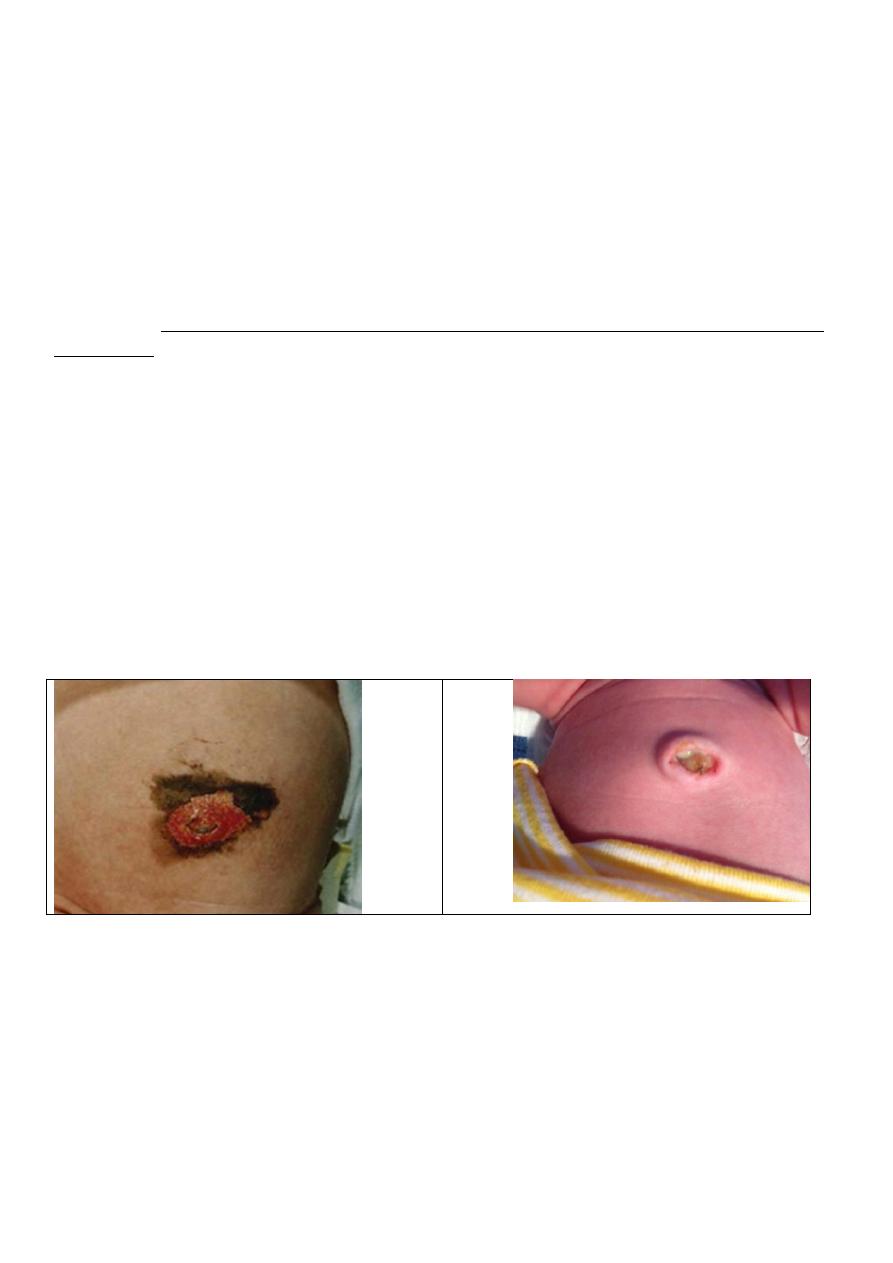
2-Extensive ulceration of the abdominal wall
. Extensive ulceration of the abdominal wall due to synergistic infection is treated in the
same way as postoperative subcutaneous gangrene
3- Septicaemia .
Septicaemia can occur from organisms entering the bloodstream via the umbilical vein.
4-Jaundice in neoborn baby this grave complication.
Infection reaching the liver via the umbilical vein may cause a stenosing intrahepatic
cholangiolitis, appearing some 3—6 weeks after birth.
5- Portal vein thrombosis .
Portal vein thrombosis and subsequent portal hypertension.
B) umbilical granuloma

Hernias
Dr. Muslim Kandel2019-20
14
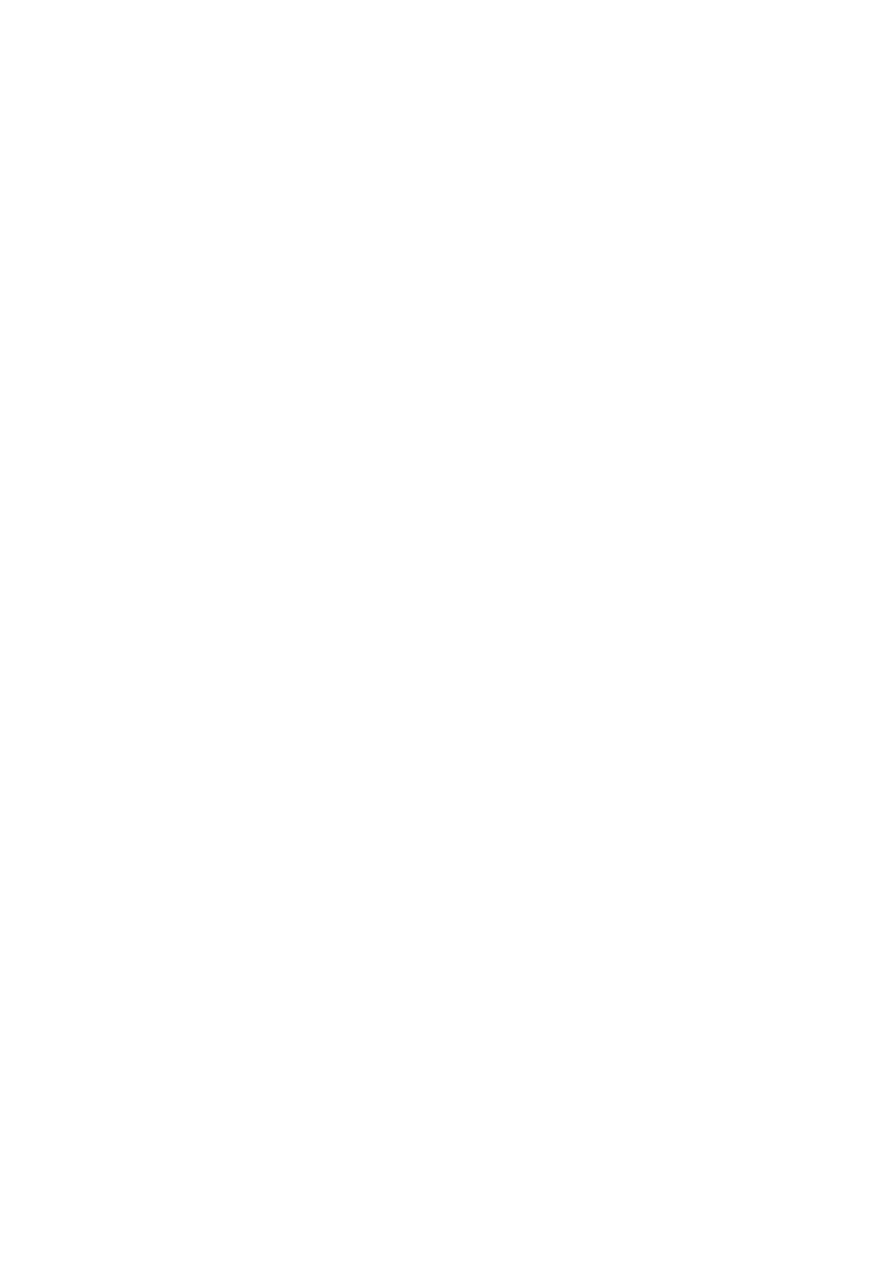
is the most common umbilical abnormality in neonates, causing inflammation and
drainage. Most fail to epithelialize and persist for more than 2 months some time with
discharge An umbilical granuloma its look as small piece of bright red, moist flesh that
remains in the umbilicus after cord separation It contains no nerves and has no feeling.
The cause of umbilical granuloma is delay healing during the drying up process, but the
exact cause is unknown.
Management :-the most common treatment is the topical application of concentrated
silver nitrate solution or double ligutuer
Umbilical fistulae
The umbilical cord contains blood vessels that carry blood to and from the fetus to the
mother
its also has fine connections with the urinary bladder and the intestines of the fetus. At
birth, the umbilical cord falls off, outside. At around the same time, the internal
communications of blood vessels and with the intestines called (vitellointestinal duct) and
bladder called (urachus) both also are shrivel off
.
A ) patent vitellointestinal duct.
The vitellointestinal duct occasionally persists and gives rise to one of the following
conditions
1•If all duct is patent umbilical fistula discharges mucus and, rarely, faeces.
2• If a small portion only of the duct near the umbilicus remains un obliterated. sinus
that discharges mucus
3• Sometimes both the umbilical and the intestinal ends of the duct close, intra-
abdominal cyst develops
4• With its lumen obliterated intraperitoneal band (there is danger, for intestinal
obstruction )
5•Such a band may contract and pull a Meckel ’ s diverticulum into a congenital
umbilical hernia
Treatment
. A patent vitellointestinal duct should be excised together with a Meckel ’ s diverticulum,
if one is present, preferably when the child is about 6 months old. When a vitellointestinal
band gives rise to acute intestinal obstruction, after removing the obstruction by dividing
the band,
Hernias
Dr. Muslim Kandel2019-20
15
B )Patent urachus.
A patent urachus seldom reveals itself until maturity or even old age. This is because the
contractions of the bladder commence at the apex of the organ and pass towards the base.
A patent urachus, because it opens into the apex of the bladder, is closed temporarily
during micturition and so the potential urinary stream to the bladder is cut off. Therefore
the fistula remains unobtrusive until a time when the organ is overfull, usually due to some
form of obstruction.
Treatment .
Treatment is directed to removing the obstruction to the lower urinary tract.
If, after this has been remedied, the leak continues or a cyst develops in connection with
the urachus, umbilectomy and excision of the urachus down to its insertion into the apex of
the bladder, with closure of the latter, is indicated
Infections of the abdominal wall
Cellulitis
can occur in any of the planes of the abdominal wall.
1- Superficial cellulitis
2- Deep cellulitis
Antibiotic therapy is the mainstay of treatment. When tenderness persists, an anatomical
incision dividing the muscles carefully, layer by layer, until pus or purulent fluid is
encountered is often advisable.
3-Progressive postoperative bacterial synergistic gangrene. This is, fortunately, a rare
complication after laparotomy, usually for a perforated viscus (notably perforated
appendicitis
The gangrenous skin liquefies exposing underlying granulation tissue. If the condition
persists, overwhelming septicaemia and associated multiorgan failure supervene.
Treatment
.Identification of the organisms and a report on their sensitivity to antibiotics is essential.
Metronidazole should be given together with a powerful broad-spectrum antibiotic.
Without vigorous and effective treatment the gangrene spreads to the flanks and the patient
may die of toxaemia
. If the infection has become established, surgical debridement of all the necrotic and
infected tissue should be performed. Hyperbaric oxygen, if available, can be life-saving.
Cellulitis due to bacteroides may give no bacterial growth by conventional techniques and
may be missed.
Hernias
Dr. Muslim Kandel2019-20
16
Neoplasms of the abdominal wall
Desmoid tumour
A desmoid tumour is a tumour arising in the musculoaponeurotic structures of the
abdominal wall, especially below the level of the umbilicus. It is a completely
unencapsulated fibroma.
80%of cases occur in women, many of whom have borne children, and the neoplasm
occurs occasionally in scars of old hernial or other abdominal operation wounds.. They can
occur in cases of familial polyposis coli (Gardner ’ s syndrome).
The tumour is composed of fibrous tissue usually of very slow growth, it tends to
infiltrate muscle in the immediate neighbourhood. Eventually it undergoes a myxomatous
change; it then increases in size more rapidly. Metastasis does not occur. Unlike fibroma
elsewhere, no sarcomatous change occurs.
Treatment.
the tumour is excised widely at least 2.5 cm of healthy tissue, recurrence commonly takes
place.
These tumours are moderately radiosensitive. (Intraperitoneal desmoids are best left alone
when possible.)
Fibrosarcoma of the abdominal wall
is rare. It is resistant to radiotherapy and only in some cases can a wide excision, with
nylon mesh repair, offer hope of a cure.