بسم هللا الرحمن الرحيم
السالم عليكم ورحمة هللا وبركاته

IN THE NAME OF GOD THE MOST
MERCIFULL
•
7/4/2020

Tumors of the lungs &bronchial
tree

Objectives
• To know the epidemiology ,etiology,
pathogenesis ,clinical presentation,
investigation ,diagnosis ,treatment
,complication ,prognosis

TUMOURS OF THE BRONCHUS AND
LUNG
• 1.8 million new cases worldwide each year
• Most common cancer in men
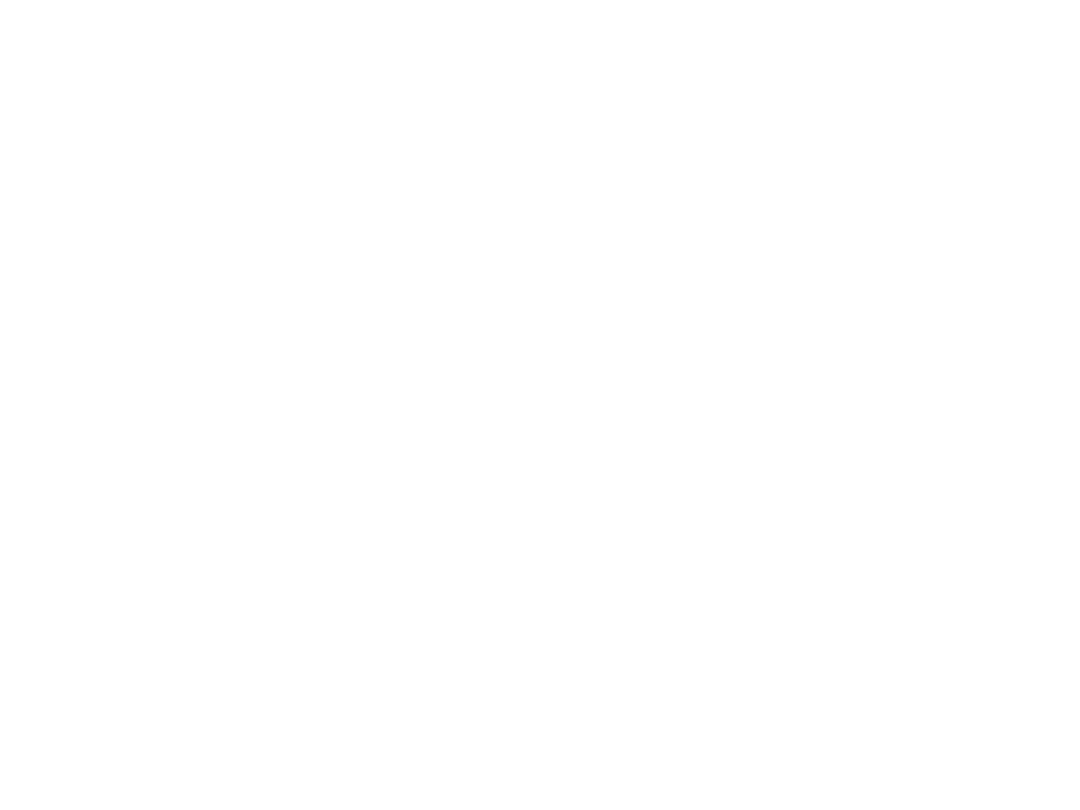
• Rates rising in women:
• Female lung cancer deaths outnumber male in some
Nordic countries
• Has overtaken breast cancer in several countries
• More than a threefold increase in deaths since 1950
• More than 50% of cases have metastatic disease at
diagnosis
• Lung cancer kills more than 120,000 Americans each year .
• Accounts for 18% of all cancer deaths

• the most common cause of death
from cancer world-wide.
• The majority are primary.
• prognosis remains poor.
• Carcinomas of other organs, as well
as sarcomas, metastatic to
pulmonary system
.

Primary tumours of the lung
• Aetiology
• Cigarette smoking
• Exposure to radon
• industrial materials (e.g. asbestos, silica,
beryllium, cadmium and chromium)

Common cell types in lung cancer
updated 2017
Cell type %
• Adenocarcinoma 35–40
• Squamous 25–30
• Small-cell 15
• Large-cell 10–15

Bronchial carcinoma
• The incidence of bronchial carcinoma
increased

• Bronchial carcinomas arise from the bronchial
epithelium or mucous glands.
• symptoms arise early, when the tumour
occurs in a large bronchus(central)
• delayed diagnosis tumors originating in a
peripheral bronchus.(peripheral)
• central necrosis and cavitation, and may
resemble a lung abscess on X-ray.(Squamous
cell carcinoma)
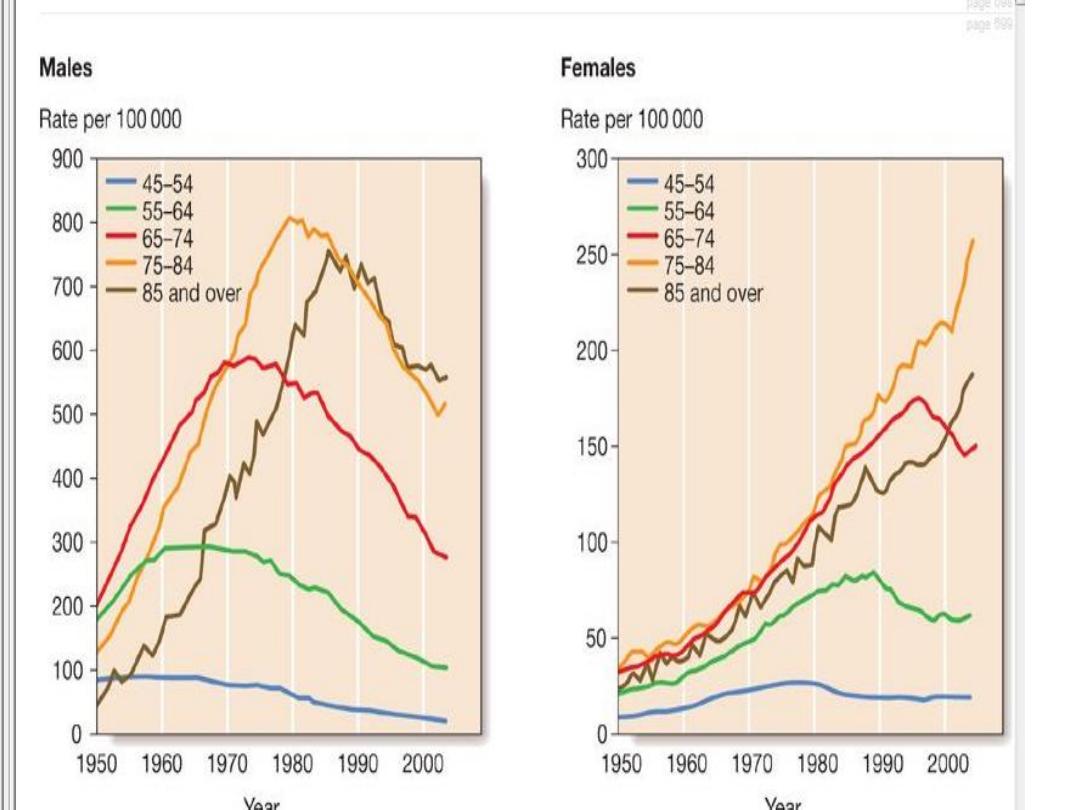
Lung cancer. An ill-defined mass is noted on the posteroanterior chest x-ray (arrows) (A).
Although this appears to be located near the right hilum, the lateral chest x-ray (B) clearly shows
the mass to be posterior to the hilum. Its shaggy appearance is very suggestive of carcinoma.
Further evaluation by computed tomography scan (C) clearly shows the mass in relation to the
mediastinal structures, such as the pulmonary artery (PA) and aorta (Ao).

Lung cancer in right lung
Chest X-ray.
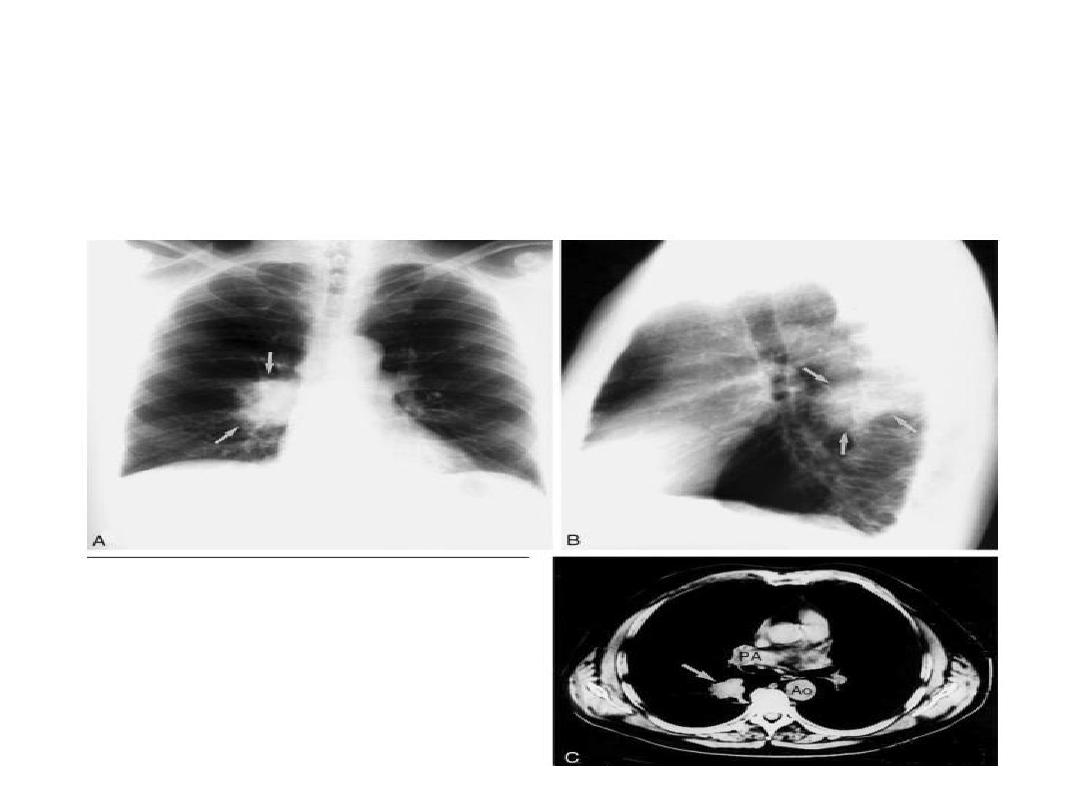
Lung cancer. A, The computed tomography scan shows a 2-cm soft tissue mass in the
middle portion of the left lung (arrow). B, A whole-body positron emission
tomography scan of the anterior chest and upper abdomen done with radioactively
labeled glucose shows markedly increased activity at the same area, indicative of very
high metabolic activity and a high probability of malignancy.

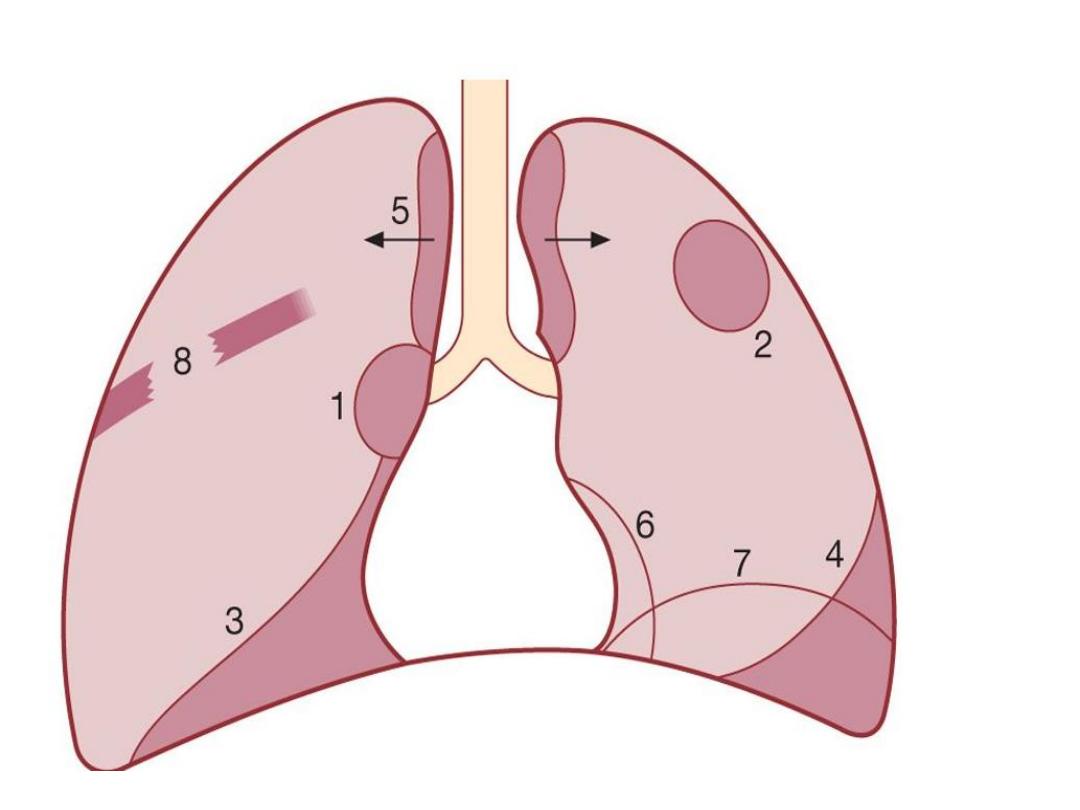
Bronchial carcinoma may involve
1-Direct invasion
• the pleura
• the chest wall,
• invading the intercostal nerves
• the brachial plexus and causing pain.
• Lymphatic spread
• mediastinal
• supraclavicular lymph nodes.

Blood-borne metastases
• Liver.
• Bone.
• Brain.
• Adrenals.
• Skin.

Even a small primary tumour
may cause widespread
metastatic deposits and this is
a particular characteristic of
small-cell lung cancers

Symptom
• Cough
• Chest pain
• Cough and pain
• Coughing blood
• Malaise
• Weight loss
• Shortness of breath
• Hoarseness
• Distant spread
• No symptoms

Tobacco 'tar'-stained fingers

clubb
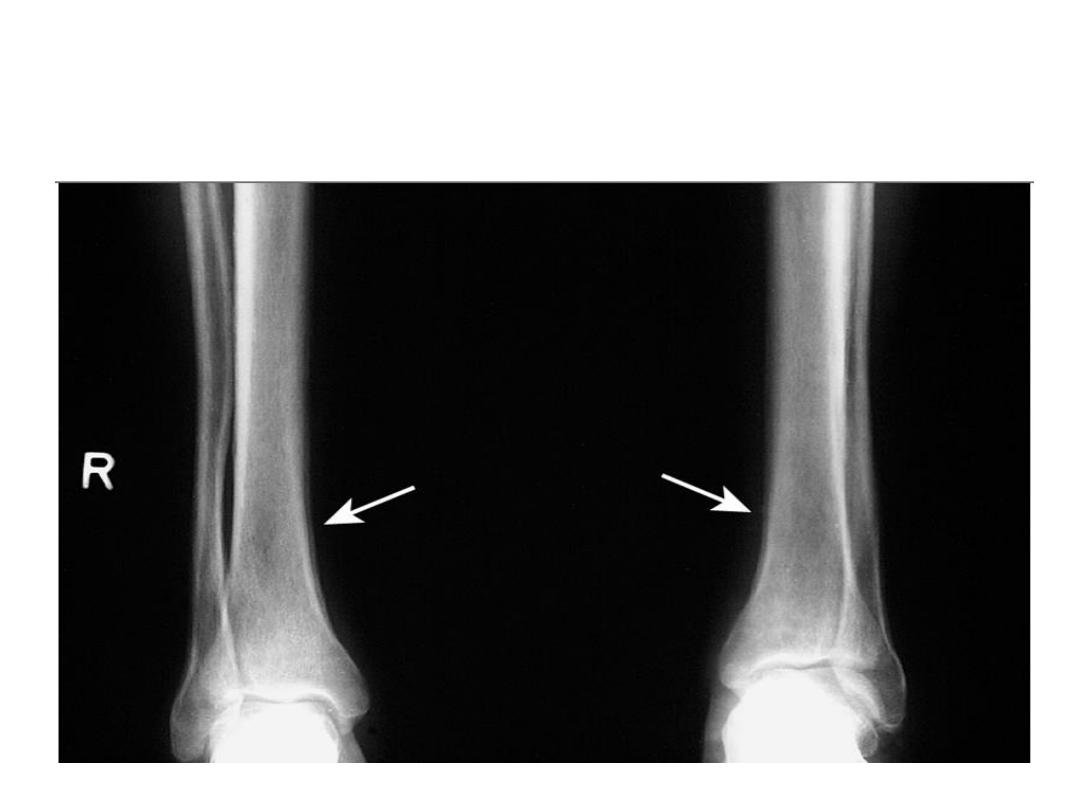
X-ray of the lower legs in hypertrophic pulmonary
osteoarthropathy. Arrows show periosteal reaction
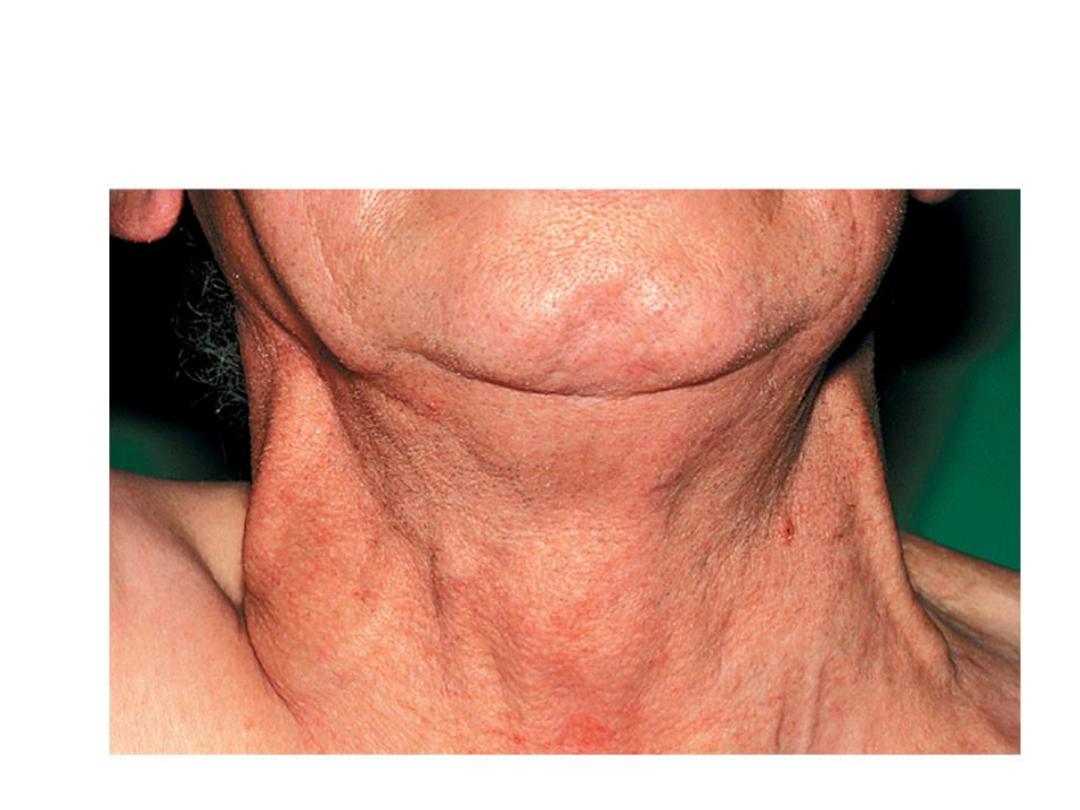
Superior vena caval obstruction Distended neck
veins.

Superior vena caval obstruction. Dilated superficial veins over
chest

local
• Cough.
• Haemoptysis.
• Breathlessness .
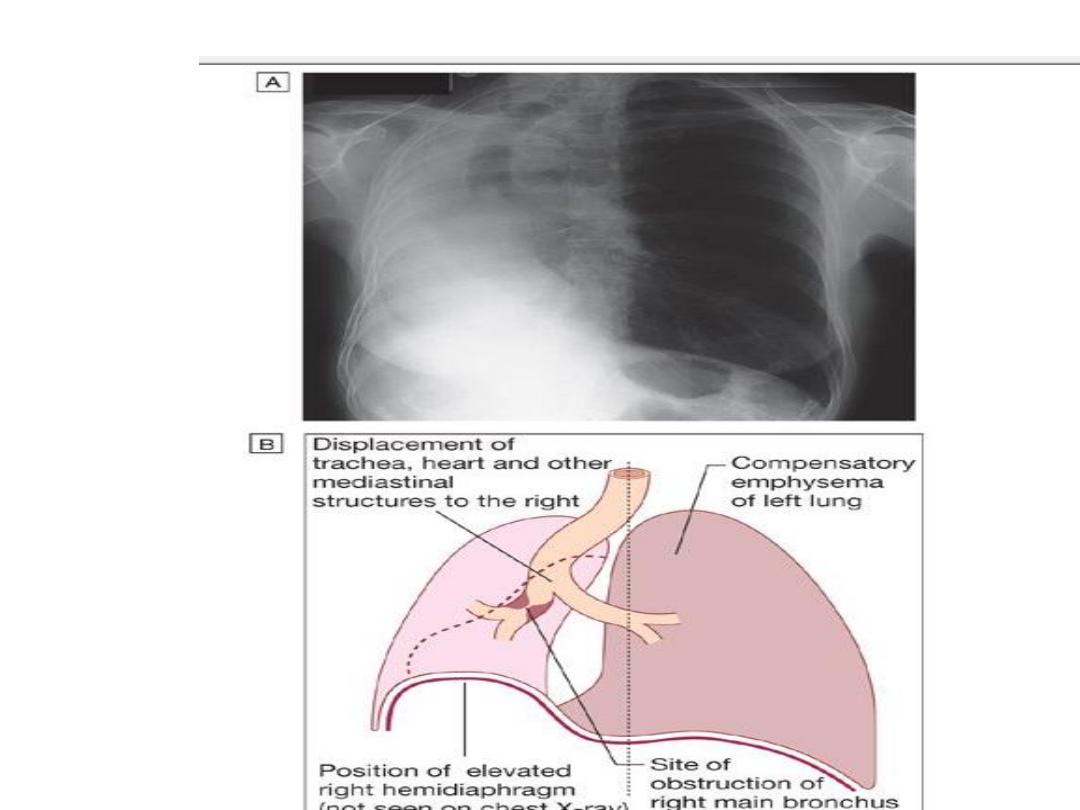
• Bronchial obstruction.
collapse of a lobe or lung .
• cause pneumonia or lung abscess.
• Recurnt Pneumonia at the same site.
• Stridor (a harsh inspiratory noise) .
• a large pleural effusion
• compressing a phrenic nerve causing diaphragmatic
paralysis.
•

Pain and nerve entrapment.
• Pleural pain.
• pain in the distribution of a thoracic
dermatome.
• Horner's syndrome (ipsilateral partial ptosis,
enophthalmos, miosis and hypohidrosis of the
face).
• Pancoast's syndrome (pain in the shoulder and
inner aspect of the arm, sometimes with small
muscle wasting in the hand).
•

Mediastinal spread.
• Dysphagia If the oesophagus is involved.
• Invasion of the pericardium, lead to
arrhythmia or pericardial effusion .
• Superior vena cava obstruction.
• left recurrent laryngeal nerve --- causes vocal
cord paralysis, voice alteration and a 'bovine'
cough (lacking the normal explosive
character).
• Supraclavicular lymph nodes -----enlarged.

Metastatic spread.
Brain
• focal neurological defects,
• epileptic seizures,
• personality change,
Liver : jaundice,
Bone : bone pain
Skin
:skin nodules.
• Lassitude, anorexia and weight loss.
• Digital clubbing.

Non-metastatic extrapulmonary manifestations of
bronchial carcinoma
Endocrine
• Inappropriate antidiuretic hormone secretion
causing hyponatraemia
• Ectopic adrenocorticotrophic hormone secretion
• Hypercalcaemia due to secretion of parathyroid
hormone-related peptides
• Carcinoid syndrome
• Gynaecomastia

• Neurological
• Polyneuropathy
• Myelopathy
• Cerebellar degeneration
• Myasthenia (Lambert-Eaton syndrome,)

• Digital clubbing
• Hypertrophic pulmonary osteoarthropathy
• Nephrotic syndrome
• Polymyositis and dermatomyositis
• Eosinophilia

• Investigations
• confirm the diagnosis .
• establish the histological cell type.
• define the extent of the disease.

• Imaging
• plain X-rays
• Spiral CT
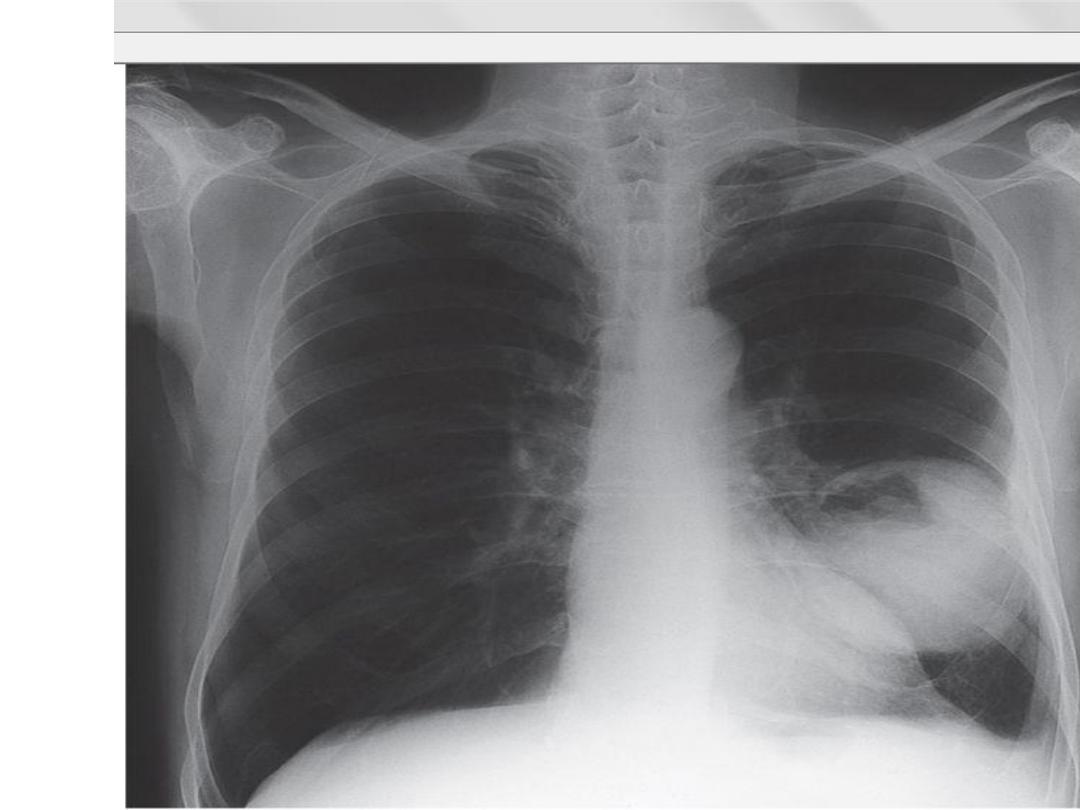

Lung cancer in right lung
Chest X-ray.
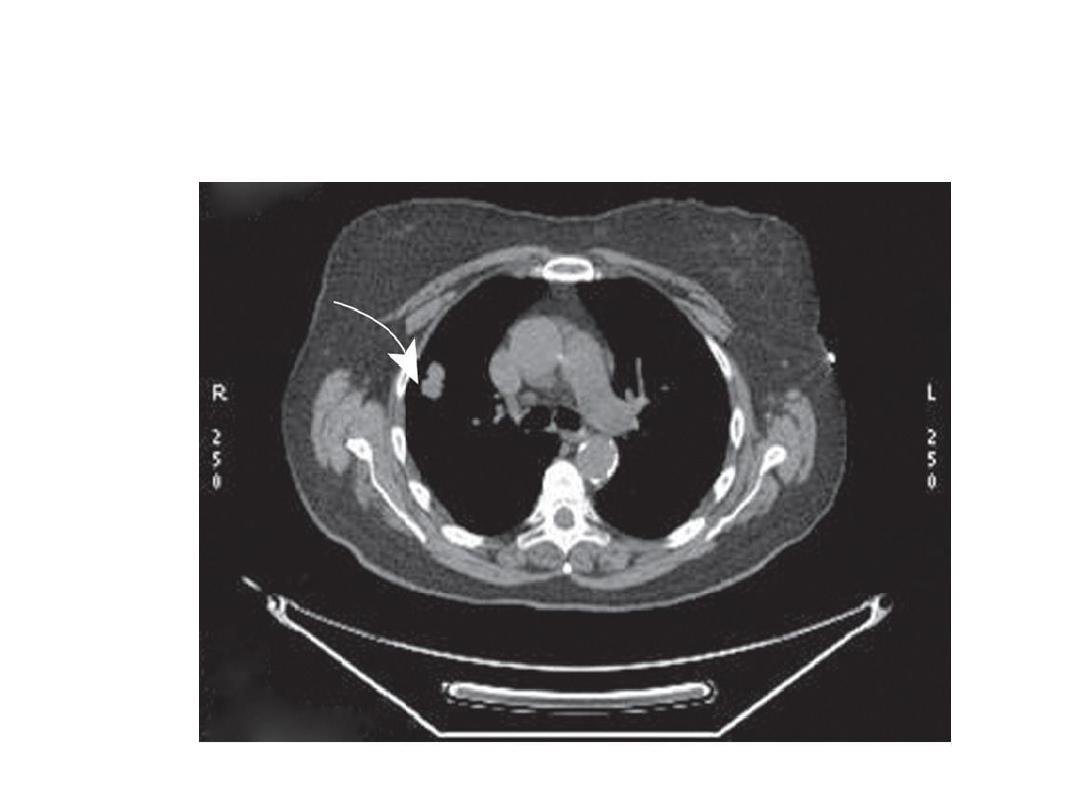
Lung cancer in right lung CT scan of thorax.
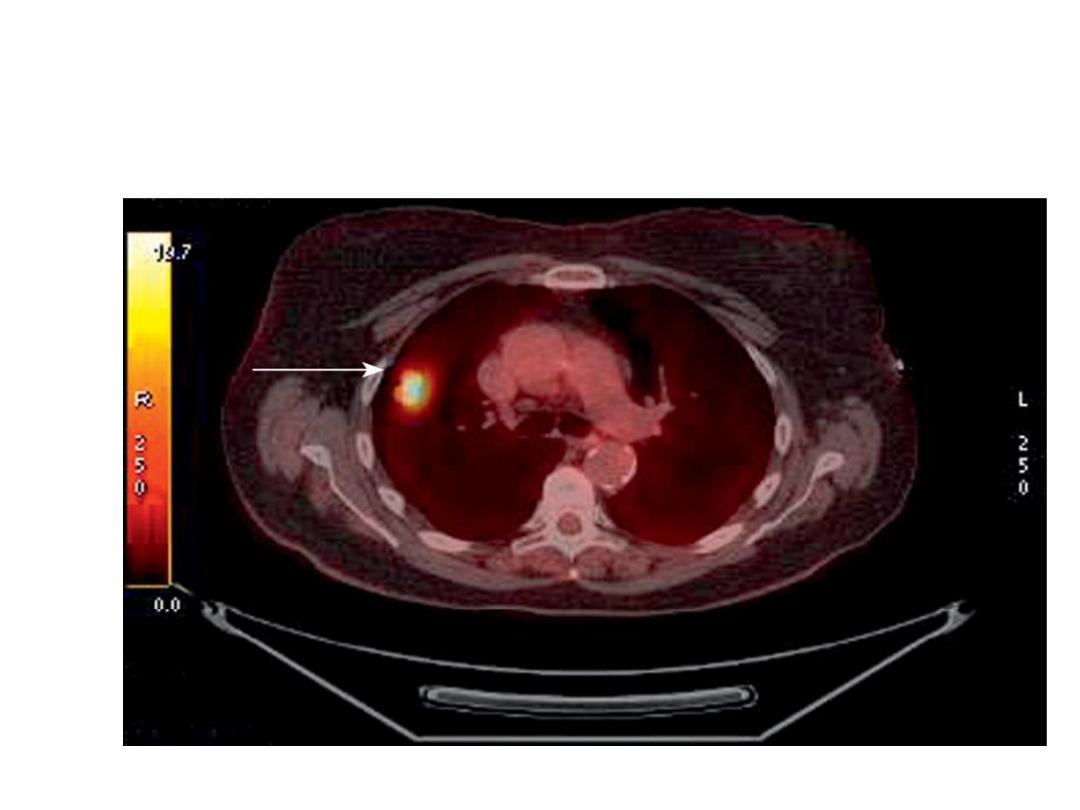
Lung cancer in right lung
Positron emission tomography
(PET) scan showing increased uptake in tumour

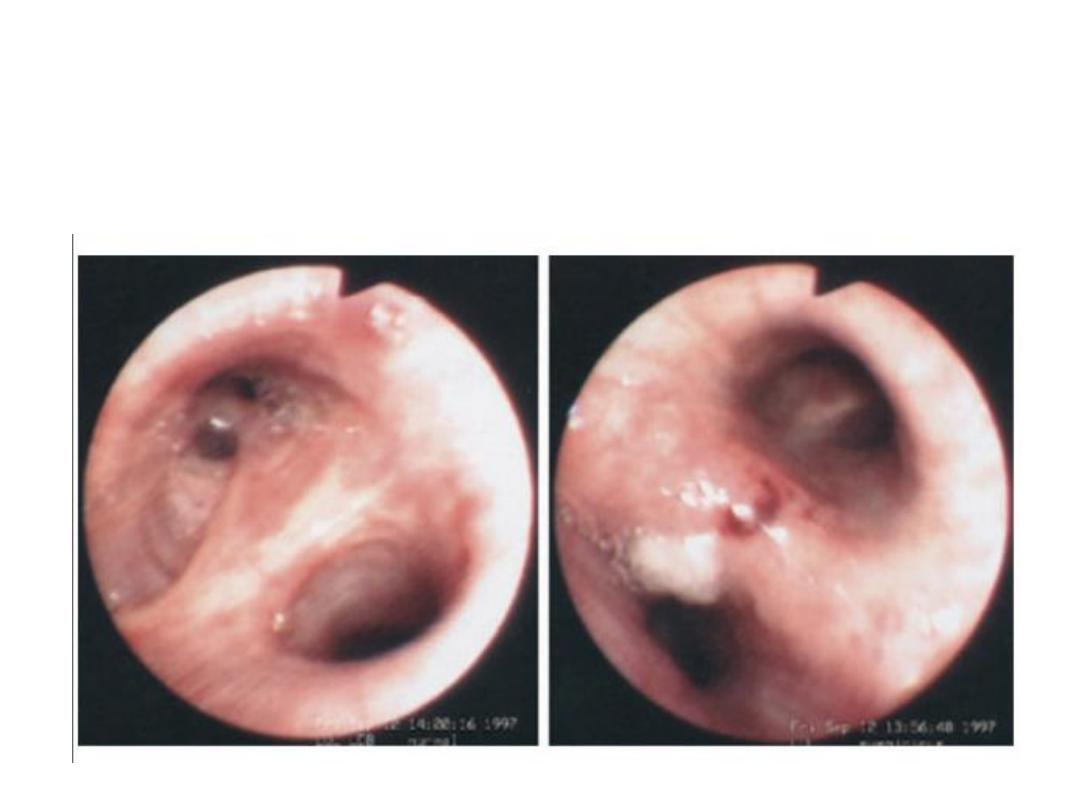
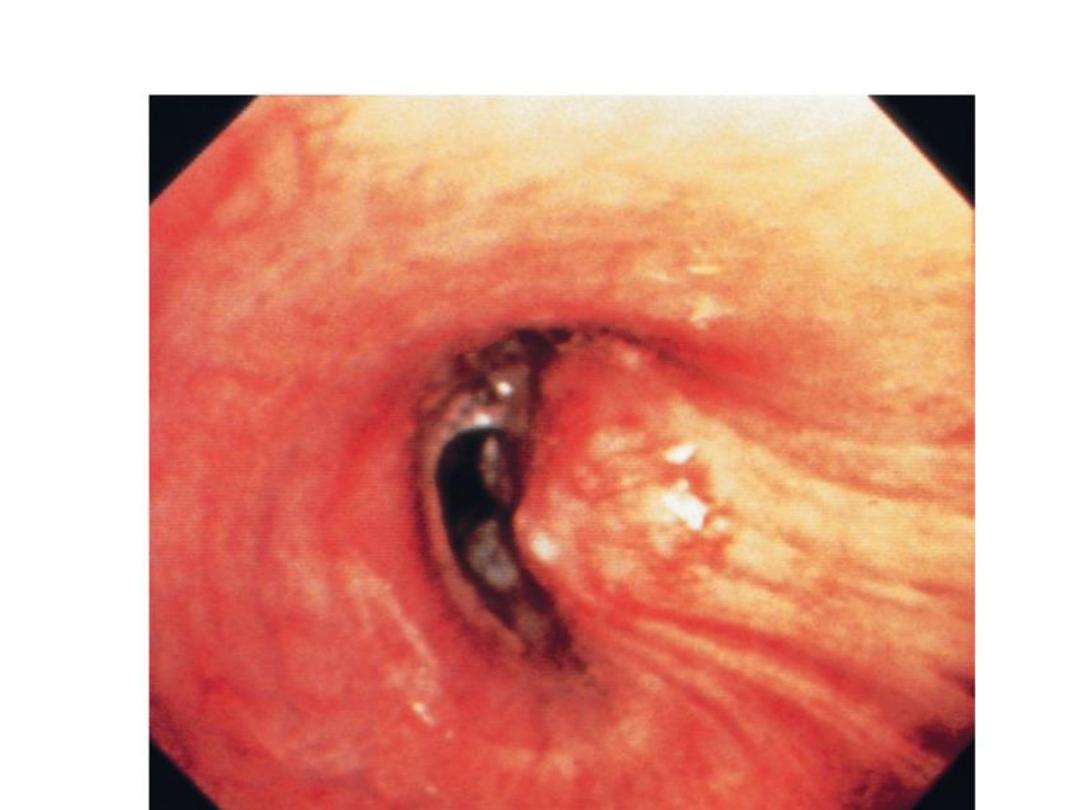
•Histological
characterisation
•
• flexible bronchoscope.
• 'blind' bronchoscopic washings and
brushings
• percutaneous needle biopsy under CT or
ultrasound guidance .
Squamous cell carcinoma.
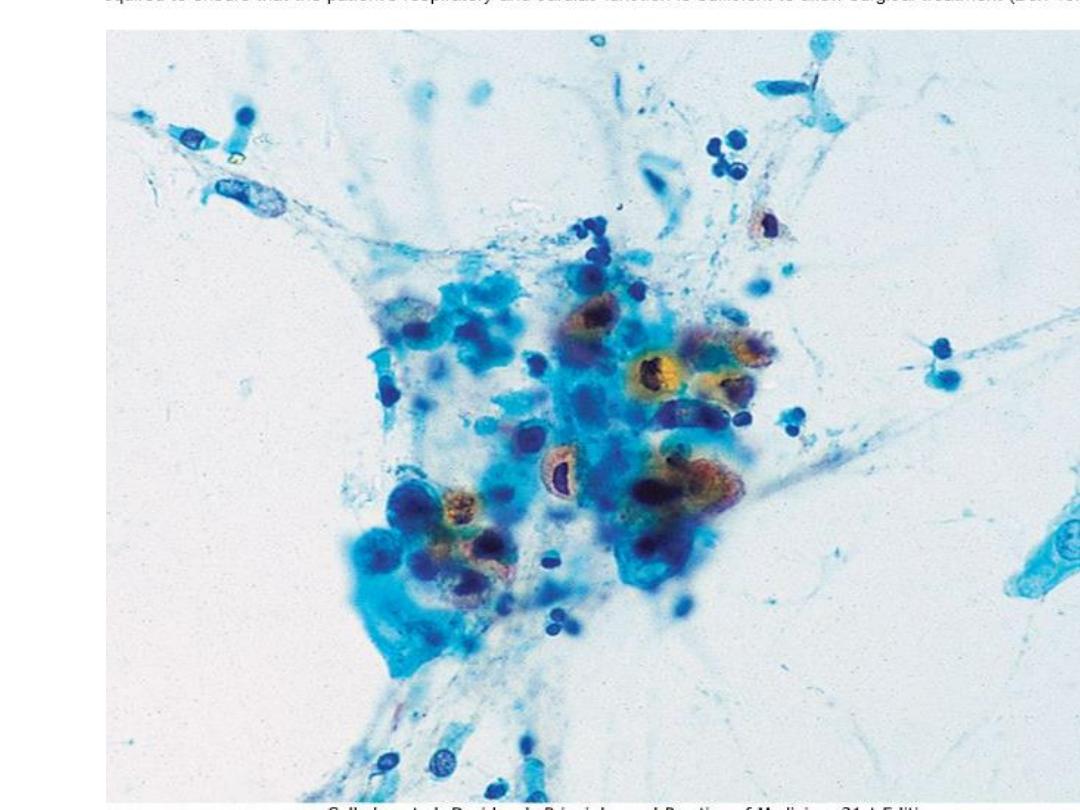
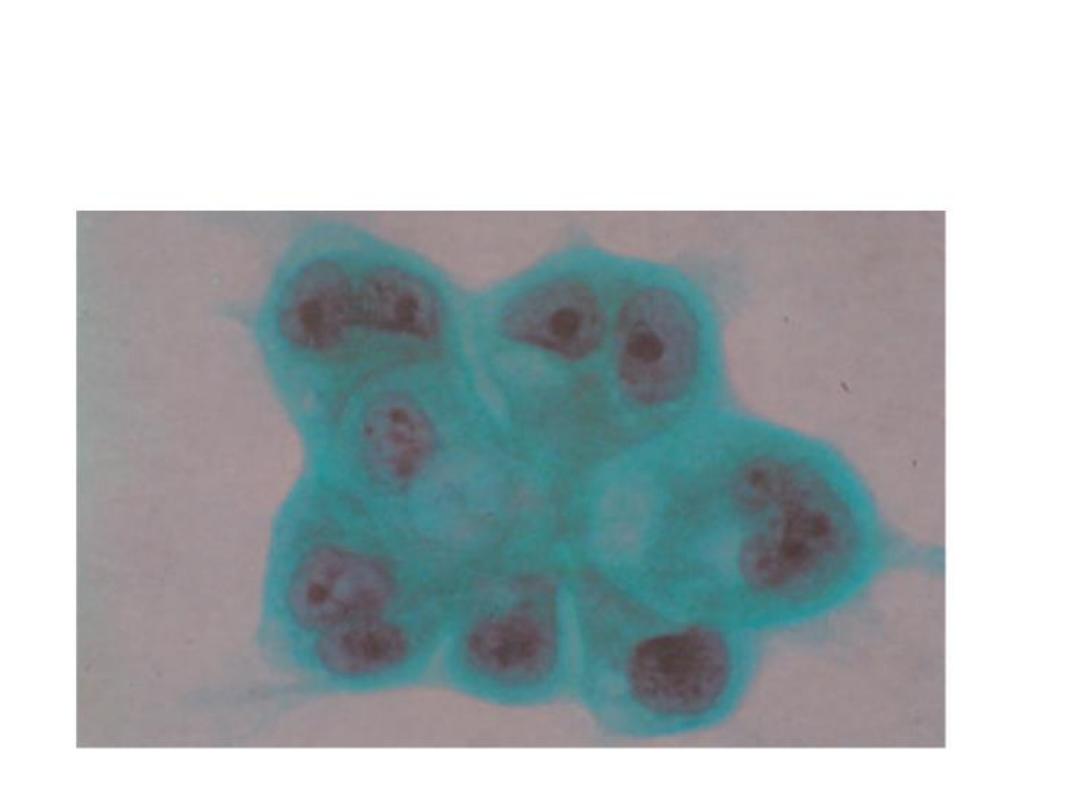
Adenocarcinoma cells in a sputum smear
Three sputum samples should be obtained for
cytology
pleural effusions, pleural aspiration and biopsy
thoracoscopy.
needle aspiration or biopsy of affected
o
lymph nodes,
o
skin lesions,
o
liver
o bone marrow.
• Management
Surgical resection carries the best hope of long-
term survival.
some patients treated with
• radiotherapy
• Chemotherapy.
over 75% of cases,NO treatment curative
treatment .
Radiotherapy, chemotherapy, can relieve
distressing symptoms.

• Contraindications to surgical resection in
bronchial carcinoma
(important)
1. Distant metastasis .
2. Invasion of central mediastinal structures
including heart, great vessels, trachea and
oesophagus .
3. Malignant pleural effusion .
4. Contralateral mediastinal nodes .
5. FEV
1
< 0.8 L .
6. Severe or unstable cardiac or other medical
condition

Laser therapy and stenting
• major airway obstruction
General aspects of management .
• The management in specialist centres by
multidisciplinary teams including
• oncologists,
• thoracic surgeons,
• respiratory physicians
• specialist nurses;
Treatment include:
• effective communication.
• pain relief .
• attention to diet .
• depression and anxiety, need specific therapy.
• drain the pleural cavity.
• pleurodesis with a sclerosing agent.

• Prognosis
• very poor .
• 70% of patients dying within a year .
• only 6-8% of patients surviving 5 years after
diagnosis.
• The best prognosis is with well-differentiated
squamous cell tumours .

Secondary tumours of the lung
Blood-borne metastatic
from many primary tumours :
•
breast,
• kidney,
• uterus,
• ovary,
• Testes
• thyroid.

Diagnosis
No symptoms
• Breathlessness .
• haemoptysis.
radiological examination
• Multiple bilateral cannon balls.
• lobar collapse
• Lymphangitic spread of
carcinoma in the lung
• Lymphatic infiltration may develop in patients
with carcinoma of the
• breast,
• stomach,
• bowel,
• pancreas
• bronchus.

• This grave condition causes severe and rapidly
progressive breathlessness associated with
marked hypoxaemia.

The chest X-ray
• shows diffuse pulmonary shadowing radiating
from the hilar regions, with septal lines.
• CT scans
characteristic.
• Palliative treatment of breathlessness with
opiates may help.

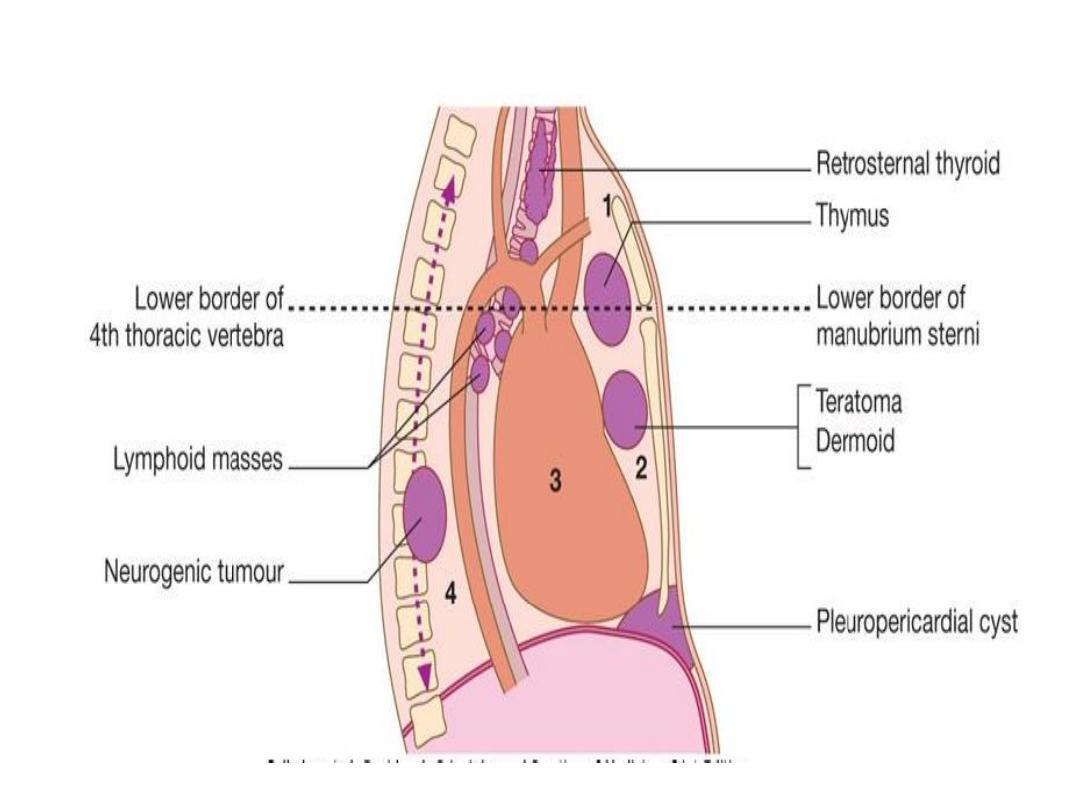
Tumours of the mediastinum
present radiologically as a mediastinal mass .
Benign tumours and cysts
• symptoms by compressing
•
the trachea
•
the superior vena cava.
• rupture into a bronchus.

Malignant mediastinal tumours
Invasion
Compress surrounding structures.
• The most common cause is mediastinal lymph
node
• metastases from bronchogenic carcinoma
• lymphomas,
• leukaemia,
• malignant thymic tumours
•
germ-cell tumours

• Aortic and innominate aneurysms
have destructive features
resembling those of malignant
mediastinal

• Causes of a mediastinal mass
• Superior mediastinum
• Retrosternal goitre
• Persistent left superior vena cava
• Prominent left subclavian artery
• Thymic tumour
• Dermoid cyst
• Lymphoma
• Aortic aneurysm

• Anterior mediastinum
• Retrosternal goitre
• Dermoid cyst
• Thymic tumour
• Lymphoma
• Aortic aneurysm
• Germ cell tumour
• Pericardial cyst
• Hiatus hernia through the diaphragmatic foramen
of Morgagni

• Posterior mediastinum
• Neurogenic tumour
• Paravertebral abscess
• Oesophageal lesion
• Aortic aneurysm
• Foregut duplication
•
• Middle mediastinum
• Bronchial carcinoma
• Lymphoma
• Sarcoidosis
• Bronchogenic cyst
• Hiatus hernia

• Radiological examination
CT (or MRI) is the investigation of choice for
mediastinal tumours .
• Large mass (intrathoracic goitre-arrows)
extending from right upper mediastinum.
• Endoscopic investigation
Bronchoscopy.

Surgical exploration
Mediastinoscopy to visualise and biopsy masses.
Management
• Benign mediastinal tumours should be removed
surgically
• neural tumours, have the potential to undergo
malignant transformation.

THANK YOU
To know the epidemiology ,etiology,
pathogenesis ,clinical presentation,
investigation ,diagnosis ,treatment
,complication ,prognosis