CANCER EPIDEMIOLOGY
Study of cancer occurrence in populations has contributed substantially to
knowledge about its origins. The now well established concept that cigarette smoking
is causally associated with lung cancer arose primarily from epidemiologic studies,
Major insights into the causes of cancer can be obtained by epidemiologic studies that
relate particular environmental, racial (possibly hereditary), and cultural influences to
the occurrence of specific neoplasms
.
Geographic and environmental factors
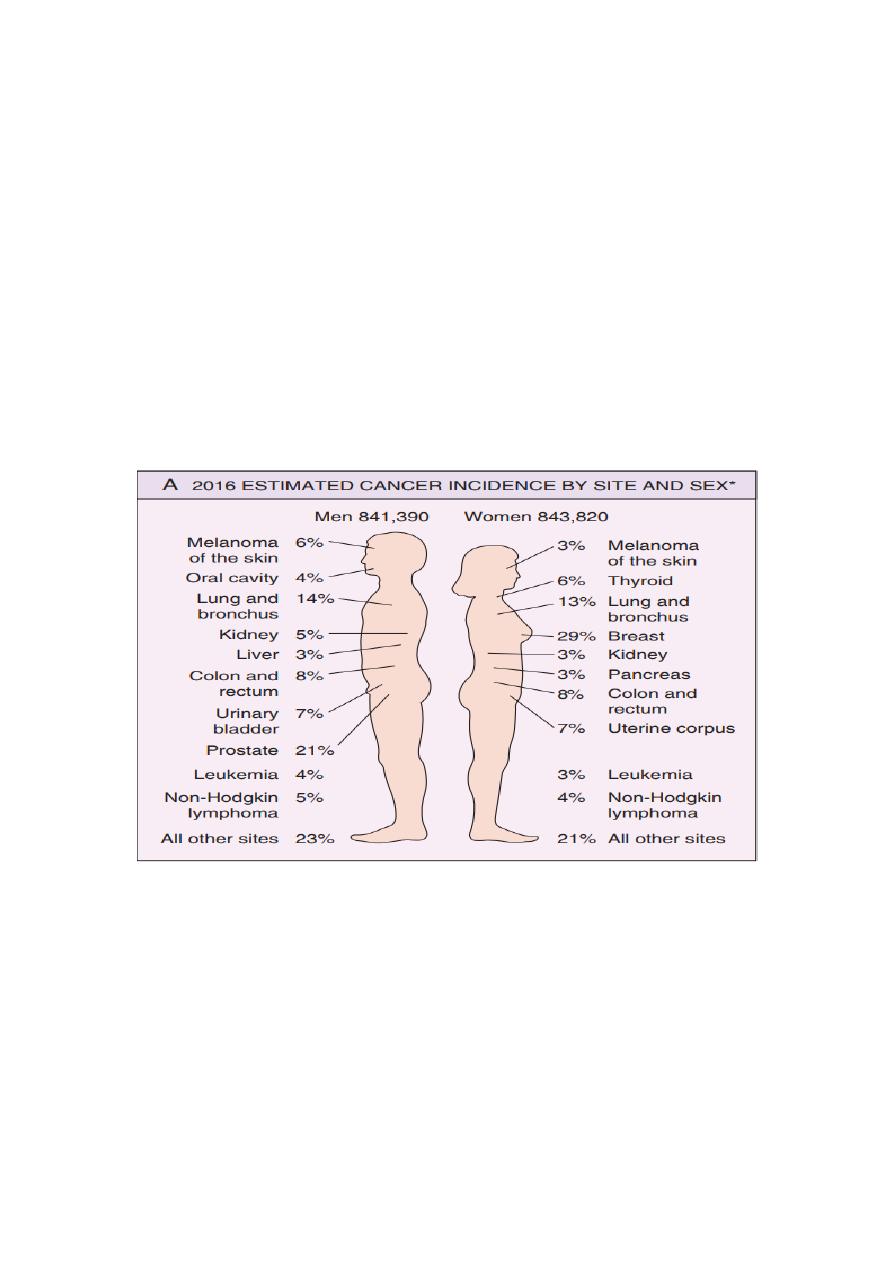
Environmental exposures appear to be the dominant risk factors for many common
cancers, suggesting that a high fraction of cancers are potentially preventable, the
common types of cancers that are
prostate,
lung
and
colon
are the leading cancers
in males.
In females cancers of the
breast
,
lung,
and
colon
are the commonest.
In Iraqi males the commonest cancers are those of the lung, bladder, larynx as well
as non Hodgkin’s lymphomas (NHL) and leukemias.
In Iraqi females breast, NHL, Leukemia, CNS tumors and lung cancers are the
commonest.
Environmental factors significantly affect the occurrence of specific forms of
cancer in different parts of the world.
In Japan carcinoma of the stomach is commoner than in USA while carcinoma of the
colon is uncommon. In Japanese immigrants to the USA, the incidence of both
cancers is intermediate between Japanese and USA natives .

Hepatocellular carcinoma is particularly common in South East Asia.
Esophageal carcinoma is common in north of Iraq, north of Iran as well as in central
Asia.
Other examples of environmental factors:
Occupational exposure to
asbestos
is associated with lung carcinoma, pleural and
peritoneal mesotheliomas.
Occupational exposure to
aniline dyes
is associated with bladder carcinoma.
Occupational exposure to
polyvinyl chloride monomers
is associated with liver
angiosarcoma.
Cigarette smoking
is associated with carcinomas of the oropharynx, larynx and
lung.
Air pollution is associated with lung cancer.
Age and Cancer :
In general, the frequency of cancer increases with age. Most cancer deaths occur
between 55 and 75 years of age. The rising incidence with age may be explained by
the accumulation of somatic mutations that drive the emergence of malignant
neoplasms and the decline in immune competence that accompanies aging also may
be a factor.
The major lethal cancers in children are leukemias, tumors of the central nervous
system, lymphomas, and soft-tissue and bone sarcomas .
Acquired Predisposing Conditions:
Acquired conditions that predispose to cancer include disorders associated with
chronic inflammation, immunodeficiency states, and precursor lesions
.
Many different precursor lesions have been described; among the most common are
the following:
1-
Squamous metaplasia and dysplasia of bronchial mucosa, seen in in habitual
smokers—a risk factor for lung carcinoma .
2-
Endometrial hyperplasia and dysplasia, seen in women with unopposed estrogenic
stimulation—a risk factor for endometrial carcinoma
3-
Leukoplakia of the oral cavity, vulva, and penis, which may progress to squamous
cell carcinoma .
4-
Villous adenoma of the colon, associated with a high risk for progression to
colorectal carcinoma .
The subsequent development of malignancy in a benign tumor is quite
uncommon, most malignant tumors arise de novo. However, there are few
exceptions, e.g., villous adenoma of the colon often develops into carcinoma.
PREINVASIVE MALIGNANCY:
Recently, cancer screening programs have emphasized the prevalence of
lesions, which appear to be early stages in the development of cancers. They
share some cytological features of infiltrative (invasive) tumors, but have not yet
become infiltrative themselves.
The implication is strong that they might become infiltrative if left long
enough, although we cannot say how long would that be. Nor it is possible to tell
how far they have evolved from normality in terms of time or biological events, or
if any of these events are reversible.
These changes are referred to as dysplasia (disorganization of tissue
structure).
Cytological features of malignancy are grouped under Atypia
Atypia + disorganization of tissue structure= Dysplasia
mild
moderate
severe
Severe dysplasia
-involve the entire thickness
-still within the normal confines of the epithelium
-intact basement membrane – No invasion
Intraepithelial neoplasia
in situ
Carcinoma
carcinoma
Invasive
progress to
Dysplasia have been described in the epithelia of the
- cervix
- vulva
- urinary bladder
- bronchial mucosa
- larynx
- oral cavity
- skin
- prostate etc,.
In the cervix, vulva and the prostate they are called “intraepithelial neoplasia”.
The cells show many of the cytological changes of malignant tumors, like cellular
overcrowding, pleomorphism, hyperchromatic nuclei, loss of normal orientation (loss
of polarity) and disorderly maturation (e.g. dyskeratosis), mitotic activity above the
basal layers .
Despite these manifestations of abnormal cell behavior, the changes are all within the
normal confines of the epithelium; the basement membrane is not breached.
When the entire thickness of the epithelium is involved by the above cellular changes,
this has been referred to as ―carcinoma in situ‖ and presently as grade 3 or high-
grade intraepithelial neoplasia.
Carcinoma in situ is the forerunner, in many cases, of invasive malignancy, However
mild degrees of dysplasia (grade 1 or low-grade intraepithelial neoplasia), common
in the uterine cervix, don’t always lead to cancer and are often reversible.
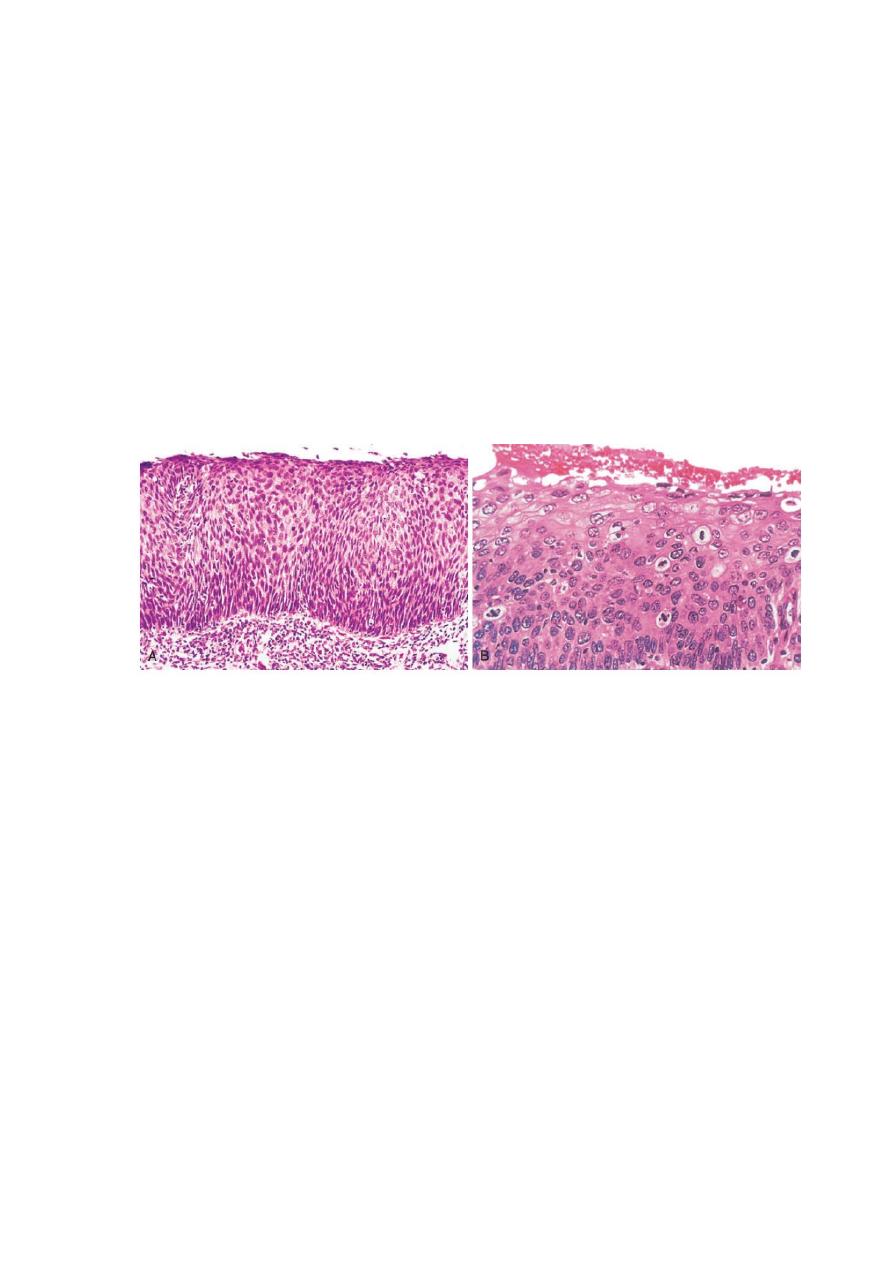
Carcinoma in situ. (A) Low-power view shows that the entire thickness of the epithelium is
replaced by atypical dysplastic cells. There is no orderly differentiation of squamous cells.The
basement membrane is intact, and there is no tumor in the subepithelial stroma. (B) High-
power view of another region shows failure of normal differentiation, marked nuclear and
cellular pleomorphism, and numerous mitotic figures extending toward the surface. The intact
basement membrane (below) is not seen in this section.