Clinical Features of Tumors:
LOCAL AND HORMONAL EFFECTS
Local effects of the tumor or its metastasis can be due to pressure or
destruction by direct infiltration, and bleeding from ulceration.
Endocrine tumors may produce hormones (commoner in benign than
malignant tumors), e-g. adrenocortical adenoma can cause Cushing’s
syndrome and pheochromocytoma can cause hypertension.
CANCER CACHEXIA
Loss of body fat, wasting, and profound weakness is referred to as cancer
cachexia.
The basis for cachexia is multifactorial:
1- Loss of appetite.
2- Metabolic changes leading to reduced synthesis and storage of fats
and increased mobilization of fatty acids from adipocytes.
3- Production of cachectin (TNF-alpha) by macrophages, and some
tumor cells and possibly other humoral factors can produce the
metabolic effects of cachexia.
PARANEOPLASTIC SYNDROMES:
Definition
Symptoms not directly related to the primary tumor or its metastasis or
elaboration of hormones indigenous to the tissue from which the tumor
arose.
Paraneoplastic syndromes may be the earliest manifestation of a tumor
and may mimic distant spread.
The commonest syndromes include:
1. Endocrinopathies: Ectopic hormone or hormone-like factors
production by nonendocrine cancers e.g., parathormone by
squamous cell carcinoma of the lung, inappropriate ACTH or ADH
release by small cell cancers of the lung, polycythaemia due to
erythropoetin production by renal cell carcinoma , hypoglycemia
due to production of insulin or a like factor by hepatocellular
carcinoma .
2- Myopathy, neuropathy, encephalopathy or myesthenic
syndromes as in lung cancers possibly due to immunological
mechanisms.

2. Hypertrophic osteoarthropathy and finger clubbing in lung
cancer (unknown cause).
3. Vascular and hematological changes:
Non-bacterial thrombotic endocarditis and DIC, in advanced
cancers due to hypercagulibility.
4. Nephrotic syndrome in various cancers mediated by tumor
antigens and immune complexes.
Grading and Staging of Cancer
Methods to quantify the probable clinical aggressiveness of a given
neoplasm and its apparent extent and spread in the individual patient are
necessary for arriving at an accurate prognosis and for comparing end
results of various treatment protocols. For instance, the results of treating
well-differentiated thyroid adenocarcinomas localized to the thyroid
gland will on average be very different from those obtained from treating
highly anaplastic thyroid cancers that have invaded the neck organs.
1-
Grading:
grading of a cancer is based on the degree of
differentiation of the tumor cells, generally range from two
categories (low grade and high grade) to four categories, Although
histologic
grading
is
useful,
the
correlation
between
histologic appearance and biologic behavior is less than perfect. In
recognition of this problem and to avoid spurious quantification, it
is common practice to characterize a particular neoplasm in
descriptive terms, for example, well-differentiated, mucin-secreting
adenocarcinoma of the stomach, or poorly differentiated pancreatic
adenocarcinoma.
2- Staging.
The staging of solid cancers is based on the size of the
primary lesion, its extent of spread to regional lymph nodes, and
the presence or absence of bloodborne metastases. The major
staging system currently in use is the American Joint Committee
on Cancer Staging. This system uses a classification called the
TNM system—T for primary tumor, N for regional lymph node
involvement, and M for metastases. TNM staging varies for
specific forms of cancer, but there are general principles. The
primary lesion is characterized as T1 to T4 based on increasing
size. T0 is used to indicate an in situ lesion. N0 would mean no
nodal involvement, whereas N1 to N3 would denote involvement
of an increasing number and range of nodes. M0 signifies no
distant metastases, whereas M1 or sometimes M2 reflects the
presence and estimated number of metastases. In modern practice,
grading and staging of tumors are being supplemented by
molecular characterization.
LABORATORY DIAGNOSIS OF CANCER:
I. HISTOLOGICAL AND CYTOLOGICAL METHODS
A. Histological methods
Histological examination is the most important method of diagnosis.
Proper diagnosis is aided by:
1- Availability of all relevant clinical data.
2- Adequate preservation and sampling of the specimen.
3- Frozen specimens are sometimes required for hormone or cell
surface receptor study.
A-Routine (H&E)
staining is the corner stone of tissue-based diagnosis. The process
stains thin tissue sections so that pathologists can visualize tissue
morphology. The process uses a haematoxylin dye to stain cell
nuclei (and other parts) blue and an eosin dye to stain other
structures pink or red. Properly applied, this technique provides
exceptional detail of tissue structure and the makeup of the cells.
This detail is required for tissue-based diagnosis, particularly in the
detection and classification of cancer.
The hematoxylin and eosin stain (H&E) is the most widely used stain in
histology and histopathology laboratories. When it is properly performed
it has the ability to demonstrate a wide range of normal and abnormal cell
and tissue components and yet it is a relatively simple stain to carry out
on paraffin or frozen sections. In histopathology a high proportion of
cases can be diagnosed by an experienced pathologist using an H&E stain
alone.

Quick frozen section
Quick frozen section is valuable tool used
to rapidly prepare slide for
microscopical examination, frozen section is used in clinical and research
settings, in surgical pathology frozen sections are routinely used for rapid
interoperative diagnosis, the slides prepared by frozen section can be
utilized for morphological, immunohistochemical and molecular method.
Clinical application of frozen section teqnique:
1-
Rapid diagnosis e.g., of breast cancer
2-
Define free margin of excision as in CA colon.
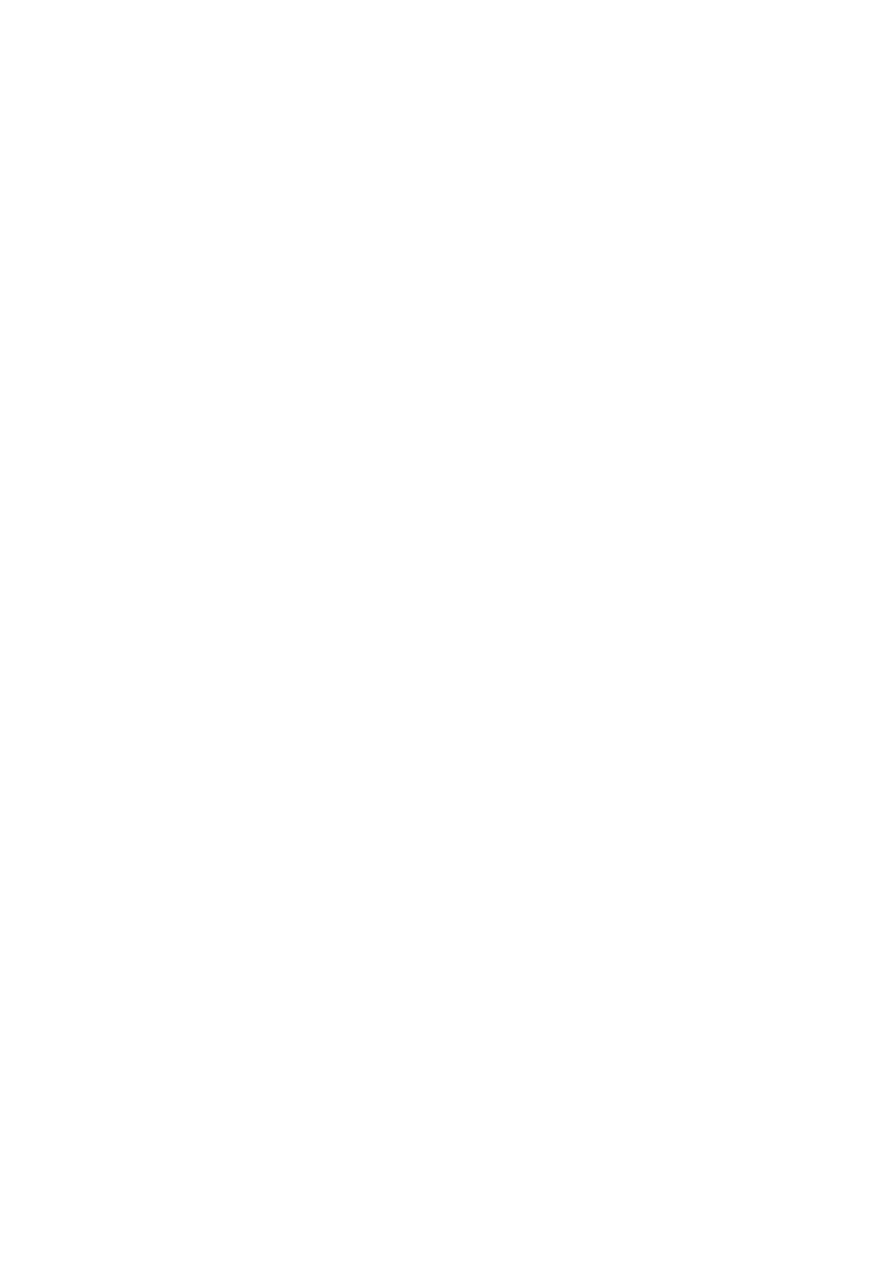
Electron microscope:
Amicroscope that uses abeam of accelerated electrons as asource of
illumination, electron microscope have a higher resolving power than
light microscope and can reveal the structure of smaller objects, cellular
organelles, there are wide range of application as using for differential
diagnosis between carcinoma and sarcoma in poorly differentiated
tumors.