1
GASTROINTESTINAL TRACT
ASS. PROF.DR. MAHA SHAKIR HASSAN
Lec.5
Colonic Diverticulosis
A diverticulum is a blind pouch leading off the alimentary tract, lined by
mucosa, that communicates with the lumen of the gut. Congenital
diverticula have all three layers of the bowel wall (mucosa, submucosa,
and most notably the muscularis propria) and are distinctly uncommon.
The prototype is Meckel diverticulum, described earlier.
Virtually all other diverticula are acquired and either lack or have an
attenuated muscularis propria. Acquired diverticula may occur anywhere
in the alimentary tract, but by far the most common location is the colon,
giving rise to diverticular disease of the colon, also called diverticulosis.
It is attributed to the consumption of a refined, low-fiber diet, resulting in
reduced stool bulk with increased difficulty in passage of intestinal
contents. Exaggerated spastic contractions of the colon isolate segments
of the colon in which the intraluminal pressure becomes markedly
elevated, with consequent herniation of the bowel wall through the
anatomic points of weakness.
MORPHOLOGY
Most colonic diverticula are small flasklike or spherical outpouchings,
usually 0.5 to 1 cm in diameter .
2
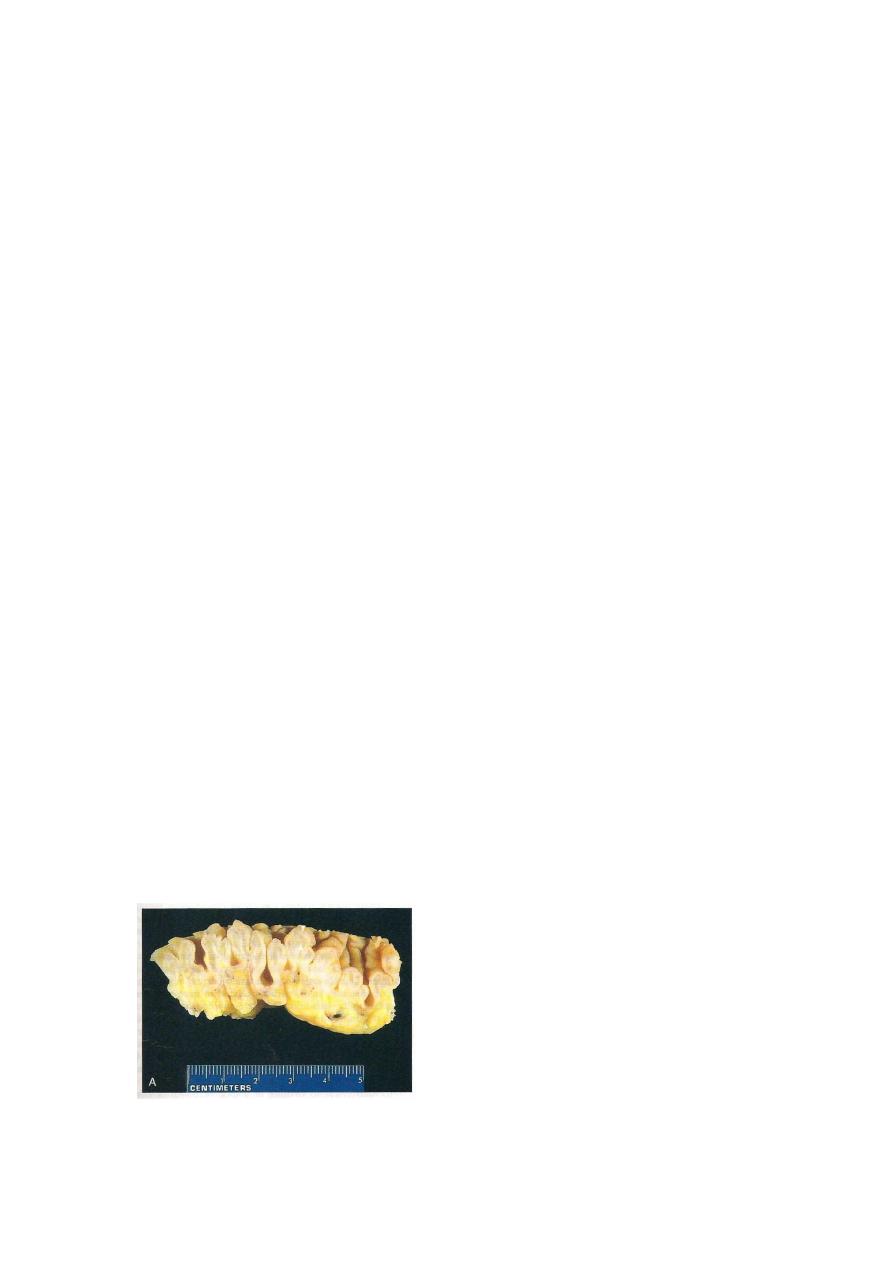
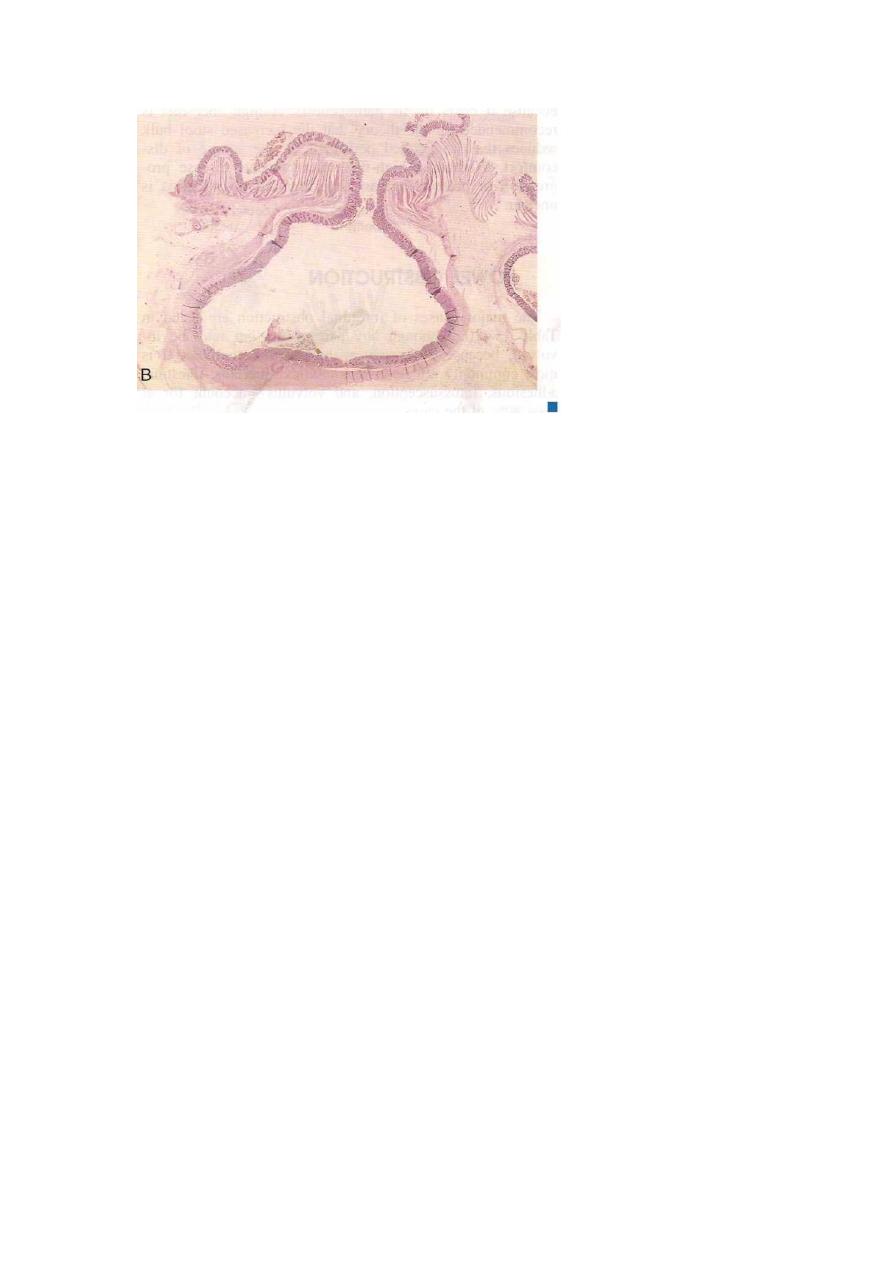
Diverticulosis. A, Section through the sigmoid colon showing multiple saclike diverticula protruding
through the muscle wall into the mesentery. The muscularis between the diverticular protrusions is
markedly thickened (arrowheads). B, Low-power ‘micrograph of diverticulum of the colon showing
protrusion of mucosa and submucosa through the muscle wall. A dilated blood vessel at the base of the
diverticulum was a source of bleeding.
TUMORS OF THE SMALL AND LARGE INTESTINES
Epithelial tumors of the intestines are a major cause of morbidity
and mortality worldwide.
The colon, including rectum, is host to more primary neoplasms
than any organ in the body.
Colorectal cancer ranks second to bronchogenic carcinoma among
the cancer killers. Adenocarcinoma constitute the vast majority of
colorectal cancers and represent 70% of all malignancies arising in
the GIT.
the small intestine is an uncommon for benign or malignant tumors
despite its great length. The classification of intestinal tumors is the
same for the
small and large intestine.
Terminology
A polyp is a tumorous mass that protrudes into the lumen of the gut;
traction on the mass may create a stalked, or pedunculated, polyp.
Alternatively, the polyp may be sessile, without a definable stalk.
3
Non-neoplastic Polyps
hvperplastic polyps, which are small (less than 5 mm in diameter). They
may occur singly but are more often multiple. Although they may be
anywhere in the colon, well over half are found in the rectosigmoid
region. Histologically, they contain abundant crypts lined by well-
differentiated goblet or absorptive epithelial cells, separated by a scant
lamina propria. The vast majority of hyperplastic polyps have no
malignant potential.
Neoplastic polyp
Adenomas
Adenomas are neoplastic polyps that range from small, often
pedunculated tumors to large lesions that are usually sessile.
40% to 50% after age 60.
Males and females are affected equally. There is a well- defined
familial predisposition.
All adenomatous lesions arise as the result of epithelial
proliferation and dysplasia, which may range from mild to so
severe as to represent transformation to carcinoma.
Adenomatous polyps are segregated into three subtypes on the
basis of the epithelial architecture:
•Tubular adenomas: mostly tubular glands.
•Villous adenomas: villous projections.
•Tubulovillous adenomas: a mixture of the above.
Tubular adenomas are by far the most common; 5% to 10% of
adenomas are tubulovillous, and only 1% are villous.
The malignant risk with an adenomatous polyp is correlated
with three interdependent features: polyp size, histologic
architecture, and severity of epithelial dysplasia, as follows:
• Cancer is rare in tubular adenomas smaller than 1 cm in
diameter.
• The likelihood of cancer is high (approaching 40%) in sessile

4
villous
adenomas
more
than
4
cm
in
diameter.
• Severe dysplasia, when present, is often found in villous areas.
MORPHOLOGY
Tubular adenomas
Histologically the stalk is covered by normal colonic mucosa
but the head is composed of neoplastic epithelium, forming
branching glands lined by tall, hyperchromatic, somewhat
disorderly cells, which may or may not show mucin secretion.
all degrees of dysplasia may be encountered, ranging up to
cancer confined to the mucosa (intramucosal carcinoma) or
invasive carcinoma-like masses.
Villous adenomas are larger and more ominous of the epithelial
polyps. They tend to occur in older persons, most commonly in
the rectum and rectosigmoid. but they may be located
elsewhere. They generally are sessile, up to 10 cm in diameter,
velvety or cauliflower extensions of the mucosa covered by
dysplastic, columnar epithelium. All degrees of dysplasia may
be encountered, and invasive carcinoma is found in up to 40%
of these lesions, the frequency being correlated with the size of
the polyp.
tubulovillous adenomos are composed of a broad mix of
tubular and villous areas. They are intermediate between the
tubular and the villous lesions in their frequency of having a
stalk or being sessile, their size, the degree of dysplasia, and the
risk of harboring intramucosal or invasive carcinoma.
5
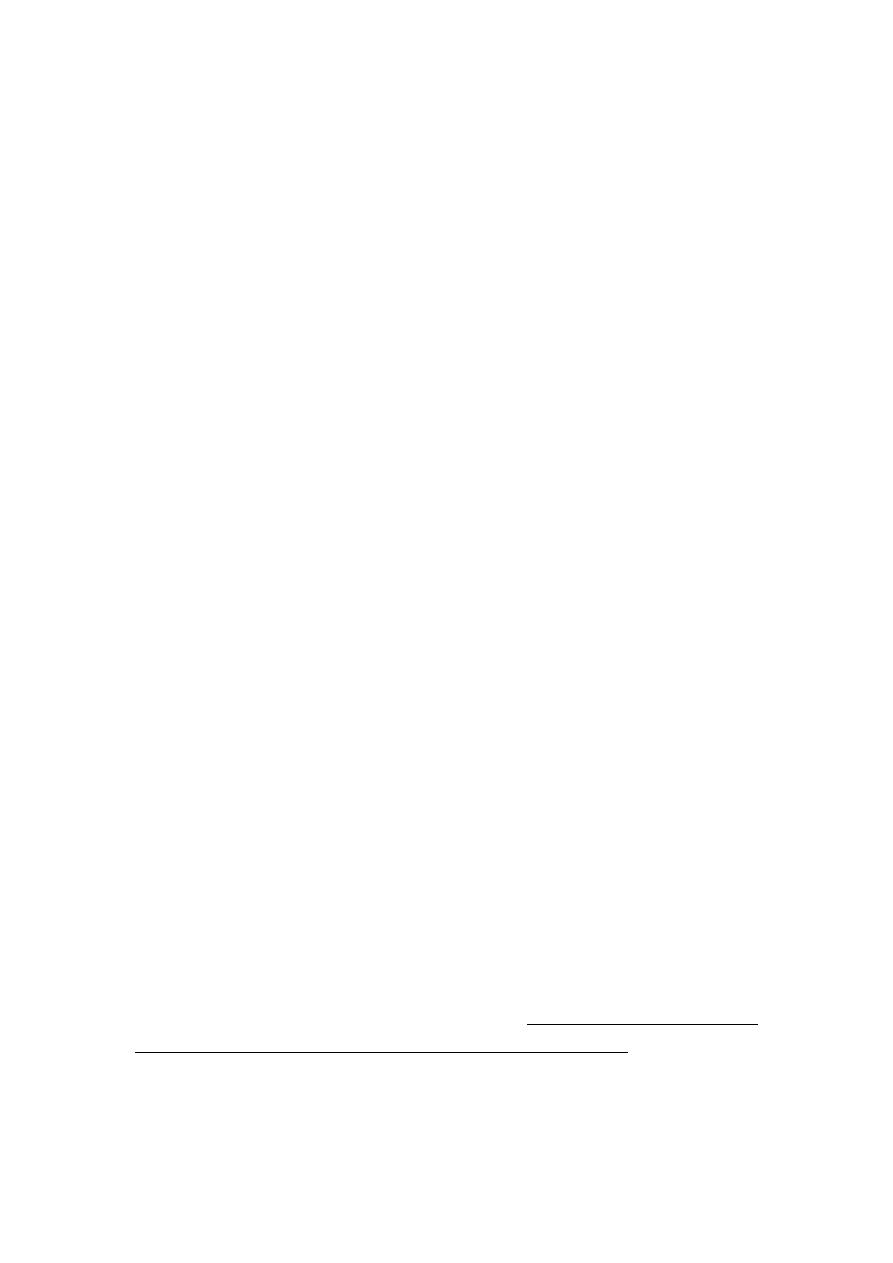
Colonic adenomas. A, Pedunculated adenoma (endoscopic view). B, Adenoma with a velvety surface.
C, Low-magnification photomicrograph of a pedunculated tubular adenoma.
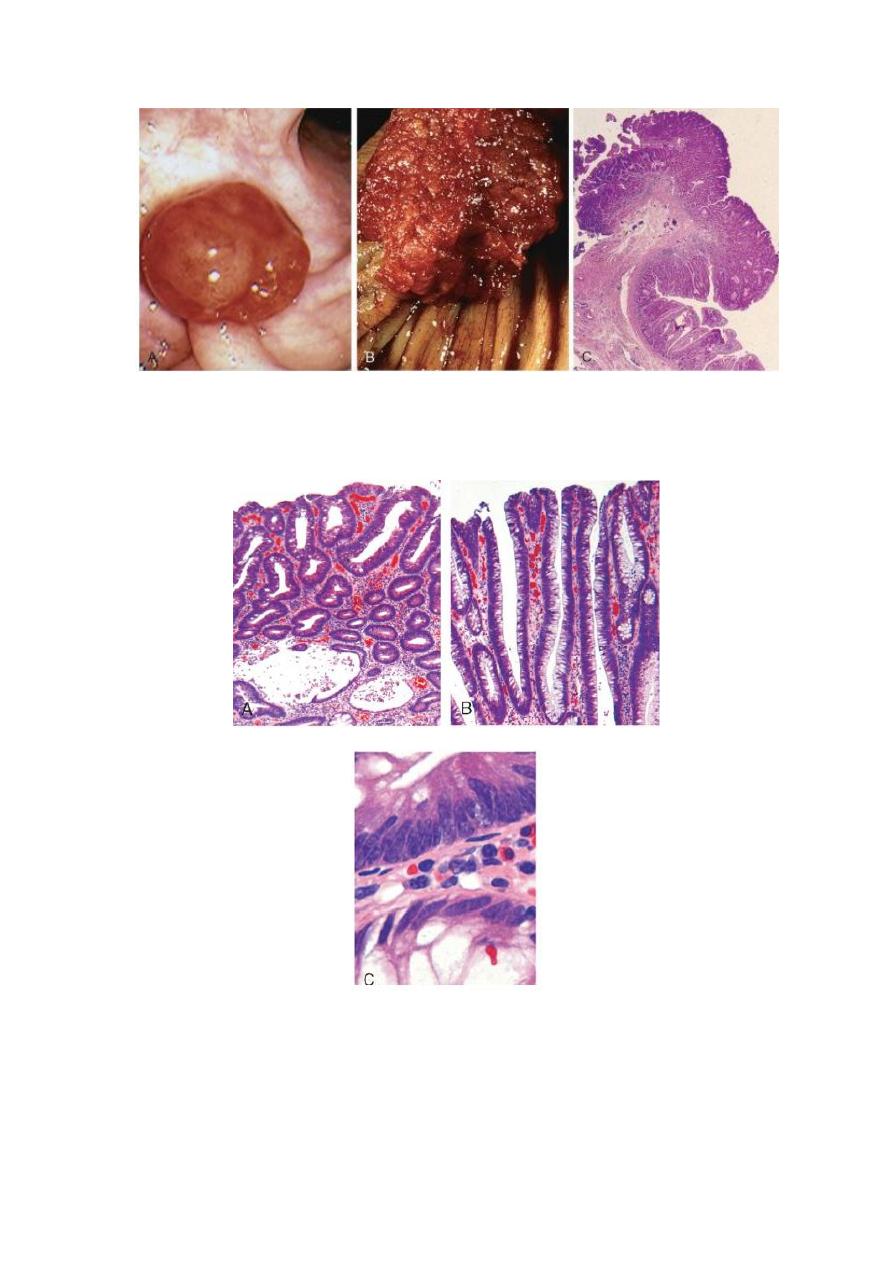
Histologic appearance of colonic adenomas. A, Tubular adenoma with a smooth surface and rounded
glands.B, Villous adenoma with long, slender projections that are reminiscent of small intestinal villi.
C, Dysplastic epithelial cells (top) with an increased nuclear-to-cytoplasmic ratio, hyperchromatic and
elongated nuclei, and nuclear pseudostratification. Compare to the nondysplastic epithelium below.

6
Familial Polyposis Syndromes
Familial polyposis syndromes are uncommon autosmal dominant
disorders.Their importance lies in propensity for malignant
transformation. In familial adenomatous polyp (FAP), patients typically
develop 500 to 2500 colonic adenomas that carpet the mucosal surface ; a
minimum number of 100 is required for the diagnosis. Multiple adenomas
may also be present elsewhere in the alimentary tract. Most polyps are
tubular adenomas; occasional polyps have villous features. Polyps usually
become evident in adolescence or early adulthood. The risk of colonic
cancer is virtually 100% by midlife, unless a prophylactic colectomy is
performed. The genetic defect underlying FAP has been localized to the
APC gene on chromosome(5q2).
Familial adenomatous polyposis.the surface is carpeted by innumerrable polypoid
adenomas