• Haemolytic anaemia
Haemolysis indicates that there is shortening of the
normal red cell lifespan of 120 days.
• The bone marrow may increase its output of red
cells six- to eightfold by increasing the proportion of
red cells produced, expanding the volume of active
marrow, and releasing reticulocytes prematurely
• Anaemia only occurs if the rate of destruction
exceeds this increased production rate .
• Red cell destruction overloads pathways for
haemoglobin breakdown in the liver, causing a
modest rise in unconjugated bilirubin in the blood
and mild jaundice.
• Increased reabsorption of urobilinogen from the gut
results in an increase in urinary urobilinogen . Red
cell destruction releases LDH into the serum
• The bone marrow compensation results in a
reticulocytosis, and sometimes nucleated red cell
precursors appear in the blood.
• Increased proliferation of the bone marrow can
result in a thrombocytosis, neutrophilia and, if
marked, immature granulocytes in the blood,
producing a leucoerythroblastic blood film.
• The appearances of the red cells may give an
indication of the likely cause of the haemolysis:
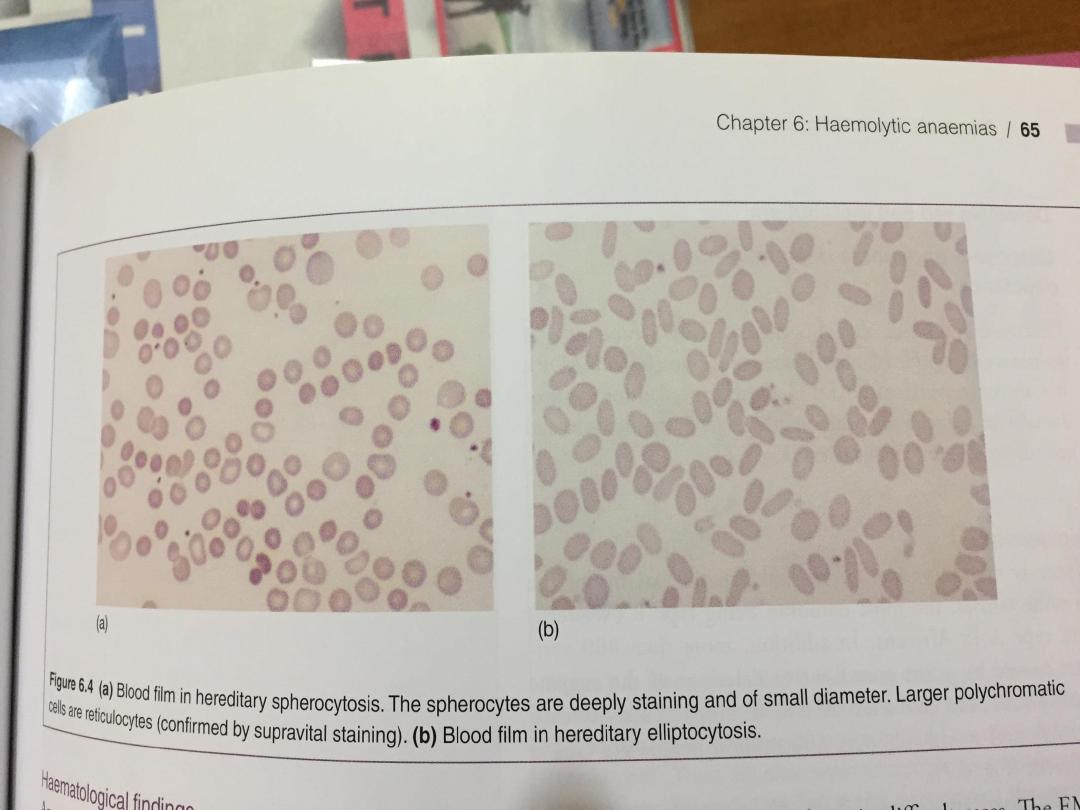
1- Spherocytes are small, dark red cells which
suggest autoimmune haemolysis or hereditary
spherocytosis.
2- Sickle cells suggest sickle-cell disease.
3- Red cell fragments indicate microangiopathic
haemolysis.
• The compensatory erythroid hyperplasia may give
rise to folate deficiency, with megaloblastic blood
features.

• Extravascular haemolysis
Physiological red cell destruction occurs in the
reticuloendothelial cells in the liver or spleen, so
avoiding free haemoglobin in the plasma.
In most haemolytic states, haemolysis is
predominantly extravascular
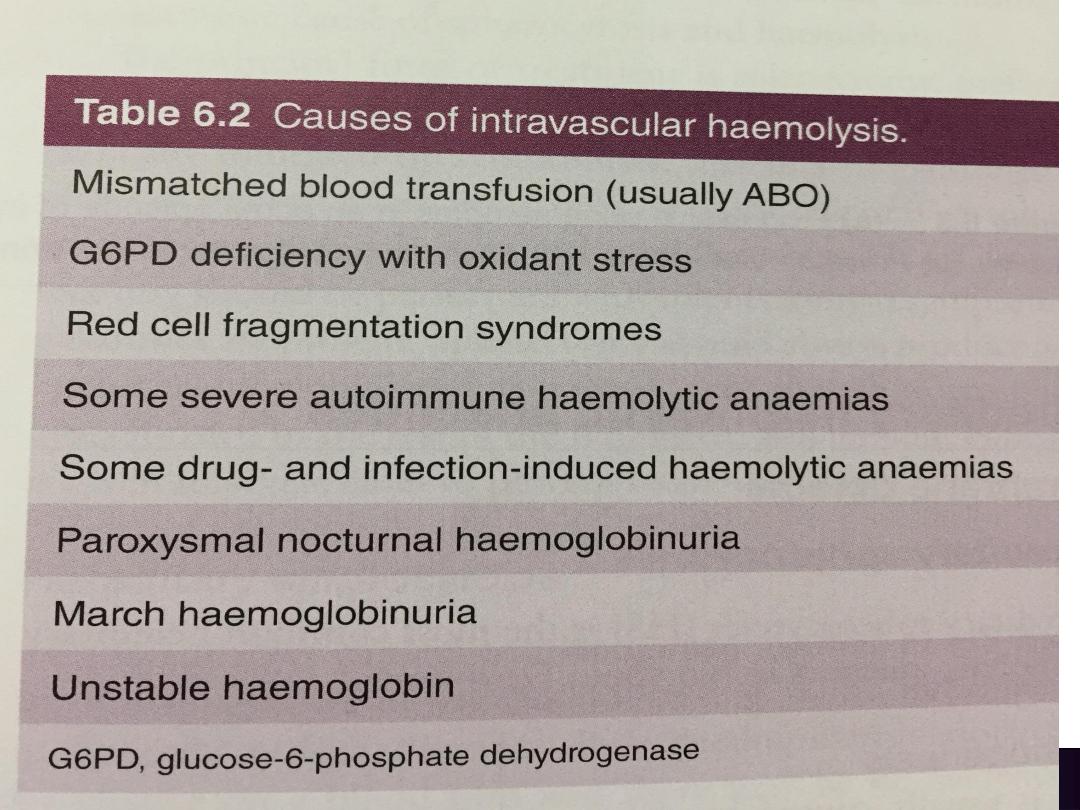
• Intravascular haemolysis
Less commonly, red cell lysis occurs within the
blood stream due to membrane damage by
complement (ABO transfusion reactions,
paroxysmal nocturnal haemoglobinuria),
• infections (malaria, Clostridium perfringens),
mechanical trauma (heart valves, DIC) or oxidative
damage (e.g. drugs such as dapsone and maloprim).
• When intravascular red cell destruction occurs, free
haemoglobin is released into the plasma. Free
haemoglobin is toxic to cells and binding proteins
have evolved to minimise this risk.
• If all the protective mechanisms are saturated, free
haemoglobin may appear in the urine
(haemoglobinuria). When fulminant, this gives rise
to black urine, as in severe falciparum malaria
infection
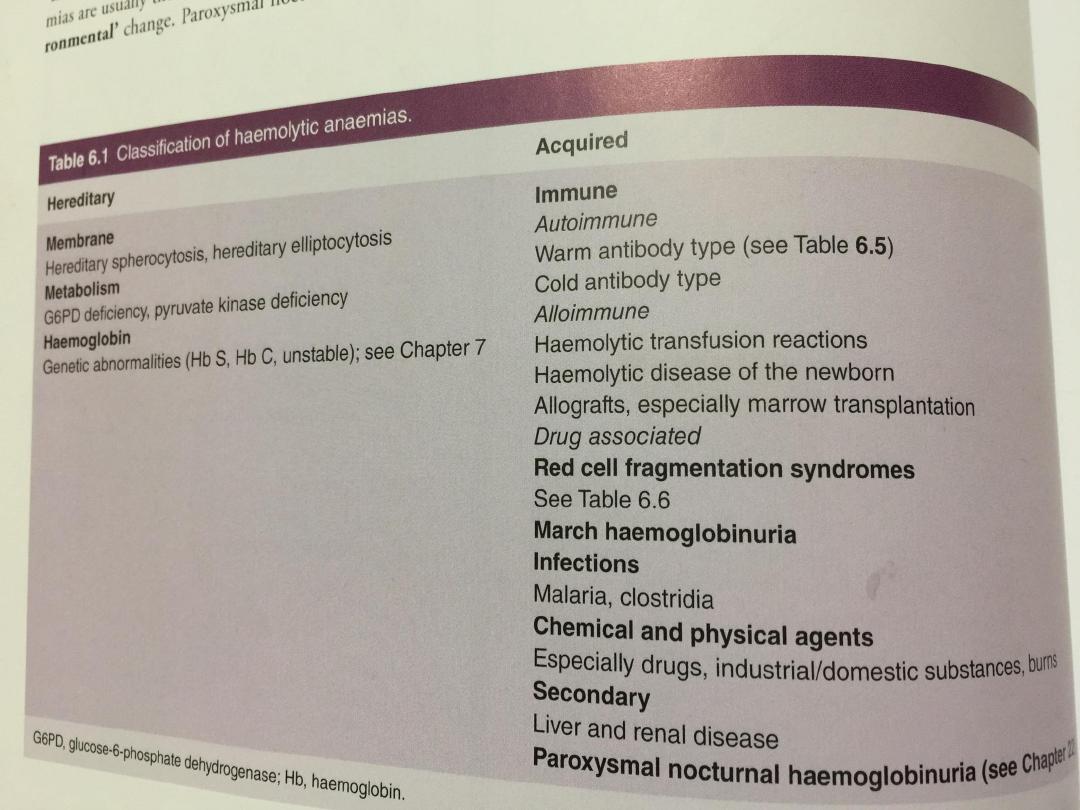
Red cell membrane defects
• Hereditary spherocytosis :This is usually inherited
as an autosomal dominant condition, although 25%
of cases have no family history and represent new
mutations. The incidence is approximately 1 : 5000
in developed countries
• The most common abnormalities are deficiencies of
beta spectrin or ankyrin The severity of
spontaneous haemolysis varies. Most cases are
associated with an asymptomatic compensated
chronic haemolytic state with spherocytes present
on the blood film, a reticulocytosis and mild
hyperbilirubinaemia.

• Pigment gallstones are present in up to 50% of
patients and may cause symptomatic cholecystitis.
The clinical course may be complicated by crises:
• A haemolytic crisis occurs when the severity of
haemolysis increases; this is rare, and usually
associated with infection.
• A megaloblastic crisis follows the development of
folate deficiency; this may occur as a first
presentation of the disease in pregnancy.
• An aplastic crisis occurs in association with
parvovirus B19 infection
Investigations
• The patient and other family members should be
screened for features of compensated haemolysis
This may be all that is required to confirm the
diagnosis. Haemoglobin levels are variable,
depending on the degree of compensation.
• The blood film will show spherocytes but the direct
Coombs test is negative, excluding immune
haemolysis.
• An osmotic fragility test may show increased
sensitivity to lysis in hypotonic saline solutions but
is limited by lack of sensitivity and specificity.

Management
• Folic acid prophylaxis, 5 mg daily, should be given for life.
• Consideration may be given to splenectomy, which improves
but does not normalise red cell survival.
• . Potential indications include moderate to severe haemolysis
with complications (anaemia and gallstones), although
splenectomy should be delayed until after 6 years of age in
view of the risk of sepsis
Hereditary elliptocytosis This term refers to a heterogeneous
group of disorders that produce an increase in elliptocytic red
cells on the blood film and a variable degree of haemolysis.
This is due to a functional abnormality of one or more anchor
proteins in the red cell membrane, e.g. alpha spectrin or
protein 4.1. Inheritance may be autosomal dominant or
recessive.

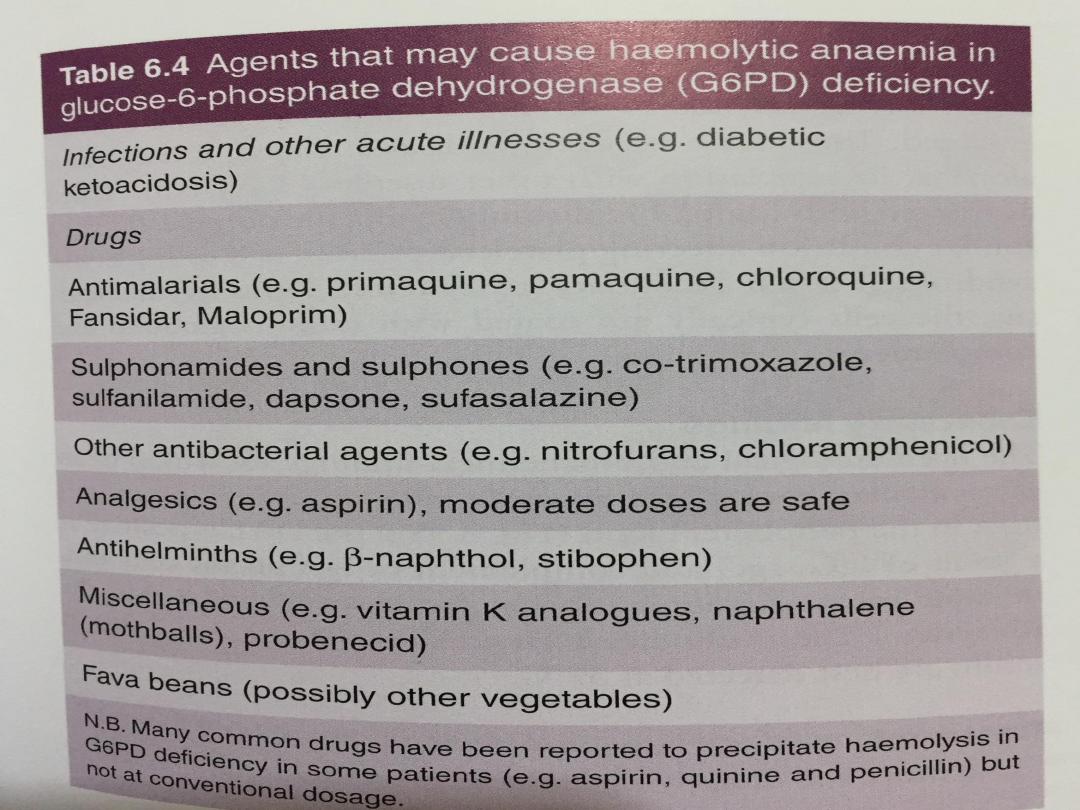
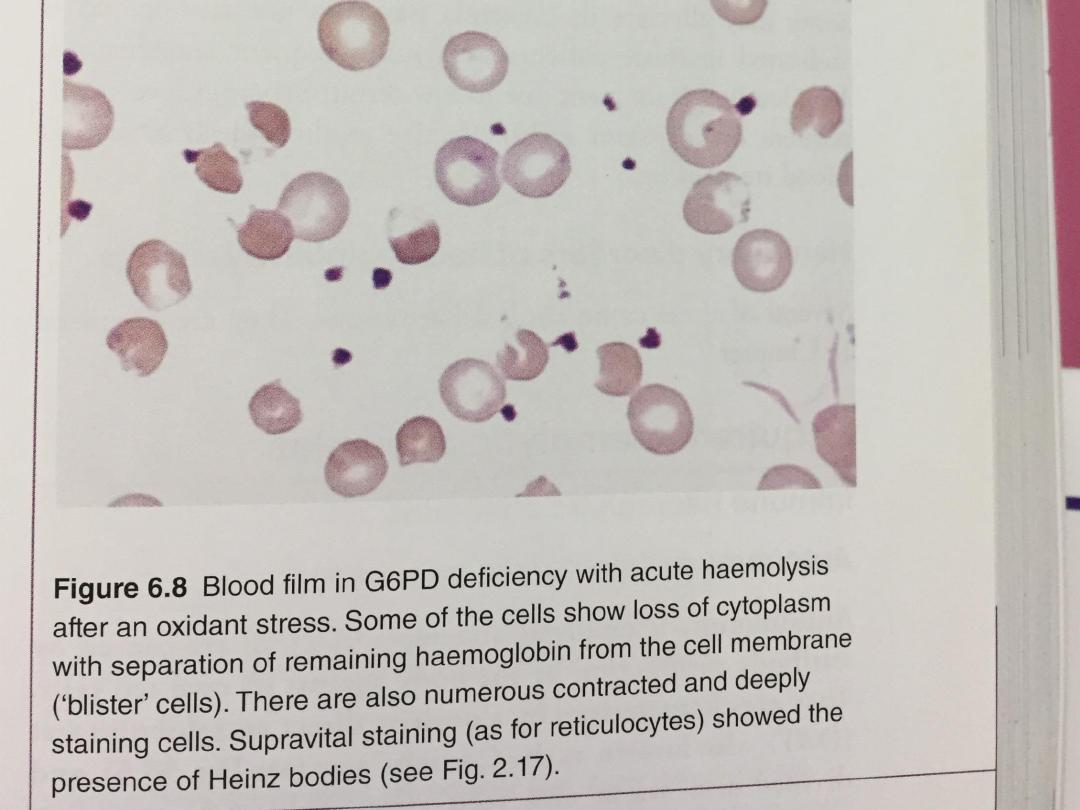
Red cell enzymopathies
1. Glucose-6-phosphate dehydrogenase deficiency
• The enzyme glucose-6-phosphate dehydrogenase
(G6PD) is pivotal in the hexose monophosphate
shunt pathway. Deficiencies result in the most
common human enzymopathy, affecting 10% of the
world’s population.
• The deficiency therefore affects males and rare
homozygous females but it is carried by females.

Clinical features
• Acute drug-induced haemolysis to (e.g.):
Analgesics: aspirin, phenacetin
Antimalarials: primaquine, quinine, chloroquine,
pyrimethamine
Antibiotics: sulphonamides, nitrofurantoin,
ciprofloxacin
Miscellaneous: quinidine, probenecid, vitamin K,
dapsone.
• Favism, i.e. acute haemolysis after ingestion of
broad beans (Vicia faba)

• G6PD level Can be indirectly assessed by screening
methods which usually depend upon the decreased ability
to reduce dyes
• Care must be taken close to an acute haemolytic episode
because reticulocytes may have higher enzyme levels and give
rise to a false normal result.
• Management aims to stop any precipitant drugs and treat
any underlying infection. Acute transfusion support may be
life-saving.
Pyruvate kinase deficiency
This is the second most common red cell enzyme defect. It
results in deficiency of ATP production and a chronic
haemolytic anaemia.
It is inherited as an autosomal recessive trait.