Common infectious diseases
Objectives:
1- These infections still common in our society, so should know the features of these infections, and differentiated from other diseases.2- to know the method of transmission of these diseases so can reduce or prevent this.
3- to know the effect of these infections on the fetus during pregnancy.
4- to know the preventive measures and encourage them.Measles (Rubeola)
ETIOLOGY:Measles virus is an RNA virus .
Humans are the only host of measles virus.
EPIDEMIOLOGY:
The age of peak incidence was 5-10yr.
TRANSMISSION:
The portal of entry of measles virus is through the respiratory tract or conjunctivae following contact with large droplets in which the virus is suspended.Patients are infectious from 3 days before the rash up to 4–6 days after its onset . Face-to fac contact is not necessary, because viable virus may be suspended in air for as long as 1 hr after the patient with the source case leaves a room.
Infants acquire immunity transplacentally from the mother and remain for the 1st. 4-6 mon. of life.
CLINICAL MANIFESTATIONS:
Measles consists of 4 phases: incubation period, prodromal illness, exanthematous phase, and recovery.1-incubation period 8–12 days from exposure to the prodromal phase.
2-prodromal phase: Lasting for 3-5 days and characterized by mild fever, conjunctivitis with photophobia, coryza, a prominent cough and increasing fever.
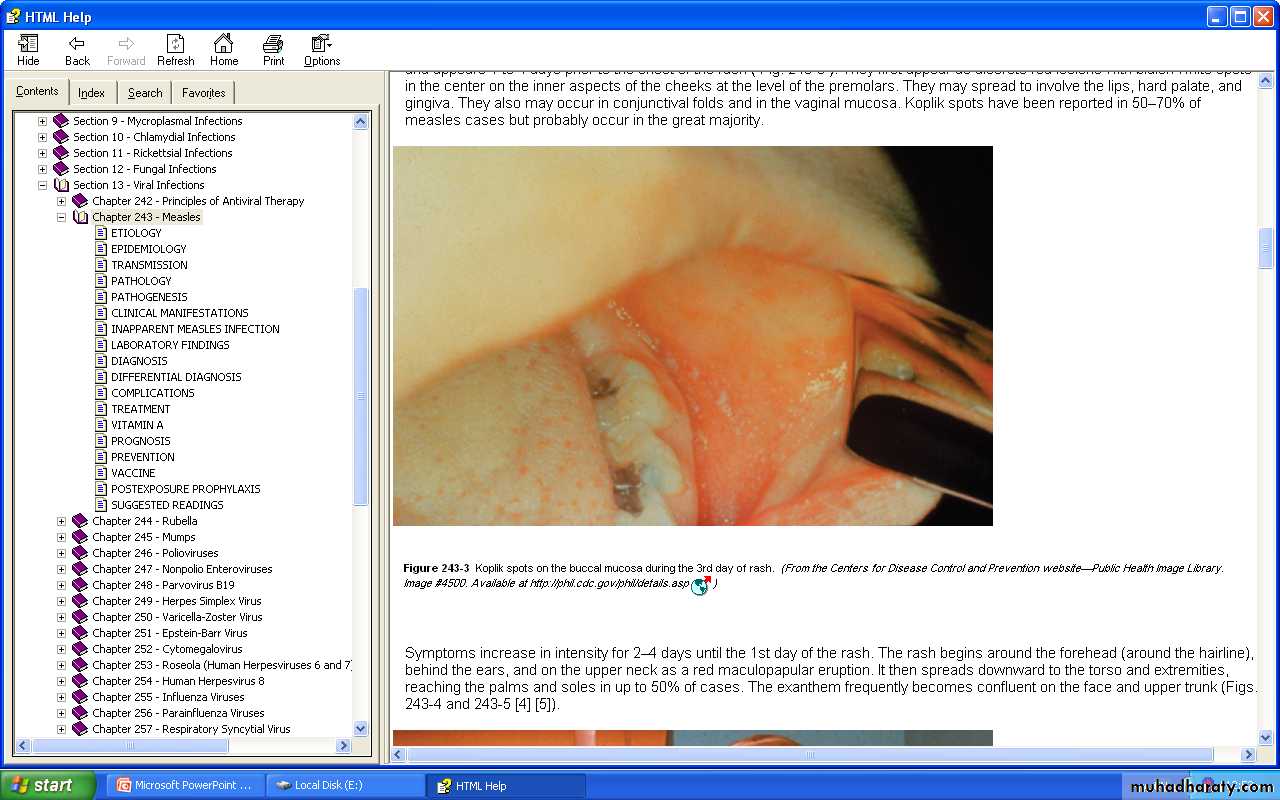
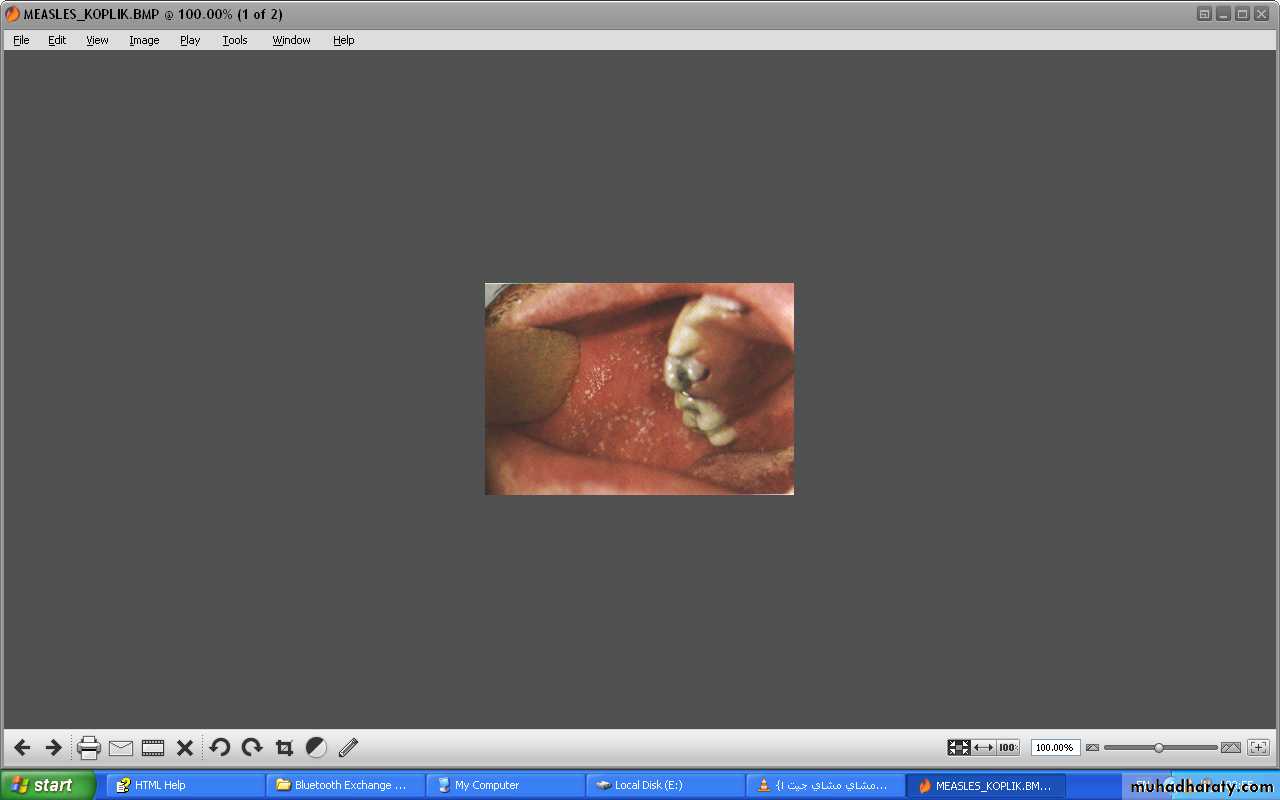
This stage precede the appearance of the enanthem, Koplik spots.
Koplik spots : is the pathognomonic sign of measles and appears 1 to 4 days prior to the onset of the rash.
These spots appear as red lesions with bluish white spots in the center on the inner aspects of the cheeks at the level of the premolars.
They appear and disappear quickly within 12-18hr.
The temperature increase rapidly as the rash appear and may reach 40-40.5 Ċ.
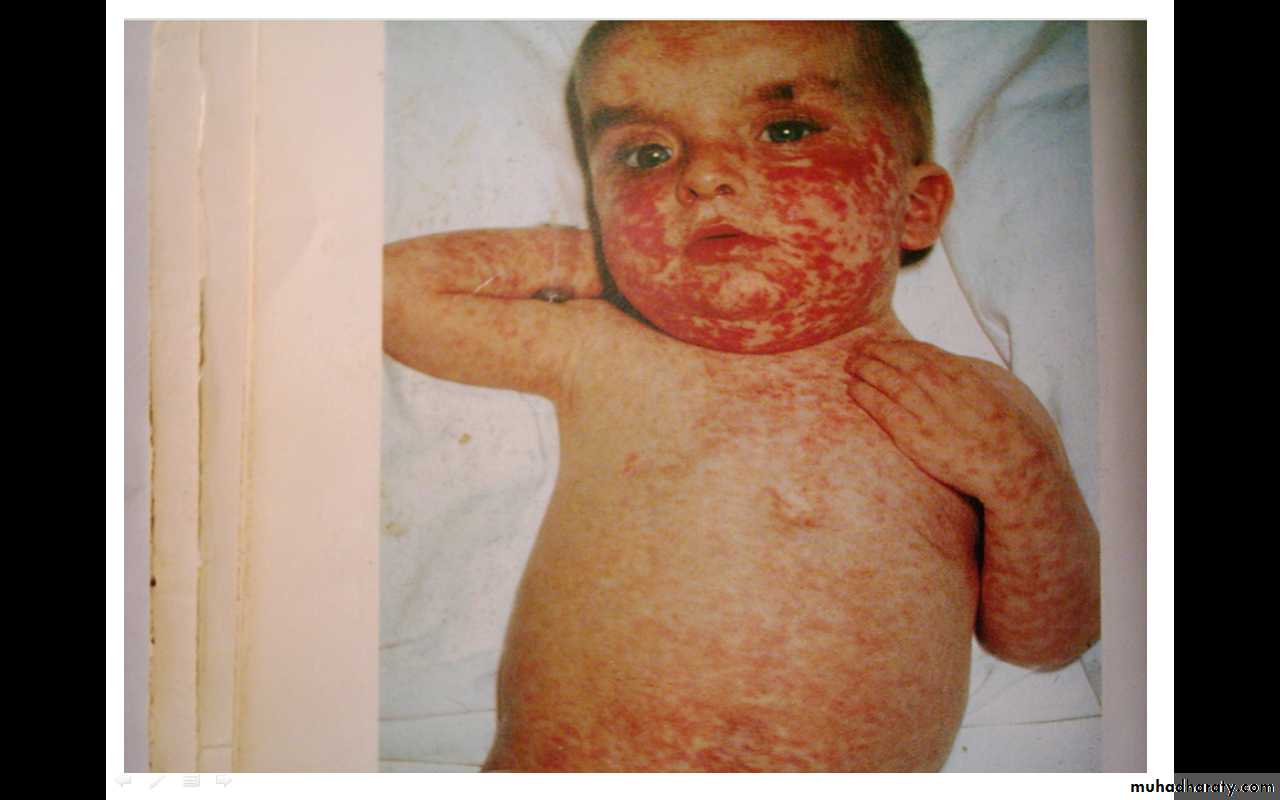
3-Exanthematous phase(rash)
The rash begins around the forehead, behind the ears, on the upper neck and upper chest as a red maculopapular eruption in the 1st 24hr. It then spreads downward to the abdomen,back and extremities through the next 24hr. to reach the feet at the 3rd day.After that, the rash fades in the same progression as it appear, leaving a fine desquamation of skin .
DIAGNOSIS.
A-clinically .B-Laboratory:
1-Serological test to identify immunoglobulin M (Ig M) antibodies in the serum. IgM Ab.appears 1-2 days after the onset of the rash and remain detectable for about 1mon.
Also detect seroconversion in IgG Ab. titer (4-fold rise in titer) between acute & convalescent serum specimens.
2-viral isolation by culture from tissue, blood, urine or respiratory secretions.
3-polymerase chain reaction(PCR).
4-Leukopenia.
COMPLICATIONS:A-Respiratory complications:1-Acute otitis media 2-Sinusitis and mastoiditis 3-Croup, tracheitis, and bronchiolitis 4-Pneumonia :is the most common cause of death in measles.
5-activation of pulmonary tuberculoses in individuals infected with Mycobacterium tuberculosis & suppress skin responsiveness to the tuberculin skin test.
B- gastrointestinal: diarrhea &vomiting, appendicitis.
C-Neurological :1-febrial seizures.
2- Encephalitis.
3-Subacute Sclerosing Panencephalitis (SSPE) : measles virus become latent intracellularly in the CNS following primary infection then reactivate after 7-10 yr. leading to neurodegenerative process.
D- Hemorrhagic or black measles.
E- keratitis , myocarditis & thrombocytopenia (rare complications).
TREATMENT :
1- supportive treatment :bed rest, adequate fluid intake, antipyretic for fever. For patient with respiratory tract involvement , airway humidification & oxygenation.2-Antibiotics for secondary bacterial infections(pneumenia, otitis media).
3-Vitamin A supplement: reduced morbidity & mortality in developing countries.Vitamin A therapy is indicated for all patients with measles. Vitamin A should be administered once daily for 2 days at doses of 200,000 IU for children 12 mo of age or older; 100,000 IU for infants 6 mo through 11 mo of age; and 50,000 IU for infants younger than 6 mo of age.In children with signs and symptoms of vitamin A deficiency, a 3rd dose is recommended 2 through 4 wk after the 2nd dose.
PREVENTION:1-Isolation from 7 days after exposure to 5 days after the onset of rash.
2-vaccination3-Postexposure prophylaxis: give immunoglobulin(Ig) which indicated in :
-susceptible household contacts of measles patients, especially infants <6 mo of age- pregnant women, and immunocompromised persons.
Rubella (German measles, 3-days measles)
ETIOLOGY :Rubella virus is an RNA virus.
EPIDEMIOLOGY.
Human is the only known host. It spread by oral droplets or transplacentally to the fetus causing congenital infection.The period of highest communicability is from 5 days before to 6 days following appearance of the rash.
CLINICAL MANIFESTATIONS
Postnatal infection (acquired rubella)-Incubation period 14–21 days.
- Prodromal phase: low-grade fever, sore throat, conjunctivitis without photophobia, headache, malaise& anorexia. The most characteristic sign is lymphadenopathy mostly Suboccipital, postauricular, and anterior cervical lymph nodes.
This LAP evident at least 24hr.befor rash & remain for 1wk.or more .
- Rash : it begins on the face& neck as small, pink macules that coalesce & spread to involve the trunk & extremities. Examination : petechial hemorrhages on the soft palate.
The duration of the rash is 3 days, and it usually resolves without desquamation.
Fever is mild or absent during appearance of rash.
DIAGNOSES.
1-Leukopenia, neutropenia, and mild thrombocytopenia.2- Serology : the diagnostic test is rubella immunoglobulin M (IgM) enzyme immunosorbent assay.
3- Isolation of the virus .
COMPLICATIONS :
1- Postinfectious thrombocytopenia :It manifests about 2 wk following the onset of the rash with petechiae, epistaxis, gastrointestinal bleeding, and hematuria. It is usually self-limited.2- Arthritis: occurs especially in women. It begins within 1 wk of onset of the exanthem and classically involves the small joints of the hands. It is self-limited and resolves without sequelae.
3- Encephalitis is the most serious complication of postnatal rubella.
4- Guillain-Barré syndrome and peripheral neuritis.5- Progressive rubella panencephalitis (PRP).
6- Myocarditis (rare complication).
Congenital Rubella Syndrome.
It is occur when non-immune mother acquired rubella in early pregnancy . Rubella virus can cross the placenta, infect the fetus & result in death of concept or birth of an infant with congenital rubella .The risk of congenital defects was 90% for maternal infection before 11wk. of gestation, 33% at 11-12wk., 11% at 13-14 wk. Defects occurring after 16wk. of gestation are uncommon.
Clinically:
- low birth wt.(IUGR)
- Hepatosplenomegaly , jaundice, petechia & purpura.
- Retinopathy, microphthalmia, corneal opacity, glucoma, cataract(unilateral or bilateral), sensory neural hearing loss.
- myocarditis, cardiac defects(PDA, pulmonary artery stenosis)
- microcephaly, mental retardation, meningoencephalitis.
• -pneumonia, hepatitis, thrombocytopenia & anemia .
Late-onset manifestations of CRS: PRP, diabetes mellitus, thyroid dysfunction, and glaucoma and visual abnormalities.
Diagnosis of CRS:
1- History of rubella in the mother during pregnancy.2- isolation of virus by serological test from urine, throat & CSF.
3- IgM antibody assay .4- polymerase chain reaction .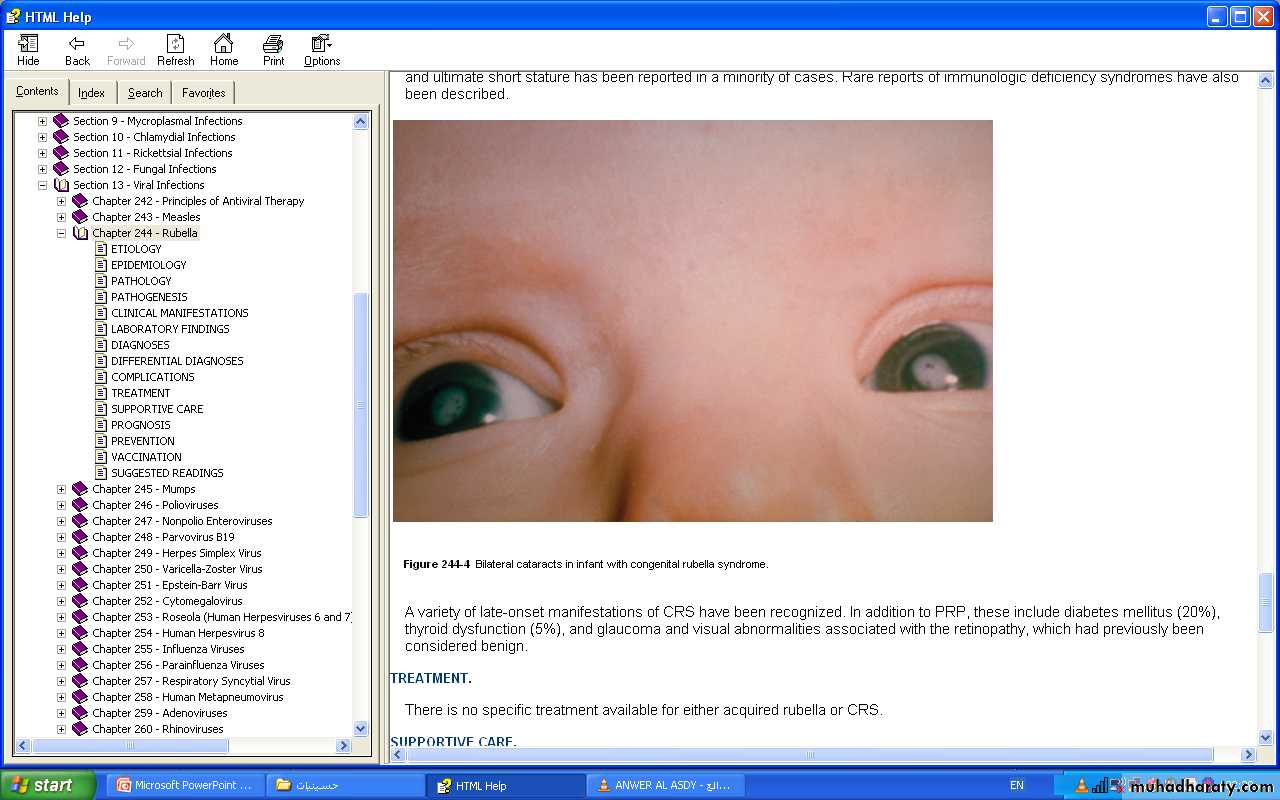
TREATMENT:
There is no specific treatment available for either acquired rubella or CRS.SUPPORTIVE CARE. Postnatal rubella → Antipyretics and analgesics. Intravenous immunoglobulin or corticosteroids can be considered for severe, non-remitting thrombocytopenia.
Management of children with CRS is more complex and requires pediatric, cardiac, audiologic, ophthalmologic, and neurologic evaluation and follow-up because many manifestations may not be readily apparent initially or may worsen with time.