By:
Ayat Mehdi & Huda Adil
Supervisor:
Dr.Mohanned Al Sherify
Acute Cholecystitis
Anatomy and physiology of Biliary treeThe gallbladder lies on the underside of the liver in the main
liver scissura at the junction of the right and left lobes of the
liver. The relationship of the gallbladder to the liver varies
between being embedded within the liver substance to being
suspended by a mesentry.
It is a pear-shaped structure, 7.5–12 cm long, with a normal capacity of about 25–30 mL. The anatomical divisions are a fundus, a body and a neck that terminates in a narrow infundibulum.
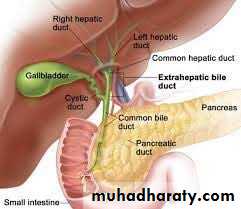
The cystic duct is about 3 cm in length but the length,is variable. The lumen is usually 1–3 mm in diameter.
The cystic duct joins the supraduodenal segment of the common hepatic
duct in 80% of cases.
The common hepatic duct is usually less than 2.5 cm long
and is formed by the union of the right and left hepatic ducts.
The common bile duct is about 7.5 cm long and formed by the
junction of the cystic and common hepatic ducts. It is divided
into four parts:
*The supraduodenal part
*The retroduodenal part
*The infraduodenal part
*The intraduodenal part which passes obliquely into the 2nd part of duodenum
And surrounded by the sphincter of oddi.
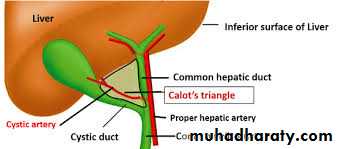
The cystic artery, a branch of the right hepatic artery, usually
arises behind the common hepatic duct,Occasionally, an accessory cystic artery arises from the gastroduodenalartery.
Calots traingle is the area bounded superiorly by:the inferior surface of the liver, laterally by the cystic duct and the medial border of the gallbladder and medially by the common hepatic duct.
It is an important surgical landmark as the cystic artery usually can be found within its boundaries.
The most dangerous anomalies are where the hepatic artery takes a tortuous course on the front of the origin of the cystic duct or the right hepatic artery.
Surgical physiology
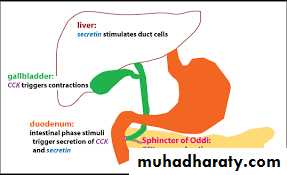
Bile is produced by the liver and stored in the gallbladder,from which itis released into the duodenum,Its composed of 97% water,1-2% bile
salts,phospholipids,cholestrol,bilirubin.
About 95% of bile salts are reabsorbed in the terminal ileum.
The rate of secretion is controlled by cholecystokinin, which is released from doudenal mucosa.
Function of the gallbladder
1-Storage of bile2-concentration of bile by active absorption of water, sodium chloride and bicarbonate.
3-secretion of mucus approximately 20 mL is produced per day.GALLSTONES(cholelithiasis)
Gallstones are the most common biliary pathology.It affect 10-15% of population.They are asymptomatic in about 80% ,about 1-2% of asymptomatic become
symptomatic requiring cholecystectomy ,there are 3 types, pigmented
(brown and black) ,cholestrol and mixed.
80% are cholestrol or mixed stones , cholestrol stones contain cholestrol
plus calcium salts, bile acids, bile pigments and phospholipids.
Pigmented gall stones contain less than 30% cholestrol.Black stones
associated with hemolysis, sickle cell anemia or hereditary spherocytosis.Brown stones are rare in the gallbladder , they are related to bile stasis and infected bile.
Pathogenesis of cholelithiasis
1-Bile is supersaturated with cholestrol or bile acid concentrations are low, unstable phospholipds vesicles form , from which cholestrol crystals may
nucleate , and stones may form .
2-Obeisty , high calorie diet and certain medications(cocp) can increase the
secretion of cholestrol and supersaturate bile , increasing the lithogenicityof bile.
3-Abnormal emptying of the gallbladder may promote the aggregation of
cholestrol crystals.Clinical presentation:
1- Gall stones may remain asymptomatic, being detected incidentallyas imaging is performed for other symptoms.
2-Symptomatic patient complain from severe right upper quadrant or epigastric pain lasting for minutes or several hours starts at the night awaking the patient , which may radiate to the back or chest , colicky(in 10-25% of patients) but more often is dull and constant associated with nausea and vomiting.Minor episodes occur during the day .
3- Dyspepsia , flatulence, food intolerance particularly to fats and some alteration in bowel frequency.
Patient may have several episodes of this nature over a period of a few
weeks and then no trouble for some months.4- Jaundice may result if the stone migrates from the gallbladder and
obstructs the common bile duct. Rarely, a gallstone can lead to bowelobstruction (gallstone ileus).
*Symptoms associated with fever and leukocytosis shlould raise the suspicion of acute cholecystitis.
Differential diagnosis
Common1- Appendicitis
2- Perforated peptic ulcer
3- Acute pancreatitis
Rare
1- Acute pyelonephritis
2- Myocardial infarction
3- Pneumonia – right lower lobe
Diagnosis:
1-History and physical examination plus CBC , In the acute phase the patient
may have right upper quadrant tenderness that is exacerbated during
inspiration by the examiner’s right subcostal palpation (Murphy’s sign).
A positive Murphy’s sign suggests acute inflammation
and may be associated with a leukocytosis and moderately
elevated liver function tests.
2-U/S showing the size of the gallbladder , the presence of stones
or polyps and the thickness of the wall measured(5-6mm and more as normally 3mm) ,the presence of inflammation around the gallbladder and the size of the common bile duct.
Other modalities including
1- MRCP : provides excellent imaging of the gall bladder and biliary , safe in pregnancy but its expensive and contraindicated in claustrophobia and morbid obeisty.2- Endoscopic retrograde cholangiopancreatography(ERCP) :This technique is used for both daignostic and therapeutic modality.
3- plain radiograph of the gallbladder will
show radiopaque gallstones in 10% of patients.
Rarely, the centre of a stone may contain radiolucent gas in
a triradiate or biradiate fissure and this gives rise to characteristic
dark shapes on a radiograph: the ‘Mercedes–Benz’ or
‘seagull’ sign.It shows the rare cases of gall bladder calssification(Porcelain
gall bladder)
4- Percutaneous transhepatic choleangiography : Its shows anatomy and biliary stricture.
Treatment
Most consider that it is safe to observe patients with asymptomatic
gallstones, with cholecystectomy reserved for patients who develop
symptoms or complications.
Indication for surgery in asymptomatic patient:
1-Diabetic patient. 2-Patients with hemolytic anemia. 3-Patient undergoing bariatric surgery for morbid obeisty.For symptomatic patient , cholecystectomy is the treatment of choice.
in more than 90% of cases, the symptoms of acute cholecystitis subsidewith conservative measures which include :
1- Nil per mouth (NPO) and intravenous fluid administration
until the pain resolves.2- Administration of analgesics.
3- Administration of antibiotics. A broad-spectrum antibiotic effective
against gram-negative aerobes is most appropriate (e.g. cefazolin,
cefuroxime or ciprofloxacillin).
3- When the temperature, pulse and other physical signs show that the
inflammation is subsiding, oral fluids are reinstated, followed by a regular
diet.
If jaundice is present MRCP is performed to exclude
choledocholithiasis. If there is any concern regarding the
diagnosis or presence of perforation CT should be performed.
Cholecystectomy may be performed on the next available list, or the
patient may be allowed home to return later when the inflammation has
completely resolved.
The timing of surgery in acute cholecystitis remains
controversial, with many units favouring an early intervention
within the first week (5-7 days) whereas others suggest that a
delayed approach within 6 weeks for the inflammation to subside is
preferable.
Complications
In the gallbladder:1-Biliary colic.
2-Acute cholecystitis .
3-Chronic cholecystitis.
4-Empyema of the gallbladder.
5-Mucocele.
6-Perforation.
In the bile duct:
1-Biliary obstruction.
2-Acute cholangitis.
3-Acute pancreatitis.
**In the intestine cause (gallstone ileus)
Empyema of the Gall bladder
Empyema may be a sequel to acute cholecystitis or the result
of a mucocoele becoming infected. The gallbladder is
distended with pus.
The optimal treatment is drainage (cholecystostomy) and,
later,cholecystectomy.
Acalculous cholecystitis
Acute and chronic inflammation of the gallbladder can occurin the absence of stones and give rise to a clinical picture
similar to that of calculous cholecystitis. Some patients have
non-specific inflammation of the gallbladder, whereas others
have one of the cholecystoses . Acute acalculous cholecystitis is
particularly seen in :
1- critically ill patients 2- Those recovering from major
surgery, trauma and burns.
The cholecytoses (cholestrosis,polyposis,Addenomyosis,cholecystitis glandularis proliferans):
There is chronic inflammatory changes with hyperplasia of all tissue elements.
Cholestrosis (strawberry gallbladder)
In the fresh state, the interior of the gallbladder looks like a strawberry.
:Cholesterol polyposis of the gallbladder
Ultrasound may show a non-mobile defect in the gallbladderlumen which does not exhibit an associated acoustic shadow.
The differential is an adenomatous polyp, and interval
follow-up is indicated to ensure stability. Surgery is only
advised if there is a diagnostic dilemma.
Cholecystectomy
Preparation for cholecystectomy:1- Full blood count
2- Renal profile and liver function tests
3- Prothrombin time
4- Chest x-ray and electrocardiogram (if over 45 years or medically indicated)
5- Antibiotic prophylaxis
6- Deep vein thrombosis prophylaxis
7- Informed consent
Laproscopic Cholecystectomy
The preparation and indications for cholecystectomy arethe same whether it is performed by laparoscopy or by open
techniques. Laparoscopic cholecystectomy is the procedure of
choice for the majority of patients with gallbladder disease.
Serious complications are :
1-Access complications.
2-Bile duct injuries.
If either a visceral or bile duct injury is suspected , conversion to open technique is recommemded.
Open cholecystectomy
For patients in whom1- a laparoscopic approach is not indicated or in
2- whom conversion from a laparoscopic approach is
required, an open cholecystectomy is performed.
Indicatios for choledocotomy:
1-A palpable stone in the common bile duct.2-Jaundice.
3-A dilated common bile duct.
4-Abnormal liver fuction test(raised AKP).
