


Working length(W.L.) determination
Determination of an accurate working length is one of the most important steps of endodontic therapy. The cleaning, shaping and obturation of root canal system cannot be accomplished accurately unless working length is determined precisely.No. 2
Generally, it is believed that the apical termination of the treatment should be at the apical constriction because this location indicates the junction between the periodontal and pulpal tissues. The working length may be determined in a number of ways but, whatever method is used, it must be accurate, repeatable and carried out easily.
No. 3
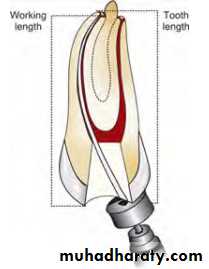
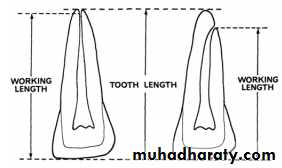
DEFINITIONSworking length is defined as “The distance from a coronal reference point to a point at which canal preparation and obturation should terminate”
No. 4
Reference point: is that site on occlusal or the incisal surface from which measurements are made.A reference point is chosen which is stable and easily visualized during preparation. Usually this is the highest point on incisal edge of anterior teeth and buccal cusp of posterior teeth. Reference point should not change between the appointments.


No. 5
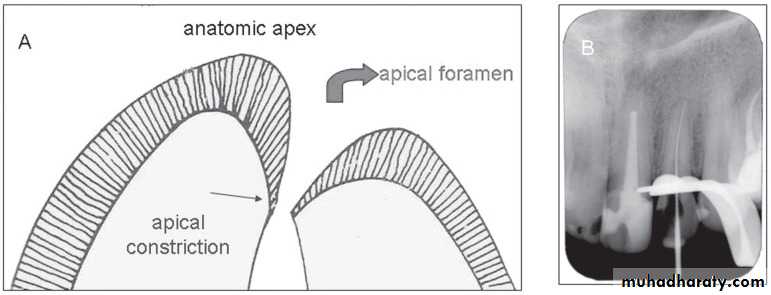
The radiographic apex is the tip or end of the root determined radiographicallyThe anatomic apex is the tip or the
end of the root determined morphologically,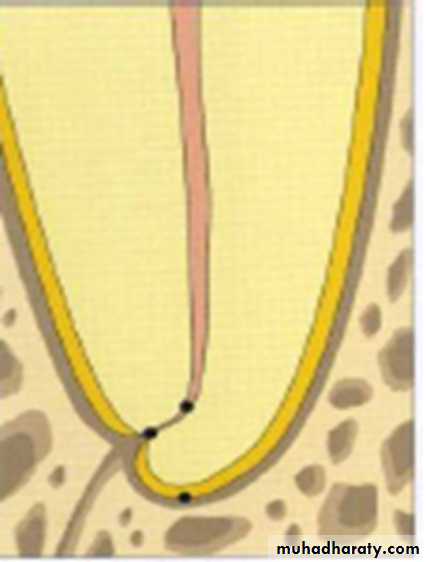


No. 6
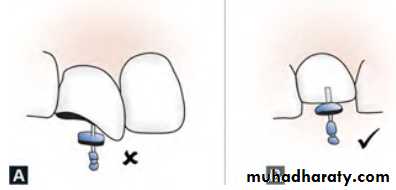
The apical constriction is the apical portion of the root canal having the narrowest diameter. This position may vary but is usually 0.5 to 1.0 mm short of the center of the apical foramen.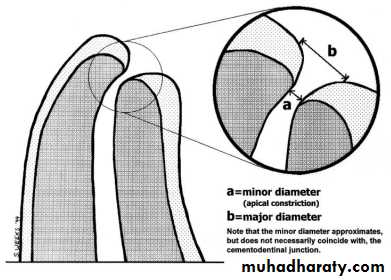
No. 7
SIGNIFICANCE OF WORKING LENGTH1. Working length determines how far into canal, instruments can be placed and worked.2. It affects degree of pain and discomfort which patient will experience following appointment by virtue of over and under instrumentation.3. If placed within correct limits, it plays an important role in determining the success of treatment.
No. 8
• Failure to accurately determine and maintain working length may result in length being over than normal which will lead to postoperative pain, prolonged healing time and lower success rate
because of incomplete regeneration
of cementum, periodontal ligament
and alveolar bone.
No. 9

• When working length is made short of apical constriction it may cause persistent discomfort because of incomplete cleaning and underfilling. Apical leakage may occur into uncleaned and unfilled space short of apical constriction. It may support continued existence of viable bacteria and contributes to the periradicular lesion and thus poor success rate.

No. 10
METHODS OF DETERMINING WORKING LENGTHTo achieve the highest degree of accuracy in working length determination, a combination of several methods should be used. This is most important in canals for which working length determination is difficult.
1- Determination of Working Length by Radiographic Methods:
The following items are essential to perform this procedure:1. Good, undistorted, preoperative radiographs showing the total length and all roots of the involved tooth.2. Adequate coronal access to all canals.3. An endodontic millimeter ruler.4. Working knowledge of the average length of all of the teeth.5. A definite, repeatable plane of reference to an anatomic landmark on the tooth.
No. 11
It is imperative that teeth with fractured cusps or cusps severely weakened by caries or restoration be reduced to a flattened surface, supported by dentin.Failure to do so may result in cusps or weak enamelwalls being fractured between appointments. Thus, the original site of reference is lost. If this fracture goes unobserved, there is the probability of over instrumentation and overfilling, particularly when anesthesia is used.
No. 12
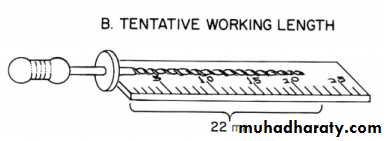
Method:1. Measure the tooth on the preoperative radiograph.2. Subtract at least 1.0 mm “safety allowance” for possible image distortion or magnification.3. Set the endodontic ruler at this tentative working length and adjust the stop on the instrument at that level .4. Place the instrument in the canal until the stop is at the plane of reference unless pain is felt (if anesthesia has not been used), in which case, the instrument is left at that level and the rubber stop readjusted to this new point of reference.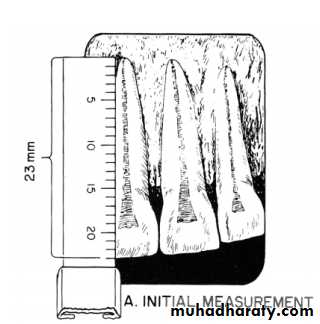
No. 13
5. Expose, develop, and clear the radiograph.6. On the radiograph, measure the difference between the end of the instrument and the end of the root and add this amount to the original measured length the instrument extended into the tooth. If, the exploring instrument has gone beyond the apex, subtract this difference.7. From this adjusted length of tooth, subtract a 1.0 mm “safety factor” to conform with the apical termination of the root canal at the apical constriction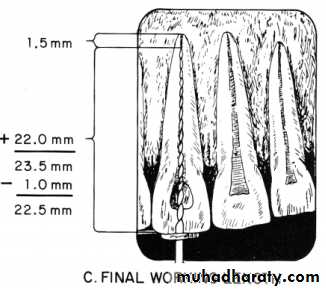
No. 14
8. Set the endodontic ruler at this new corrected length and readjust the stop on the exploring instrument.9. Because of the possibility of radiographic distortion, sharply curving roots, and operator measuring error, a confirmatory radiograph of the adjusted length is highly desirable.
10. When the length of the tooth has been accurately confirmed, reset the endodontic ruler at this measurement.11. Record this final working length and the coronal point of reference on the patient’s record.

No. 15
Advantages of radiographic methods of working lengthdetermination1. One can see the anatomy of the tooth2. One can find out curvature of the root canal3. We can see the relationship between the adjacent teeth and anatomic structures.Disadvantages of radiographic methods of working length determination1. Varies with different observers2. Superimposition of anatomical structures3. Two-dimensional view of three-dimensional object4. Risk of radiation exposure5. Time consuming6. Limited accuracy
No. 16
2- Non-radiographic Methods
1. Digital tactile sense: In this clinician may see an increase in resistance as file reaches the apical 2-3 mm.Advantages• Time saving• No radiation exposure.Disadvantages• Does not always provide the accurate readings• In case of narrow canals, one may feel increased resistance as file approaches apical 2-3 mm.• In case of teeth with immature apex instrument can go periapically.
No. 17
2. Periodontal sensitivity test: This method is based on patient’s response to pain (no anesthesia is given). But this method does not always provide the accurate readings, for example, in cases of canal with necrotic pulp, instrument can pass beyond apical constriction and in case of vital or inflamed pulp, pain may occur several mm before periapex is crossed by the instrument.
Any method of working length determination, based on the patient’s response to pain, does not meet the ideal method of determining WL.
No. 18
3. Paper point measurement method: In this method, paper point is gently passed in the root canal to estimate the working length. It is most reliable in cases of open apex where apical constriction is lost because of perforation or resorption. Moisture of blood present on apical part of paper point indicates that paper point has passed beyond estimated working length. It is used as supplementary method.This method, however, may give unreliable data:
If the pulp not completely removedIf the tooth – pulpless but a periapical lesion rich in blood supply present
If paper point – left in canal for a long time
No. 19
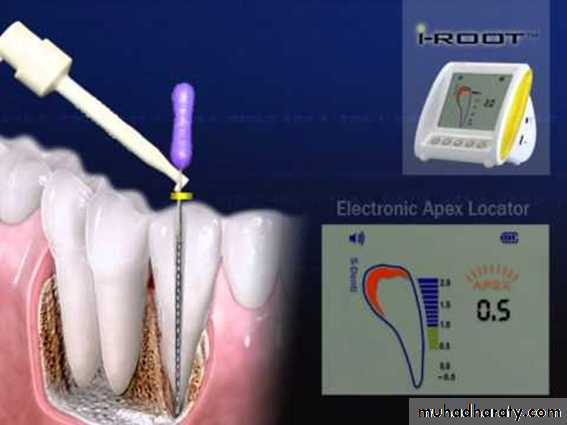
Electronic apex locatos (EAL)

No. 20
Electronic apex locators (EAL) are used for determining working length as an adjunct to radiography. They are basically used to locate the apical constriction or cementodentinal junction or the apical foramen, and not the radiographic apex.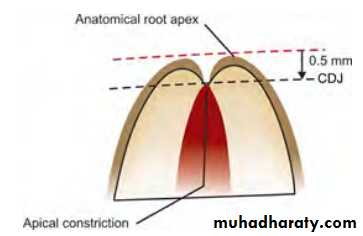
No. 21
Components of Electronic Apex Locators• Lip clip• File clip• Electronic device• Cord which connects above three parts.
No. 22
Lip clipFile clip
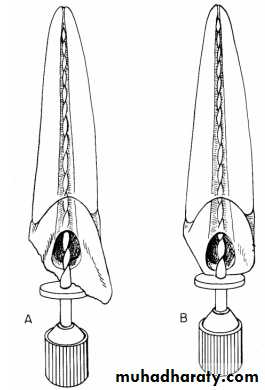
With apex locator the working length is determined by comparing the electrical resistance of the periodontal membrane with that of gingiva surrounding the tooth, both of which should be similar
A probe , such as a file, is attached to an electronic instrument with an electric cord and is inserted through the root canal until it contacts the surrounding PDL.
When the probe touches the soft tissues of the PDL, the electrical resistance gauges for both gingiva and PDL would have similar readings.
By measuring the depth of insertion
of the probe, one may determine the
working length of root canal
No. 23
Advantages of EAL• Devices are mobile, light weight and easy to use
• Much less time required
• Additional radiation to the patient can be reduced (particularly useful in cases of pregnancy)
• 80 - 97 % accuracy observed
• Provide objective information with high degree of accuracy.
• Some apex locators are also available in combination with pulp tester, or with rotary system, so can be used in combination.
No. 24
Disadvantagesa. Can provide inaccurate readings in following cases:- i. Presence of pulp tissue in canal ii. Too wet canals iii. Blockage of canal iv. Incomplete circuit v. Low battery
b. Chances of over estimationc. May pose problem in teeth with immature apex
No. 25