The second stage of development
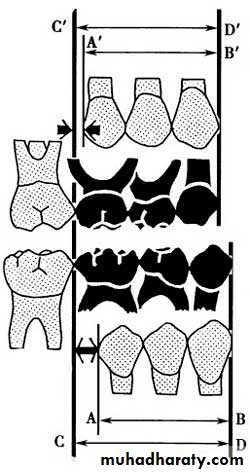
In the second stage of permanent teeth development: the C, D and E are replaced by 3, 4, and 5. In contrast to the incisor dentition, the combined mesiodistal length of the primary canine and molar teeth is greater than that of the permanent canine and premolars, an excess known as the leeway space. In the maxilla, this is approximately 1.5 mm per quadrant, whereas in the mandible it is closer to 2.5 mm, because of the increased size of the lower second primary molar.This difference in space is very important for the development of normal occlusion during late mesial shift.
The variation exist in this period includes:
Impaction of lower 5(s) due to lack of space for it due to or since it is the latter tooth which is erupted in the lower jaw mesial to the lower seven. While in the upper jaw, the lack of space will influence the canine eruption, since the latter tooth erupts prior to the upper seven in maxilla.For the lower second premolar: it may be erupted in the lingual direction or it may be impacted under the first permanent molar; while, for the upper canine: it could be erupted to the buccal direction or it could be impacted if it is directed palatals. Also in this period the reduction of the arch size “lack of space” is seen if one of these reasons is/are occur.
In Iraq, the malposed canine can be seen in female more than in male and if it is erupted into a buccal direction it takes a mesiobuccal angulation and a buccal inclination. But, if it is directed palatally then, it will be mostly impacted because the masticatory mucosa cannot be pierced by the canine due to the presence of high amount of collagen fibers. The upper canine is influenced by the problem of malocclusion in a great amount in comparison to the other teeth due to its long path of eruption “ development” since its early development occur under the orbit.
For the canine to developed normally, it should firstly directed mesially until it touches the apical part of the root of the lateral incisors, then it directed into a downward direction, and lateral direction till reaches the occlusal level. If the root of the lateral incisor is abnormal or the lateral is missed, then the canine will loss its guidance plane of eruption and it will be erupted in any direction or in any situation; therefore it will be subjected to more problem of malocclusion due to its tortuous path of eruption and due to the lack of space available for it, and due to its dependence on the presence or absence of the permanent lateral incisors.
In this stage, there is a reduction in arch length as a result of;
v Premature loss of primary second molars.v Ectopic eruption of the permanent maxillary first molar.
v Reduction in arch length as a result of caries.
They erupt at the age of 12 years old, and they occupy the same position of the 6s and usually the upper seven developed below the maxillary antrum and situated in a high level in the maxillary tuberosity and it takes a long path of eruption, but it is less than the canine.
In comparison with canine’s path of eruption is twice as long as the second molar’s path of eruption. Therefore, it is subjected ‘7’ to a less amount of crowding in comparison with the canine.
About the eruption of Sevens (upper & lower):
Usually the upper sevens when erupt, they directed distally, occlusally and buccally, but for the lower sevens, they have a short path of eruption in spite of they developed at the anterior border of the ramus, but they are directed mesially and occlusally. Therefore, they are “lower 7s” subjected to a less amount of crowding in comparison with the upper sevens.
The upper 7s in their eruption try to move in a faster rate to compensate for the downward and backward growth of the maxilla at the pterygomaxillary fissure = maxillary tuberosity.
For the lower sevens: the ramus will increase in its width by bone resorption at the anterior part, and bone deposition at the posterior part. I.e. posterior border. This will provide a space for the eruption of the lower sevens.
The malocclusion of the sevens is very rare and the impaction of the upper sevens is very rare, while the lower sevens may be impacted in some instances.
Third stage of development:
The eight try to erupt between the ages of 18- 24 years of age. The path of eruption of the 8s is nearly similar to the path of eruption of the 7s. The upper 8s developed at the posteroinferior position of the maxillary tuberosity, so, these teeth are subjected to a high amount of crowding in comparison with the 6s or 7s ⇒ due to the lack of space available for them. The lower third molar may be subjected to impaction due to lack of space. These teeth may be absent congenitally due to etiological reasons since the human jaws tend to be reduced in size while, the size of teeth are remaining as it is.Occlusal changes in the permanent dentition
The dentition does not remain static throughout life. Crowding of the mandibular incisors is one of the most common problems encountered in the permanent dentition and lower incisor alignment is one of the most likely things to relapse after orthodontic treatment.Studies of untreated subjects followed from the mixed dentition into adulthood have shown a tendency for the width and length of the mandibular arch to decrease and for crowding of the anterior teeth to increase .
Primary crowding refers to a discrepancy of tooth dimension and jaw size, mainly determined genetically. Secondary crowding is caused by environmental factors, including local space conditions in the dental arches and the position and function of the tongue, the lips and the buccal musculature. Tertiary crowding occurs during adolescence and post-adolescence with a predilection for the lower labial segment.
Factors contributing to late lower incisor crowding may include:
• Mandibular growth rotations;• Physiologic mesial drift;
• Soft tissue maturation;
• Degenerative periodontal changes allowing teeth to drift under light pressures;
• Change in diet and lack of interproximal wear;
• Tooth size and shape;
• Tooth loss and drifting leading to changes in occlusal function; and
• Mandibular third molars – presence and position.
In reality, all of these factors may contribute to the development of late lower incisor crowding but the contribution of developing third molars is regarded as being minimal as crowding can develop even in the absence of their development. The prophylactic removal of developing third molars is not recommended to prevent late lower incisor crowding.

Tooth eruption
Although researchers agree that tooth eruption is a complex process, there is little agreement on the identity of the mechanism that controls eruption.[Some commonly held theories that have been disproven over time include: (1) the tooth is pushed upward into the mouth by the growth of the tooth's root, (2) the tooth is pushed upward by the growth of the bone around the tooth, (3) the tooth is pushed upward by vascular pressure, and (4) the tooth is pushed upward by the cushioned hammock.
The cushioned hammock theory, first proposed by Harry Sicher, was taught widely from the 1930s to the 1950s. This theory postulated that a ligament below a tooth, which Sicher observed under a microscope on a histologic slide, was responsible for eruption. Later, the "ligament" Sicher observed was determined to be merely an artifact created in the process of preparing the slide.
The most widely held current theory is that while several forces might be involved in eruption, the periodontal ligaments provide the main impetus for the process. Theorists hypothesize that the periodontal ligaments promote eruption through the shrinking and cross-linking of their collagen fibers and the contraction of their fibroblasts.
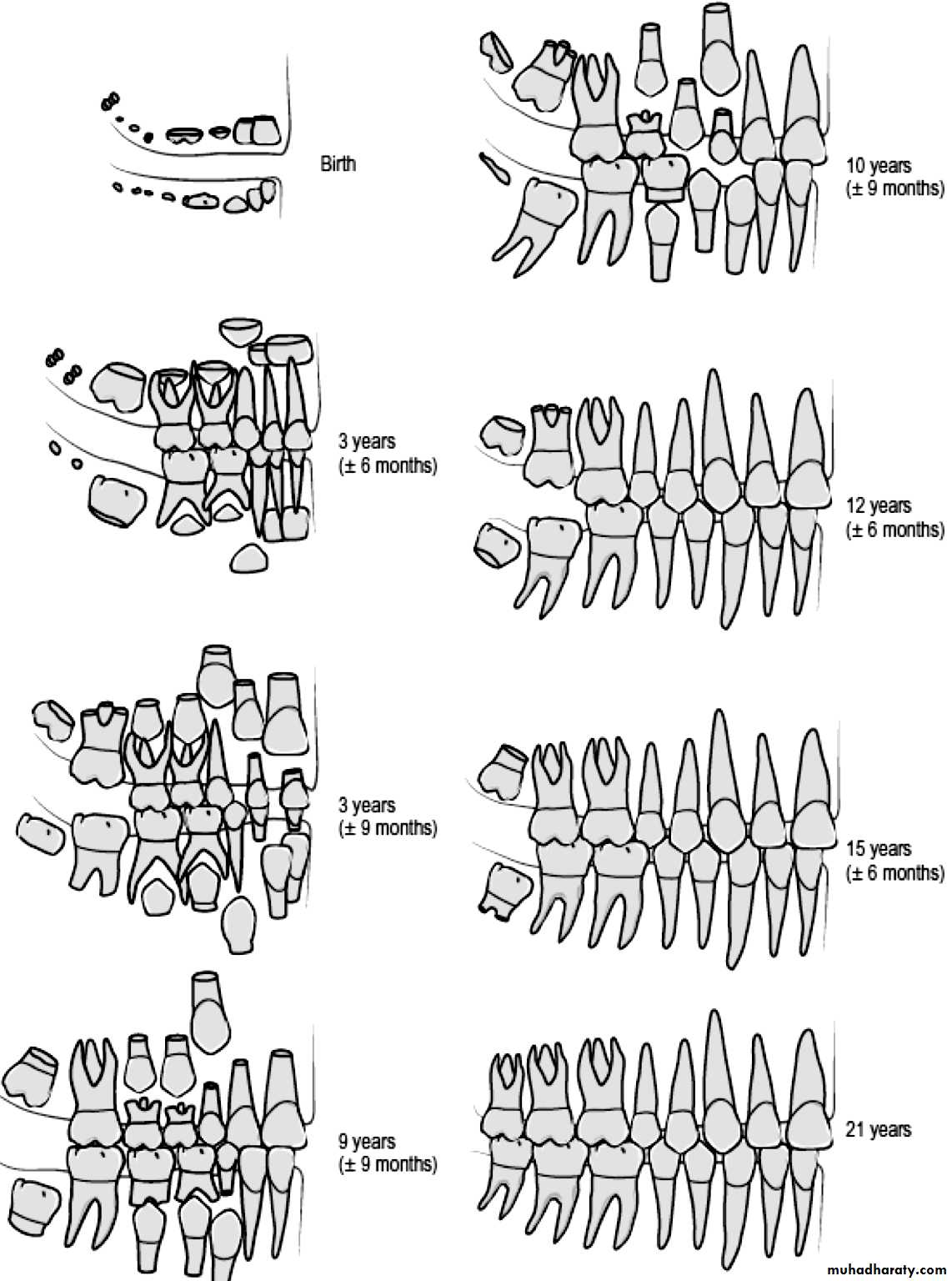
• Although tooth eruption occurs at different times for different people, a general eruption timeline exists. Typically, humans have 20 primary (baby) teeth and 32 permanent teeth.
• Tooth eruption has three stages. The first, known as deciduous dentition stage, occurs when only primary teeth are visible. Once the first permanent tooth erupts into the mouth, the teeth are in the mixed (or transitional) dentition. After the last primary tooth falls out of the mouth—a process known as exfoliation—the teeth are in the permanent dentition.
• Primary dentition starts on the arrival of the mandibular central incisors, usually at eight months, and lasts until the first permanent molars appear in the mouth, usually at six years. The primary teeth typically erupt in the following order: (1) central incisor, (2) lateral incisor, (3) first molar, (4) canine, and (5) second molar.
•
• As a general rule, four teeth erupt for every six months of life, mandibular teeth erupt before maxillary teeth, and teeth erupt sooner in females than males.
• During primary dentition, the tooth buds of permanent teeth develop below the primary teeth, close to the palate or tongue.
•
• Mixed dentition starts when the first permanent molar appears in the mouth, usually at six years, and lasts until the last primary tooth is lost, usually at eleven or twelve years.

• Permanent teeth in the maxilla erupt in a different order from permanent teeth on the mandible. Maxillary teeth erupt in the following order: (1) first molar (2) central incisor, (3) lateral incisor, (4) first premolar, (5) second premolar, (6) canine, (7) second molar, and (8) third molar. Mandibular teeth erupt in the following order: (1) first molar (2) central incisor, (3) lateral incisor, (4) canine, (5) first premolar, (6) second premolar, (7) second molar, and (8) third molar. Since there are no premolars in the primary dentition, the primary molars are replaced by permanent premolars.
• The permanent dentition begins when the last primary tooth is lost, usually at 11 to 12 years, and lasts for the rest of a person's life or until all of the teeth are lost (edentulism). During this stage, third molars (also called "wisdom teeth") are frequently extracted because of decay, pain or impactions. The main reasons for tooth loss are decay and periodontal disease.
Eruption times for primary and permanent teeth [52]
Primary teethTeeth
CentralincisorLateralincisor
Canine
Firstpremolar
Secondpremolar
Firstmolar
Secondmolar
Thirdmolar
Maxillary teeth
10 mo
11 mo
19 mo
-
-
16 mo
29 mo
-
Mandibular teeth
8 mo
13 mo
20 mo
-
-
16 mo
27 mo
-
Permanent teeth
Teeth
CentralincisorLateralincisor
Canine
Firstpremolar
Secondpremolar
Firstmolar
Secondmolar
Thirdmolar
Maxillary teeth
7–8 yr
8–9 yr
11–12 yr
10–11 yr
10–12 yr
6–7 yr
12–13 yr
17–21 yr
Mandibular teeth
6–7 yr
7–8 yr
9–10 yr
10–12 yr
11–12 yr
6–7 yr
11–13 yr
17–21 yr