Rheumatology lecture-1
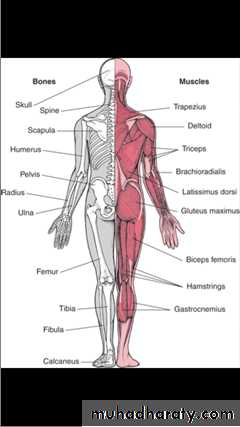
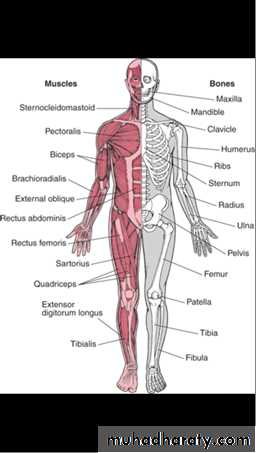
The human musculoskeletal system(also known as the loco-motor system) is an organ system that gives humans(and many animal species) the ability to move using the muscular & skeletal systems.It provides form, support, stability & movement to the body. It is made up of the body's bones(the skeleton), muscle, cartilage, tendon, ligament, joint& other connective tissue that supports & binds tissues & organs together.

Disorders of musculoskeletal system are prevalent throughout the world, affecting all ages ðnic groups.
The principal manifestations are pain& impairment of locomotor function.
MSK disorders are divided into:
1-Non inflammatory conditions like neck & back pain ,OA, osteoporosis& fibromyalgia
2-inflammatory conditions like RA, connective tissue disease(SLE, gout, pseudo gout, polymyalgia rheumatica, & seronegative spondarthritis).
Noninflammatory conditions are much more common than inflammatory conditions.
Low back pain (LBP) this is a common example of musculoskeletal disorders(MSDs). LBP may be classified by duration as acute(pain lasting less than 6 weeks), or sub chronic(6-12 weeks) or chronic( more than 12 weeks).One of the most common reasons for seeking medical attention, second only to respiratory issues
84% of adults will have low back pain at some point
Wide variety of approaches for treatment
Suggests that optimal approach is unsure
Most episodes are self-limited
Some suffer from chronic or recurrent courses, with substantial impact on quality of life
The condition may be further classified by the underlying cause as either:
1- mechanical : accounts for 90% of cases & affecting patients aged 20-55 years.The onset is acute, provoked by sudden movement(lifting or bending )& relieved by rest.
The pain is not radiated beyond the knee& usually asymmetrical.
2- non-mechanical pain( referred pain): usually constant& not relieved by rest. Common causes include malignancy(secondary), fracture, & infection.
In most episodes of LBP, a specific underlying cause is not identified or even looked for, with the pain believed to be due to mechanical problem such as muscle or joint strain.
The symptoms of LBP usually improve within few weeks with 40-90% of people become completely better by 6 weeks. However this is not the case in other patient members who experience a disgusting pain throughout their life.
Cauda equina syndrome(CES)
Is a serious neurologic condition in which damage to the Cauda equina causes acute loss of function of the lumber plexus( nerve roots) of the spinal canal below the termination(conus medullaris) of the spinal cord.CES is a lower motor neuron lesion.
CES is manifested by difficulty with micturition, loss of anal sphincter tone or incontinence, saddle anesthesia, progressive motor weakness, gait difficulty& finally sensory level.Tumor, trauma, spinal stenosis& inflammatory conditions are often the etiological factors of CES.
It usually an urgent neurological condition, requiring urgent surgical interference.
3-inflammatory :common cause is ankylosing spondylitis.
The pain is gradual & often occur before the age of 30, associated with morning stiffness & improves rather than worsening with activity.4- radicular(nerve root) pain: sever& sharp. It radiates down below knee & aggravated by cough, sneezing & straining rather than by back movement. It manifested by parasthesia & reduced straight leg rising which reproduce leg pain.
Motor, sensory& reflex signs are limited to one nerve root. Prognosis is reasonable(50% recovery at 6-weeks).
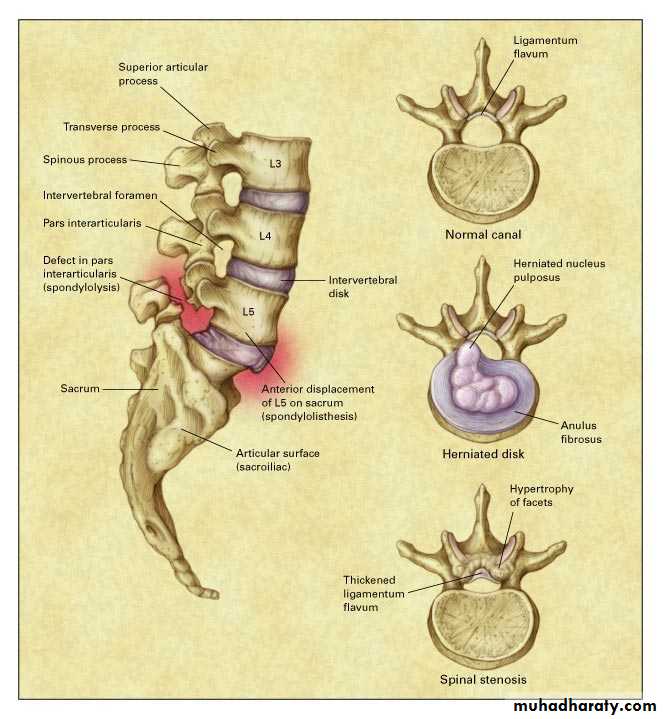
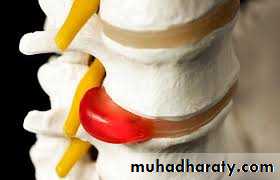
Disc prolapse frequently occur at L4-L5 due to increased mechanical forces across this area.
Any neurological deficit at 6-weeks is an indication to consider surgery.
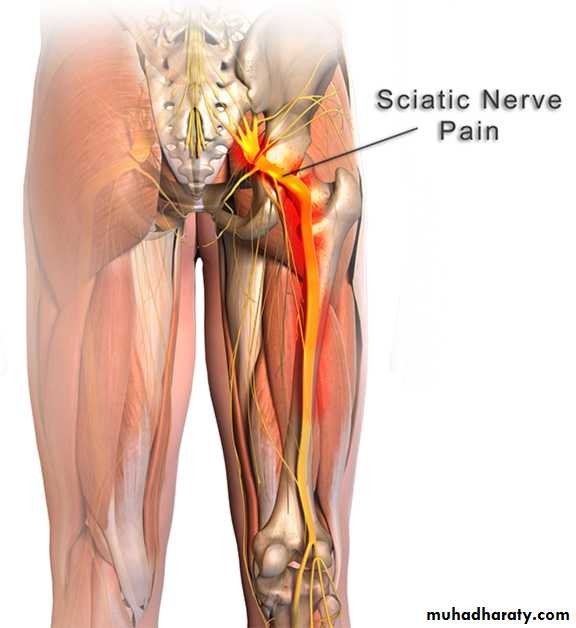
Sciatica
Sciatica refers to pain that radiates along the path of the sciatic nerve, which branches from the lower back through hips and buttocks and down each leg. Typically, sciatica affects only one side of the body.Sciatica most commonly occurs when a herniated disk, bone spur on the spine or narrowing of the spine (spinal stenosis) compresses part of the nerve. This causes inflammation, pain and often some numbness in the affected leg.
.
Although the pain associated with sciatica can be severe, most cases resolve with non-operative treatments in a few weeks. People who have severe sciatica that's associated with significant leg weakness or bowel or bladder changes might be candidates for surgery
Investigations of LBP:
1-plain x-ray=rarely helpful in acute mechanical low back pain, however, it may be helpful in young patients with Ankylosing spondylitis, patients with suspicion of malignancy& history of fracture.
2- MRI- in any patient with suspected malignancy & normal plain radiography, MRI should be undertaken.
3-CT is inferior to MRI in soft tissue pathology & nerve involvement, but it is useful in bone disease& when MRI is contraindicated.
4- blood tests: low Hb, elevated CRP, elevated ESR, indicate infection, malignancy, & inflammation.
Increased acid phosphatase &prostate specific antigen(PSA) are associated with Ca-prostate. Increased alkaline phosphatase indicates bone metastasis & paget's disease of bone.
Multiple myeloma is associated with normal alkaline phosphatase, myeloma band in protein electrophoresis& urine test Bence Jone's protein(light chain).
EMG & nerve conduction studies are helpful to localize the nerve root lesions.
TREATMENTRemoval of the underlying cause of backache is the gold standard of treatment of LBP. However, this is not appropriate in most cases.
Symptomatic treatment of this condition includes analgesia& rest, back exercise& traction, joint injections with steroids& rapid return to work to reduce the risk of chronic disability.
SURGERY is indicated in 1% of cases only.
Herniated intervertebral discs
Nonsurgical treatment for at least a month
Exceptions: cauda equina syndrome, progressive neurologic deficits
Early treatment same as for nonspecific low back pain, but may need short courses of narcotics for pain control
Bed rest not useful
Some patients benefit from epidural corticosteroid injections
If severe pain, neurologic deficits MRI and consider surgery