
Primary myocardial diseases:
1- Myocarditis:-
It's an inflammatory processes of the myocardium that result in injury to the
cardiac myocytes. It's either
secondary
to other heart diseases as ischemic injury,
or
primary
myocarditis which's caused by several types of microorganisms as
viruses, parasites and bacterial infections or may be caused by immune mediated
reactions that cross react with myocardial cells as occur in rheumatic heart
disease .
Morphology:-
The heart may be of normal size or dilated, the myocardium is flabby and pale
with small areas of hemorrhage.
Microscopically:-
The microscopical changes depend on causative agents but in
general it consists of inflammatory cells infiltrate as lymphocytes, mononuclear
cells and even neutrophils, with degeneration and/or necrosis of myocytes.
Cardiomyopathies:-
Or heart muscle disease, it is heart disease result from a primary abnormality in
the myocardium.
It's divided into 3 major groups:
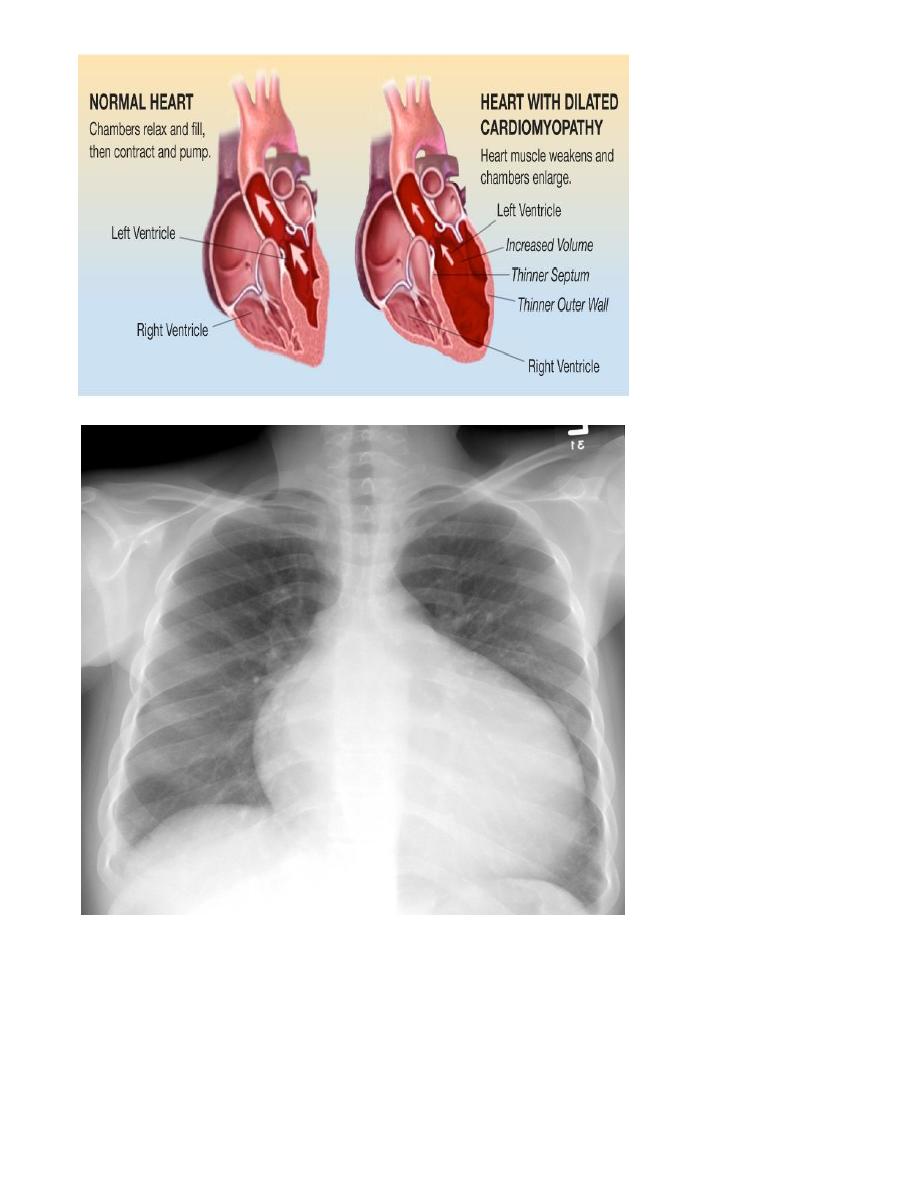
(I) Dilated cardiomyopathy:-
It's usually idiopathic but it may be secondary to other causes, it's characterized
by progressive cardiac hypertrophy, dilation and contractile (systole) dysfunction.
Dilated cardiomyopathy occur at any age but it usually common between ages of
20-60 years.
Morphology:-
The heart is enlarged by dilation and hypertrophy of all chambers. The dilation
and poor contractile function cause stasis of blood in cardiac chambers and
predispose to development of fragile mural thrombi and emboli.
(II) Hypertrophic cardiomyopathy:-
It consists of a symmertric septal hypertrophy and idiopathic hypertrophic
subaortic stenosis, it' s characterized by myocardial hypertrophy, abnormal
diastolic filling and intermittent ventricular outflow obstruction.
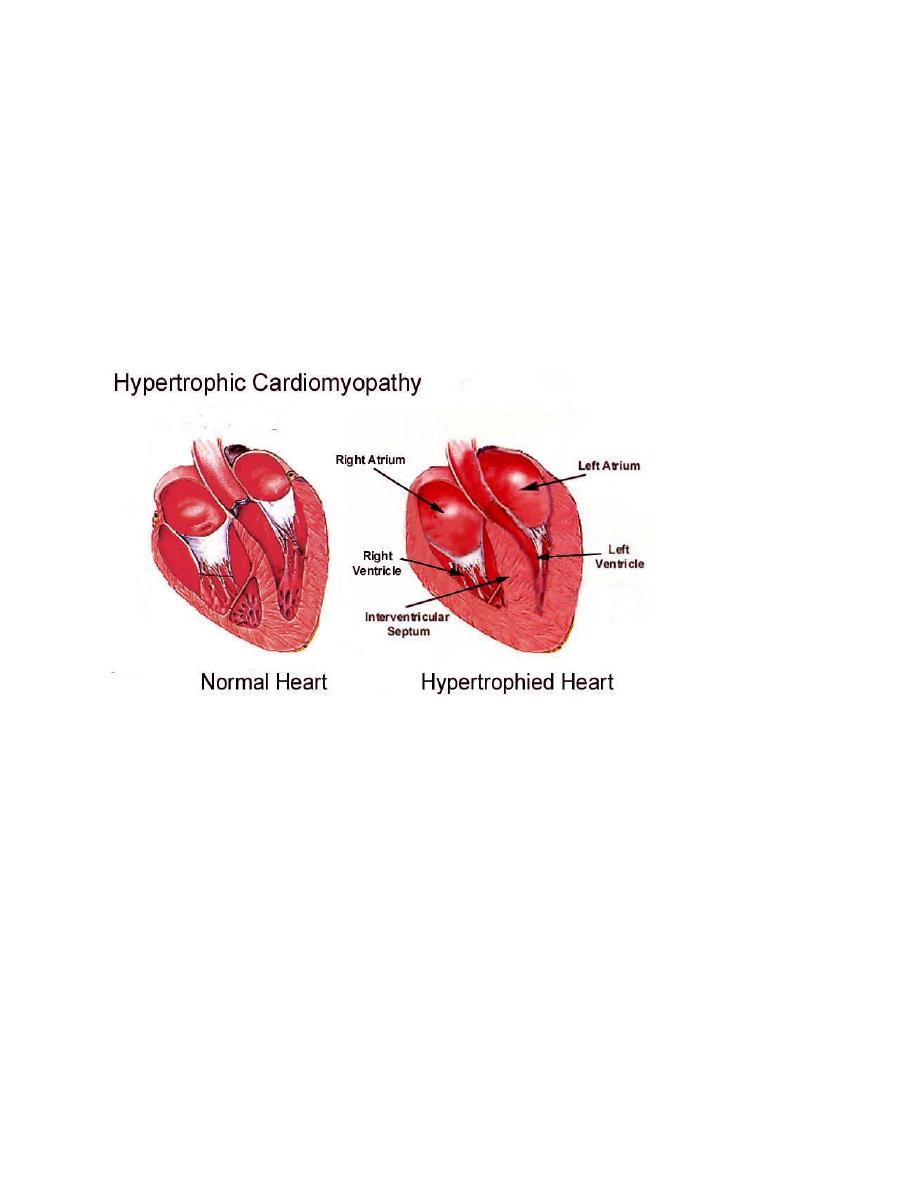
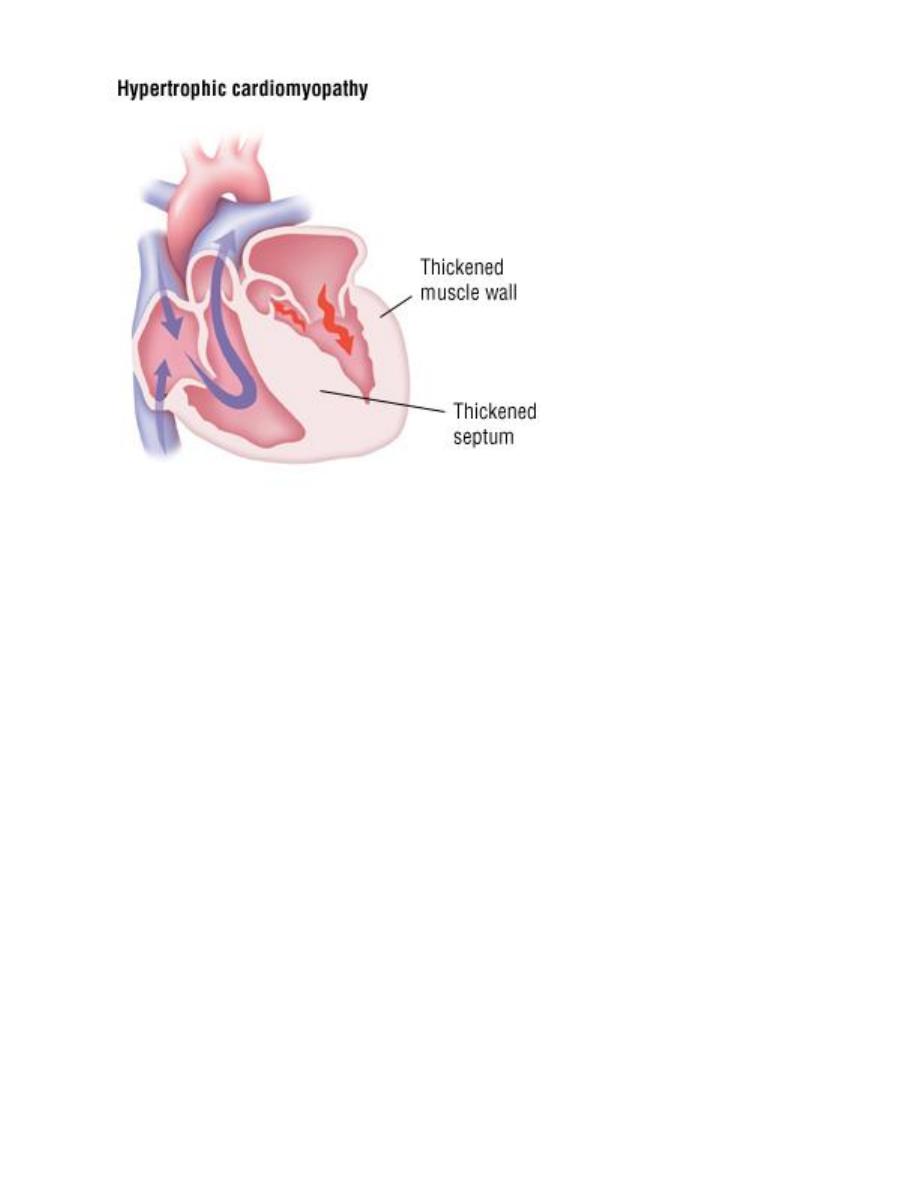
Morphology:-
The essential feature of hypertrophic cardiomyopathy is myocardial hypertrophy
which is most pronounced in the left ventricle and inter-ventricular septum.
The hypertrophy is usually conspicuous in sub-aortic region of the septum, so
this asymmetric hypertrophy is often associated with ventricular outflow
obstruction during systole, so it's called "idiopathic hypertrophic sub-aortic
stenosis" .
Ventricular dilation is uncommon but left atrium may be dilated because of
impaired diastolic filling of thickened rigid left
ventricle.
Restrictive cardiomyopathy:-
It's a disorder characterized by a primary decrease in ventricular compliance,
resulting in impaired ventricular filling during diastole, most common cause of
this decrease of compliance due to endomyocardial fibrosis.
Hypertensive heart disease:-
Hypertensive heart disease (HHD) is a consequence of the increased demands
placed on the heart by hypertension, causing pressure overload and ventricular
hypertrophy. Myocyte hypertrophy is an adaptive response to pressure overload;
there are limits to myocardial adaptive capacity, however, and persistent
hypertension eventually can culminate in dysfunction, cardiac dilation, CHF, and
even sudden death. Although hypertensive heart disease most commonly affects the
left side of the heart secondary to systemic hypertension, pulmonary hypertension
also can cause right-sided hypertensive changes—so-called “cor pulmonale.”
Pericardial diseases:-
The most diseases of pericardium are:
1- Inflammatory condition (pericarditis).
2- Pericardial effusion.

Pericardial effusion:-
It's accumulation of fluid in pericardial space is often asymptomatic if it accumulate
slowly, but rapid developing effusions may cause tamponade the most cause of
effusions are congestive heart failure, hypoalbuminemia, malignancy, and
mediastinal lymphatic obstruction.
Congenital heart diseases:-
It's most common types of congenital malformations and it's most common
cause of heart disease in children.
Its causes in 90%
idiopathic
, while 10% of it reveal either
genetic factors
or
environmental factors
such as congenital rubella infection.
The types of congenital heart diseases include:
1- Malformations causing a left-to-right shunt.
2- Malformations causing a right-to-left shunt (cyanotic congenital heart diseases).
3- Malformations causing obstruction.
(I) Left-to-right shunts:-
is most common types of cardiac malformations, this is usually a cyanotic in early
stage but in later stages can cause cyanosis when produced significant pulmonary
hypertension and reversal blood flow through the shunt occurs, that include:-
1- Atrial septal defects.
2- Ventricular septal defects.
3- Patent ductus arteriosus.
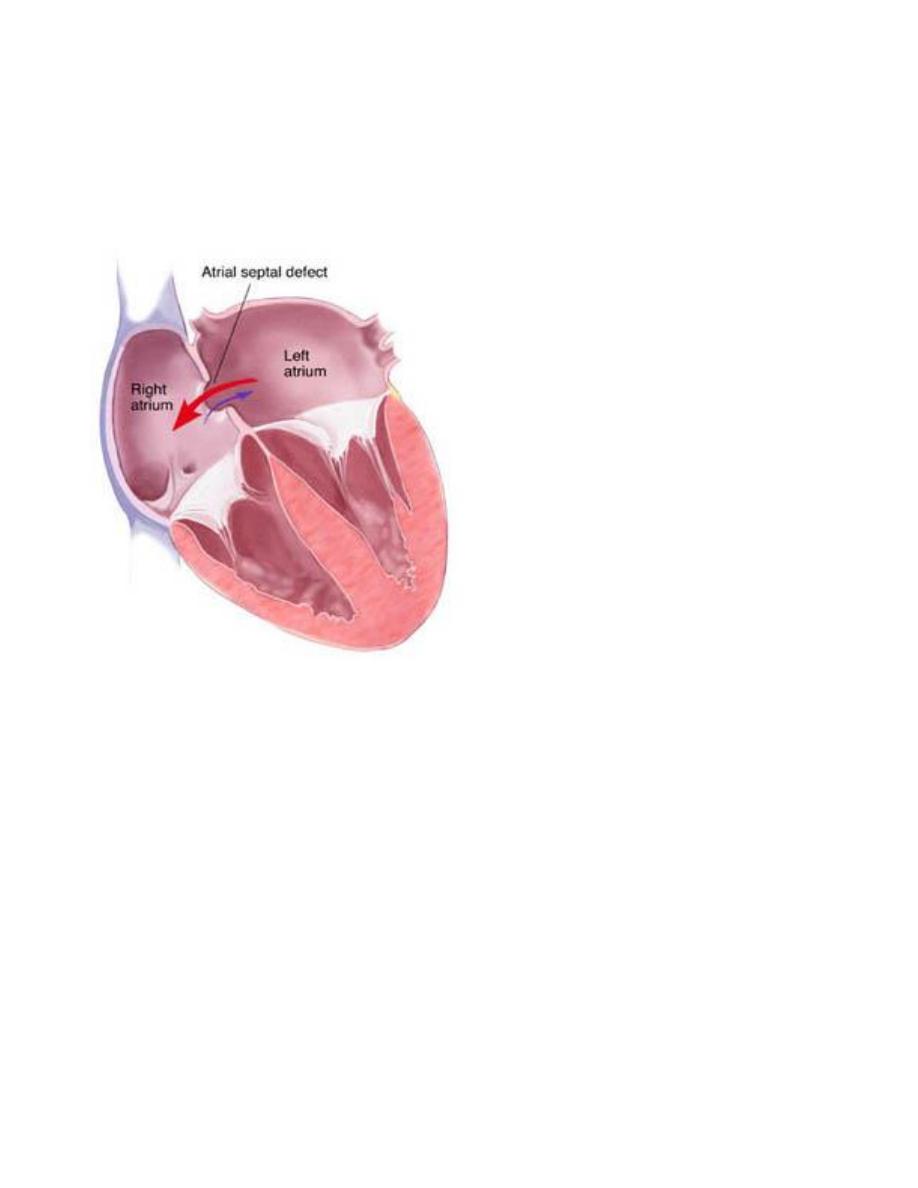
1- Atrial septal defects:-
Is caused most commonly by failure to close of foramen ovale after birth, the
foramen ovale is a flap of tissue in septum between 2 atrium act as a one-way valve
allowing blood to keep flowing from right to left during intrauterine life at the time
of birth as pulmonary vascular resistance fall and systemic arterial pressure
increases, so pressure in the left atrium rises above that in right atrium and must
cause functional closure of the foramen ovale.
Patency persist in about 25% of general population and this will cause shunt of
blood from left to right atrium, this defect usually well tolerated if it's less than 1
cm in diameter but even larger lesions do not produce any symptom in childhood
because the flow of blood is from left to right, but with time when pulmonary
vascular resistance increase and pulmonary hypertension developed so reversal of
shunt so the shunt become right to left and developed cyanosis.
Morphology:-
Manifested as right atrial and ventricular dilation, right ventricular hypertrophy and
dilation of pulmonary artery, pulmonary hypertension developed.
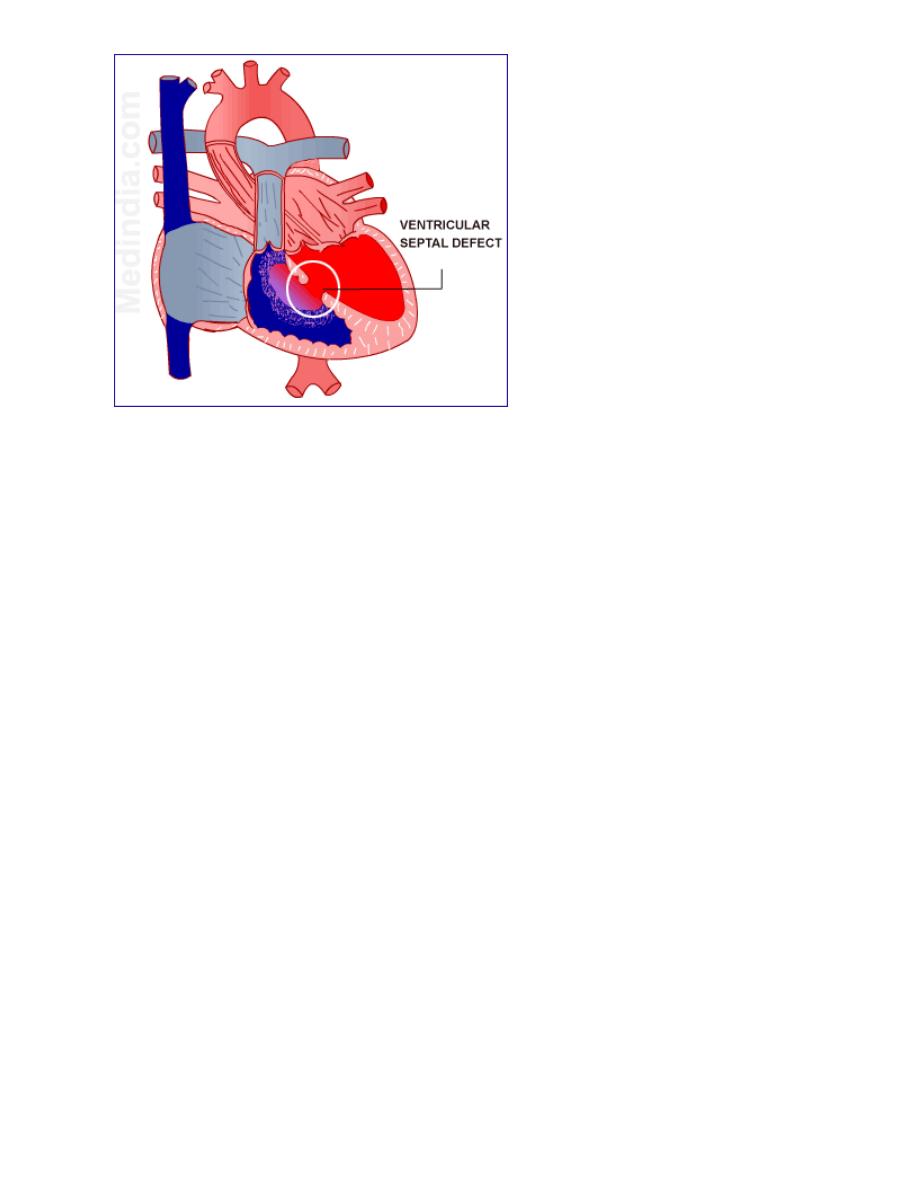
Ventricular septal defect:-
VSDs are the most common congenital heart defects and this like ASDs occur in
isolation or in association with other cardiac malformations, the size and location of
defect is variable ranging from minute to large defect and this may close
spontaneously during infancy or childhood.
Morphology:-
In large defect associated with significant left to right shunt so right
ventricle is hypertrophied and dilated, with pulmonary hypertension developed if
this occur so reverse of shunt and cyanosis occur.
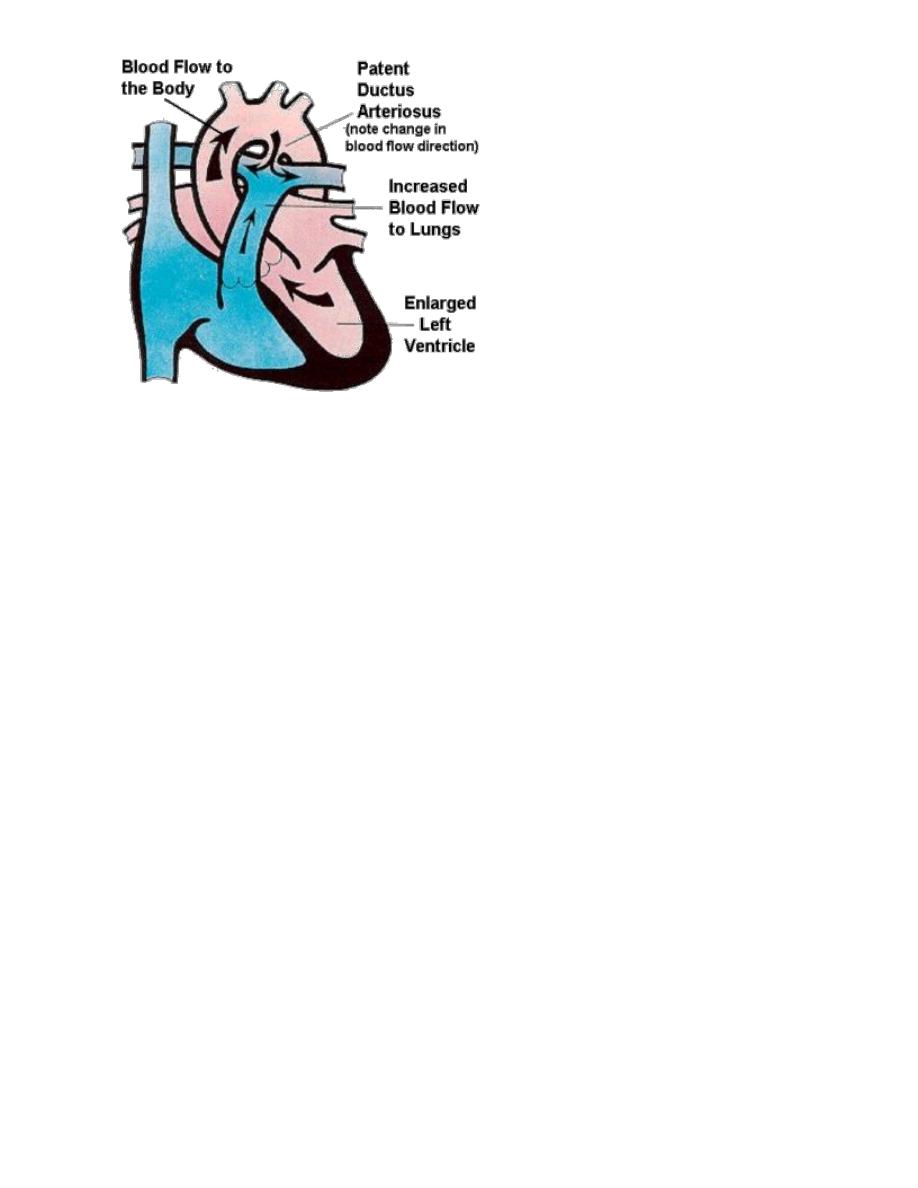
Patent ductus arteriosus:-
Ductus arteriosus:
is an arterial channel that courses between the pulmonary artery
and aorta. During intrauterine life, the DA permits blood to flow freely from the
st
pulmonary artery to the aorta. Complete irreversible closure occurs within the 1
few months after birth, this closure may be delayed or failed to occur to give PDA
condition.
Morphology:-
The oxygenated blood flows from the left ventricle to the lungs and is returned to
the left atrium, so form volume overload to cause dilation and hypertrophy of left
atrium and ventricle.
The proximal pulmonary arteries are also dilated with development of pulmonary
hypertension and cause right ventricular hypertrophy and dilation and right atrial
dilation.
(II) Right-to-left shunts:-
Cardiac malformations associated with right-to-left shunts are distinguished by
cyanosis at or near the time of birth, this occur because poorly oxygenated blood
from the right side of the heart is introduced directly into the arterial circulation.
2 important conditions cause cyanotic congenital heart disease:
1-Tetralogy of Fallot
2- Transposition of great vessels.
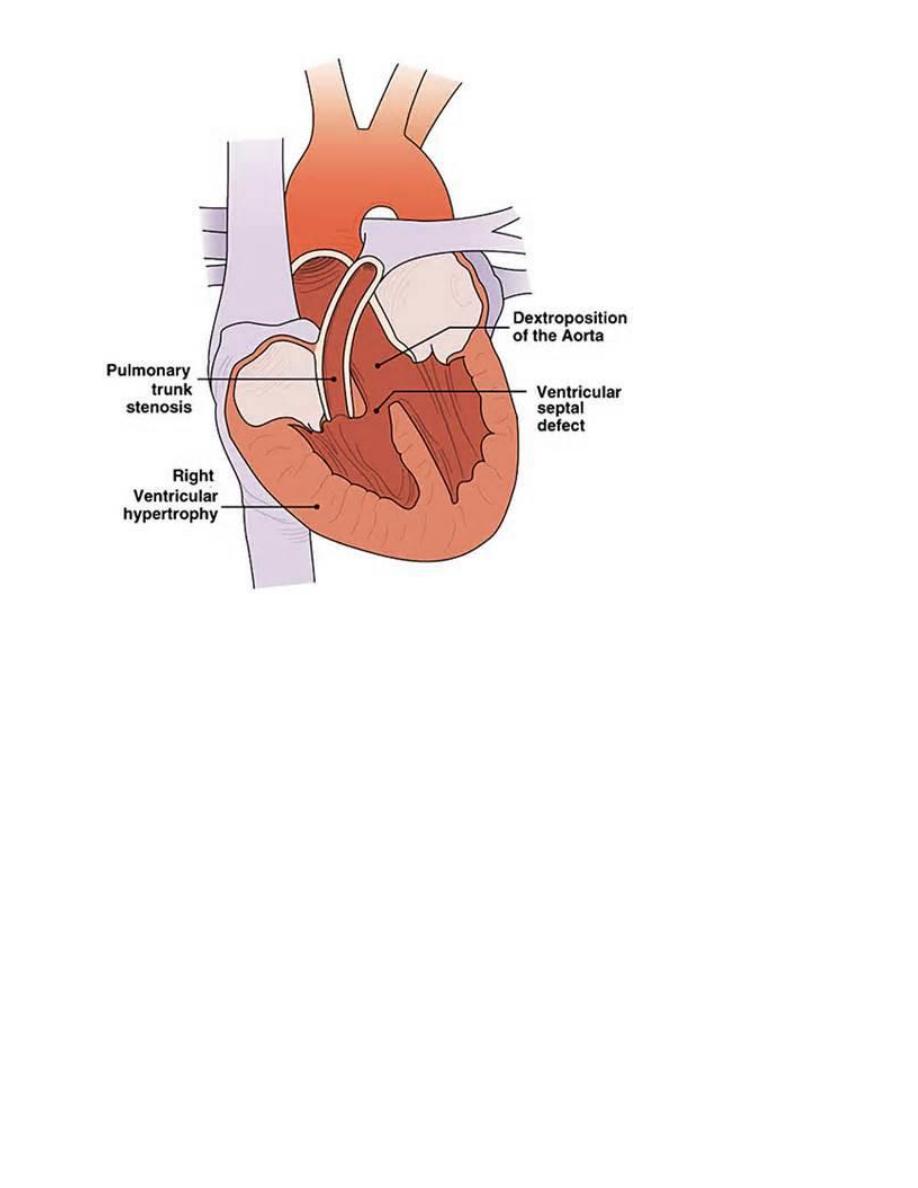
Tetralogy of Fallot:-
TOF is the most common cause of cyanotic congenital heart disease, the four
components of TOF:
1- VSD.
2- Dextraposed aortic root that overrides the VSD.
3- Right outflow obstruction.
4- Right ventricular hypertrophy.
Patient with TOF is at risk to develop infective endocarditis, systemic emboli and
brain abscesses.
Morphology:-
The heart is enlarged externally by right ventricular hypertrophy, the
proximal aorta is larger than pulmonary trunk, so that because of stenotic
pulmonary artery, this will lead to shunt unoxygenated blood from right ventricle
through VSD to go to left ventricle and aorta.
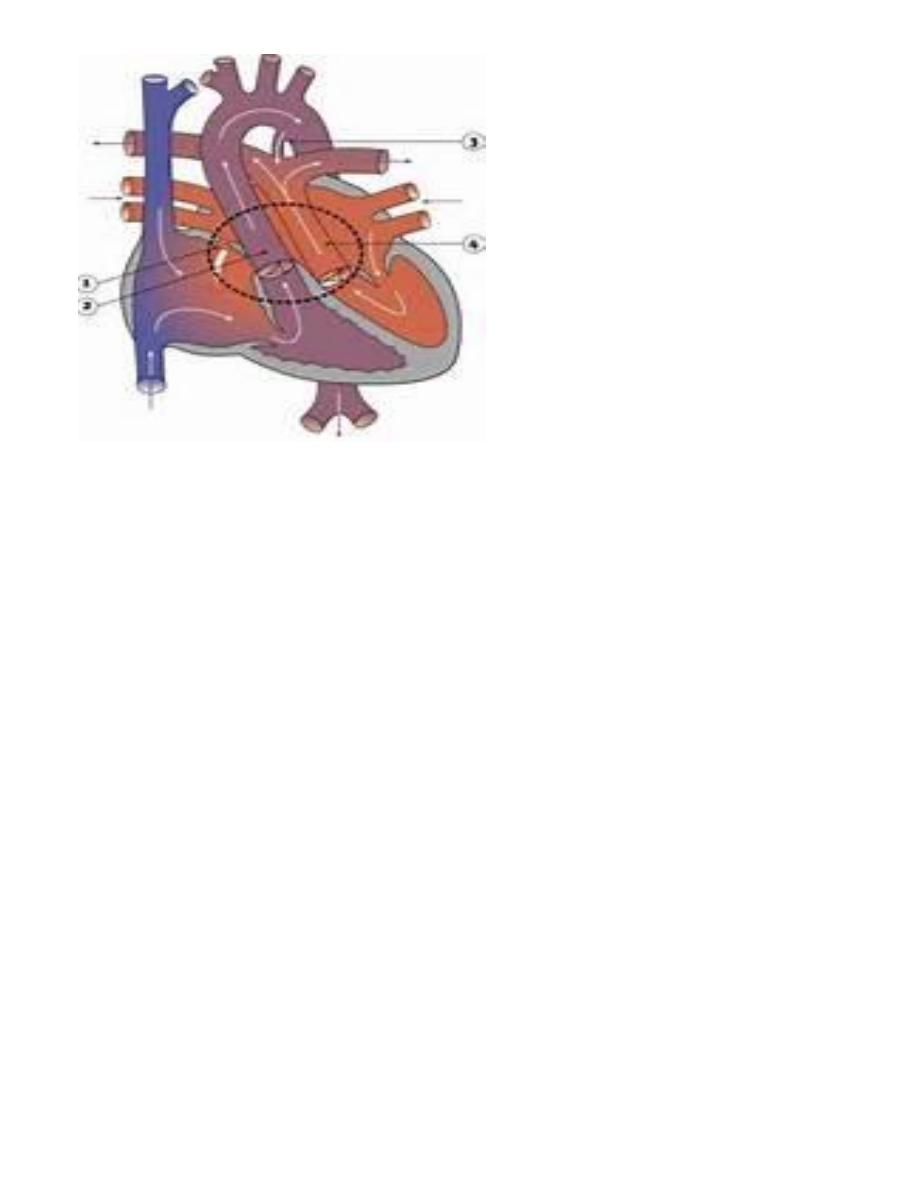
Transposition of great arteries:-
There's abnormal truncal septation, the aorta arises from the right ventricle and the
pulmonary artery from the left ventricle, so all unoxygenated blood with pump from
right ventricle to systemic circulation by aorta and cause cyanosis but with
presence of another defect as
ASD, VSD
and
PDA
, this allows
oxygenated blood to reach aorta.
Congenital obstructive lesions:-
As :
1- valvular aortic stenosis.
2- Pulmonic stenosis.
3- Coarctation of aorta.
Cardiac tumors:-
Metastatic carcinoma:-
It's more common than primary one, the most common sites of metastasis to the
heart are: lungs, breast and malignant melanoma, the metastatic cells usually goes
to pericardium to cause pericarditis and hemorrhagic pericardial effusions.
Primary neoplasms:-
Less common and the common primary neoplasm are:
1- Myxoma: is a benign tumor,
2- Cardiac rhabdomyoma: is a benign tumor.
3- Lipoma.