1
Orthopedic Surgery
5
th
Stage
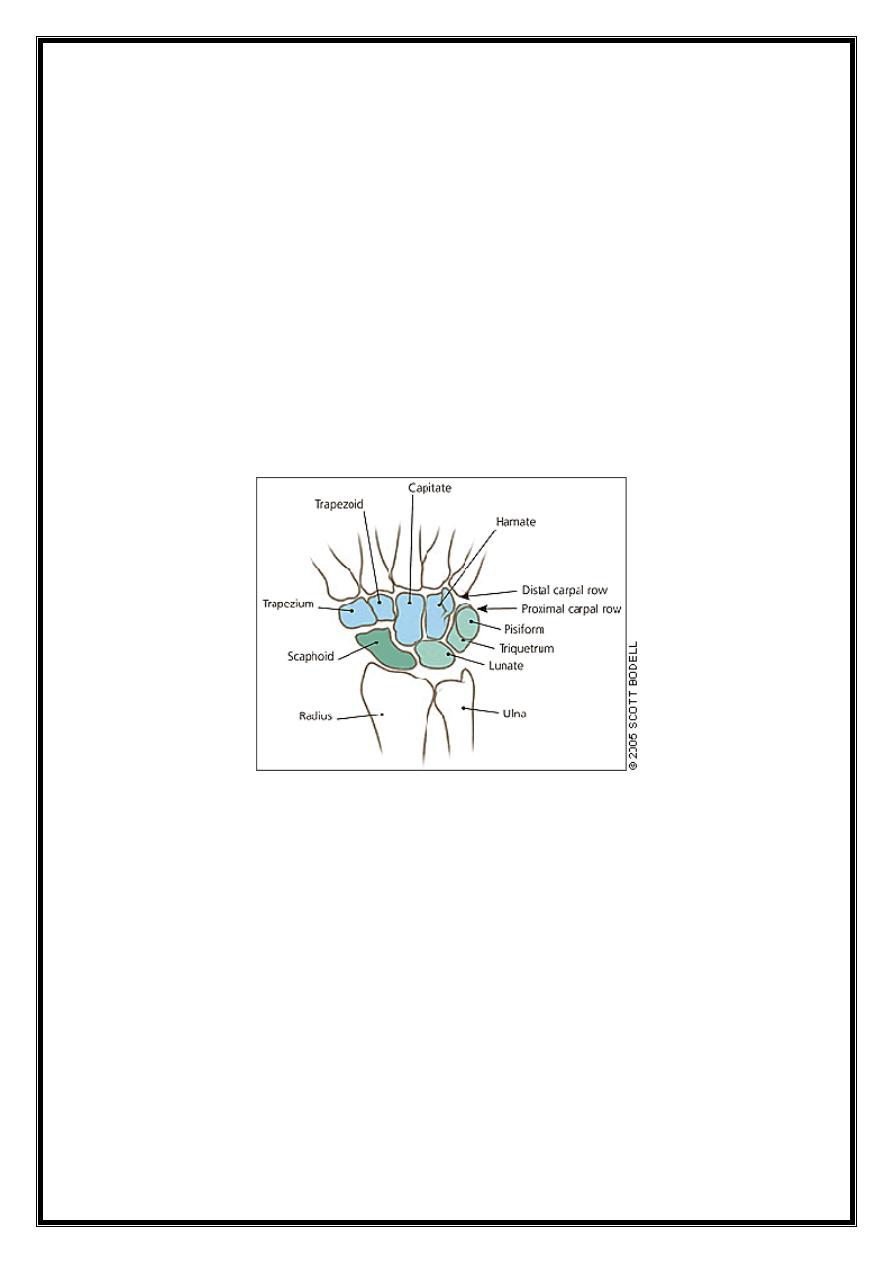
Carpal injuries
Carpal injuries are common, includes:
Fractures of carpal bones
Carpal dislocations
Wrist sprain
Fractures of the carpal bones
Fracture carpal Scaphoid
Accounts 75% of all carpal injuries
rare in elderly & children
Most of the #s are stable in unstable there is displaced
fragment .
2
Caused by fall on dorsiflexed hand possibly with radial
deviation —stress on the scaphoid.
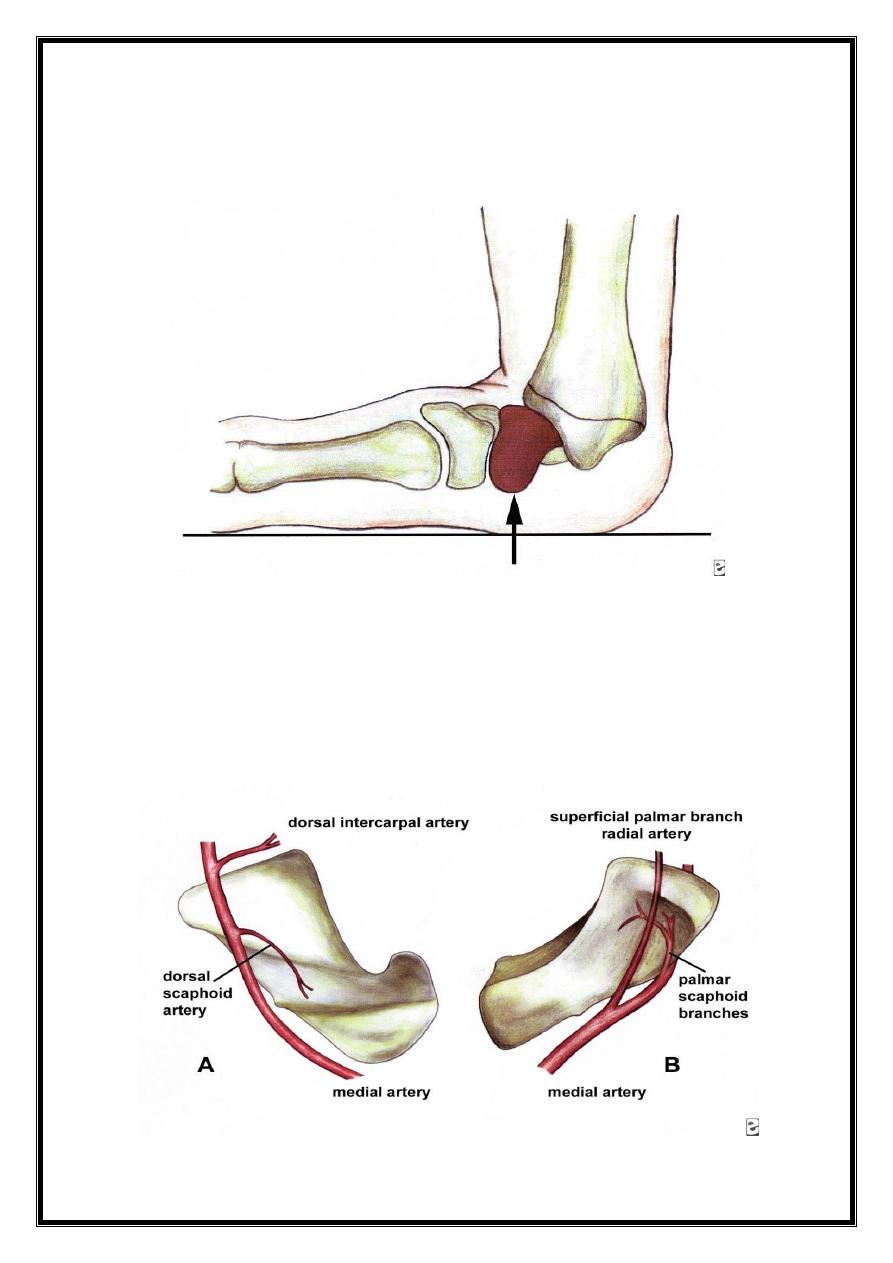
Blood supply
Vessels supplying are distal to proximal in orientation,
diminishes proximally so interruption of the supply by # is
responsible for avascular necrosis of the proximal pole &
nonunion
.
3
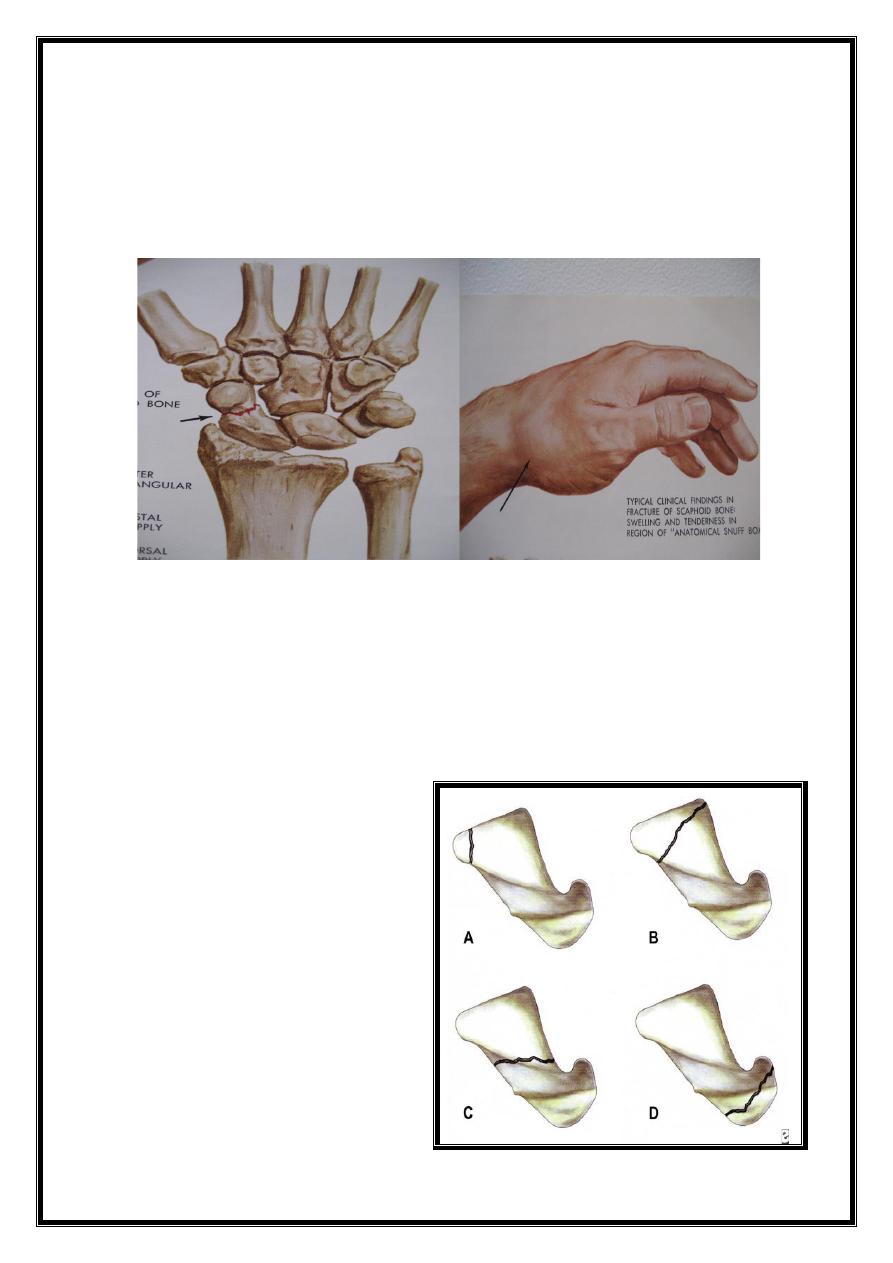
C/F:
Fullness in the Anatomical Snuff box
Local tenderness
Proximal pressure along the axis of thumb may be
painful.
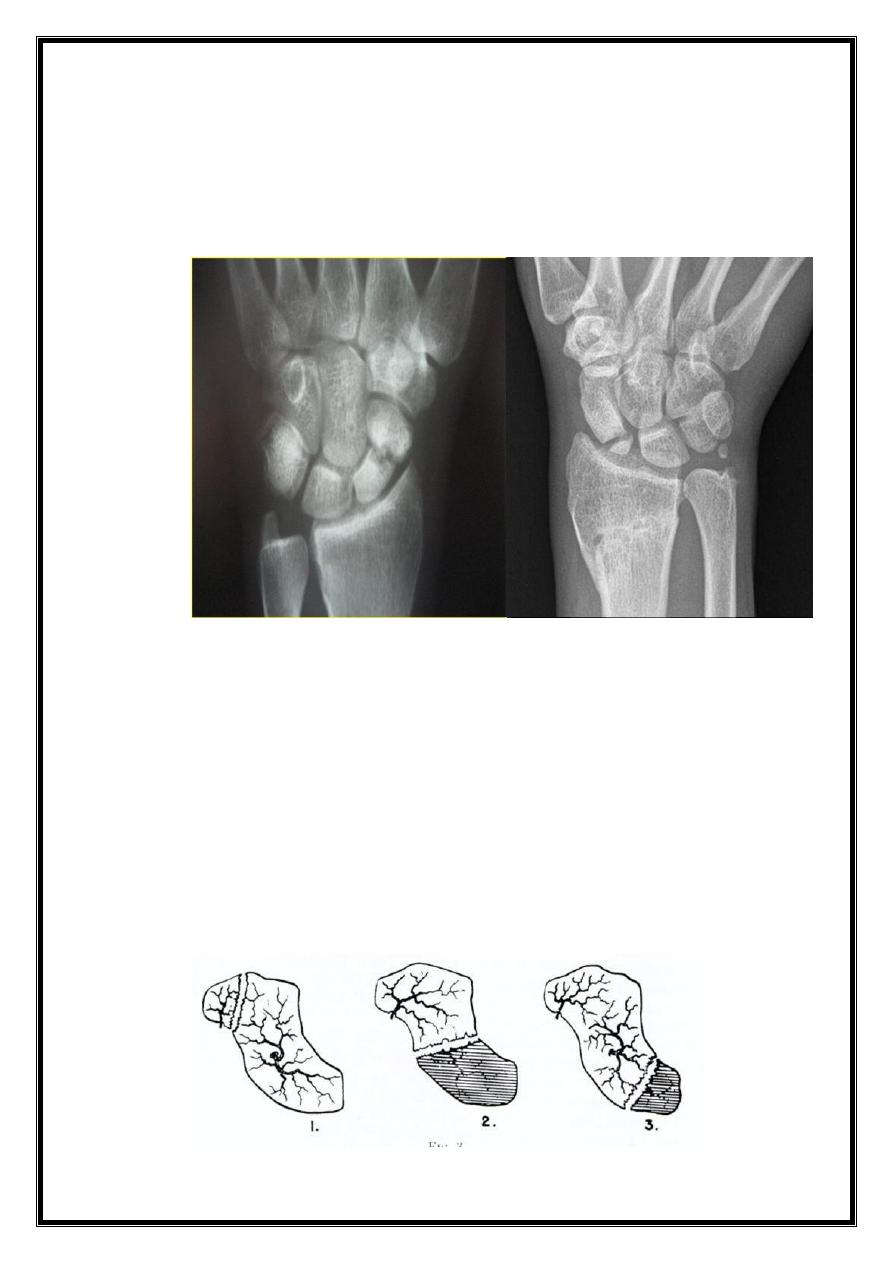
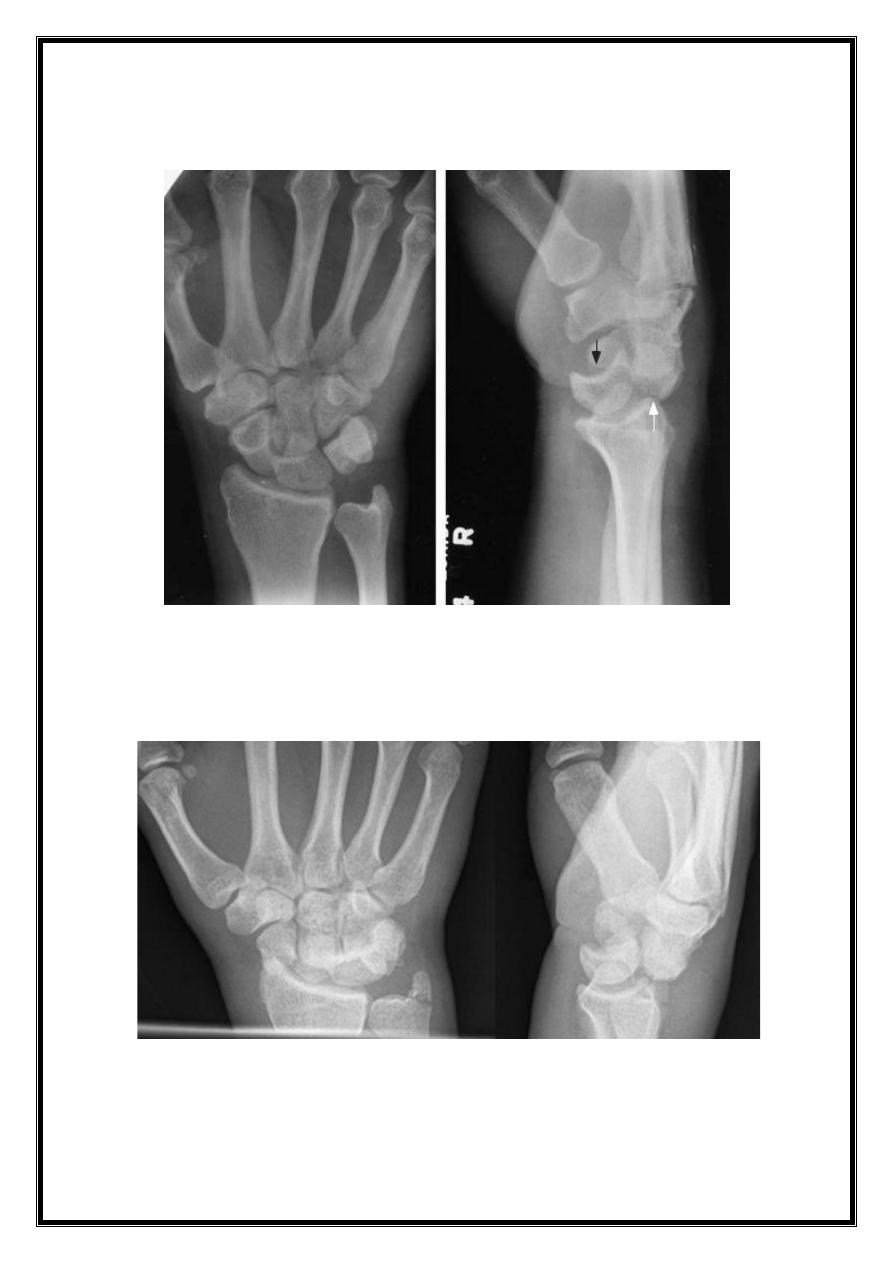
X Ray; AP, Lateral & oblique views
# may be invisible immediately after injury
when there is doubt repeat the X Ray after 2 weeks —may
be more obvious
Often a recent # shows in oblique view .
# line is usually through
A. Tubercle
B. Distal pole
C. Waist (commonest)
D. Proximal pole

4
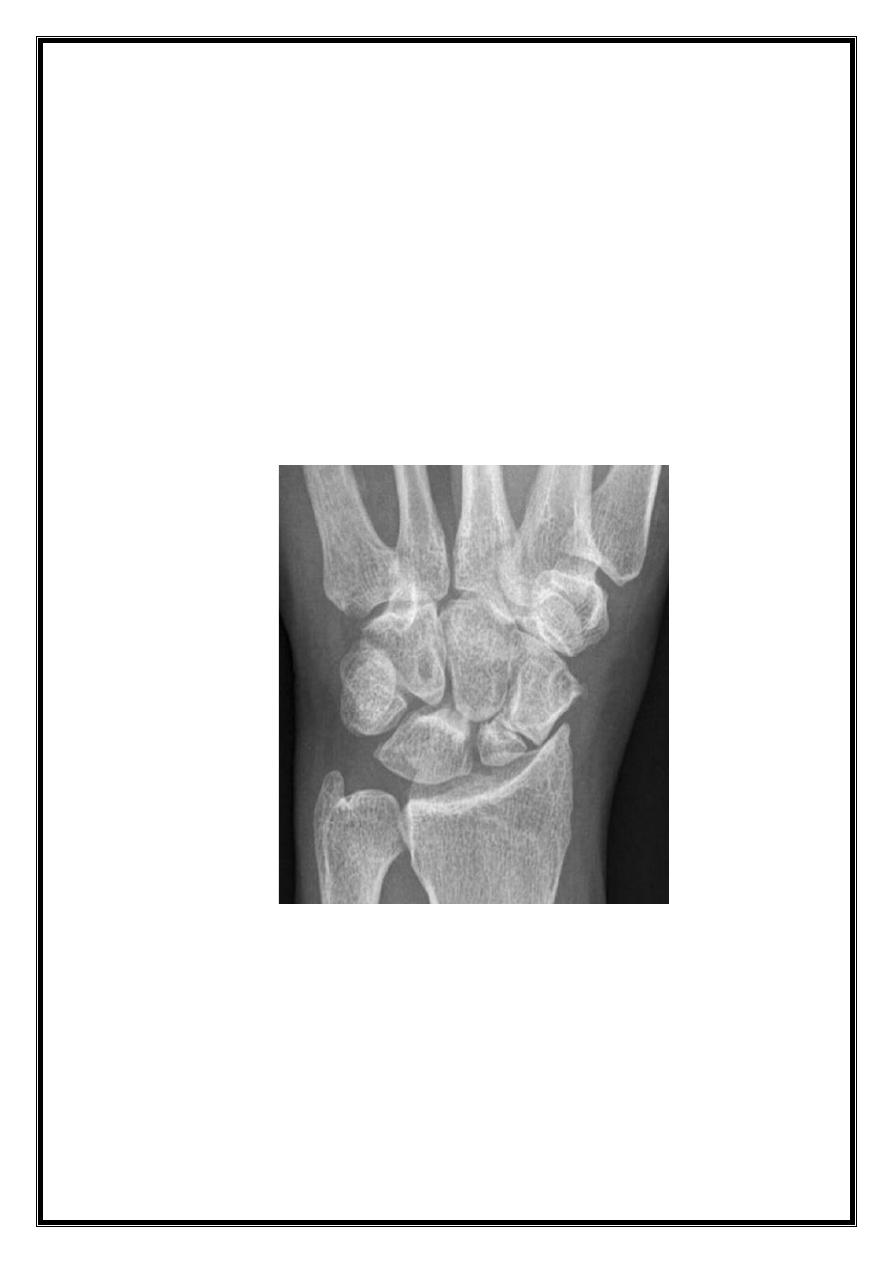
# Waist
# distal pole
5
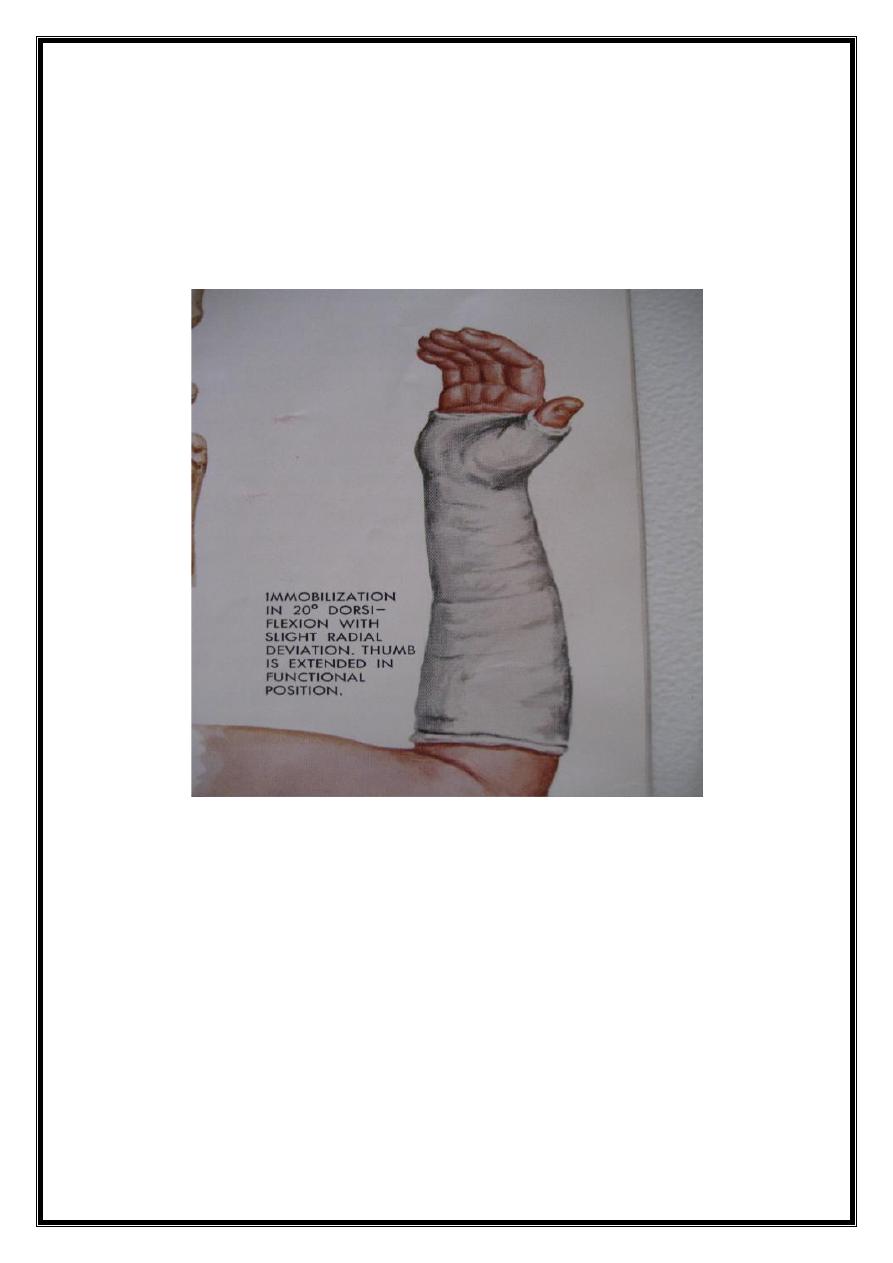
Treatment
Tubercle # – just crepe bandage
Undisplaced # -- POP from upper forearm to just short of
MPJ incorporating proximal phalanx of thumb
wrist dorsiflexed and thumb forwards in (Glass holding
position) for 8 weeks.
After 8 weeks remove the POP and examine the wrist
clinically & by X Ray
No tenderness & X Ray shows signs of healing —wrist left
free (complete X Ray union may take 4 to 6 months)
There is tenderness & in X Ray # line still visible (no
healing)—Reapply the cast for another 4 weeks.
6
At that stage (after 12 wks) one of these pictures may emerge
1. Painless wrist & # had healed—discard the cast
2.
Delayed union, X Ray shows bone resorption & cavitation
around the # which needs bone graft & internal fixation.
3.
There is established Nonunion
In unstable displaced #s of scaphoid or when associated with
carpal dislocations better treated by open reduction & internal
fixation.
Complications
1. Avascular Necrosis Proximal fragment may die especially
after proximal pole
& waist #s (30%)
X Ray; at 2 to 3 months it appears dense (sclerotic proximal
piece)
7
2. Nonunion may be obvious by 6 months
X Ray: gap is present with sclerotic # edges Hard borders as
extra carpal bone but viable bone.
Treatment :
In young; Bone graft + or-screw fixation
In elderly; with no pain may be left untreated
4. Osteoarthritis of the wrist may be a sequale to nonunion
& avascular necrosis
Treatment
If OA is localized — Excise radial styloid
If OA changes progress involving mid carpal joint:
proximal row carpectomy , or excision of scaphoid with 4
corner fusion .
If OA changes progress to Radiocarpal joint,
then: wrist Arthrodesis
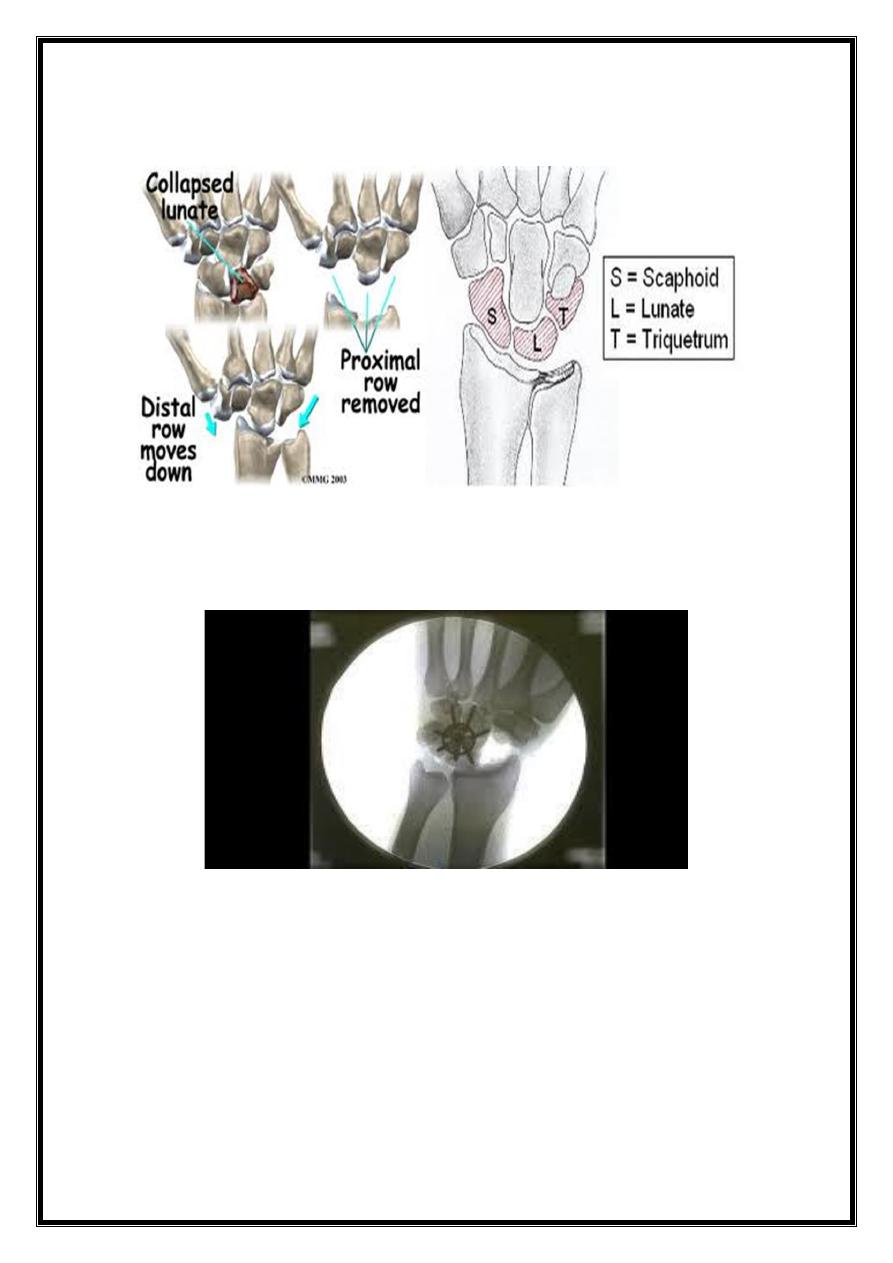
8
Proximal row carpectomy
Four –angle fusion
Carpal dislocations
fall with hand forced into dorsiflexion-tear intercarpal
ligaments
Lunate dislocation
Perilunate dislocation
Transsaphoid perilunar # dislocation
9
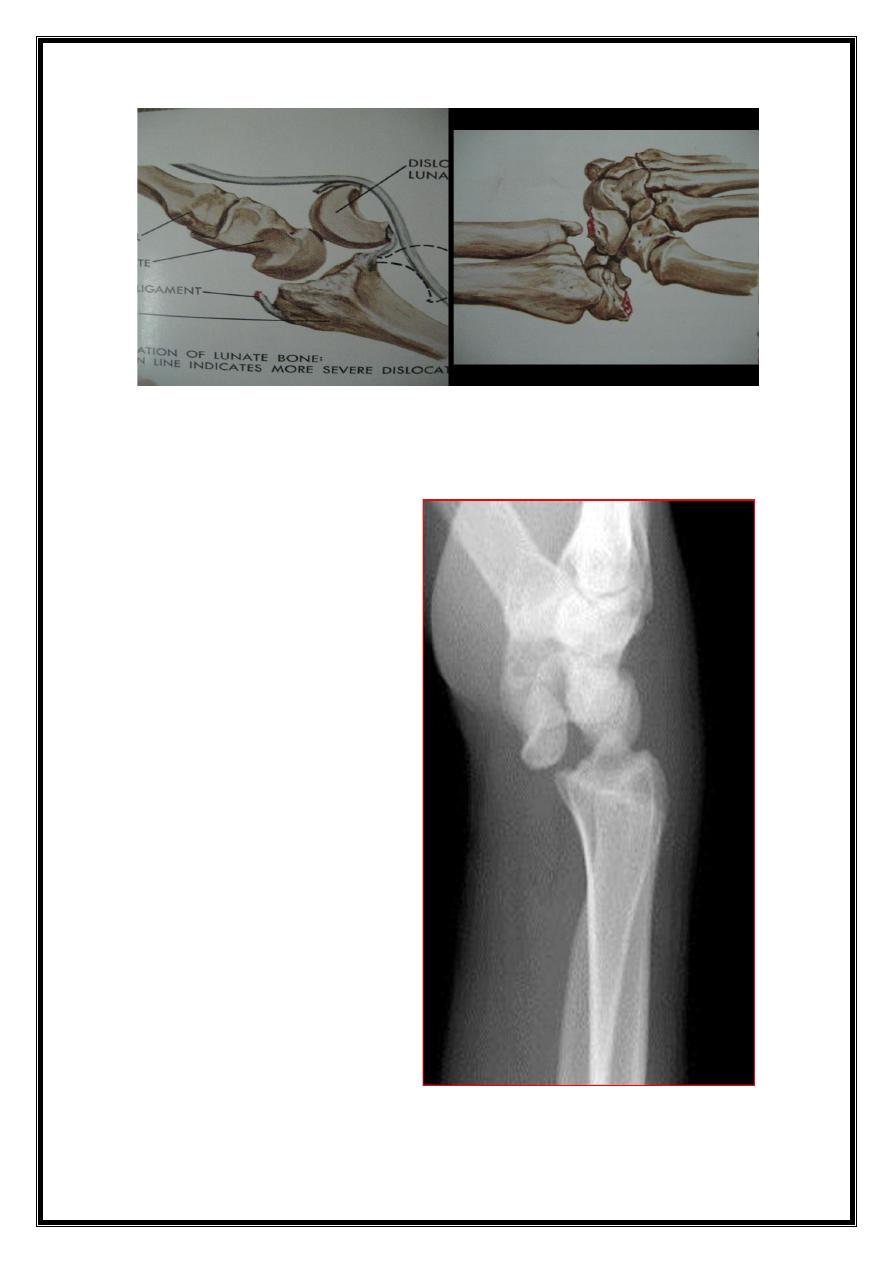
Lunate dislocation
10
Perilunate dislocation
Transsaphoid perilunar # dislocation

11
C/F; painful swollen wrist, sometimes with compression of
median nerve
X Ray: if lunate dislocated it appears triangular in shape
(normally quadrilateral) # Scaphoid
Treatment
try close reduction& cast if failed
do open reduction & IF
12
Wrist Sprain
Wrist Sprain: Should not be diagnosed unless more severe
injuries has been excluded
Fall on the hand (trivial injury) may torn the ligaments &
later may develop carpal instability
C/F; Painful swollen wrist with local tenderness
X Ray; may be normal, look for # scaphoid & carpal
dislocations
Treatment;
Serial X Rays later are important
Initially crepe bandage or plaster splints and after 2 to 3
weeks repeat the X Rays if still normal observe the
patient till symptoms settle down If in doubt sent for CT
or MRI .
144'8+