Skull and brain imaging
By
Dr. Firas Abdullah
Aims of our lectures:
To know the normal appearance of skull on X-ray
To learn the normal CT and MRI of brain and skull
To discuss some cerebral pathologies and see some
cases of trauma
To know about pathology of sinus, orbit, and neck
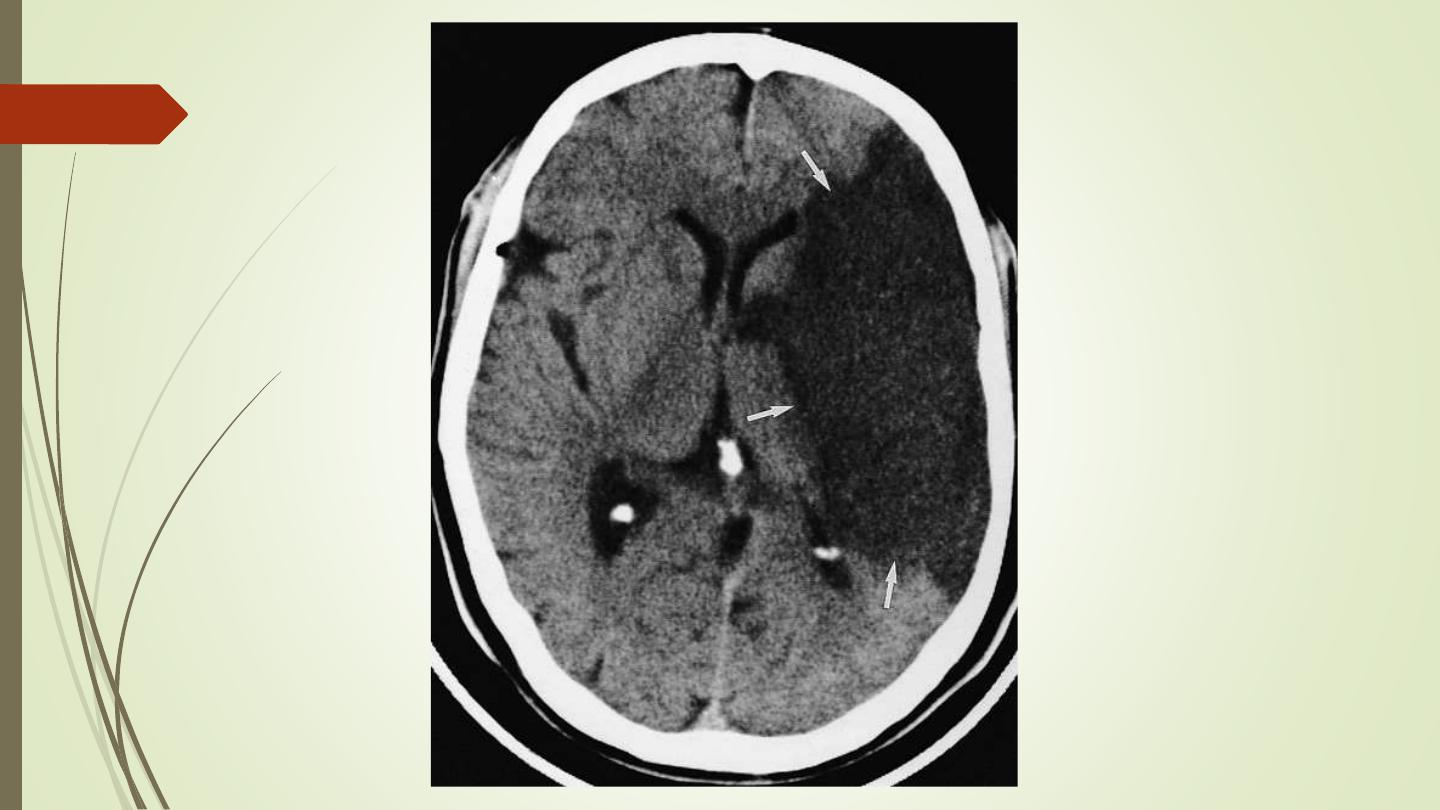
Cerebral infarction:
• Changes of acute infarction are not usually recognized on CT
before 6 hours
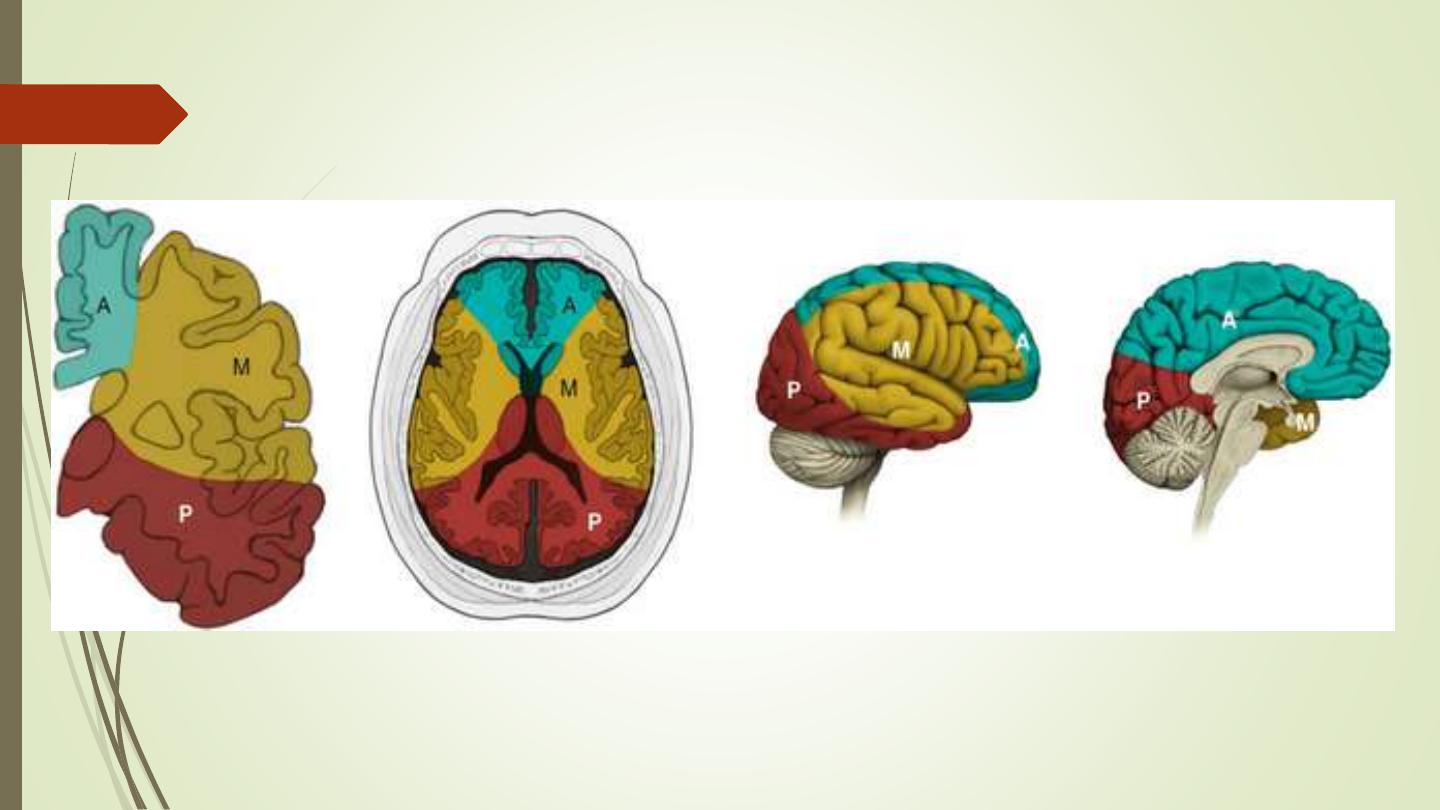
• Over the next few days the infarct evolves into a low attenuation
area conforming to the shape of a recognizable arterial distribution
• The infarct may gradually resolve, leaving an atrophic area and/or
a persistent scar
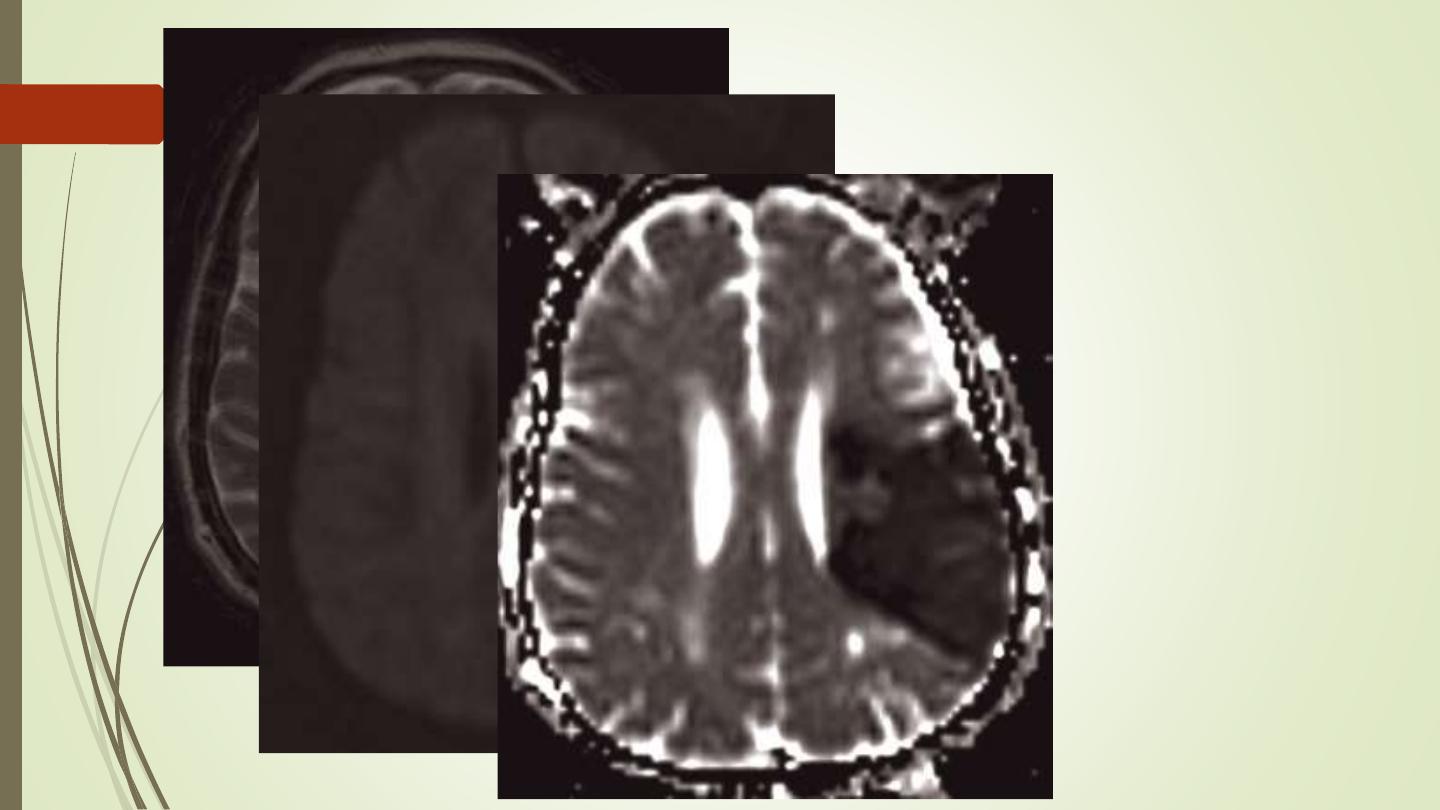
• MRI scanning : hyperintense areas on a T2-weighted scan, within 8
hours of the onset of symptoms. Special fast scanning techniques
such as perfusion / diffusion scans show changes within minutes of
the onset of symptoms.
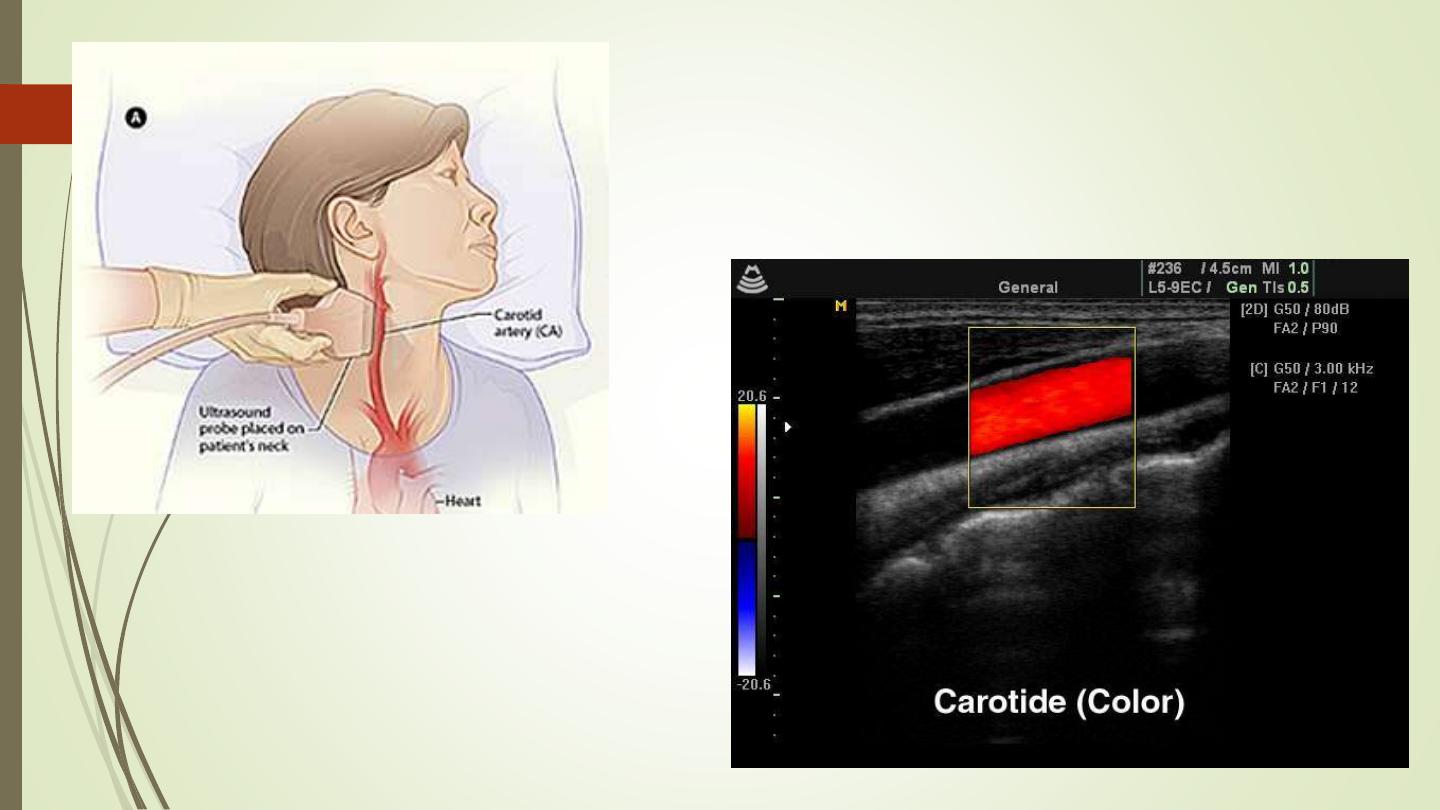
• Patients whose symptoms resolve within 24 hours are
referred to as having a transient ischaemic attack (TIA). A
common cause for a TIA is embolus from an atheromatous
stenosis of the internal carotid artery. The presence of
atheromatous plaque and degree of stenosis can be
assessed with Doppler ultrasound of the neck. Ultrasound
can also demonstrate a dissection of the carotid artery in
the neck.
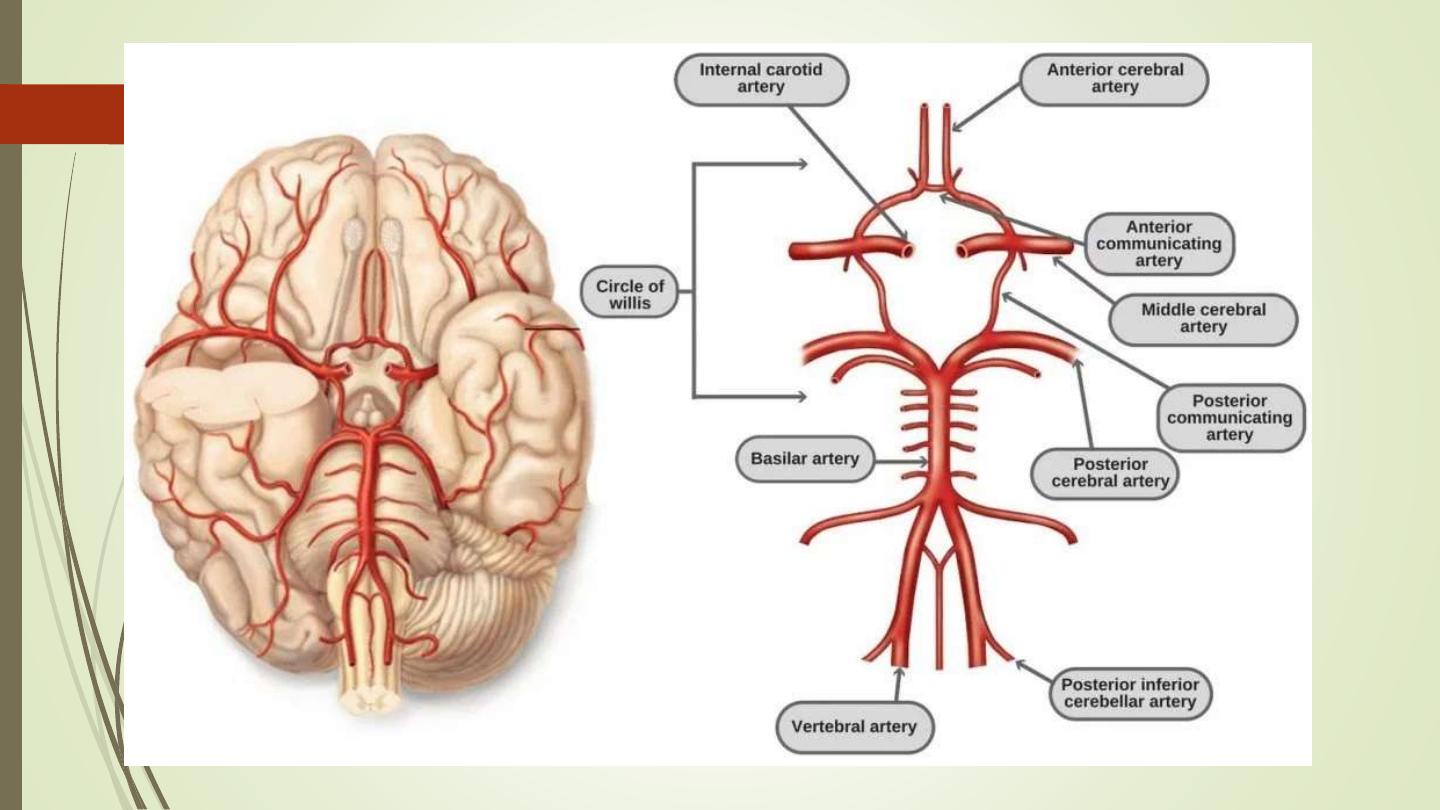
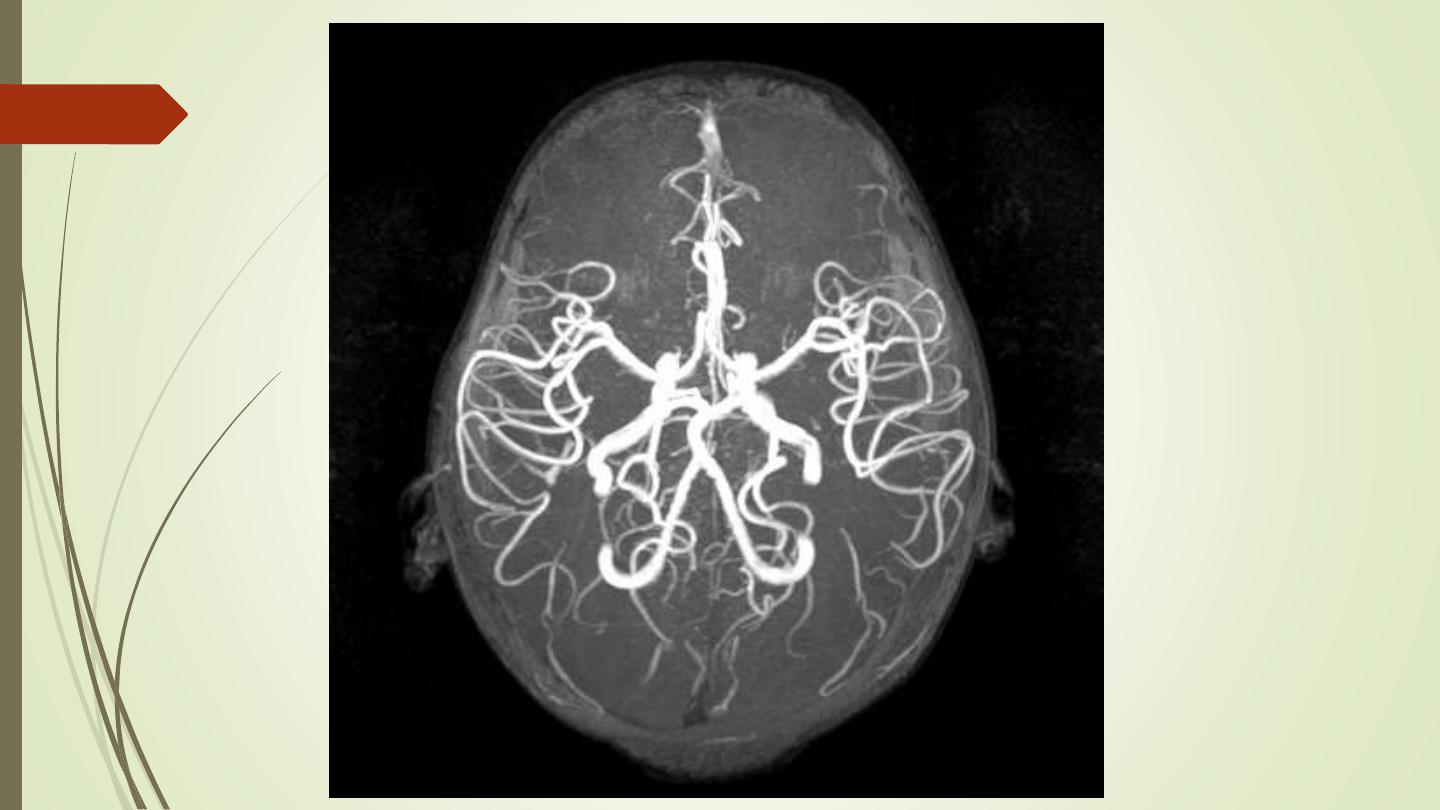
• The cerebral vessels may be imaged non-invasively with
MR angiography (MRA).
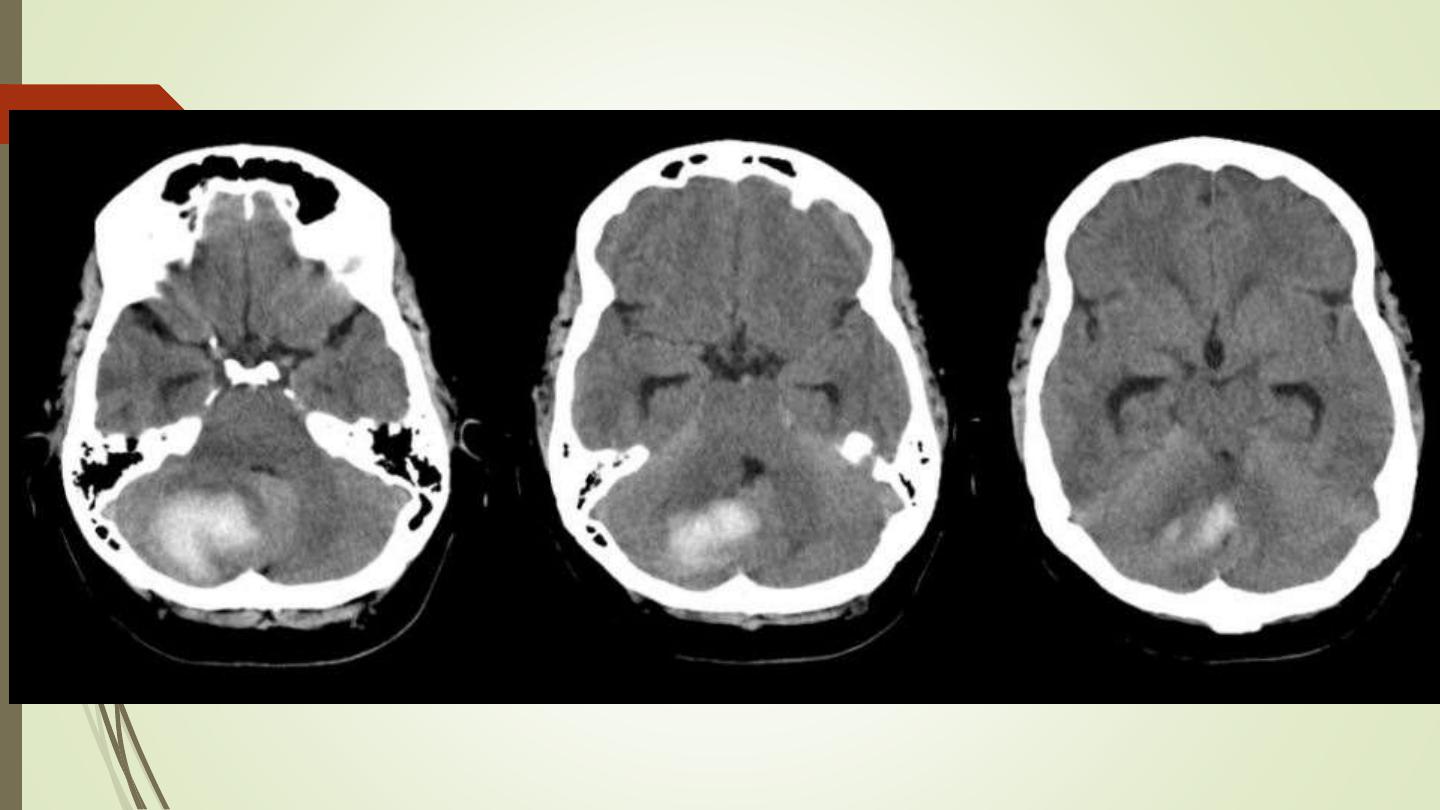
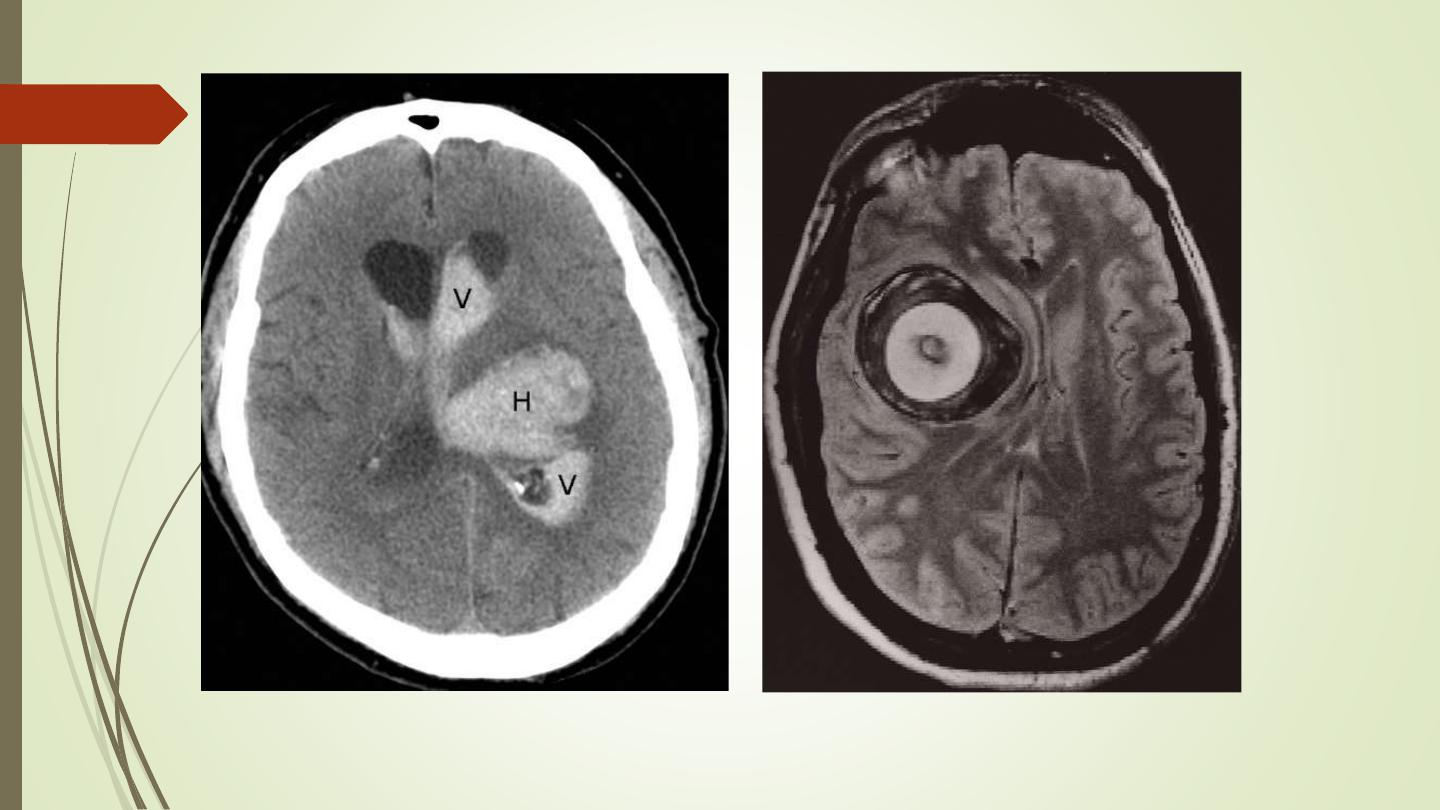
Cerebral haemorrhage:
• Haemorrhage is demonstrable on CT immediately after the
event as a region of high attenuation
• Frequently causing mass effect.
• The initial high density of haemorrhage lessens over the following
week or two leaving a low- density area indistinguishable from
an infarct.
• May be associated with intraventricular or subarachnoid
bleeding

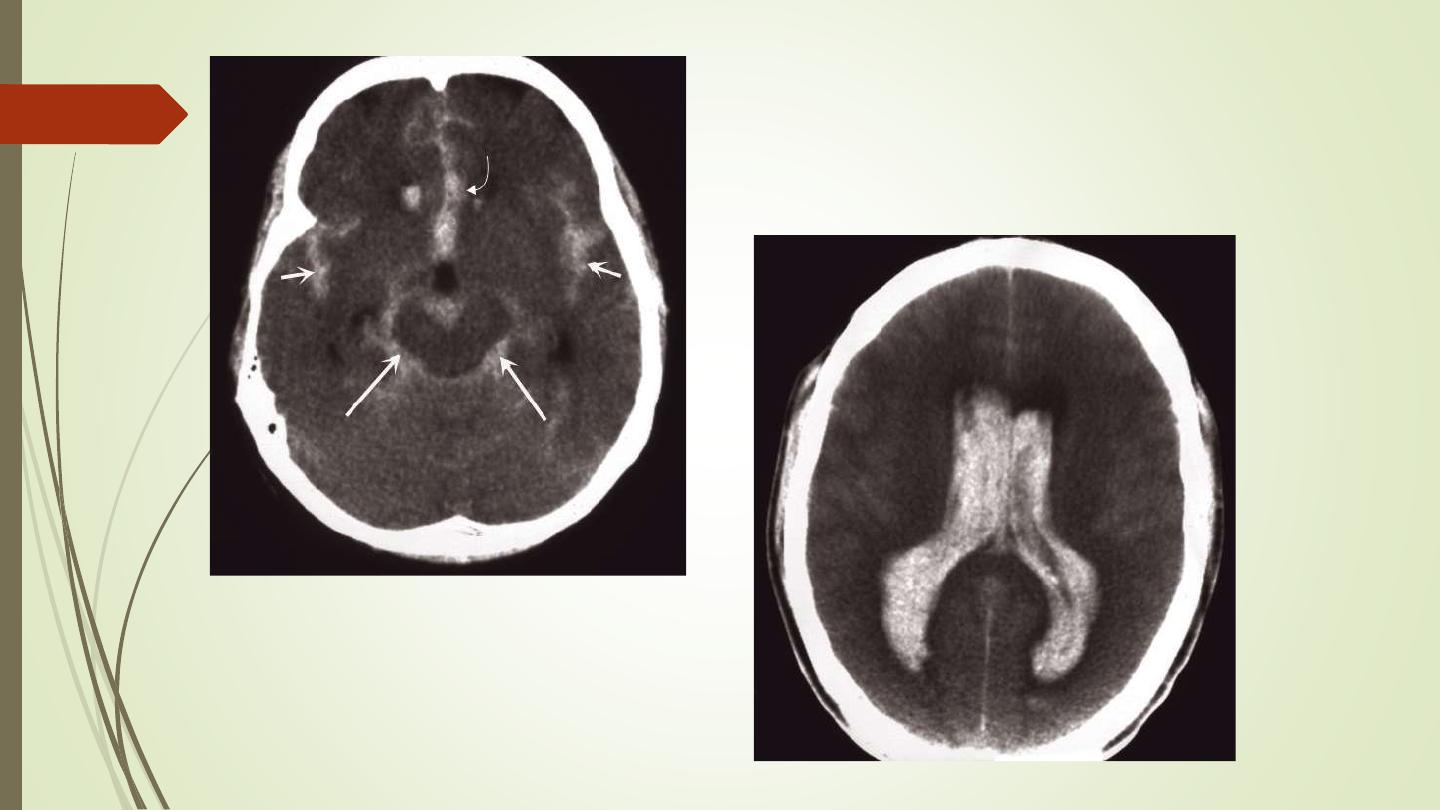
Subarachnoid haemorrhage
• Usually due to a ruptured intracranial aneurysm or less commonly
an arteriovenous malformation.
• CT is the best initial investigation to diagnose.
• A subarachnoid haemorrhage is recognized by high density blood
in the cortical sulci, Sylvian fissures and basal cisterns.
• CT will also show any intracerebral haemorrhage or blood in the
ventricles
• An unenhanced routine head CT is followed by CT angiography as
a single investigation to diagnose subarachnoid haemorrhage,
localize the bleeding and demonstrate the aneurysm.
Head injury
• Computed tomography is performed without intravenous
contrast administration
• brain and bone window.
• Computed tomography can distinguish between extracerebral
and intracerebral lesions
• CT can also demonstrate fluid levels in the sinuses and mastoid
air cells suggesting a facial or skull base fracture, air in the orbits
and in severe head injury, air in the cranial cavity.
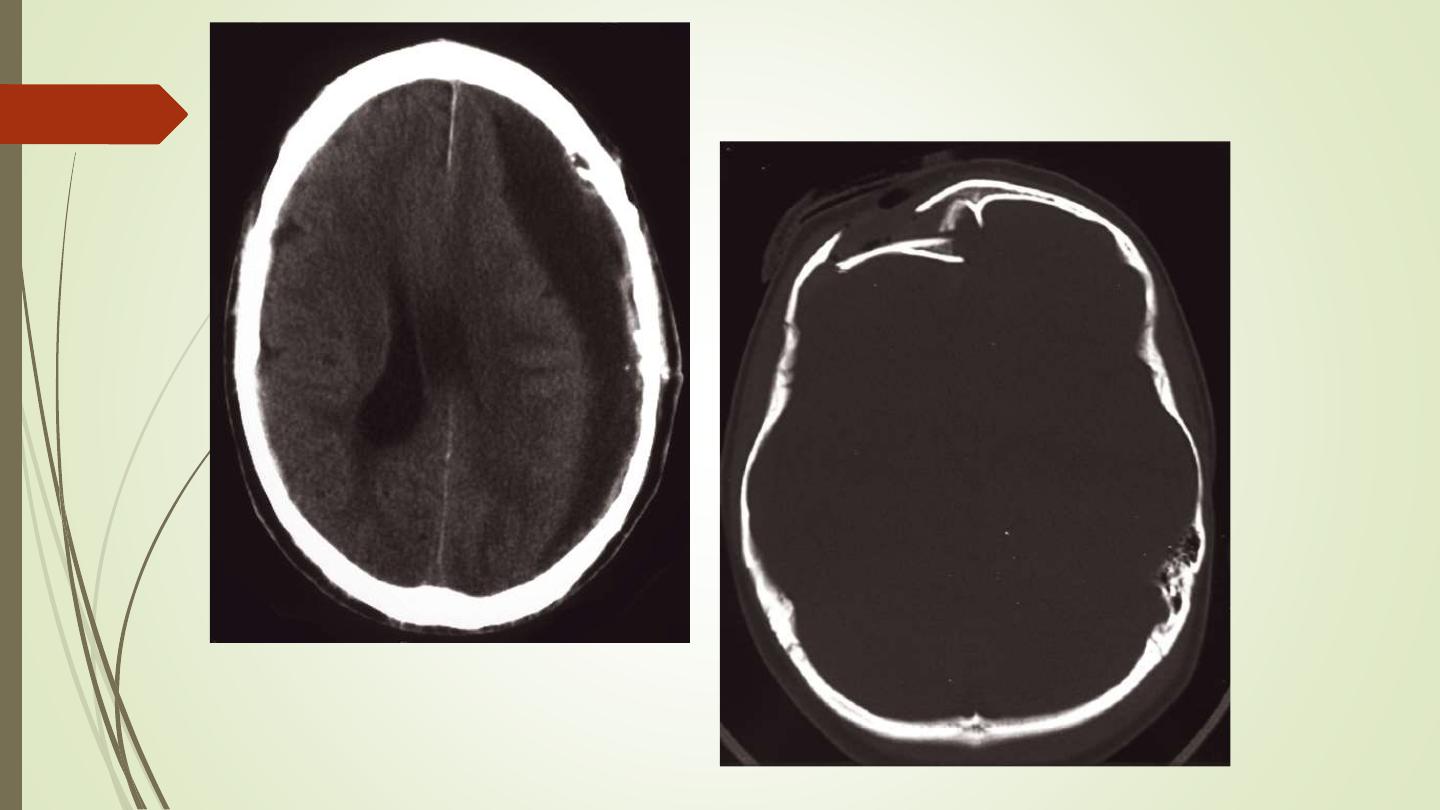
• Examination on bone windows can demonstrate fractures of the
skull vault, face or skull base.
• Extracerebral haematomas show a high density for about 1–2 weeks
following the injury, but after 3–4 weeks the density decreases to
become lower than that of the brain. In the intervening period,
haematomas pass through a phase of being isodense with the brain
• Causes Midline or ventricular displacement.
• Extradural haematoma is seen as a lens-shaped, smoothly
demarcated, high-density area situated over the surface of the
hemisphere associated with a skull fracture
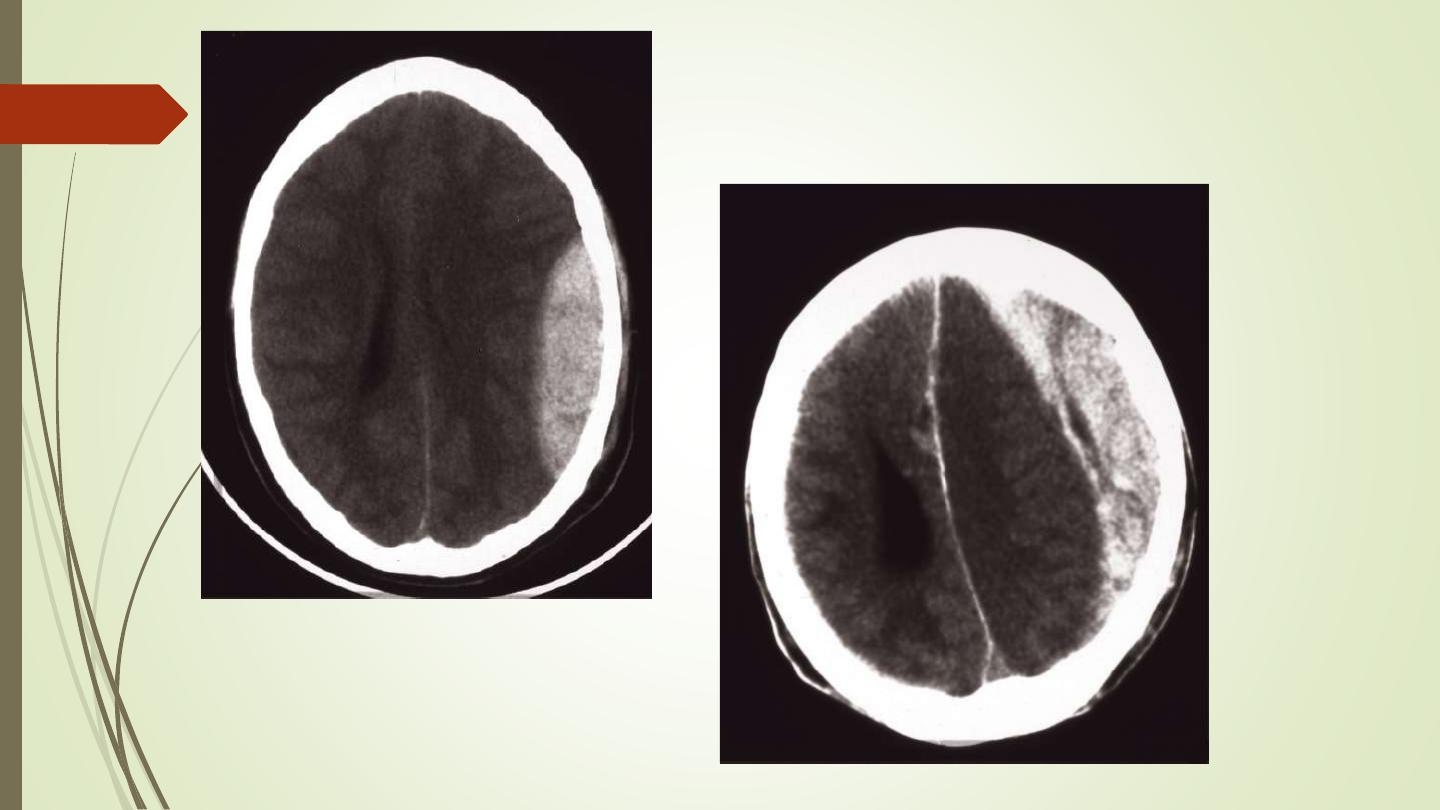
• Subdural haematoma conforms to the shape of the underlying brain
(crescentic shape) and occurs most commonly over the convexity of
the brain, but can also arise along the falx and tentorium
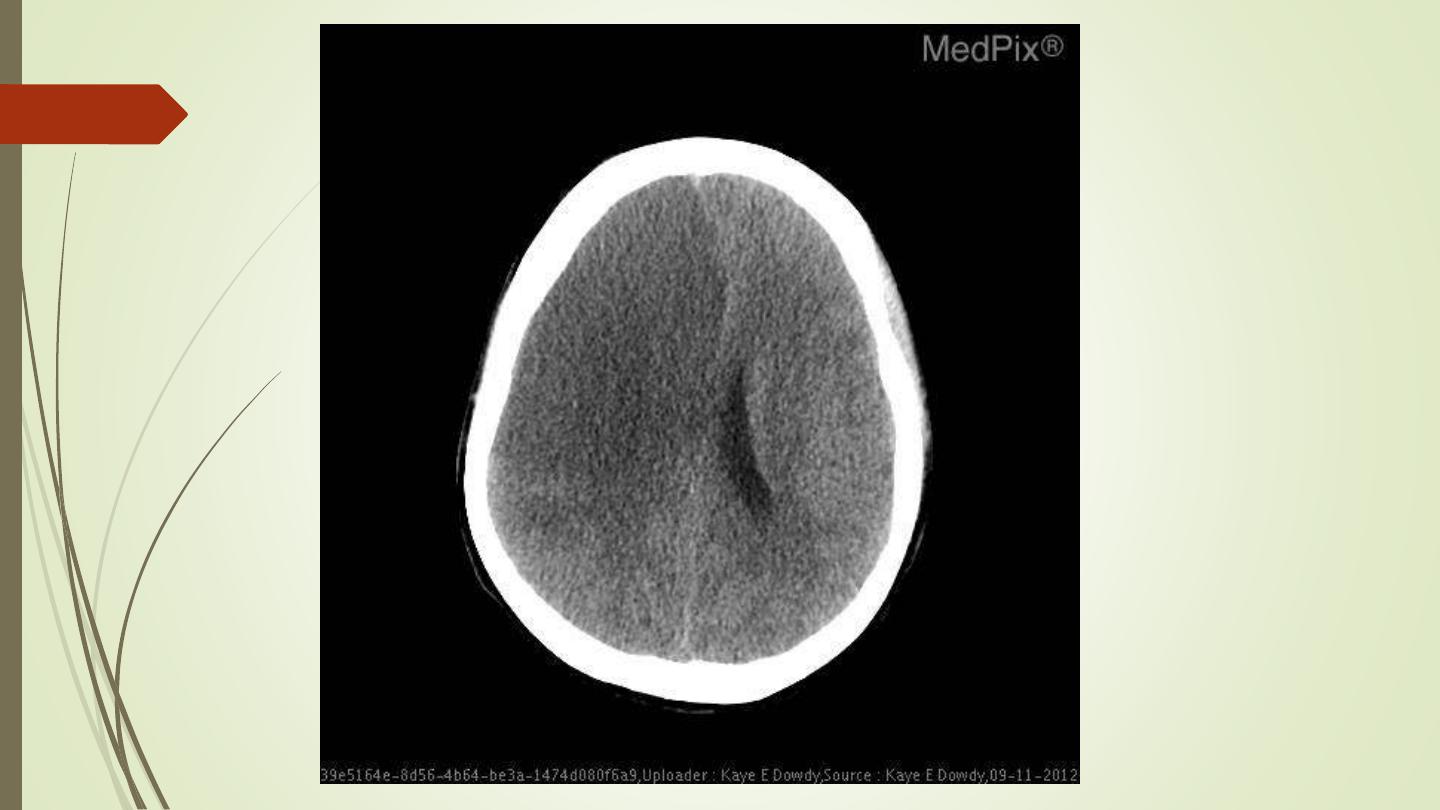
• Contusions are bruises of the brain which appear as areas
of low attenuation and may be associated with high-
density areas due to haemorrhage.
• Intracerebral haematomas are seen as areas of high
density, which may be multifocal. There may be mass
effect causing displacement of the ventricles and
accompanying brain oedema.
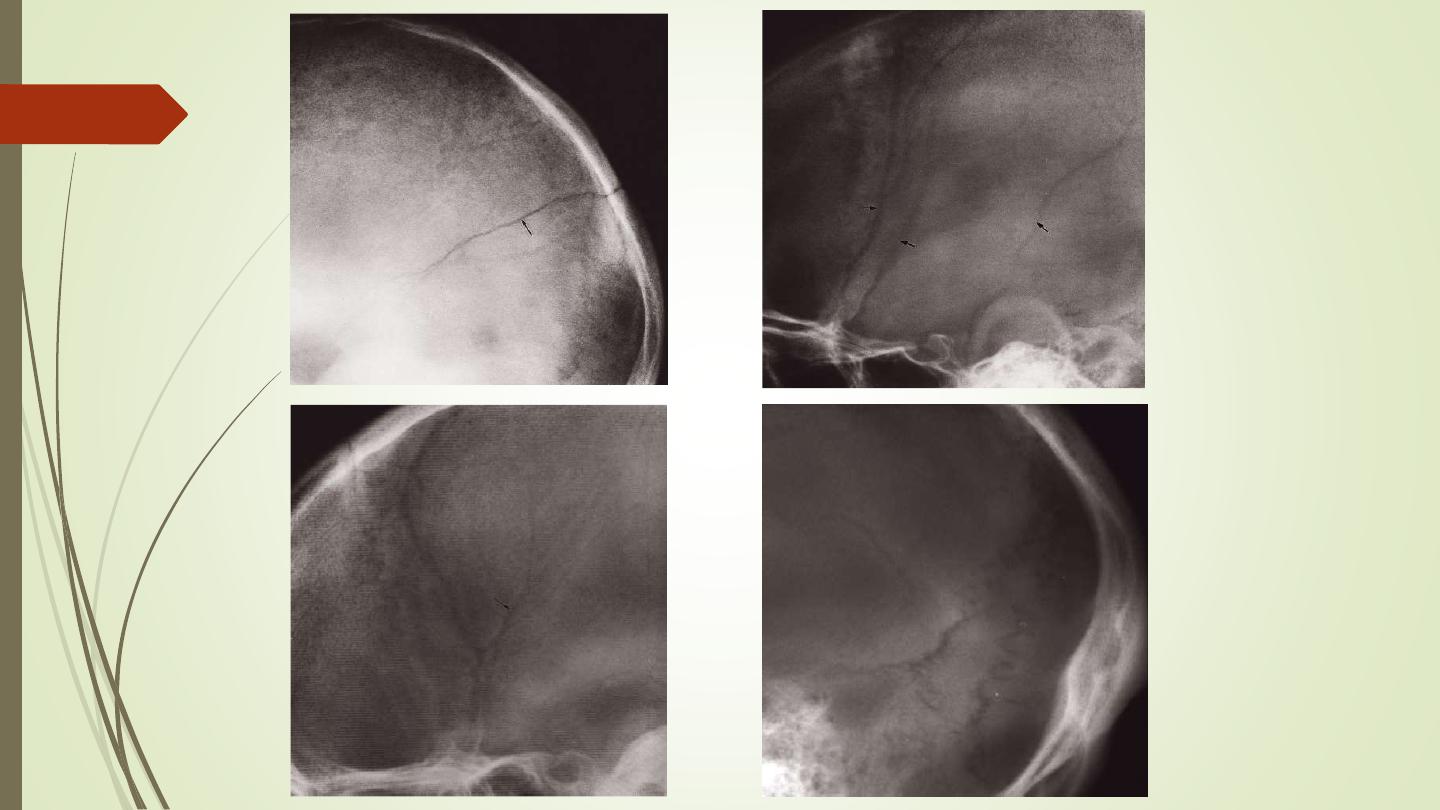
• Fractures of the skull base or vault should be looked for on
bone window settings.
• Assessment of fracture type: linear or depressed . Also
assessment of Paranasal sinuses, sphenoid, petrous and
occipital bones
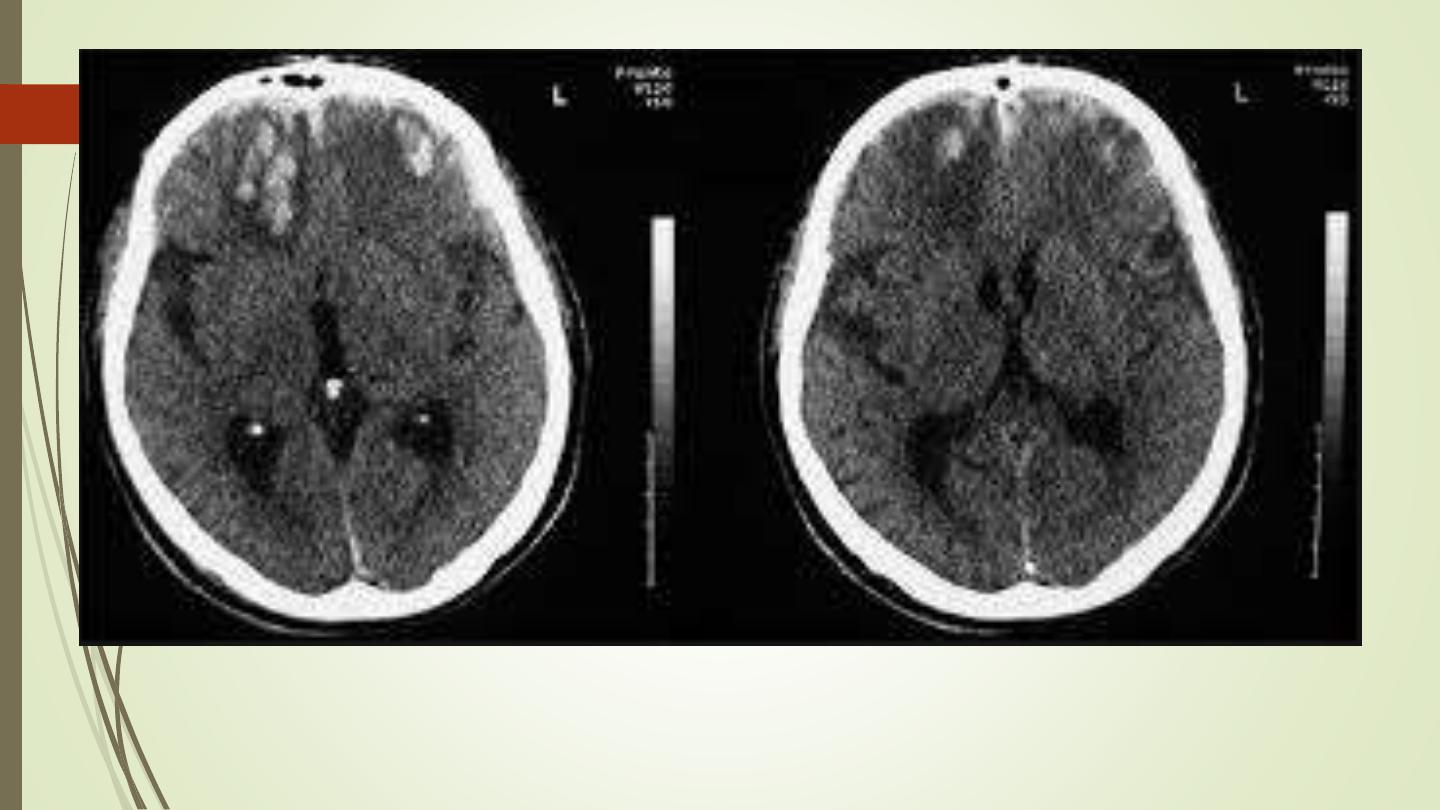
Brain Contusion

Thank you