


Bone Tumours II
Dr. Wahby GhalibFJMC, CABO, MRCS
Giant cell tumour
= osteoclastomaBenign but locally aggressive
Histology : abundant multinucleated giant cells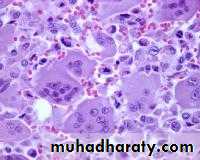
Age : 20-40 yr
Site : around the knee
distal radius
Metaphyseal-epiphyseal


XR : soap – bubble appearance
Rx : curettage + tumouricidalHi recurrence rate
Malignant potential : 5%Osteosarcoma
Commonest primary malignant bone tumour in child
Highly malignantHistology : malignant cells
producing osteoid10% metastasis at presentation
C/FAge : 10 -25 yr
Pain : constant & more at night
SwellingPathologic # : rarely
XRMetaphyseal lesion
Usually around the knee
Osteolytic & osteoblastic areas
Soft tissue invasion sun-ray appearancePeriosteal elevation Codman`s triangle


Rx
CT + surgery
5 yr survival : 60 %
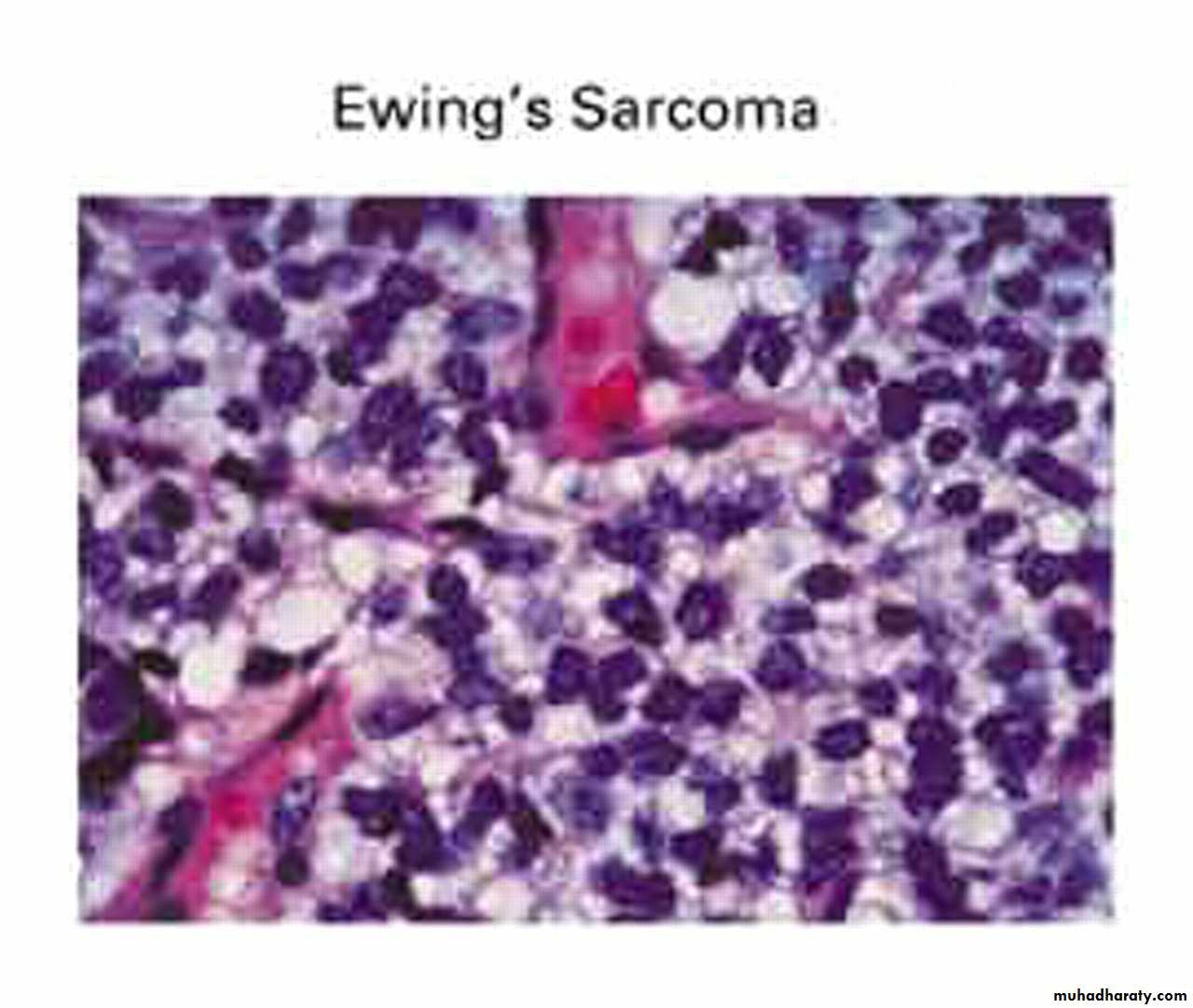
Ewing sarcoma
Highly malignant
Histology : small round cells25 % metastasis at presentation
C/F
Age 10 -25 yr
Pain
SwellingGeneralized illness & fever
Pathologic # rare
XR
Diaphyseal lesion
Tibia & fibula more common
New bone formation multiple layers onion – peel appearanceRx
CT + surgery
5 yr survival : 60 %
ChondrosarcomaSlowly growing
Primary or secondary to preexisting lesionC/F
Age 40 -50 yr
XR
Lytic lesion + flecks of calcification



Rx
Surgery
Radio- & chemoresistant
5 yr survival 60 %Objectives :
Stressing the importance of the bone tumours as being a significant source of mortality and morbidity.Training the students to acquire the basic skills of XR interpretation in case of bone tumours.
Objectives :
Emphasizing the general outlines of treatment including the medical and surgical lines.Emphasizing the significance of classifying the bone tumours and the tumour-like conditions.