


Hair Problems
Types of hair:1 Lanugo hairs.
Fine long hairs covering the fetus before birth.
2 Vellus hairs.
Fine short hairs covering much of the body surface.3 Terminal hairs.
Coarse long hairs e.g. scalp or pubic hair.The hair cycle:
There are three phases of follicular activity.
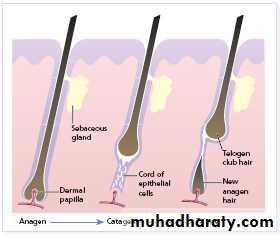
1 Anagen :
active phase of hair production.
2 Catagen :
short phase of conversion from active to resting phase.
3 Telogen :
resting phase at the end of which hair is shed.
Regarding the scalp hair:
Anagen lasts 3 years, catagen 3 weeks, and telogen 3 months.85% of hairs in anagen , 15% in the telogen.
Scalp contains an average of 100 000 hairs, and shed about 100 hairs/day as a normal consequence of cycling.
Hair growth rate is 1 cm / month.
Alopecia
means loss of hair which has many causes.Alopecia is divided into
-Localized (patchy)-Diffuse.
Each in turn is divided into
-Scarring
-Non-scaring
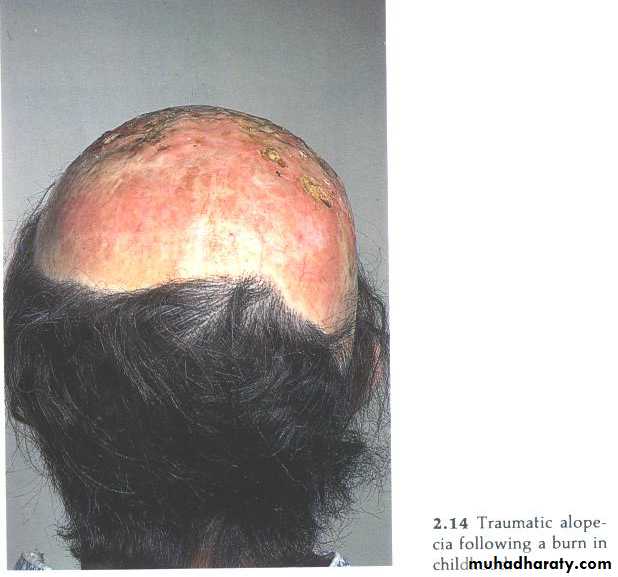
Scarring localized hair loss
Hair follicles can be damaged in many ways.If the follicular openings can no longer be seen with a lens, regrowth of hair cannot be expected.
Causes:
trauma,
burn,
carbuncle,
Kerion
radiodermatitis.
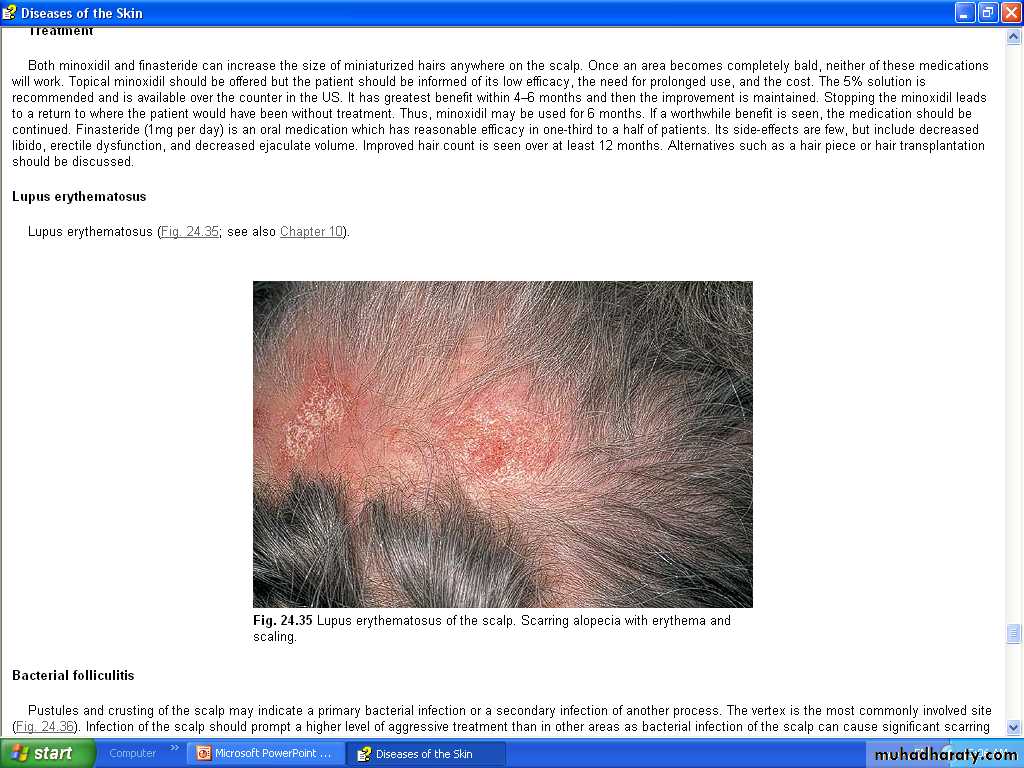

DLE,
lichen planus,morphoea
Epidermal warts,congenital naevi,
cysts and neoplasms

Pseudopelade
Slowly progressive non-inflamed type of scarring which leads to irregular areas of hair loss without any apparent preceding skin disease.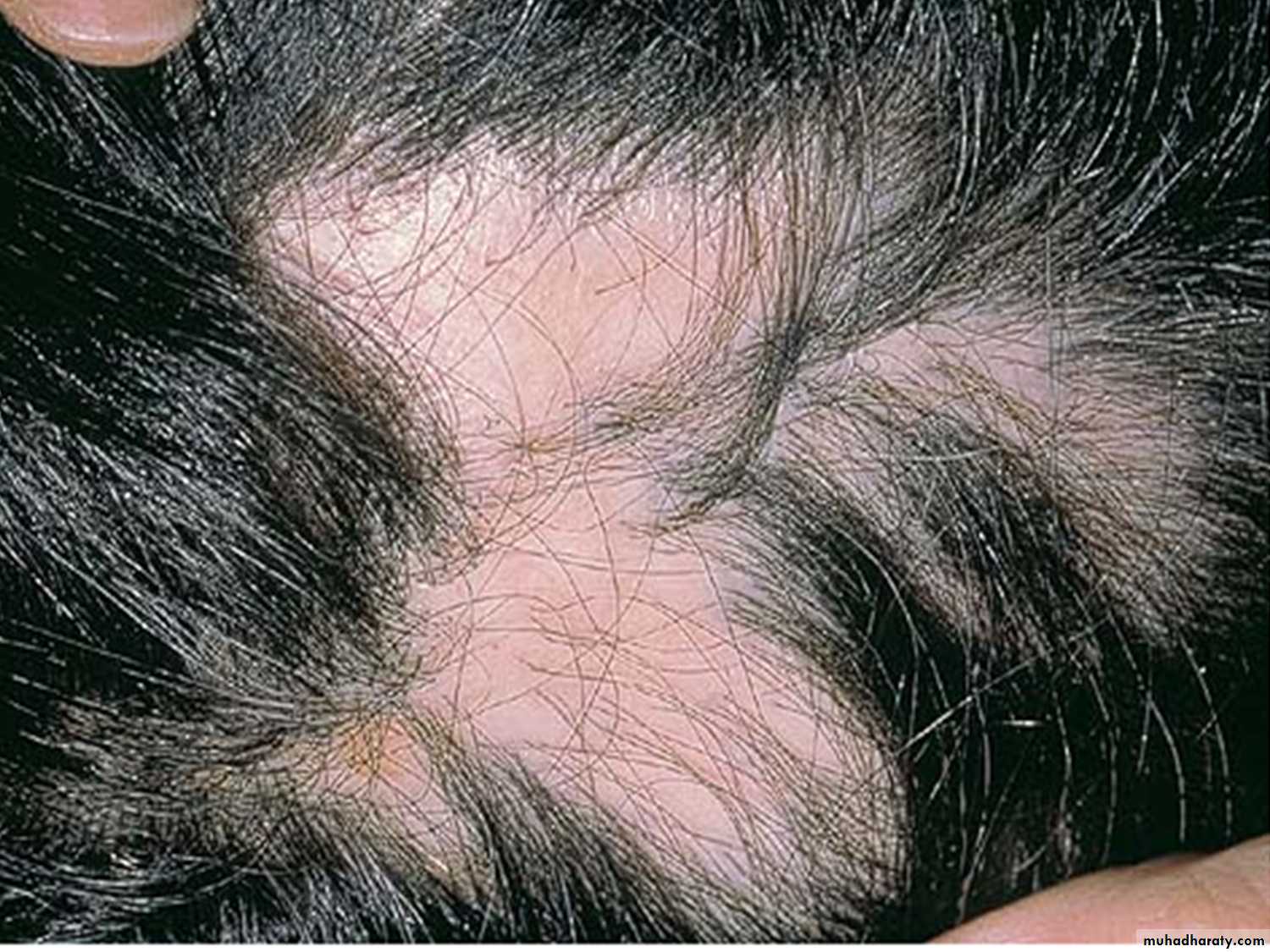
1-Alopecia areata:
Discussed later.2-Androgenetic alopecia:
Localized or a diffuse alopecia.Discussed later.
Non scarring localized hair loss
3-Neonatal alopecia:
Transient, physiological event that occurs in the first 3 months of life,Probably due to estrogen withdrawal or trauma of labor.
Present mostly as patchy occipital hair loss (friction with the pillow) or sometimes as a diffuse hair loss,
Recover spontaneously (after a period) and needs no treatment.
4-Pyogenic infection:folliculitis or boil of the scalp may cause transient localized non-scarring alopecia,
followed by spontaneous regrowth that may last months.History of previous infection will suggest the diagnosis;
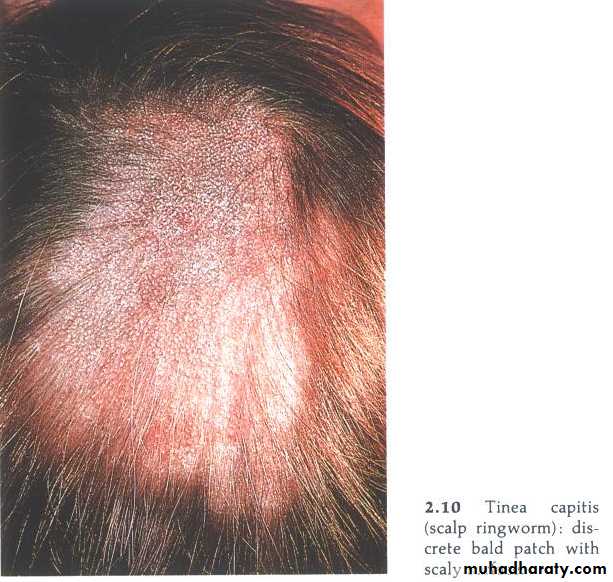
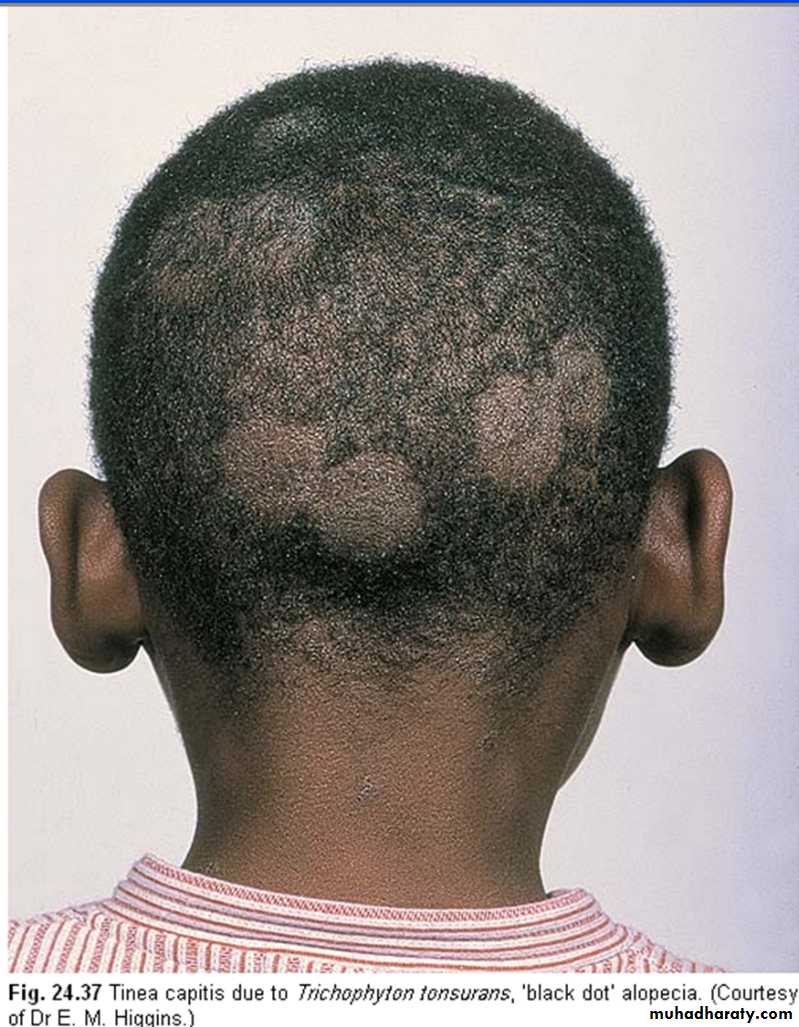
otherwise, it may be confused with alopecia areata.5-Tinea capitis (human):
a common cause among children in Iraq.The classical scalp ringworm derived from human sources causes areas of scaling with broken hairs.
6-Traumatic hair loss: 4 groups
A-Traction alopecia:
B- Hair-pulling habit (Trichotillomania):
C- Neurodermatitis:
D- Massage alopecia:
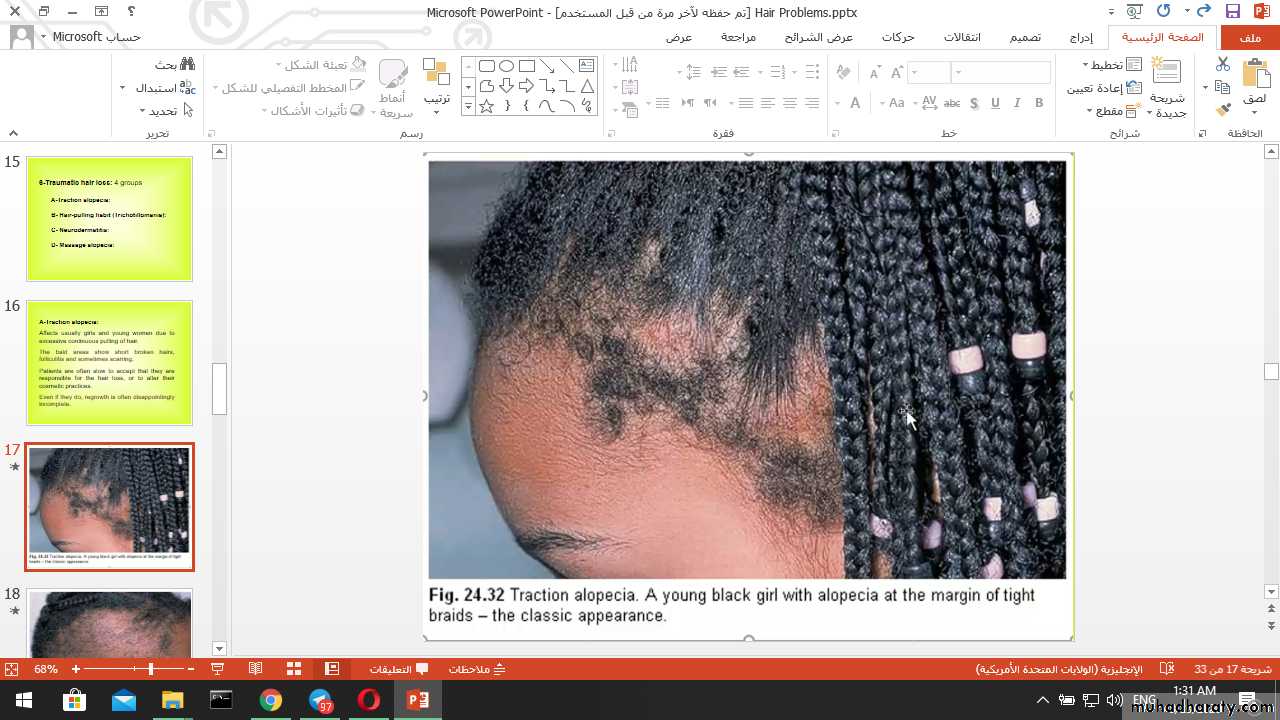
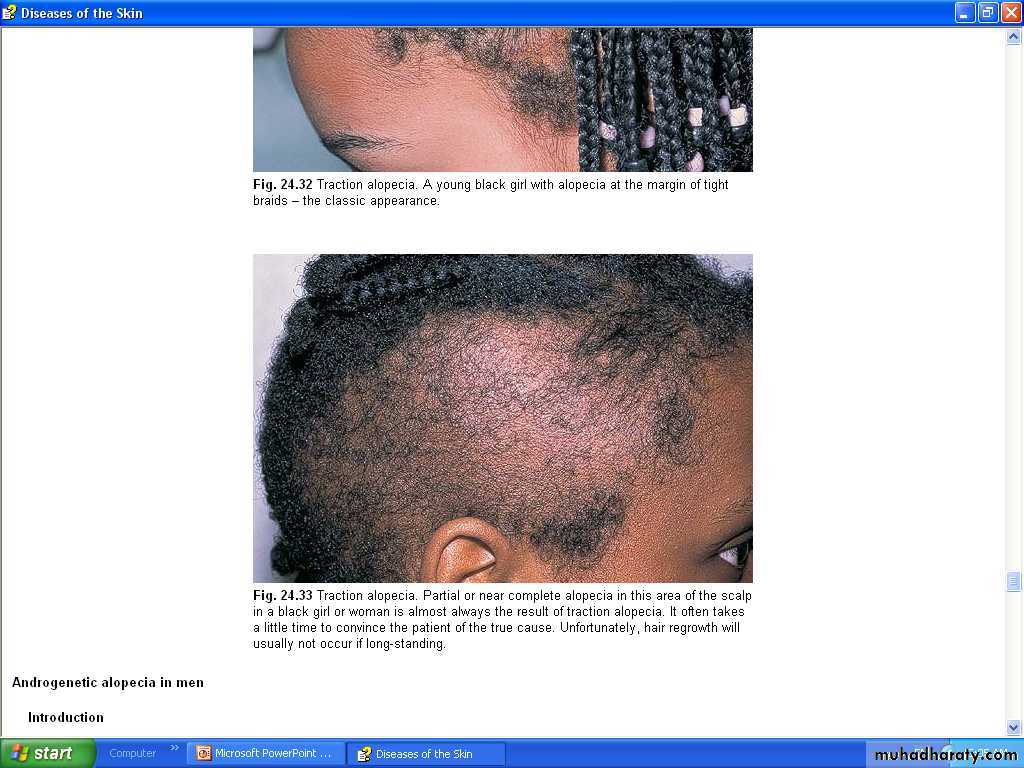
A-Traction alopecia:Affects usually girls and young women due to excessive continuous pulling of hair.
The bald areas show short broken hairs, folliculitis and sometimes scarring.
Patients are often slow to accept that they are responsible for the hair loss, or to alter their cosmetic practices.
Even if they do, regrowth is often disappointingly incomplete.
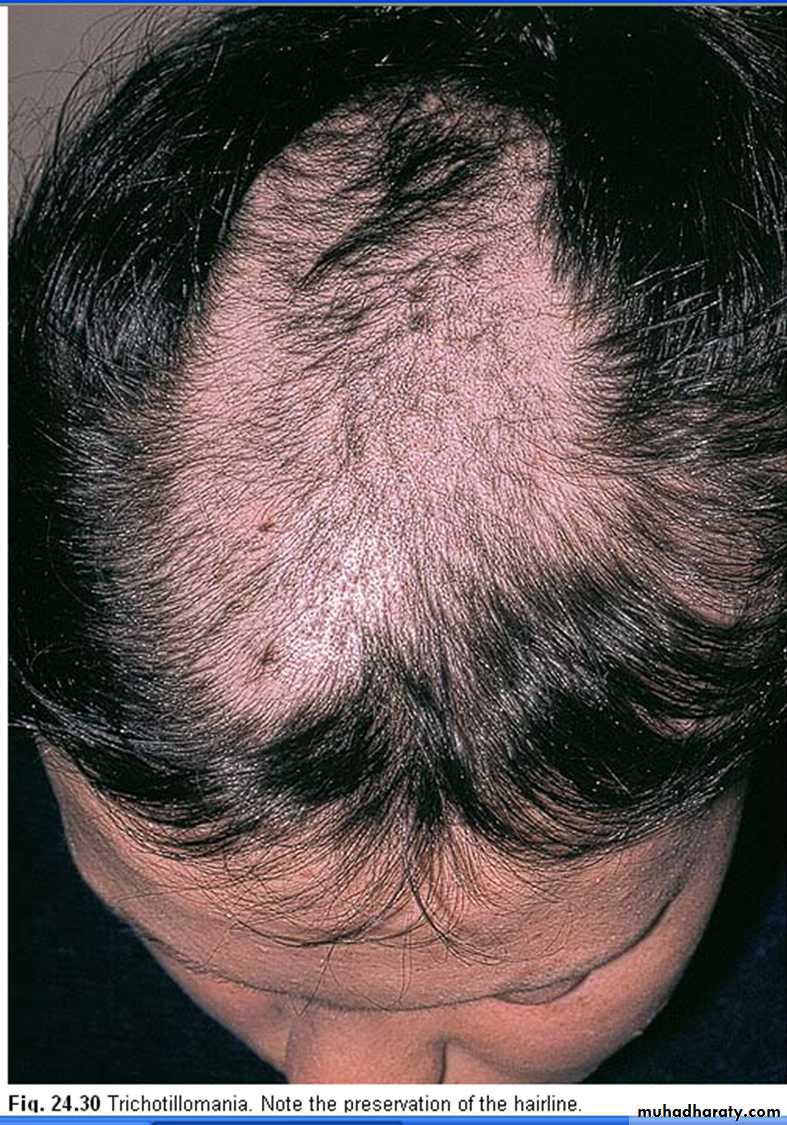
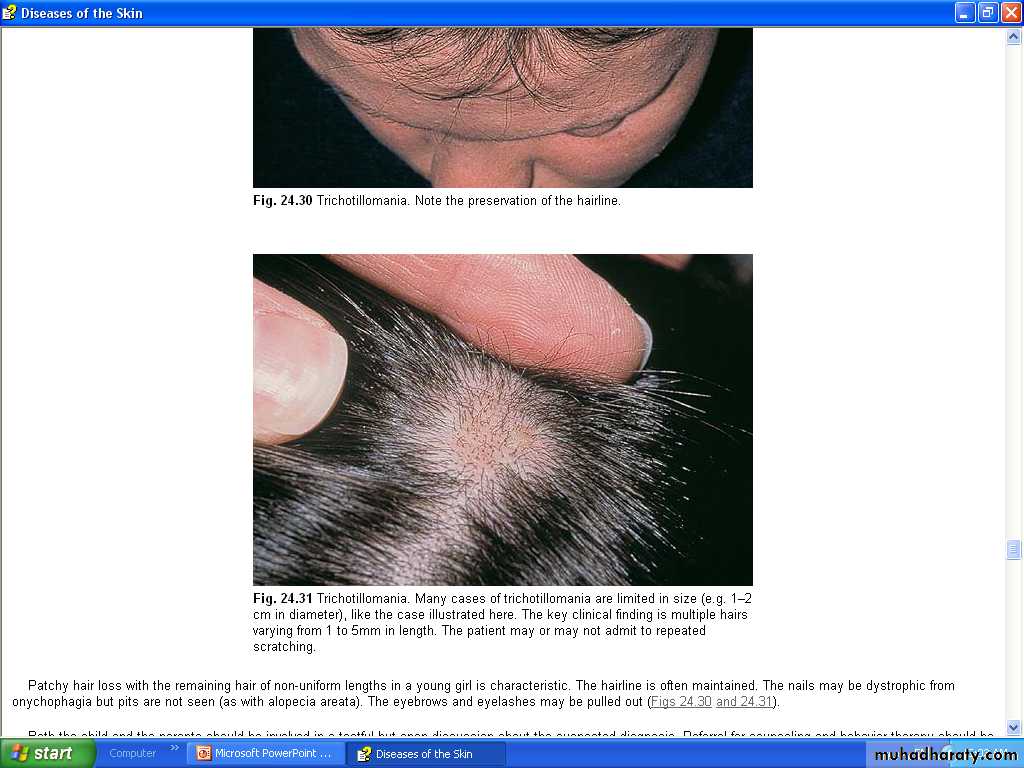
B- Hair-pulling habit (Trichotillomania):
Is a minor comfort habit in children or young adults.The hair is twisted and pulled continuously especially during psychological tension.
The bald areas are irregular in outline and hair loss is never complete.
Those hairs that remain are bent or broken, and of variable length.
Common sites are mustache in males, eyebrows and lashes in females, and scalp hair in both.
The patient usually deny the habit and some parents do not know what is going on.

C- Neurodermatitis:
is a disease of adults, with a habit of scratching a localized area under psychological tension.
In hairy areas this will result in alopecia with broken hair and hyperpigmented thick lichenified skin.
D- Massage alopecia:
by massaging the hair.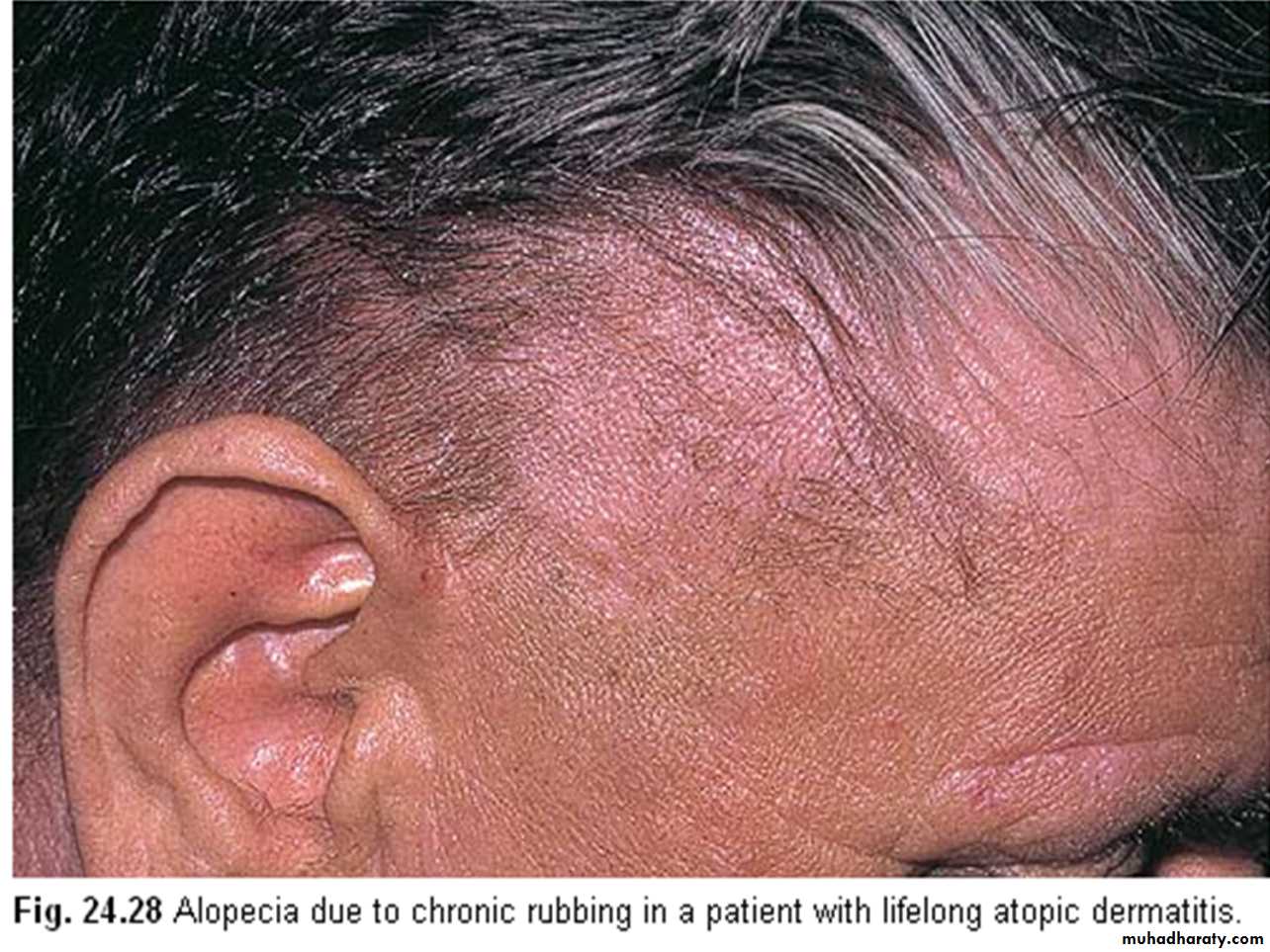
Alopecia areata
A common disease, affects 2% skin clinics' patients.It affects any age group, mostly 5-40 years
with equal male to female ratio.Cause:
An immunological basis is suspected because of an association with thyroid disease, vitiligo and atopy.Alopecia areata is probably inherited as a complex genetic trait, with a positive family history in 30% of cases.
The existence of trigger factors, such as stress, fits with this idea.
Presentation:Rapid and almost complete hair loss in patchy area(s).
usually asymptomatic and discovered by others.
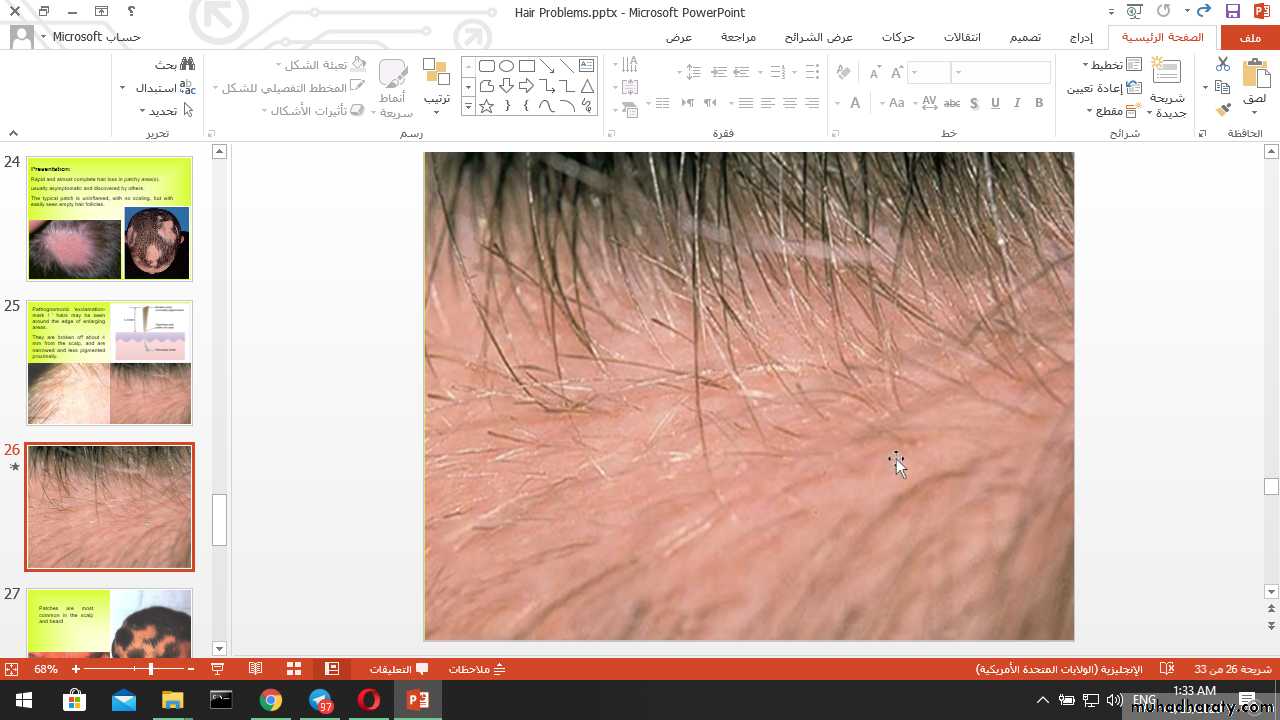
The typical patch is uninflamed, with no scaling, but with easily seen empty hair follicles.
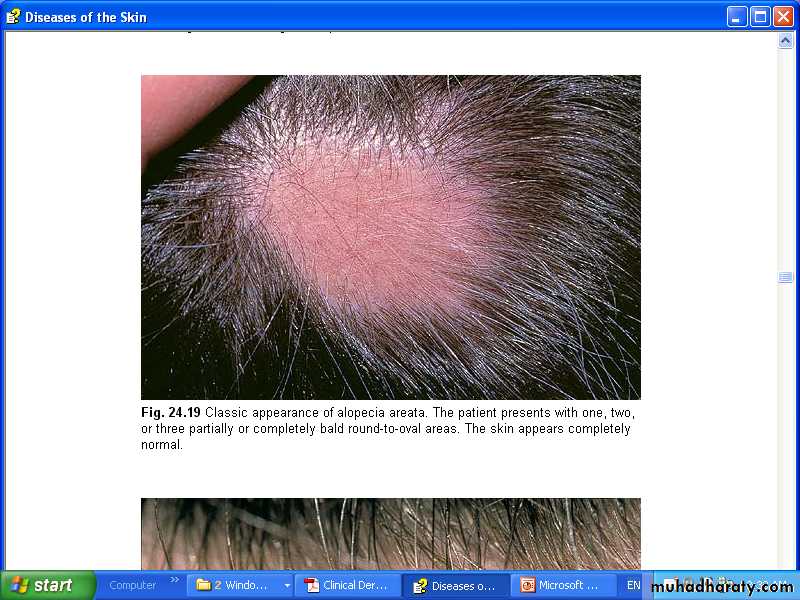
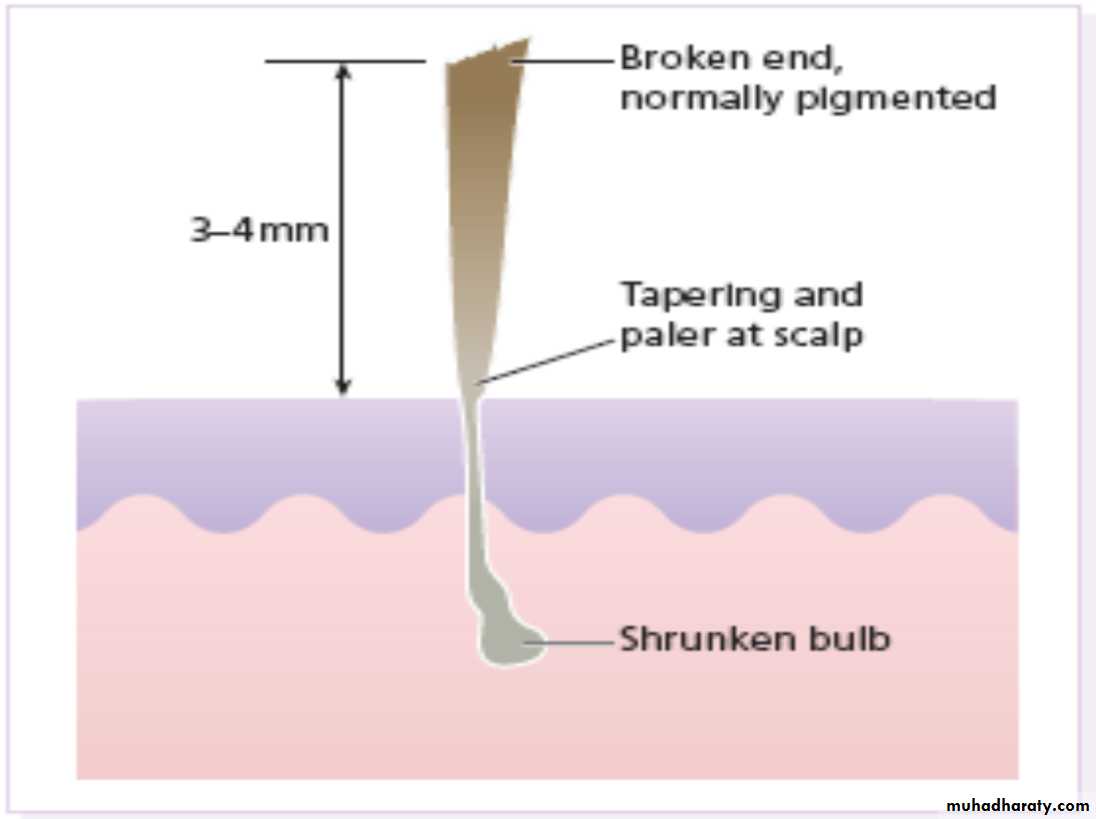
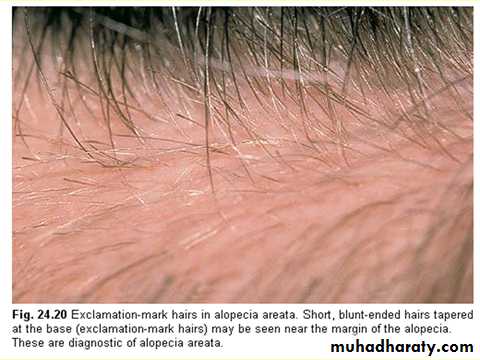
Pathognomonic ‘exclamation-mark ! ’ hairs may be seen around the edge of enlarging areas.
They are broken off about 4 mm from the scalp, and are narrowed and less pigmented proximally.


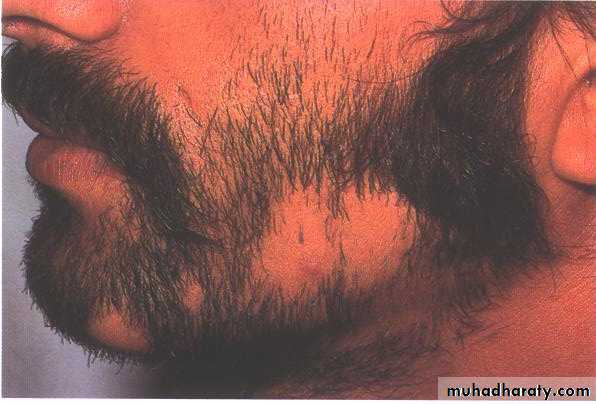
Patches are most common in the scalp and beard
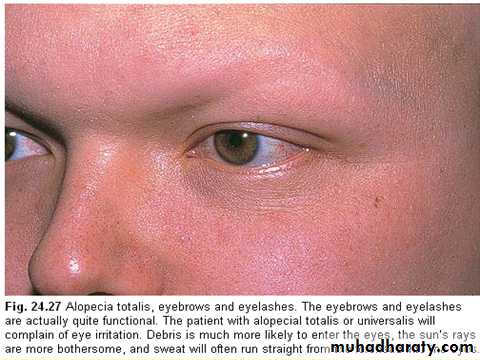
but other areas, especially the eyelashes and eyebrows, can also be affected.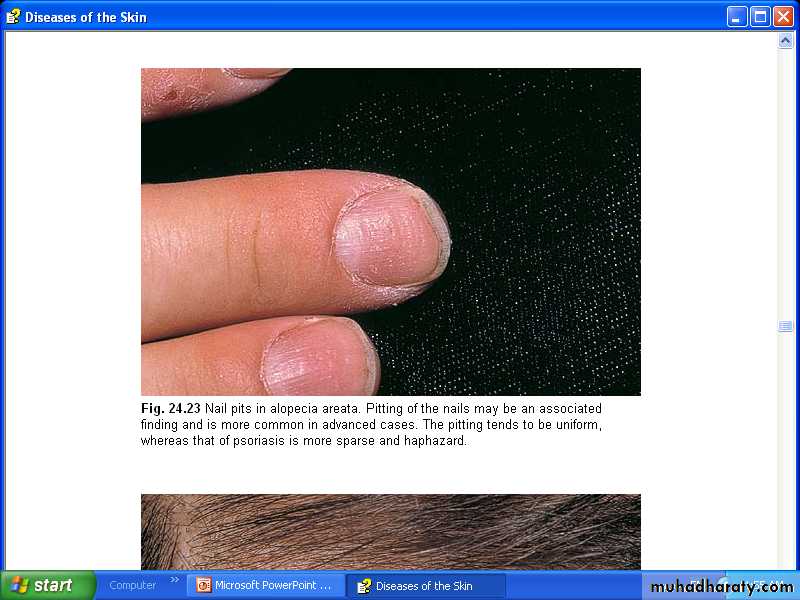
Up to 50% of patients show fine pitting or wrinkling of the nails.
Course:
The outcome is unpredictable.
In a first attack, regrowth is usual within a few months.
Subsequent episodes tend to be more extensive and regrowth is slower.
A few patients lose all the hair from their heads (alopecia totalis) or from the whole skin surface (alopecia universalis).
Prognosis:
the following suggest a poor prognosis.1 Onset before puberty.
2 Association with atopy or Down’s syndrome.3 Unusually widespread alopecia, (totalis, universalis).
4 Involvement of the scalp margin (ophiasiform type).5 Positive family history.
6 Association with nail changes.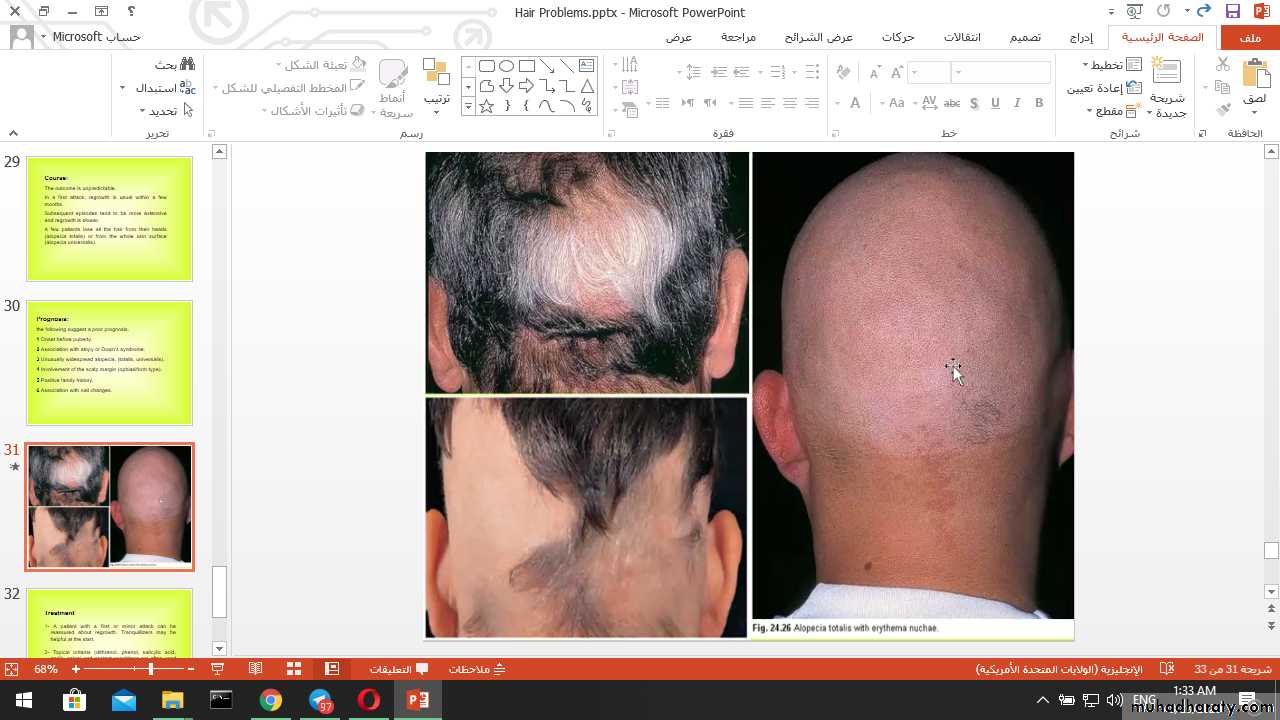
Treatment
1- A patient with a first or minor attack can be reassured about regrowth. Tranquillizers may be helpful at the start.2- Topical irritants (dithranol, phenol, salicylic acid, garlic, onion) and contact sensitizers are often used to induce dermatitis that disturb the already disturbed immunity hoping for hair regrowth.
3- Topical steroid lotions and creams.
Treatment4- Intradermal injection of steroid leads to localized tufts of regrowth while not affecting the overall outcome. This may be useful to re-establish eyebrows or to stimulate hope.
5- Ultraviolet radiation or even PUVA therapy may help extensive cases.
6- Topical immunosuppressive agents (e.g. tacrolimus).7- Systemic therapy: in sever conditions such as systemic steroid, psoralen, oral zinc sulphate and immunomodulation with BCG vaccination.