Lecture 4

Dr.Safaa Hussain Alturaihy
Lecture
4
Atopy
is a tendency to develop an exaggerated IgE antibody response
Allergy
is the clinical presentation of atopic disease in the presence of
allergen
Aetiology
G
enetic and family history
E
nvironmental factors like exposure to allergen ,air pollution and
irritant, occupational allergen like flour, wood dust, latex in surgical
gloves,tobacco,detergents and bleach.
F
ood occasionally provoke IgE allergic rhinitis, it may be due to sensitivity to
preservatives, some type of food contain histamine like cheese and wine
D
rugs like penicilline, asprin, antihypertensive, B-blocker, ACE inhibitor

The allergic responses can be divided into two
phases. The first is an acute response that occurs
immediately after exposure to an allergen. This
phase can either subside or progress into a "late
phase reaction" which can substantially prolong the
symptoms of a response, and result in tissue damage

Pathogenesis
IgE has a property of binding to high affinity receptor on the mast cell
and basophil .the interaction of allergen with IgE initiate secretion of
active mediators that cause clinical manifestation,thes mediators either
preformed
mediators (histamine, proteases, chemokines, heparine);
or
newly formed
mediators (prostaglandins, leukotrienes, thromboxanes)
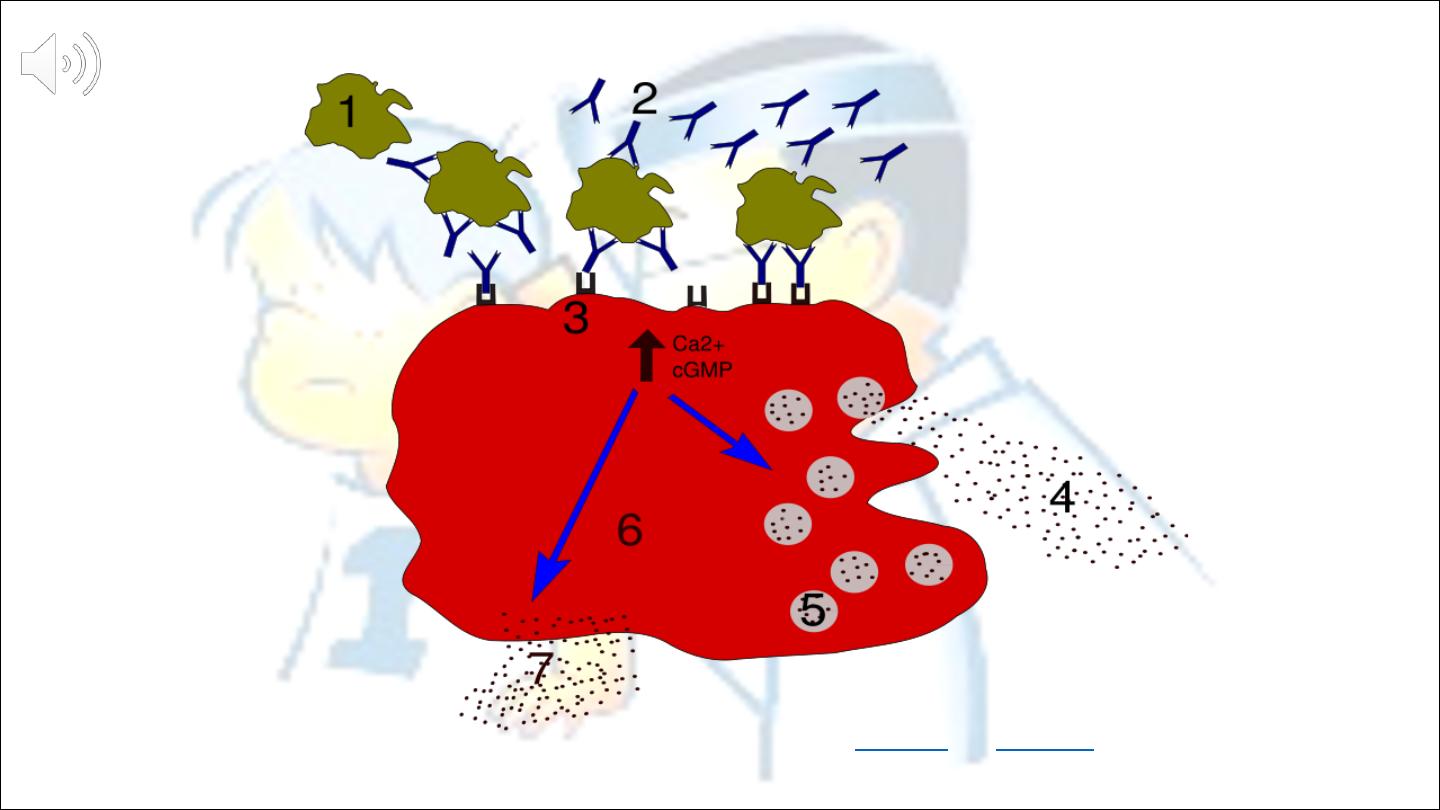
Degranulation process in allergy.1 - antigen; 2 - IgE antibody; 3 - FcεRI receptor; 4 -
preformed
mediators
(histamine, proteases, chemokines, heparine); 5 -
granules
; 6 -
mast cell
; 7 -
newly
formed mediators
(prostaglandins, leukotrienes, thromboxanes)


Allergic rhinitis
Rhinitis if defined clinically by a combination of two or more
nasal symptoms
Nasal obstruction…….blocking
Rhinorrhea…………...running
Itching and sneezing
Allergic rhinitis occur when these symptoms are the result of
IgE mediated inflammation following exposure to allergen
Classification
Seasonal
Perennial
occupational
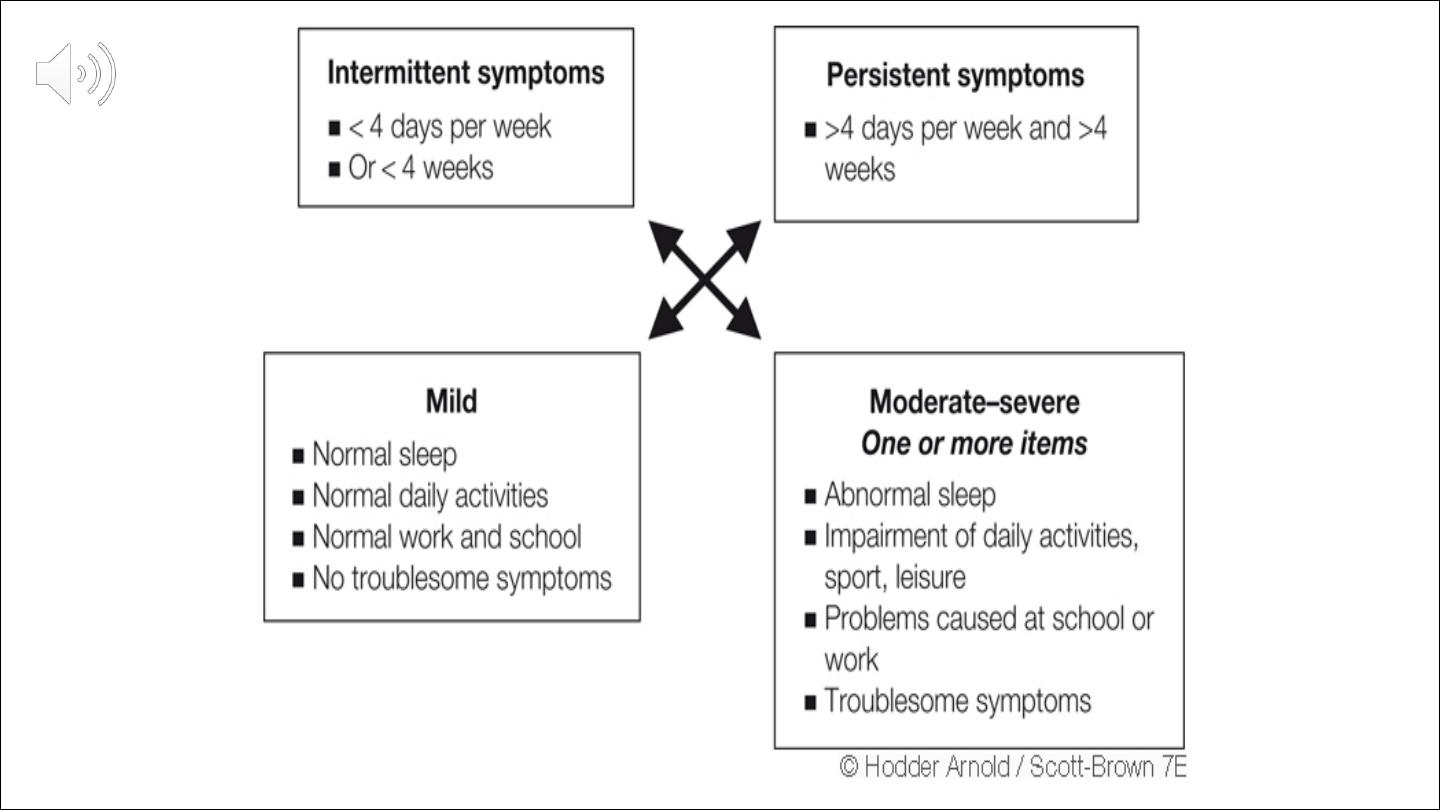

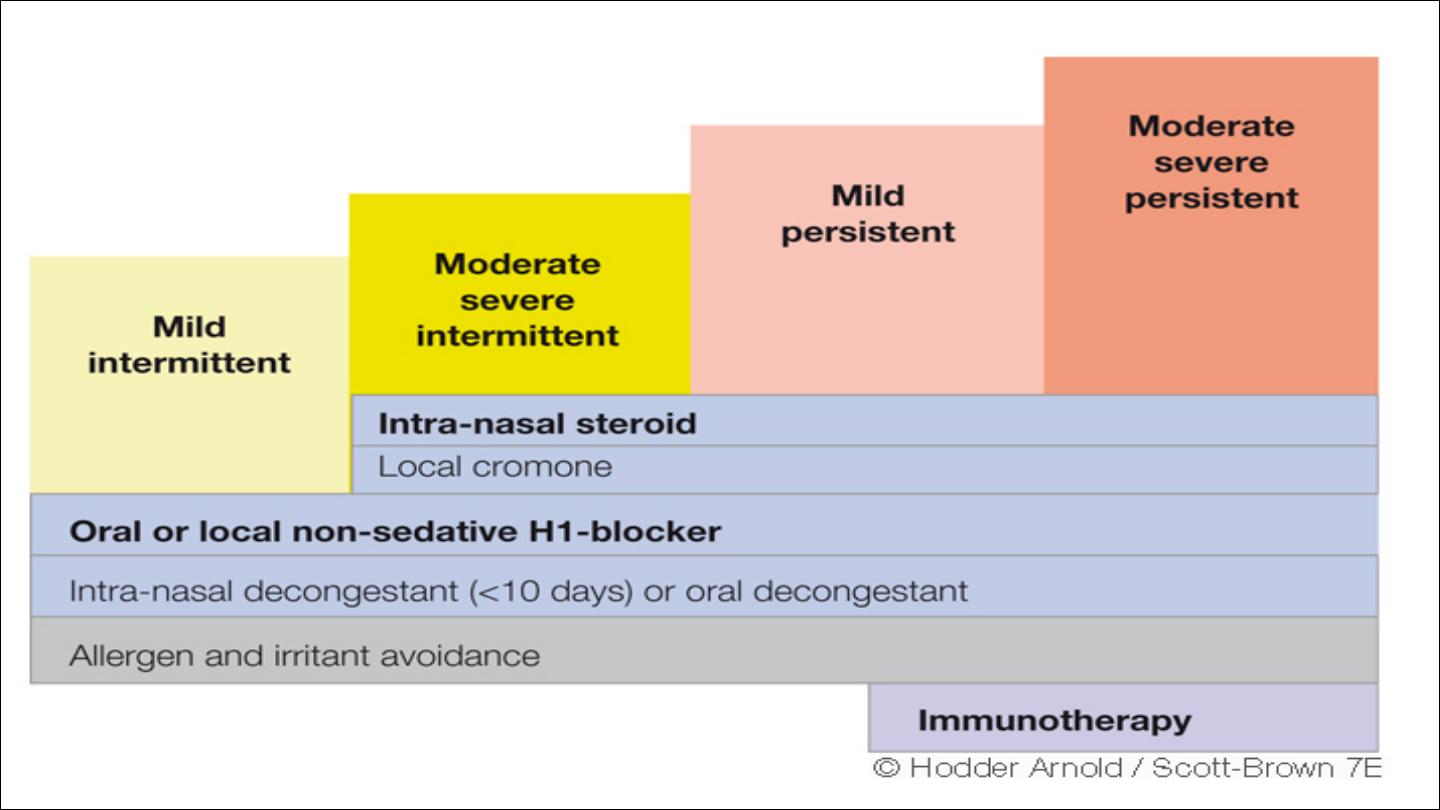
New classification by ARIA guideline (allergic rhinitis and its impact on
asthma)
Mild
Normal sleep
Normal daily activities
Normal work and school
No troublesome symptoms
Moderate or severe
Abnormal sleep
Impairment of daily activities
Problems caused at school and work
Troublesome symptoms

Intermittent symptoms
Less than 4 days/week
Or less than 4 weeks
Persistent symptoms
More than 4 days/week and more than 4 weeks
Co-morbidities
Other conditions associated with allergic rhinitis are
asthma,sinusitis,otitis media,sleep disorder,lower
respiratory tract infection
Rhinitis and asthma are linked by
epidemiological,pathophysiological characteristics and by
common therapeutic approach.
█
Rhinitis is a risk factor for the development of subsequent
asthma ,
█
is a frequent cause of asthma exacerbations ,and
█
effective rhinitis treatment reduce asthma
So patient with persistent allergic rhinitis should be
evaluated for asthma and the converse is true

Clinical presentation
Immediate
type allergic symptoms of sneezing ,rhihinorrhea
and itching are easily recognized
Perennial
allergic inflammation is mainly expressed as nasal
obstruction,hyperreactivity and poor sense of smell,the
sinus lining is also usually involved so that the picture is of
one of a chronic inflammatory rhinosinusutus,in those
patient immediate symptom not present and may undergo
unnecessary operations for septal deviation or turbinate
befor the true nature of the problem is diagnosed
properly
!!!!

Examination
The mucosa appear pale, or
bluish,boggy,swollen,NSD,polyp,inferior turbinate
hypertrophy

Lab tests
1
skin prick test
2
serum IgE measurement either
RAST
radioallergosorbant test
ELISA
enzyme linked immunosorbant test
3
nasal cytology for eosinophil
4
nasal swab for bacterial and viral studies
5
nasal allergen challenge
Treatment
◙
identification and avoidance
◙
pharmacotherapy
Antihistamine
It relieve running,itching,and sneezing but have little or no effect on
blockage
First generation like chlorpheneramine,diphenhydramines should be
avoided because of sedation,psychomotor retardation and learning
impairment because it cross the BBB and interact with histamine
receptors
Second generation antihistamine act with an hour topical ones
within 15 minutes
Terfenadine,astemazole
block potassium channel and cause cardiac
arrhythmia, QT prolongation,so care taken not overdose and nor to
combine with erythromycin,ketokanazole,grapefruit
juice,antiarrythmia .
Citrizine,fexofenadine,and desloratidine
not block potassium channels
even at supranormal dose
Desloratidine is exception that affect on nasal blockage

Topical corticosteroid
Are the most effective treatment of rhinitis especially if started prior to
allergen exposure it reduce the relative risk of asthma exacerbation by
50%
Side effects
are minor include epistaxis and nasal irritation
Beclomethasone-------- Beconase
Budenoside--------------Rhinocort
Fluticasone -------------Floxanase
Sodium cromoglicate
It is weakly effective against all rhinitis but safe means it is useful for
small children less than four years for whom a topical corticosteroid is
not available

Fluticasone
Beclomethasone
Budenoside
Fluticasone
Triamcinolon Acetonide
Mometasone Furoate
?
Decongestants
Used topically reduce nasal obstruction but increase rhinorrhea,regular
use for more than few days result in rhinitis medicamentosa
Systemic decongestant are relatively ineffective with side effects like
hyperactivity,insomnia in children and hypertension in adult
Ipratropium bromide
Response in patients who do not response to topical corticosteroid
alone
Systemic corticosteroid
Used to unlock the nose at start of treatment or for sever
symptoms,used for few days Depot injection not recommended
because they are not stopped if side effects occur
Antileukotriens LRA
Recently been licensed in rhinitis it can also be helpful in polyposis
Nasal douching

◙
Immunotherapy
It is alter the course of allergic disease and prevent the
progression of allergic rhinitis to asthma .session long
As more as 2-3 years and should be given by trained
personnel and only under medical observation
◙
Surgery
May play role especially when the main symptom is
nasal obstruction.
Correction of NSD ,reduction of IT,surgery to improve
nasal patency.