Lecture 5

Dr.Safaa Hussain Alturaihy
Lecture
5

Epistaxis is the commonest otolaryngologic emergency, affecting up to
60% of the population in their lifetimes, with 6% of cases requiring
medical attention.
The nasal cavity is extremely vascular.
Terminal branches of the external and internal carotid arteries supply the
mucosa of the nasal cavity
with frequent anastomoses between these systems
The anterior nasal septum is the site of a plexus of vessels called Little’s
or
Kiesselbach’s area, which is supplied by both systems
The maxillary sinus ostium serves as the dividing line between
“anterior” and “posterior” epistaxis.
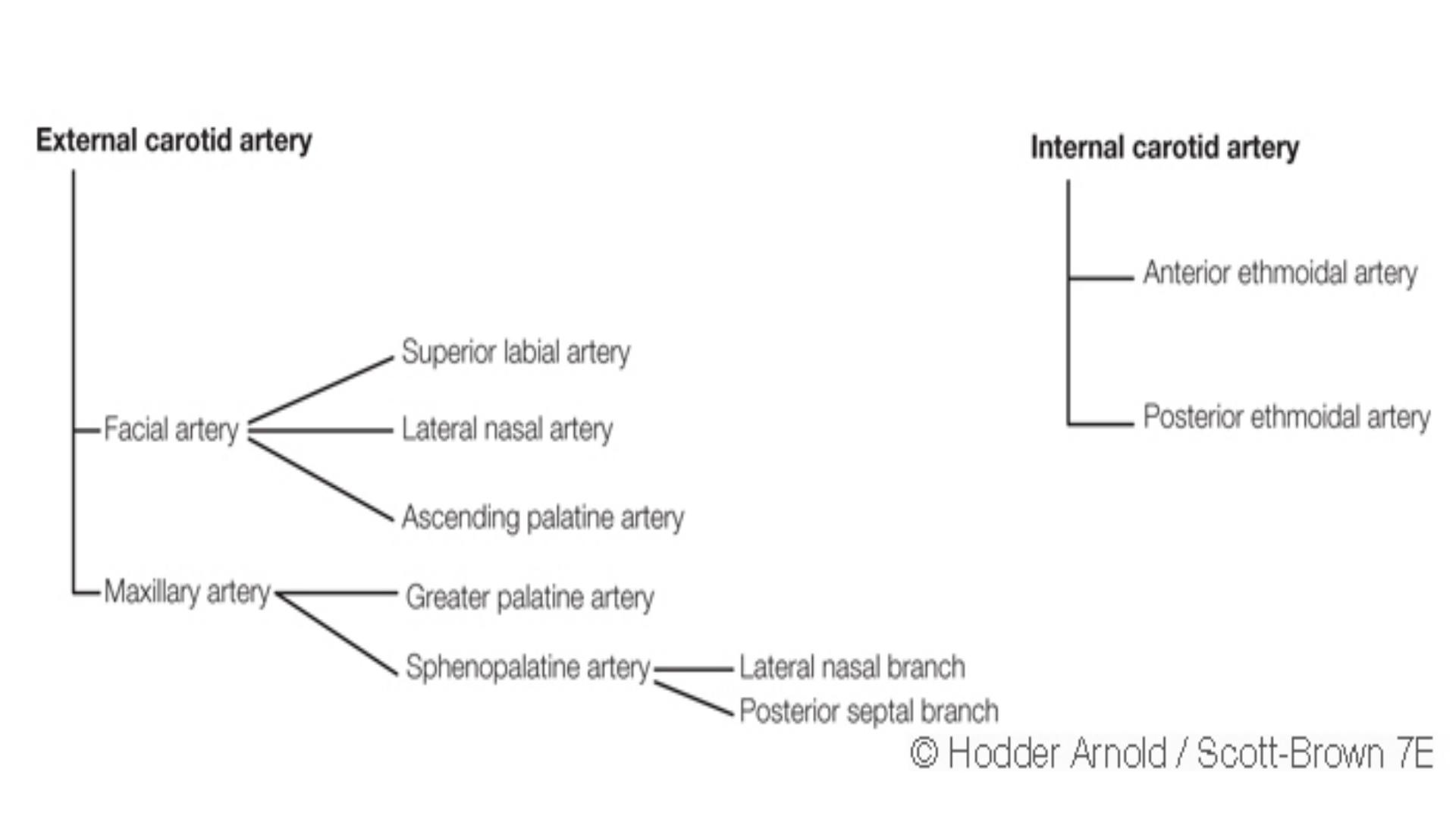
Arterial supply
external carotid artery-
facial artery-
superior
labial artery nasal branch
maxillary artery-
sphenopalatine
greater
palatine artery
internal carotid artery-
anterior ethmoid artery
posterior ethmoid artery

Little`s area or Kiesselbach`s plexus
It is an area in the anterior part of the septum just behind the
skin margin contain aggregation of poorly supported blood
vessels represents the most important and commonest site of
epistaxis
It formed by anastamasis of
*
Septal br.of sphenopalatine artery
*
Superior labial artery
Greater palatine artery
*
*
Ant.ethmoid artery

Aetiology
A
idiopathic---------from little`s area
B
Trauma
Nose picking
F.B
Maxillofacial trauma
Itrogenic

C
infection acute or chronic.viral or bacterial
D
Inflammatory
Rhinosinusitis
Nasal polyp
E
Neoplasm
Benign angiofibroma, papilloma
Malignant
sq.cellcarcinoma,adenocarcinoma, lymphoma
F
Drug induced
Cocaine abuse
Rhinitis medicamentosa
medicamentosa,asprin,anticoagulant.chloramphinicol,im
munosuppressant,alcohol
G
inhalant
Tobacco
H
endocrine

2
General
A
atherosclerosis
B
bleeding disorder
A
coagulopathy
1
inhereted coagulation factors deffeciancy like
factor vii,factor ix
2
acquired :anticoagulant,liver disease,vitamin
k defficiancy
B
platelate disorders
●
thrombocytopenia
●●
platelate disfunction
►
congenital like vonwillbrand disease
►►
acquired like leukemia,uremia,drugs as
asprin & NSAID
C
blood vessel disorders
●
congenetal----osteogenesis imperfecta
●●
acquired-----amyloid,vasculitis,vit.K
defeciancy
D
hyperfibrinolysis
●
congenital------αantitrypsin deficiency
●●
acquired------
malignant DIC

Anterior bleeding
is usually easier
to access and is therefore less dangerous.
Posterior epistaxis is more
difficult to treat because visualization is more difficult and blood is
often swallowed, making it more difficult to gauge the amount of
blood loss
The term “
posterior bleeding
” is all too often used incorrectly to
label bleeding that cannot be visualized with a head lamp. It
transpires
in many cases that endoscopic examination shows the bleeding to be
located high on the septum

Classification
Primary No proven causal factor
Secondary Proven causal factor
Childhood <16 years
Adult >16 years
Anterior :Bleeding point anterior to piriform aperture
Posterior :Bleeding point posterior to piriform aperture
The maxillary sinus ostium serves as the dividing line
between
“anterior” and “posterior” epistaxis

Classification
Anterior epistaxis
Incidence
---- Amore common
Site
---------mostly from little`s area or anterior area of the nose
Age
---------mostly occur in children or young adult
Cause
------mostly trauma
Bleeding
---usually mild,can be easily controlled by local pressure or anterior
pack

posterior epistaxis
Incidence
---- less common
Site
---------mostly from posterosuperior part of the nasal
cavity,often difficult to localize the bleeding point
Age
---------mostly occur after 40 yerars of age
Cause
------spontanous,often due to hypertention or atherosclerosis
Bleeding
---bleeding is sever,requires
hospitalization,post nasal packing often required
If bleeding continue!
How do manage a patient with
epistaxis?
!

Management
Initial Assessment
The amount of blood loss should be estimated (the physician should
ask about whether the patient has lost enough to soak a handkerchief,
a facecloth, or a towel; the last would indicate a significant loss), and
over what period (a regular minor bleed can cause anemia).
A clinical assessment of the patient’s cardiac status and circulating blood volume
should include looking to see if the patient is pale, sweating, or cool,
or has tachycardia; any of these findings would indicate significant
hypovolemia. A reduction in blood pressure is often a late sign, particularly
in young people, who can maintain blood pressure until the
circulatory volume is critical.
Obtaining intravenous access, checking for and correcting any
clotting abnormalities, and taking blood for “group and save” and/or
crossmatching may be required. In our unit patients admitted via the
emergency department can be “fast-tracked” to the otorhinolaryngo-

- logic emergency unit if stable This practice helps avoid
unnecessary and counterproductive nasal packing in the emergency
department as well as transfer of patients before they are fit enough to
travel.
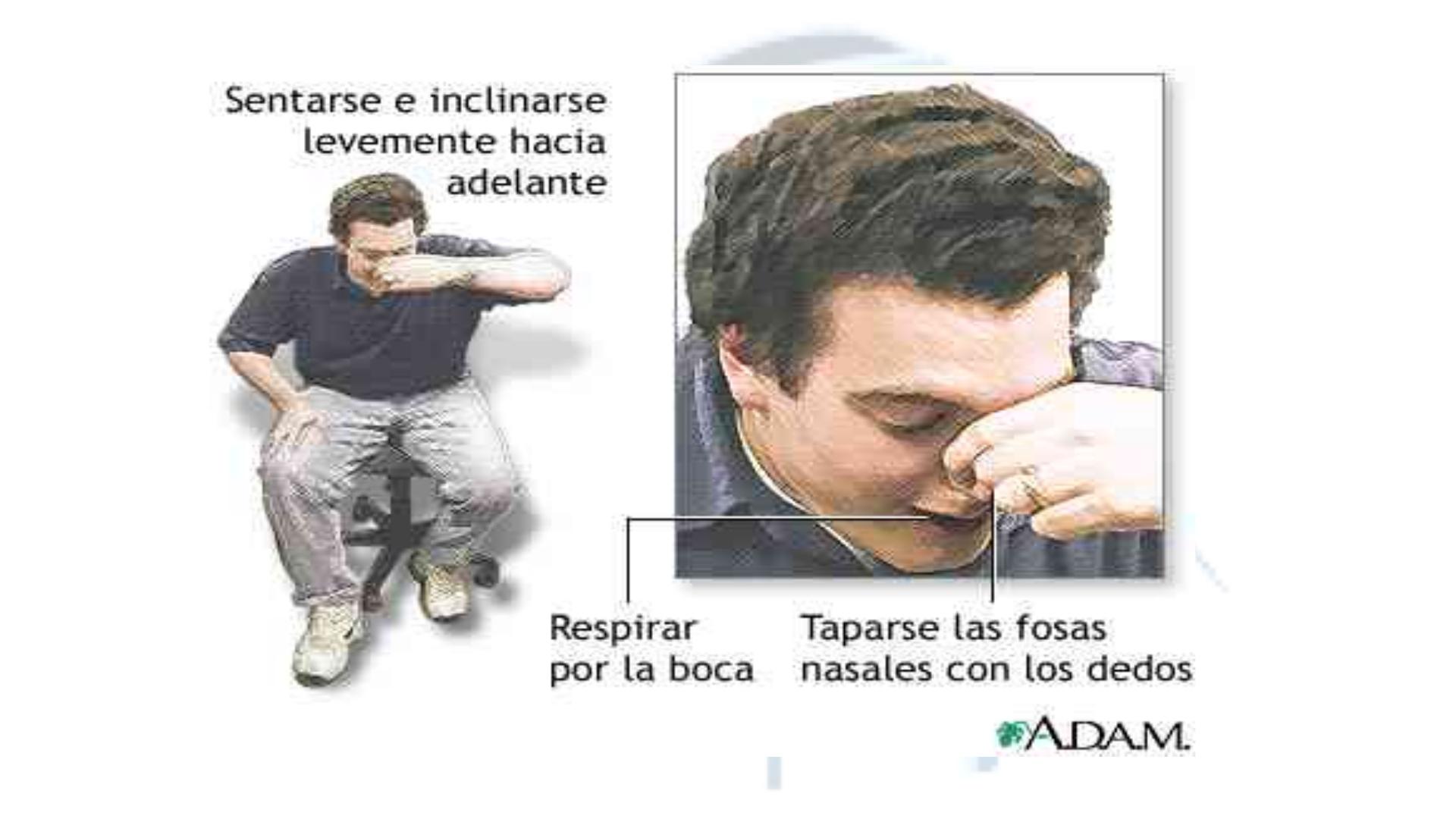
First aid measures
include asking the patient to apply constant firm
pressure over the lower (non-bony) part of the nose for 20 minutes and
to lean forward with the mouth open over a bowl so that further blood
loss can be estimated. Otherwise, blood dripping postnasally will be
swallowed, and the next warning sign of a serious loss could be several
hundred milliliters of blood being vomited up.
It is important to establish both the site and the cause
The
philosophy of this approach can
be
summarized as follows:
1. Establish the site of bleeding.
2. Stop the bleeding.
3. Treat the cause
.

The clinician must remember that epistaxis is frequently idiopathic
but can be a manifestation of a possible underlying pathology.
Your patient should undergo further investigationaccording to the
history.

The key to controlling most epistaxis is to find the site of the bleeding,
and although
chemical cautery
with silver nitrate can be used,
Biopolar diathermy
is more effective for stopping the bleeding. Protection from
blood contamination is important. A plastic apron for both parties is
helpful in order to avoid staining of clothes, and eye protection is advisable
if there is active bleeding because some patients have a reflex to
blow away any fluid dripping down the upper lip, which can create a
bloody aerosol. Once the clots have been sucked out, the nasal airway
should be inspected, initially with a headlamp and then, if the bleeding
point cannot be located, with an endoscope.

Epistaxis in Children
Young children usually bleed from a vessel just inside the nose at the
mucocutaneous junction on the septum, and the bleeding invariably
stops spontaneously. In children with epistaxis in whom no prominenvessel can
be seen, the regular local application of a cream can help,
but petroleum jelly
(Vaseline) alone does not.
As many as
5% to 10% of children
with recurrent nosebleeds
may have undiagnosed von Willebrand’s disease.
Children who have leukemia or are undergoing chemotherapy often have
epistaxis associated with thrombocytopenia. Older children, adolescents,
and adults often bleed from Little’s area or a maxillary spurt

Epistaxis in Adults
The caudal end of the septum, where several branches of the external
and internal carotid anastomose in Little’s area or Kiesselbach’s plexus,
is the most common site of bleeding in adults.
Less commonly bleeding,
comes from further back on the septum, and a septal deviation
may make it difficult to visualize .Some patients with
seasonal allergic rhinitis complain of more nosebleeds in the hay fever
season, and topical nasal steroids aggravate the bleeding in approximately
4% of users
. Many people believe that a nosebleed signifies a
release of pressure and may herald a stroke,
and it is important for the
clinician to address these anxieties for the patient. Although many
patients are found to be hypertensive during nosebleeds, few remain soon
follow-up.
The association between hypertension
and epistaxis is
disputed.
Many clinicians report that hypertension is not related to
nosebleed.
However, nosebleeds in patients with hypertension
are more likely to lead to admission and to be associated with
comorbidity.

In over-anticoagulated
patients, fresh frozen plasma, clotting factor extracts, and vitamin K
help. Vitamin K takes more than 6 hours to work, however, and it can
delay anticoagulation for 7 days after warfarin is started.
.
Tranexamic acid
(Cyclocapron)
, an antifibrinolytic agent, has not been shown to help. But other litriture advice to give it Scott brown)
Tranexamic
acid has been shown to reduce the severity and risk of rebleeding in epistaxis at a dose of 1.5 g
three times a day. These drugs do not increase fibrin deposition and so do not increase the risk of
thrombosis. Preexisting thromboembolic disease is a contraindication Other drugs associated with bleeding
are aspirin, which interferes with
platelet function for up to 7 days, clopidogrel, and nonsteroidal antiinflammatory
drugs.
In patients who do not have a history of a
bleeding disorder or undergoing anticoagulant therapy, routine clotting
studies do not add to the management. There is a higher incidence
of epistaxis in patients with a high alcohol intake, even when there is
no laboratory evidence of a coagulation abnormality.

Topical Treatment
A randomized controlled trial of silver nitrate cautery with topical
antiseptic nasal carrier cream versus topical alone showed both to be effective
Use of cold pack is advisable although hot water irrigation 50c has been
proposed as an alternative to packing

Nasal Packing
If a bleeding point cannot be found, ideally the nose is packed with an
absorbable hemostatic agent that produces minimal mucosal trauma.
Various nonabsorbable packs have been used, but their insertion is
uncomfortable, as is their presence once in position. The insertion of
a pack can cause local mucosal trauma and complicate localization of
the bleeding point The insertion of a nasal pack has
conventionally meant that the patient has to be admitted, although one
study discharged 46 of 62 patients whose nasal airways had been
packed, with outpatient follow-up arranged for 48 hours later If anterior packing fails,
a
posterior balloon
may have to
be placed and inflated in the postnasal space

Cautery
Most anterior epistaxis can be controlled with identification of the
bleeding point and cautery using a headlamp. The vast majority of
posterior bleeding sites can be identified by endoscopy without the use
of general anesthesia
After cautery the patient should be advised against blowing the
nose for about 10 days to allow the area to heal. A greasy antiseptic barrier
cream should be applied several times daily for 2 weeks to
prevent the eschar from drying and coming off with a resulting rebleed.
The ointment should not be placed directly on the area treated but is
best placed inside the rim of the nostril with the tip of the finger, and
“milked up” by massaging the nostril rims, and then sniffed up. This
advice can also be given to patients with a crusted septal area from
picking or excessive drying

. An anterior pack is then
placed, and gentle traction used to pull the balloon forward against the
anterior pack this arrangement is held by placement of a clip over the
catheter anteriorly as it emerges through the anterior pack The morbidity and
physical discomfort
associated with nasal packing includes pain, hypoxia, alar necrosis, and
toxemia, and is well described in the literature; Packing not only traumatizes the
nasal lining but also can
cause cardiorespiratory complications and local infection.
46
The role of prophylactic systemic antibiotics in patients who have
nasal packs is not well established. If the patient does not experience rebleeding
within 12 to 24
hours, the packs should be removed
If bleeding continue!
If bleeding continue
!

Septal surgery
When epistaxis originates behind a prominent septal deviation or
vomeropalatine spur, septoplasty
or submucosal resection (SMR) may be required to access the bleeding point.
Some authors have
advocated septal surgery as a primary treatment for failed packing. The
rationale is that by
elevating the mucoperichondrial flap for septoplasty or SMR, the blood supply
to the septum is
interrupted and haemostasis secured. Cumberworth et al.
58
showed a strategy
involving SMR and
repacking to be more effective and economic than ligation in patients who had
failed with packing.
If bleeding continue!
If bleeding continue
!

Endoscopic sphenopalatine
artery ligation (ESPAL
);
has replaced the need for
posterior nasal packs
,
If bleeding continue!
If bleeding continue
!

Ligation of ant ethmoid artery
Ligation of posterior ethmoid artery
Ligation of external carotid artery
Angiography and embolization Embolization
under angiographic guidance has been shown to control
severe epistaxis