
Benign tumours of the
Ovary
Dr.Nadia Mudher Al-Hilli
FICOG
Department of Obs&Gyn
College of Medicine
University of babylon

Objectives of lecture
• Understand the pathophysiology of different
types of ovarian mass
• Know the possible presentation & differential
diagnosis
• How to deal with such condition
• How to manage in pregnant women with
ovarian cyst

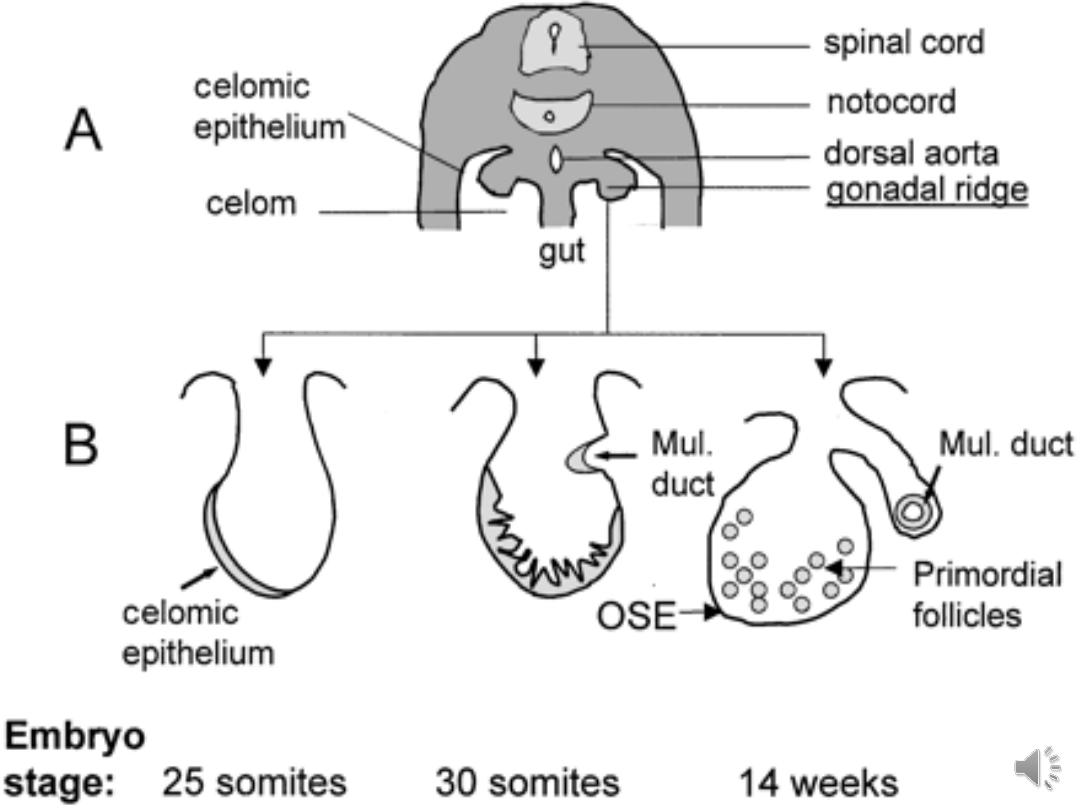
Development of the ovary:
It is of triple origin:
• Coelomic epithelium of the genital
ridge.
• the underlying mesoderm
• Primitive germ cells
Causes of benign ovarian cysts

• Functional cyst:
The risk of developing these
cysts is reduced by the use of the combined
oral contraceptive pill.
• Follicular cyst:
may persist for several
menstrual cycles & rarely achieve a diameter of up
to 10 cm. may produce estrogen causing menstrual
disturbance & endometrial hyperplasia
• Luteal cyst:
Corpora lutea are not called luteal
cyst unless they are more than 3 cm, usually
presented with pain due to rupture or
haemorrhage.

• Ovarian tumours are a group of neoplasms
affecting the ovary and have a diverse spectrum
of features according to the particular tumour
entity.
• They include benign, low-malignant
potential/borderline and malignant subtypes.

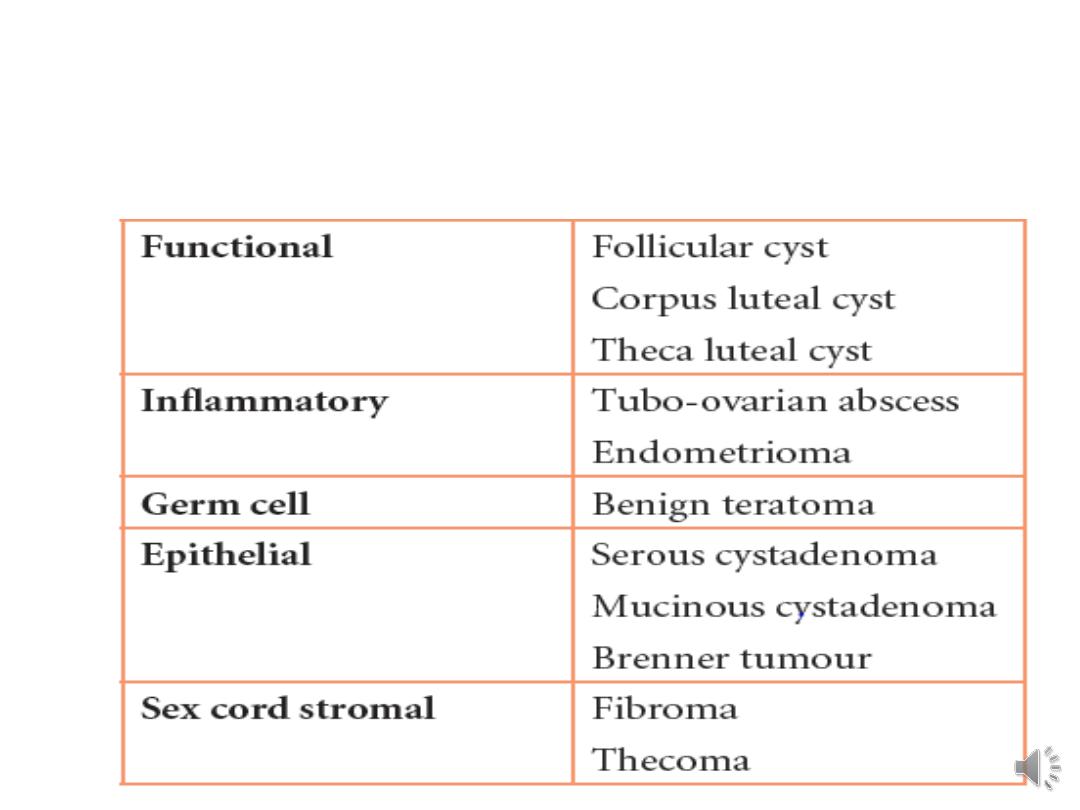
• Histological Classification of benign ovarian
tumours :
I- Benign germ cell tumours:
– Dermoid cyst (mature cystic teratoma)
– Mature solid teratoma
II- Benign epithelial tumours
:
– Serous cystadenoma
– Mucinous cystadenoma
– Endometrioid cystadenoma
– Brenner tumours

III- Benign sex cord stromal tumours:
– Theca cell tumours
– Fibroma

Benign germ cell tumours:
• The commonest ovarian tumours seen in
women less than 30 years old.
• arise from totipotential germ cells & may
contain elements of all three germ layers
(embryonic differentiation).
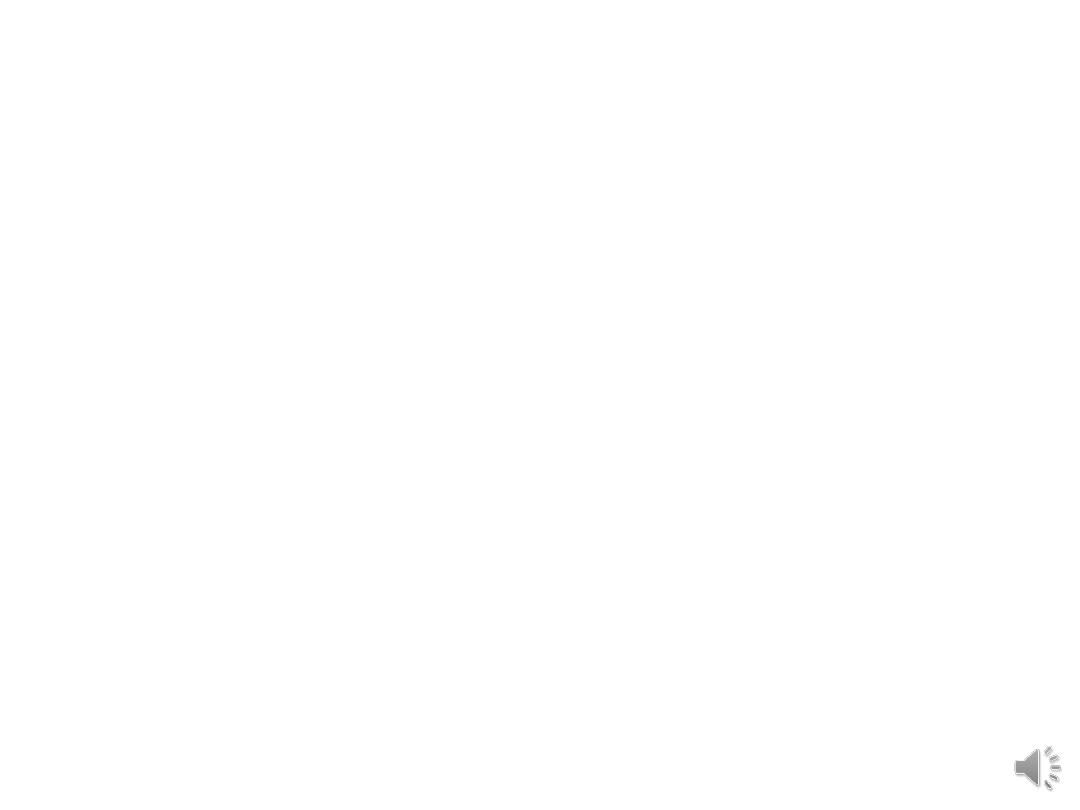
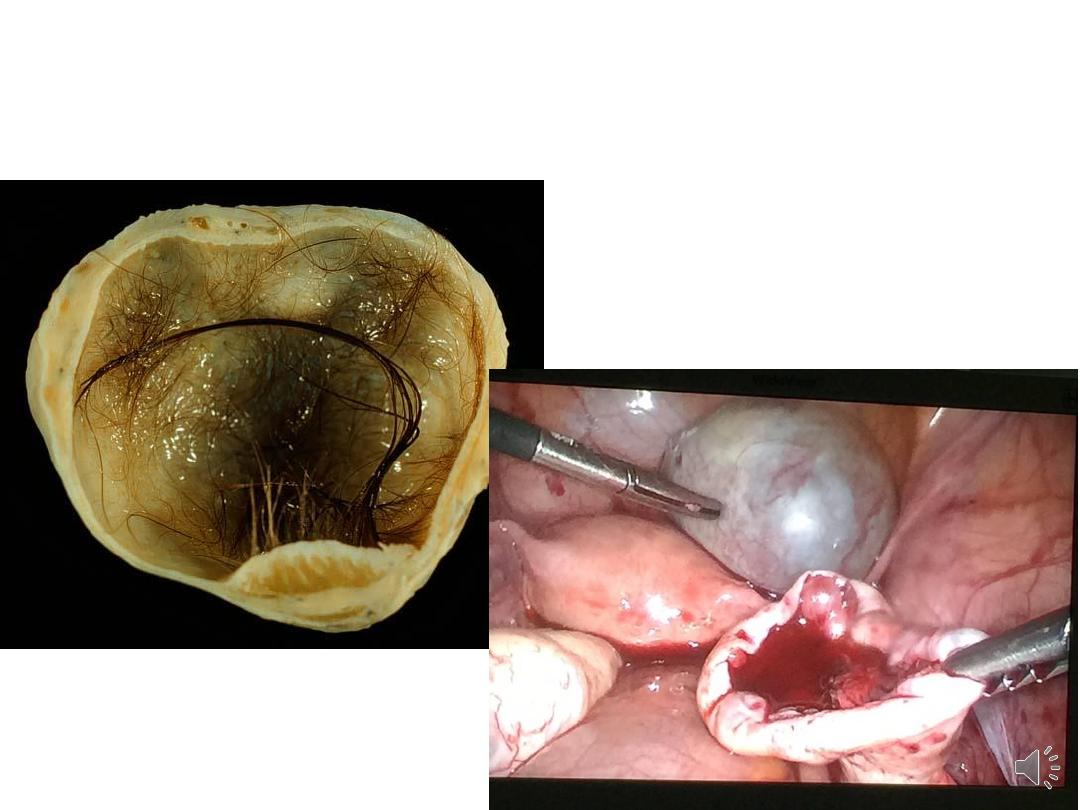
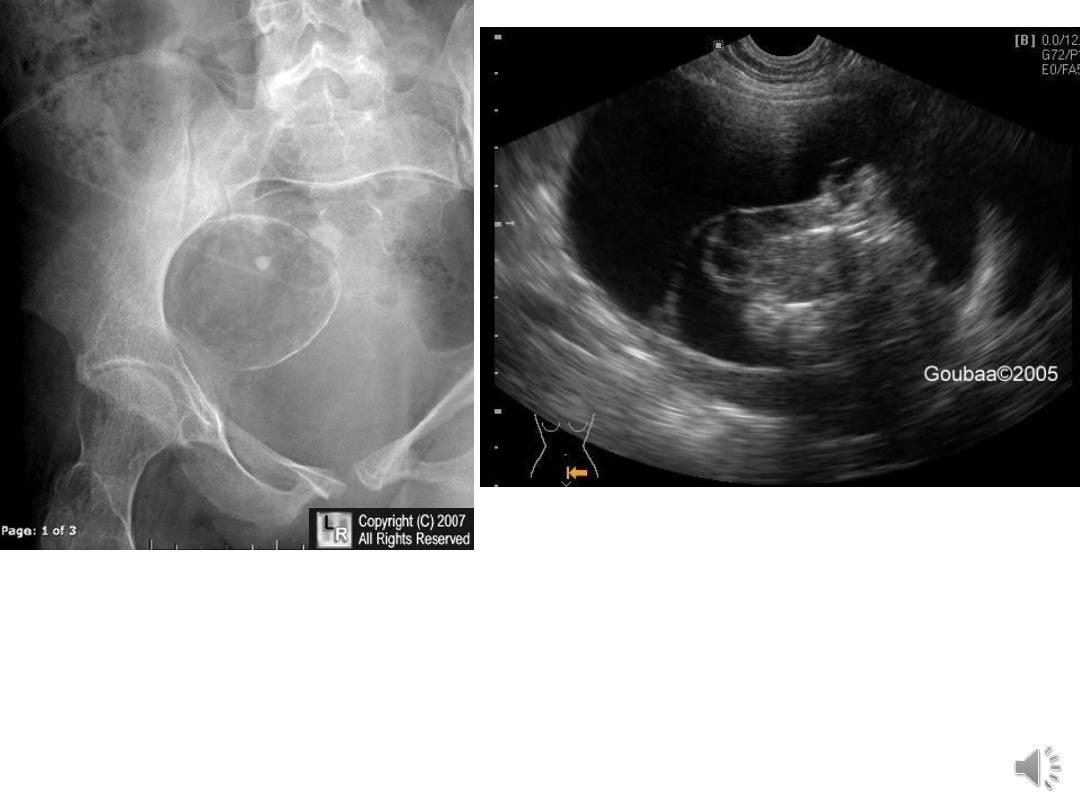
Dermoid cyst (mature cystic teratoma):
• usually unilocular
• < 15 cm in diameter
• ectodermal structures are predominant. lined
with epithelium like the epidermis & contains
skin appendages, teeth, sebaceous material, hair
& nervous tissue.
• Endodermal derivatives include thyroid,
bronchus & intestine,
• the mesoderm may be represented by bone,
cartilage & smooth muscle

Mature cystic teratoma

• monodermal teratoma: The classic example is
struma ovarii which contains hormonally active
thyroid tissue.
• majority are asymptomatic. may undergo torsion
or rupture spontaneously, either suddenly,
causing an acute abdomen & chemical
peritonitis; or slowly causing chronic
granulomatous peritonitis.
• < 2% contain malignant component

Benign Epithelial tumours:
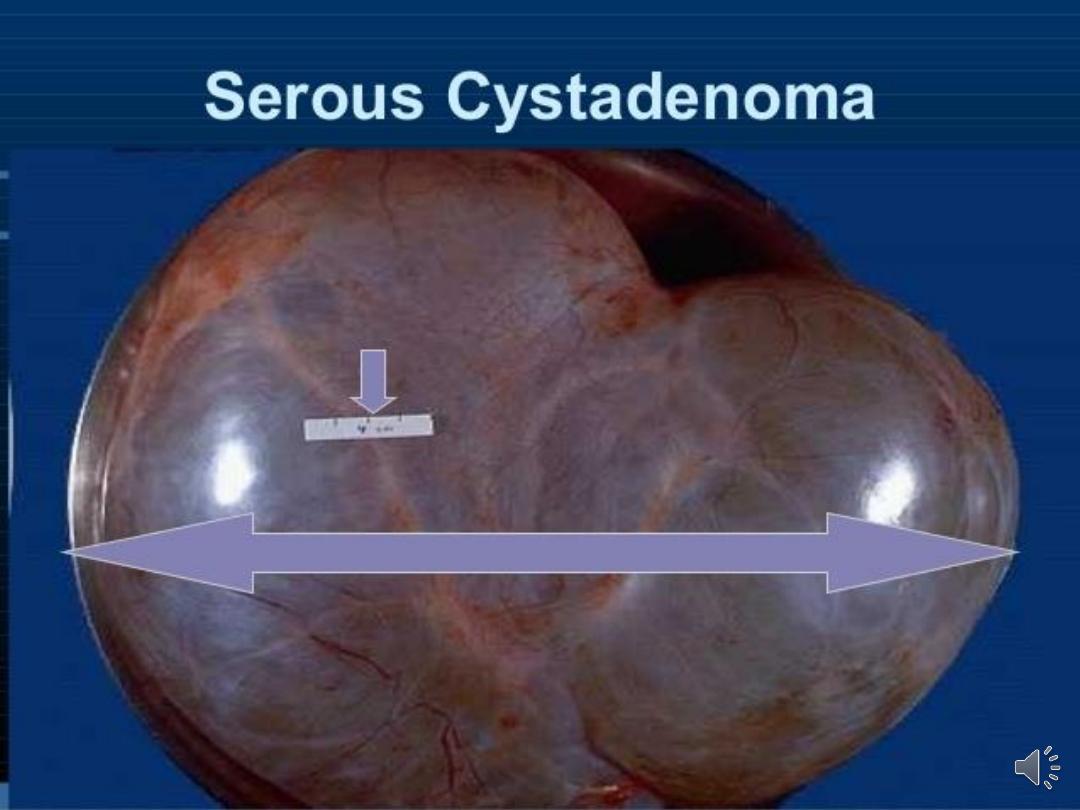
Serous cystadenoma
• The most common benign epithelial tumour
• usually unilocular cyst with papilliferous
processes on the inner surface.
• The cyst fluid is thin & serous. They are
seldom as large as mucinous tumours.




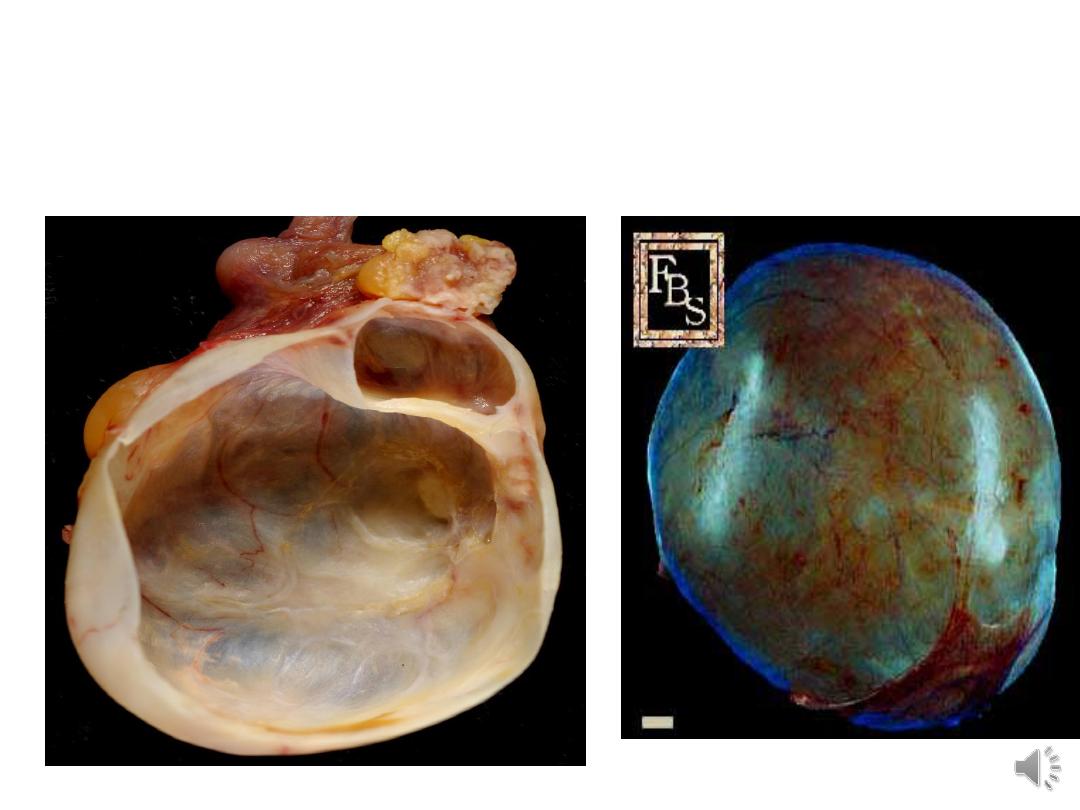
Mucinous cystadenoma
• Large
• Unilateral
• multilocular cysts
• smooth inner surface.
• lining epithelium consists of columnar
mucus-secreting cells.
• The cyst fluid is thick & gelatinous.
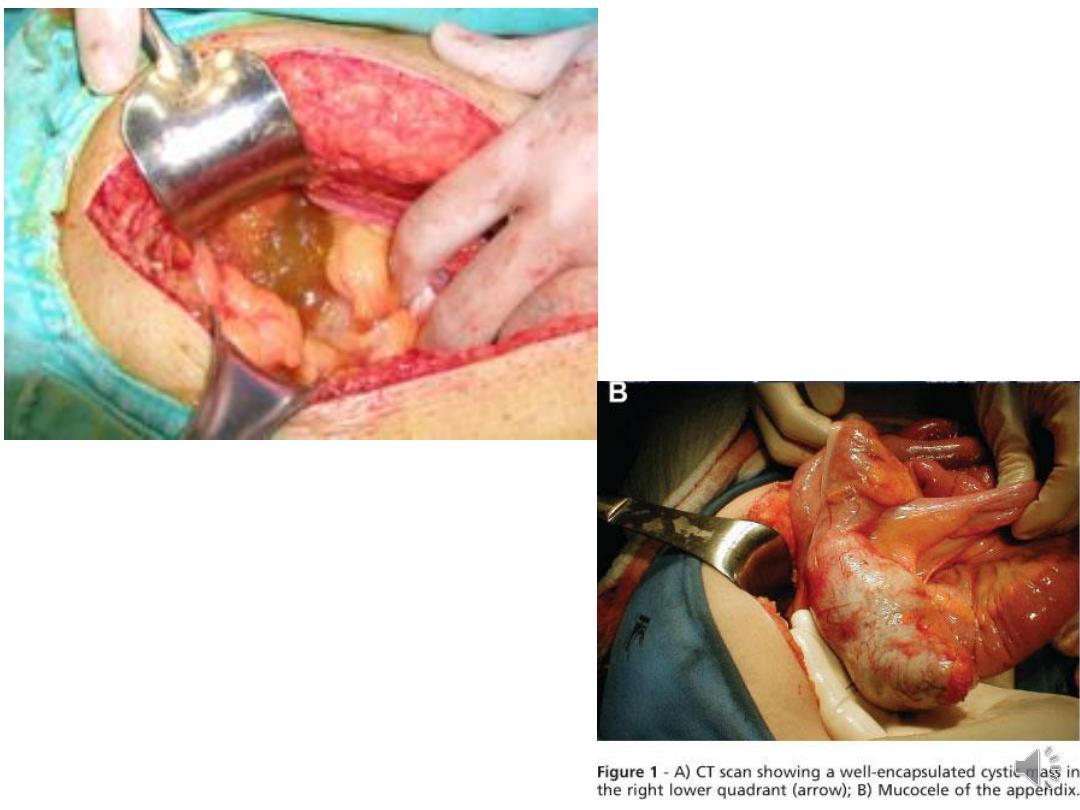
• Complication: pseudomyxoma peritonei

Benign sex cord stromal tumours:
• Constitute a small percentage of benign
ovarian tumours.
• They occur at any age
• Theca cell tumour secrete hormones &
present with symptoms of inappropriate
hormone effects
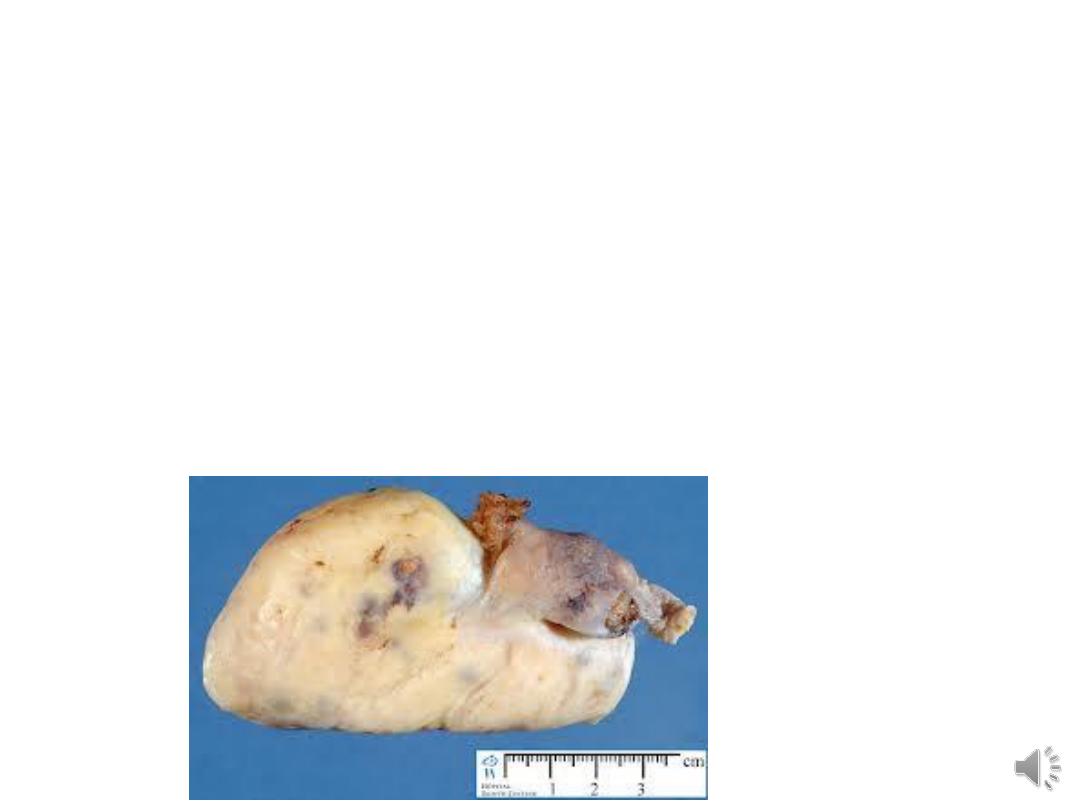
Fibroma:
• Solid, composed of stromal cells, present in
older women.
• Meig's syndrome: ascites & pleural effusion in
association with fibroma of the ovary, seen in
only 1% of cases.

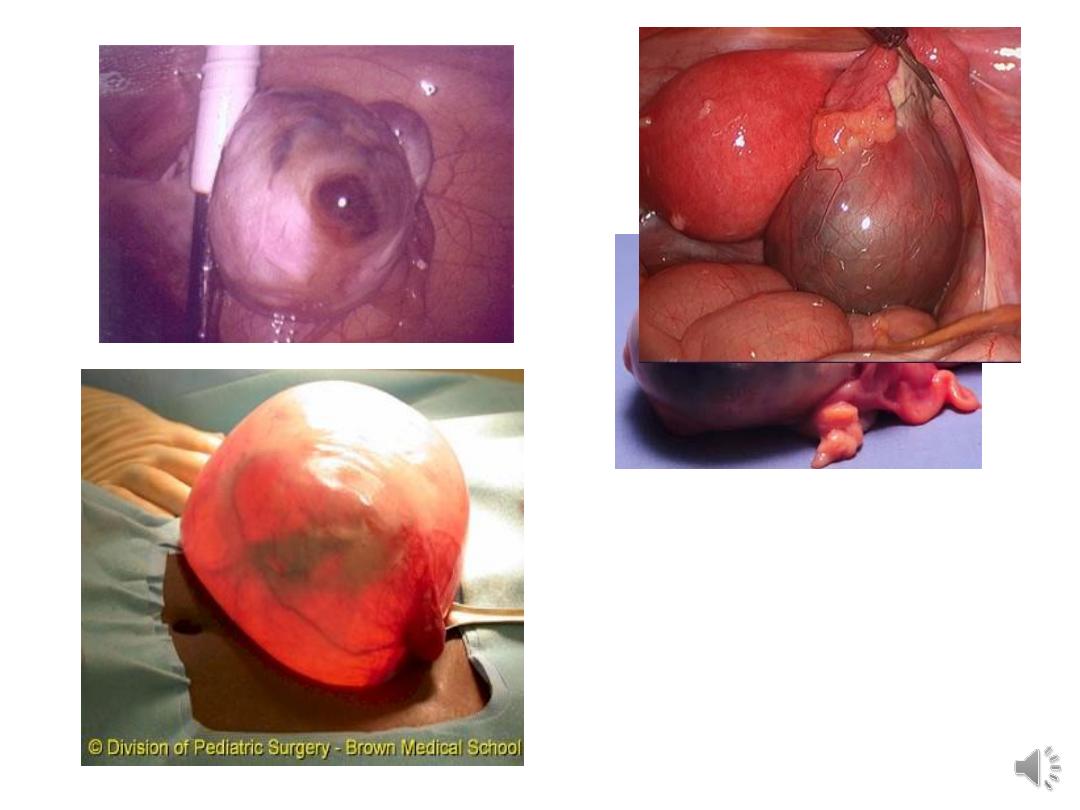
Presentation of Benign Ovarian Tumours:
• Asymptomatic
• Pain ( cyst accident)
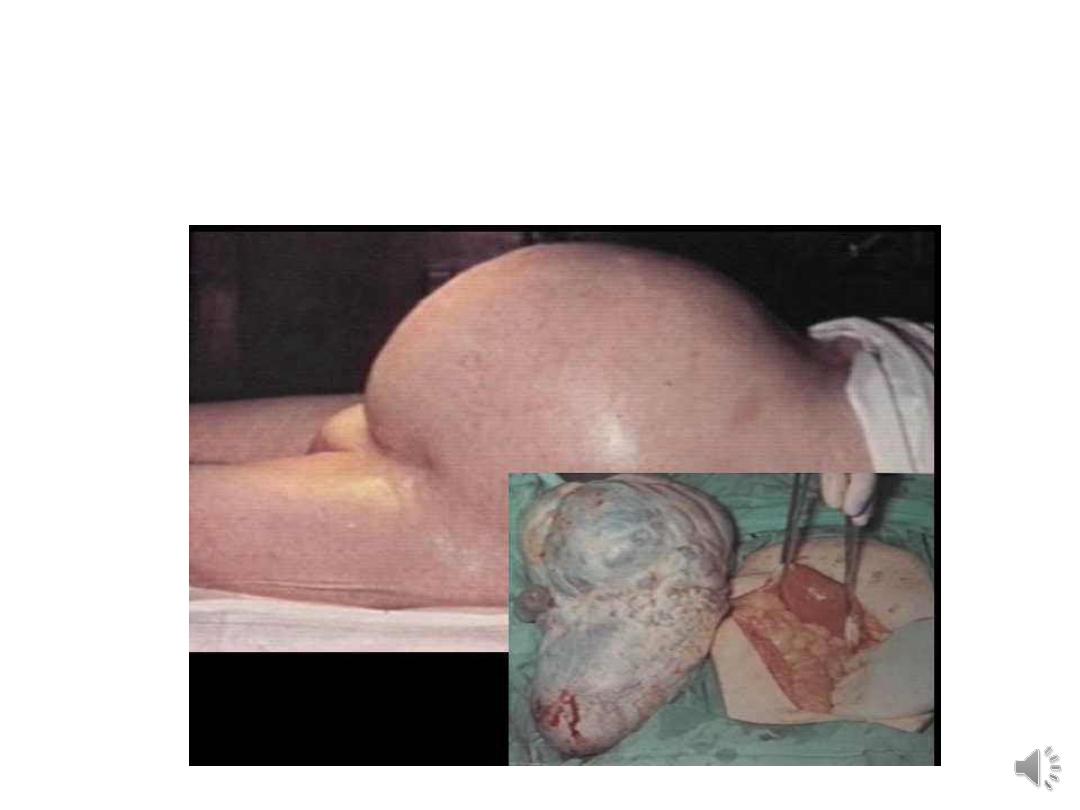
• Abdominal swelling: noticed only when the
tumour is very large.
• Pressure effects
• Menstrual disturbance
• Hormonal effects
• Abnormal cervical smear

Differential diagnosis of benign ovarian tumours:
Pain
• Ectopic pregnancy
• Spontaneous abortion
• Pelvic inflammatory diseae
• Appendicitis
• Meckel's diverticulum
• Diverticulitis

Abdominal swelling
• Pregnant uterus
• Fibroid
• Full bladder
• Ovarian malignancy
• Colorectal carcinoma
Pressure effects
• Urinary tract infection
All other causes of menstrual irregularities,
precocious puberty & postmenopausal
bleeding.

Diagnosis:
• History:
• Examination:
• peritonism is an ominous sign.
• Bimanual examination is essential for
palpating the mass between the vaginal &
abdominal hands, its mobility, texture &
consistency, presence of palpable lymph
nodes . Hard, irregular, fixed mass is
likely to be invasive.
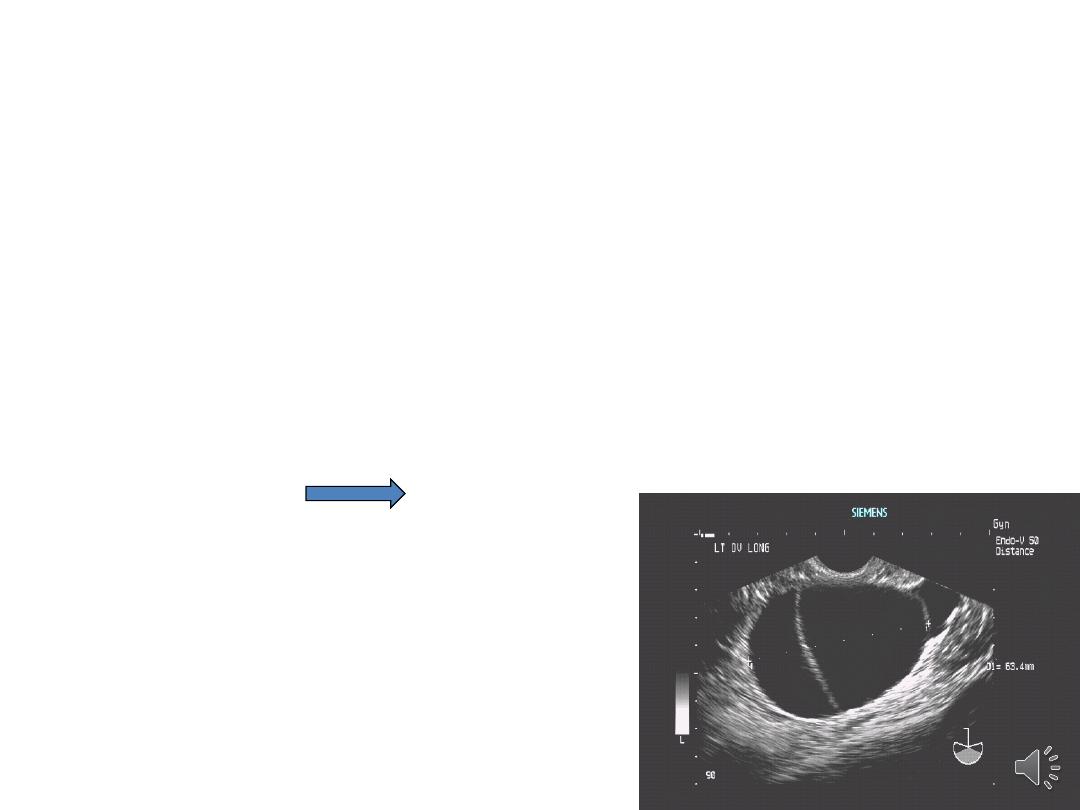
Investigations:
•
Ultrasound: TVUS may need abdominal US,
mass size, consistency, and internal
architecture. Bilatrality, ascites
•
Doppler ultrasonographies to evaluate the
resistive index of the mass vessels, which,
when low, may indicate a malignancy.
• if in doubt MRI

Blood test & serum markers:
some times
needed:
1.serum CA 125
2.beta-human chorionic gonadotrophin (β-
hCG)
3.Oestradiol
4.Androgen
5.alpha-fetoprotein levels
6.Lactate dehydrogenase (LDH)

• A serum CA-125 assay does not need to be
undertaken in all premenopausal women
when an ultrasonographic diagnosis of a
simple ovarian cyst has been made.
• Lactate dehydrogenase (LDH), α-FP and hCG
should be measured in all women under age
40 with a complex ovarian mass because of
the possibility of germ cell tumours.

The underlying management rationale is to
minimise patient morbidity by:
● conservative management where possible
● use of laparoscopic techniques where
appropriate, thus avoiding laparotomy where
possible
● referral to a gynaecological oncologist where
appropriate.

problems
The following masses pose the greatest concern:
• Those that have a complex internal structure
• Those that have solid components
• associated with pain
• Masses in prepubescent or postmenopausal
women
• Large cysts

In Perimenopausal Women: What is the best
way to estimate the risk of malignancy?
By:
Risk of Malignancy Index:
The RMI is a
product of the ultrasound scan score, the
menopausal status and the serum CA-125
level (IU/ml) as follows:
RMI = U x M x CA-125.
If ≥200 high suspicion of malignancy

Management of Ovarian cyst:
Criteria for observation of asymptomatic ovarian
cyst:
• Unilateral
• Unilocular cyst without solid components
• Premenopausal women tumour 3-7 cm in
diameter
• Normal CA 125 ( <35mIU/mL)
• No free fluid or masses suggesting omental cake
or matted bowel loops.

• Women with small (less than 50 mm diameter) simple
ovarian cysts generally
do not require follow-up
as these
cysts are very likely to be physiological and resolve
within 3 menstrual cycles.
• Women with simple ovarian cysts of 50–70 mm in
diameter should have yearly ultrasound follow-up
• those with larger simple cysts should be considered for
either further imaging (MRI) or surgical intervention.
• Ovarian cysts that persist or increase in size are unlikely
to be functional and may warrant surgical management.
• Patient with symptoms:
• severe, acute pain or signs of intraperitoneal
bleeding an emergency laparoscopy or
laparotomy will be required.
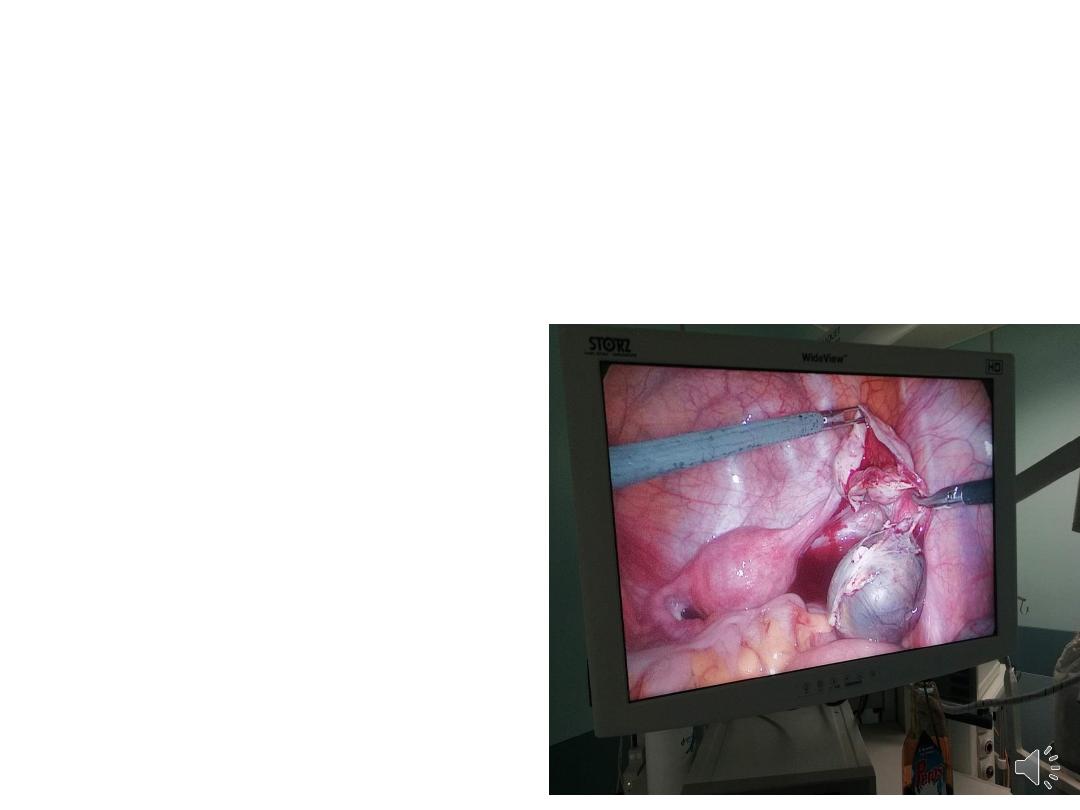
Laparoscopic procedures:
• The laparoscopic approach is associated with :
– Less adhesion formation
– lower postoperative morbidity
– shorter recovery time.
– cost-effective
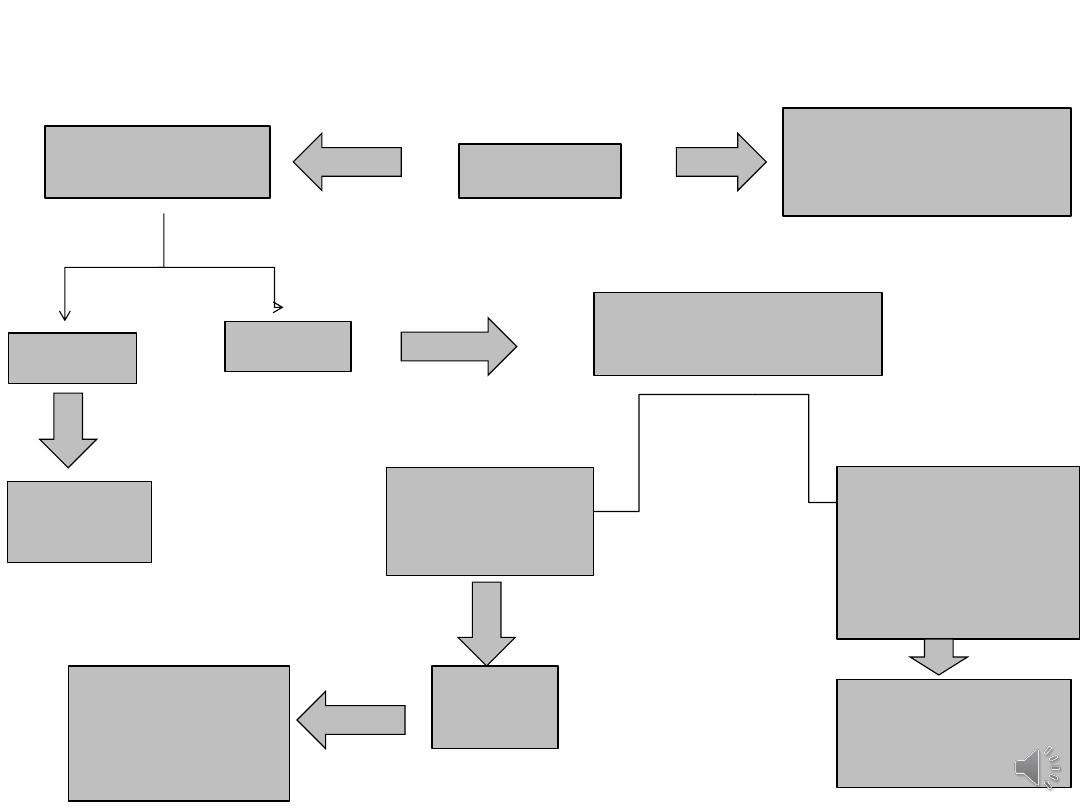
pregnant patient with Ovarian cyst
acute pain
Yes
laparotomy regardless
of the stage of
pregnancy
No
Depend on GA
<14 wk
Wait &
observe
> 14 Wk
Depend on the
features of cyst
<10 cm,
US: simple
appearance
Observe
by US
If not resolved
after
peurperium do
Surgery
>10 cm, features
suggestive of
malignancy on
ultrasound or one
that is growing
Surgery

Thank You