Dr.Safaa Hussain Alturaihy
Lecture
6

Nasal obstruction
Nasal Breathing Function
During normal nasal breathing, air passes through the anterior nares
over the nasal mucosa to the nasopharynx, with resulting humidification,
cleansing, filtering, and warming of the air but without the sensation
of obstruction. These functions are influenced by changes in the
natural environment, normal physiologic reflexes, normal anatomic
variations, and pathologic conditions
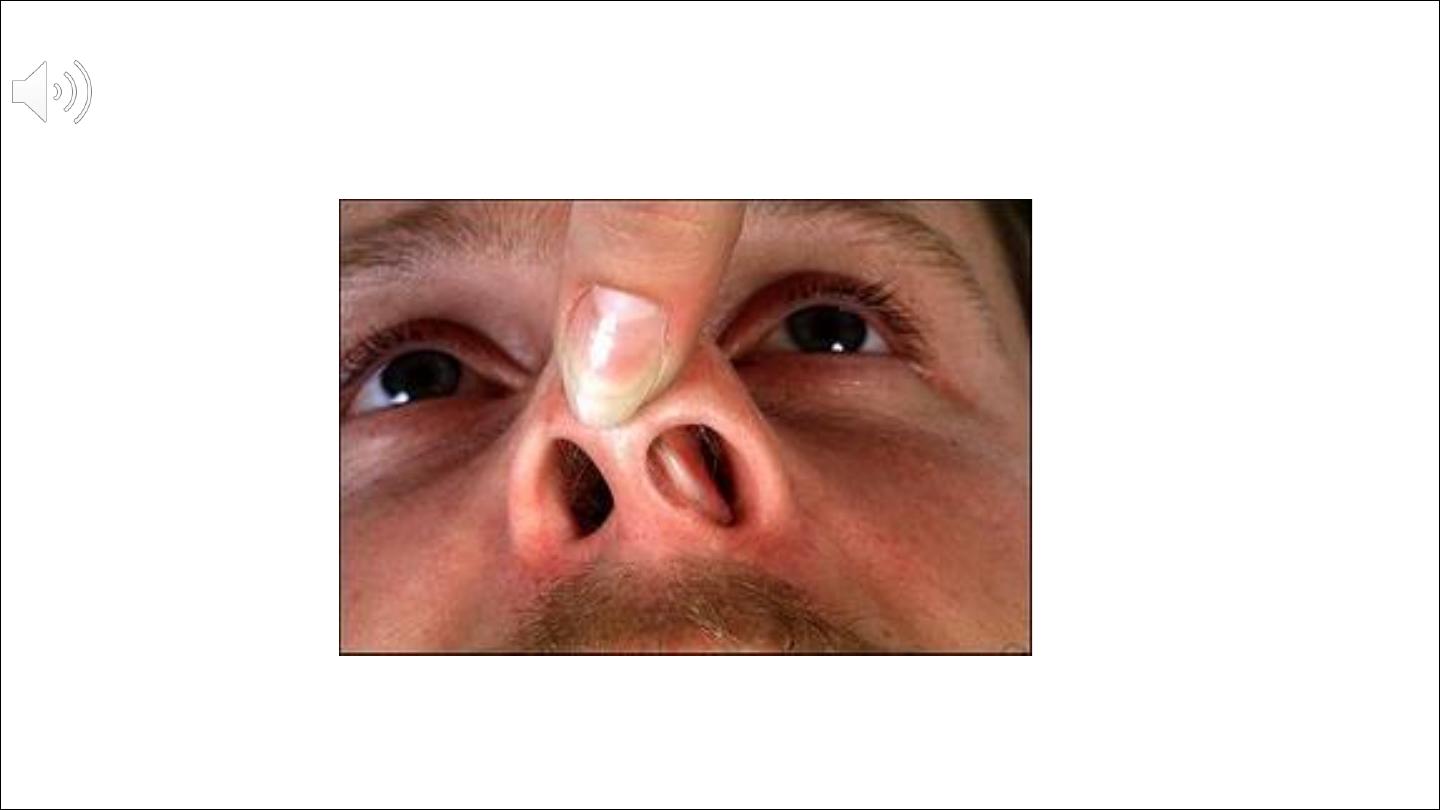
Nasal Septal Deviation
Nasal septal deviation is an asymmetric bowing of the nasal septum
that may compress the middle turbinate laterally, narrowing the middle
meatus
Bony spurs
are often associated with septal deviation,
which may further compromise the ostiomeatal unit. Nasal septal
deviation is usually congenital but may be a posttraumatic finding in
some patients life in utero onwards there are many risks of nasal trauma in which the septum is
involved.
Therefore, in adulthood a straight septum is more the exception than the rule
A straight septum is the exception rather than
the rule.

Cleft lip and palate
are two of the most common congenital conditions in
which the septum is involved, not only because the basal support of the
septum is missing, but also because surgical closure at a very young age
causes scar formation that inhibits further development of the surrounding
structures
Septal trauma is very common. It may occur at any stage of life. Often a
septal deformity is the only sign of trauma, which previously went
unnoticed or was forgotten

so the
causes of septal deviation
1 Trauma
2 Minimal with caecerian section
3 Moderate with normal vertex presentation
4 Severe with persistant occipitoposterior position
5 Genetic
Septal deviation Can be divided to
Spur
……sharp angulation occur at junction of vomer with septal cartilage
usually result of vertical compression force
Deviation
…….c or s shape involve cartilage and bone
Dislocation
….lower border of septal cartilage displaced from its medial
position into one of the nostril
The
symptoms
and
signs
accompanying septal deviation may be nasal
blockage, dryness,
crusting, bleeding, itching, rhinorrhoea, anosmia, headache and cosmetic
complaints

examination
First, the mucosa is inspected for swelling, vulnerable blood vessels, secretions,
pus, crusts, atrophy and dysplasia.
Congestion of the mucosa can mask or accentuate pathology related to the
skeleton, such as septal deviations, spurs and crests.
In order to observe these properly, decongestion by adrenaline or similar is
strongly recommended
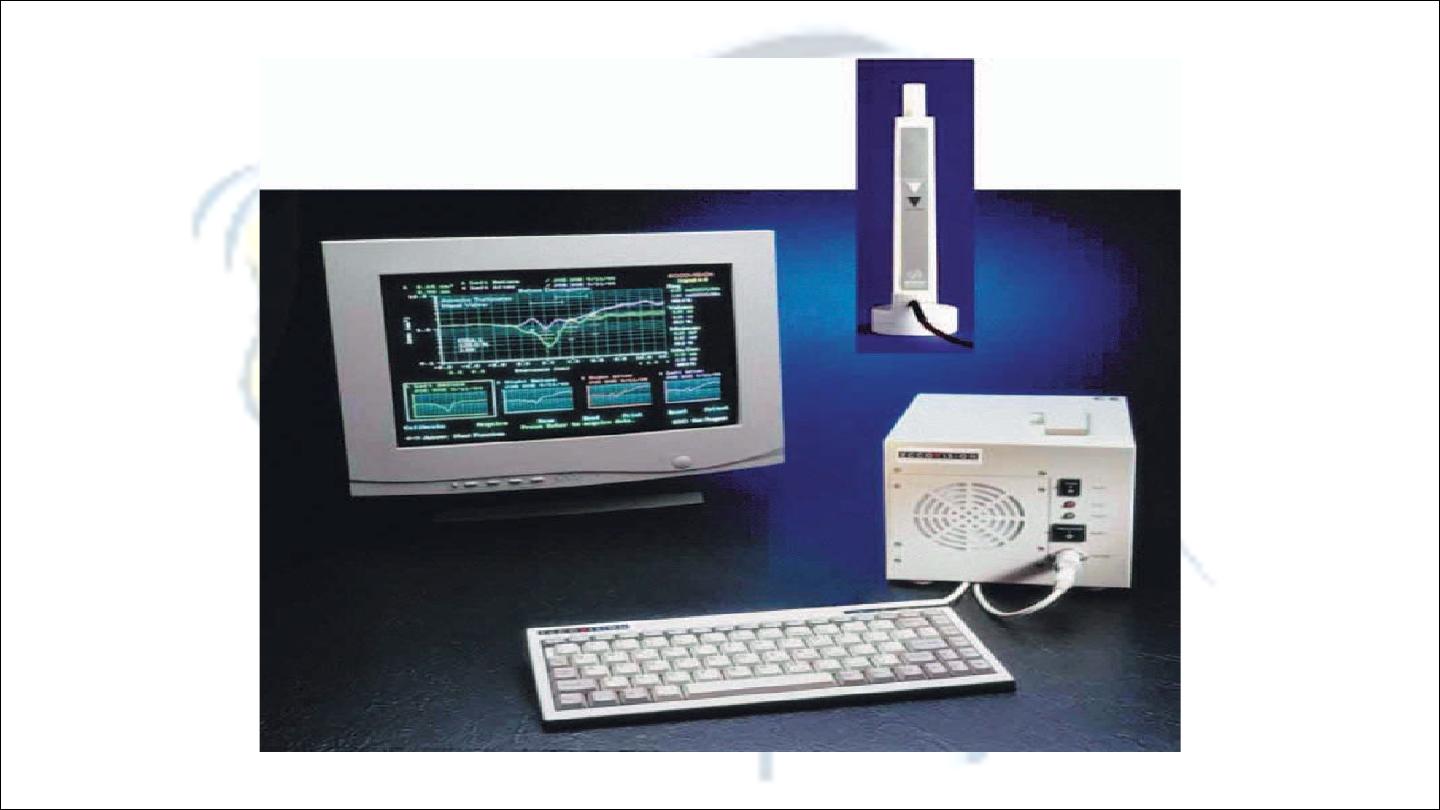
In
rhinomanometry
, two graphs are produced, one representing the relationship
between thepressure and flow in the right half of the nose and the other
in the left half of the nose
Acoustic rhinometry
is a means of measuring the cross-sectional area of the nose
INDICATIONS FOR SEPTOPLASTY
Nasal obstruction, crusting, rhinorrhoea, post-nasal
discharge, recurrent sinus pressure or pain,
epistaxis, headache, snoring and sleep apnoea
In septoplasty four general principles
1 Incision
2 Exposure
3Mobilization and straightening
3 fixation

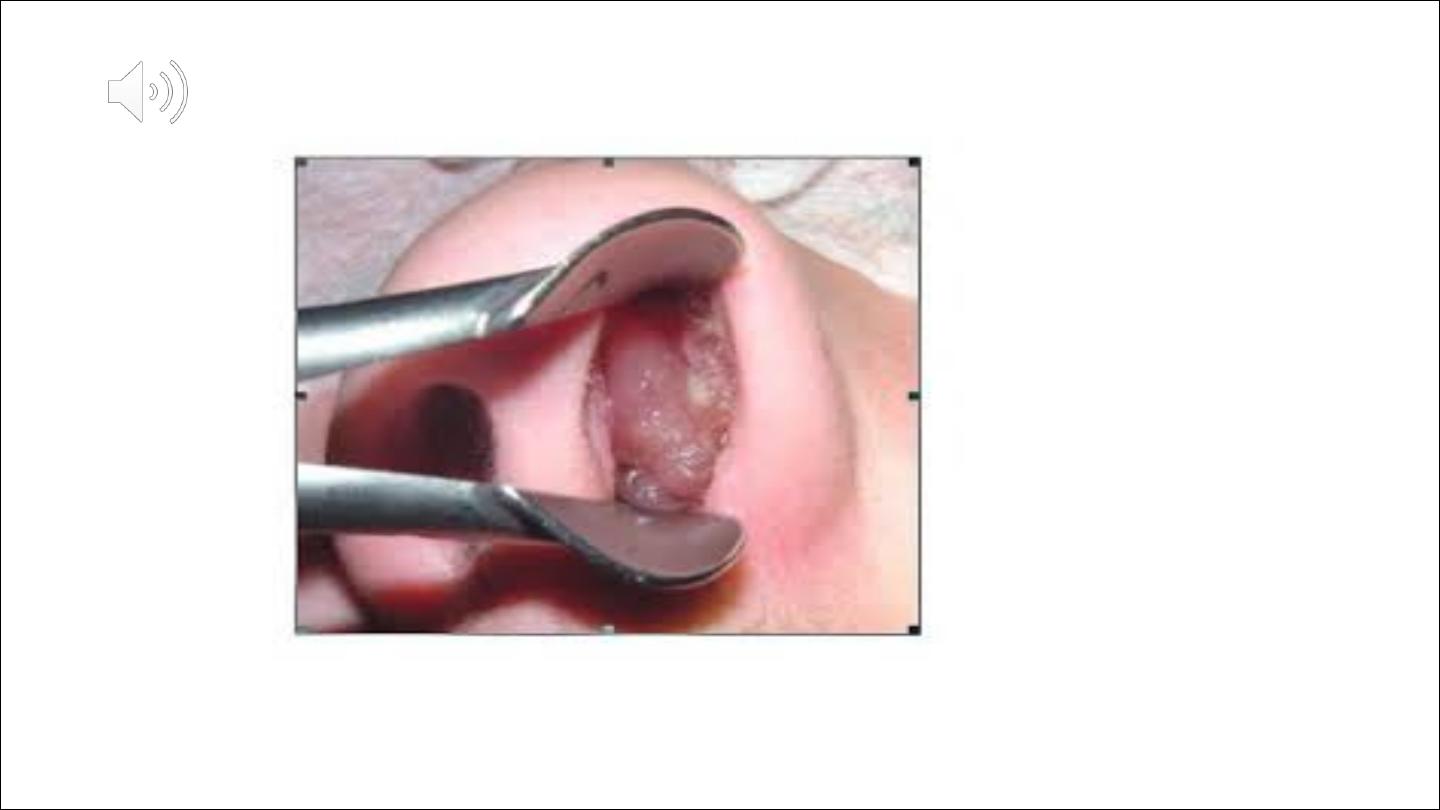
Nasal polyp
It is around ,smooth,translucent,soft,yellow or pale
structure results from prolapsed lining of ethmoid sinus

Aetiology
1
bernouilli phenomenon
If there is constriction the pressure will drop result in
prolapse of mucosa
2
polysaccride changes in ground substance
3
vasamotor imbalance when patient is not atopic
4
infection
5
allergy 90% or more of polyps have eosinophil and threr is
association with asthema,and the nasal finding mimic
allergy(rhinorrhea,sneezing &nasal obstruction


Incidence
It is a disease of adult, male predominance.
If present below
2 year
think of maningocele
If present below
10 year
think of cystic fibrosis
Any child with nasal polyps should be regarded as having
cystic fibrosis until proved otherwise
Unilateral nasal polyp need histopathological study


Sign and symptoms
☻
Polyp seen by anterior rhinoscopy occasionally seen
normal externally
☻
Mouth breathing due to nasal obstruction which is
constantly present but of varying degree depending on the
size of polyp
☻
Watery rhinorrhea
☻
Post nasal drip
☻
Anosmia
☻
Hyponasal voice
☻
Hypertelorism may develop if patient develop polyp
befor fusion of facial bone
Management
Aneroir rhinoscopy is enough to diagnose nasal polyp
Plain x-ray
CT scan
Nasal polyp treated either
medically
by short course of
systemic steroid or intranasal steroid(betamethasone) or
steroid nasal drops for one month this depend on the extent
of the polyposis

Surgical treatment
1
simple polypectimy
2
intranasal ethmoidectomy which done
endoscopically
3
external ethmoidectomy

Antrochoanal polyp
Antrchoanal polyps are a separate entity,this polyp has two
components,a solid nasal one and a cystic maxillary one
It is less common arise from maxillary antrum and prolapsed
through the ostium of the sinus to the nasal cavity and
nasopharynx
It is common in adolescence
Ther is no place of medical treatment in antrochoanal polyp
It is due to collection of blood beneath the
mucoprechondrium of the nasal septum this
collection interfere with the vitality of the cartilage
,the cartilage remain viable for 3 days more than 3
days the chondrocyte die lead to absorption of the
cartilage
Clinical pictures
Nasal obstruction---
complete bilateral nasal obstruction
Discomfort
Septal swelling soft red in colour
Complication
Septal abcess
Cartilage necrosis
Nasal saddle deformity

Treatment
Simple aspiration ---if haematoma is small
Incision and drainage
Packing to obliterate dead space with or without
quilting suture
Systemic AB

Septal abcess
*
Mostly due to trauma 75%
*
Infective –measle,scarlet
fever,furenculosis,AIDS.
*
Complicate ethmoid and sphenoid sinus infection
Complication
Spread infection to orbit,meningies,brain,cavernous
sinus

Clinical pictures
Sever pain
Septal swelling
Nasal obstruction
Pyrexia
Treatment
Immediate drainage
Systemic AB
Reconstruction of the defect in the acute phase will
reduce growth impaction
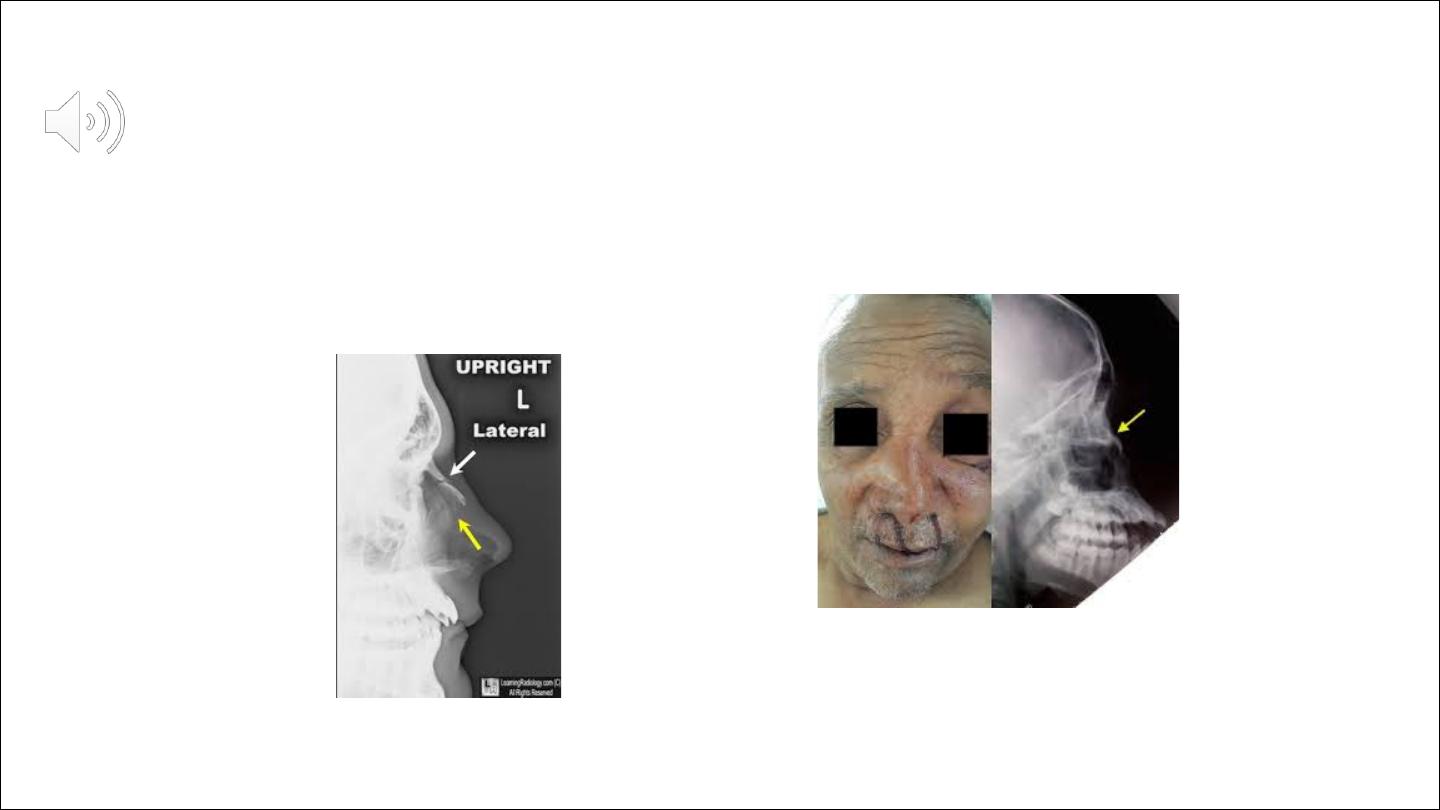
Fracture nasal bone
Treatment of nasal fractures was first recorded 5000 years ago during the early
Pharonic period inAncient Egypt
Delays in management can result in significant cosmetic
and functional deformity that is often a cause for subsequent medicolegal action
The prominence and delicate structure of the nose make it vulnerable
to a broad spectrum of injurywhich accounts for why it is the most
frequently fractured facial bone.
Sports, falls, and assaults
are the
usual mechanisms responsible for the majority of nasal fractures, with
alcohol consumption being an important contributing factor in many
cases. Males are affected approximately twice as often as females
in both the adult and pediatric populations, with a peak incidence
occurring during the second and third decades of life
Deformity, swelling, epistaxis, and periorbital ecchymosis are signs that
are suggestive of nasal fracture, whereas bony crepitus and nasal
segment
mobility are diagnostic

Pathophysiology
Understanding the process by which nasal fractures occur and how
injuries to key areas of support can alter appearance and function are
essential to appropriate treatment. Variables such as force, impact
direction, nature of the striking object, patient’s age, and other host factors
will influence the pattern of injury to both the bony and cartilaginous
components of the nose.

The cartilaginous portions of the external nose are able to absorb
a greater amount of force without fracture as compared with the bony
components,
Pattern of fracture
Nasal fractures can be subdivided into three broad categories that
characterize the patterns of damage sustained with increasing force.
This classification has some practical utility as each category of fracture
requires a different method of treatment
CLASS 1
are the result of low–moderate degrees of force and hence the extent of
deformity is usually not marked.
The simplest form of a class 1 fracture is the depressed nasal bone,
The fractured segment usually remains in position due to its inferior attachment
to the upperlateral cartilage which provides an element of recoil.
The nasal septum is generally not involved. In the more severe variant, both nasal
bones and the septum are fractured .
Class 1 fractures tend not to cause gross lateral displacement of the nasal bones
and may not even be perceptible.
Deformity generally results from a persistently depressed fragment, which is
often due to impaction of the flail segment beneath the residual nasal bone. In
children, these fractures may be of the ‘greenstick’ variety and significant nasal
deformity may only develop at puberty when nasal growth becomes accentuated
Class 2
fractures are the result of greater force and are often associated with
significant cosmetic deformity.
In addition to fracturing the nasal bones, the frontal process of the maxilla
and septalstructures are also involved.
The ethmoid labyrinth and adjacent orbital structures remain intact.

Class 3
fractures are the most severe nasal injuries encountered and usually result from
highvelocity trauma.
They are also termed naso-orbito-ethmoid fractures and often have associated
fractures of the maxilla.
The external butresses of the nose give way and the ethmoid Labrynth collapses
on itself. This causes the perpendicular plate of the ethmoid to rotate and the
quadrilateral cartilage to fall backwards. These movements cause a classic, ‘pig-
like’ appearance to the patient, with a foreshortened saddled nose and the
nostrils facing more anteriorly, like the snout of a pig.
There is also telecanthus, which may be exaggerated further by disruption of the
medial canthal ligament from the crest of the lacrimal bone
Management
Look after
• details of how the injury was sustained;
• nasal obstruction;
• change in appearance;
• epistaxis;
• hyposmia;
• watery rhinorrhoea;
• visual disturbance;
• diplopia;
• epiphora;
• altered bite;
• loose teeth;
• trismus
Examination
deviation, depression, step deformities;
• mobility, crepitus, specific areas of point
tenderness;
• generalized swelling;
• skin lacerations;
• septal fracture/haematoma/abscess/perforation;
• mucosal laceration

Investigation
The need for nasal x-rays is controversial and in many places it is actively
discouraged.
Unlike other fractures, nasal x-rays are not required in order to make the
diagnosis or aid subsequent reduction.

Treatment
A very significant number of patients do not require any active treatment.
Many do not have a nasal fracture and, in those that do, the fracture
may not be displaced.
Soft tissue swelling can produce the misleading appearance of a deformity
which disappears as the swelling subsides.
Reassurance is all that these patients require and some may heed suggestions to
avoid further trauma.
Topical vasoconstrictor drops are helpful to alleviate congestion and obstructive
symptoms.
A reexamination about five days later is prudent
where there is uncertainty about the need for reduction,a large number of
patients will have a preexisting nasal deformity caused by a previous incident
Manipulation of the nose will, at best, only return it to its most recent
appearance.
Patients that fall into this category are probably better advised to consider a
formal rhinoplasty when everything has settled down some months later.
The indications for surgical intervention in the acute phase are significant
cosmetic deformity
and
nasal obstruction caused by a septal haematoma
As a general rule, primary care physicians should refer all patients to ENT
departments forevaluation if there is any deformity or significant nasal
obstruction.
Patients with a suspected septal haematoma should be seen urgently at the first
possible opportunity.

Reduction of a fractured nose can be performed under local or general anaesthesia.
Local anaesthesia has the advantages of reduced cost and convenience
Local anaesthetic can be used as a combination of external infiltration with internal
application of topical preparations.
Lignocaine is injected along the nasomaxillary groove, infraorbital nerve in its
foramen and around the infratrochlear nerve.
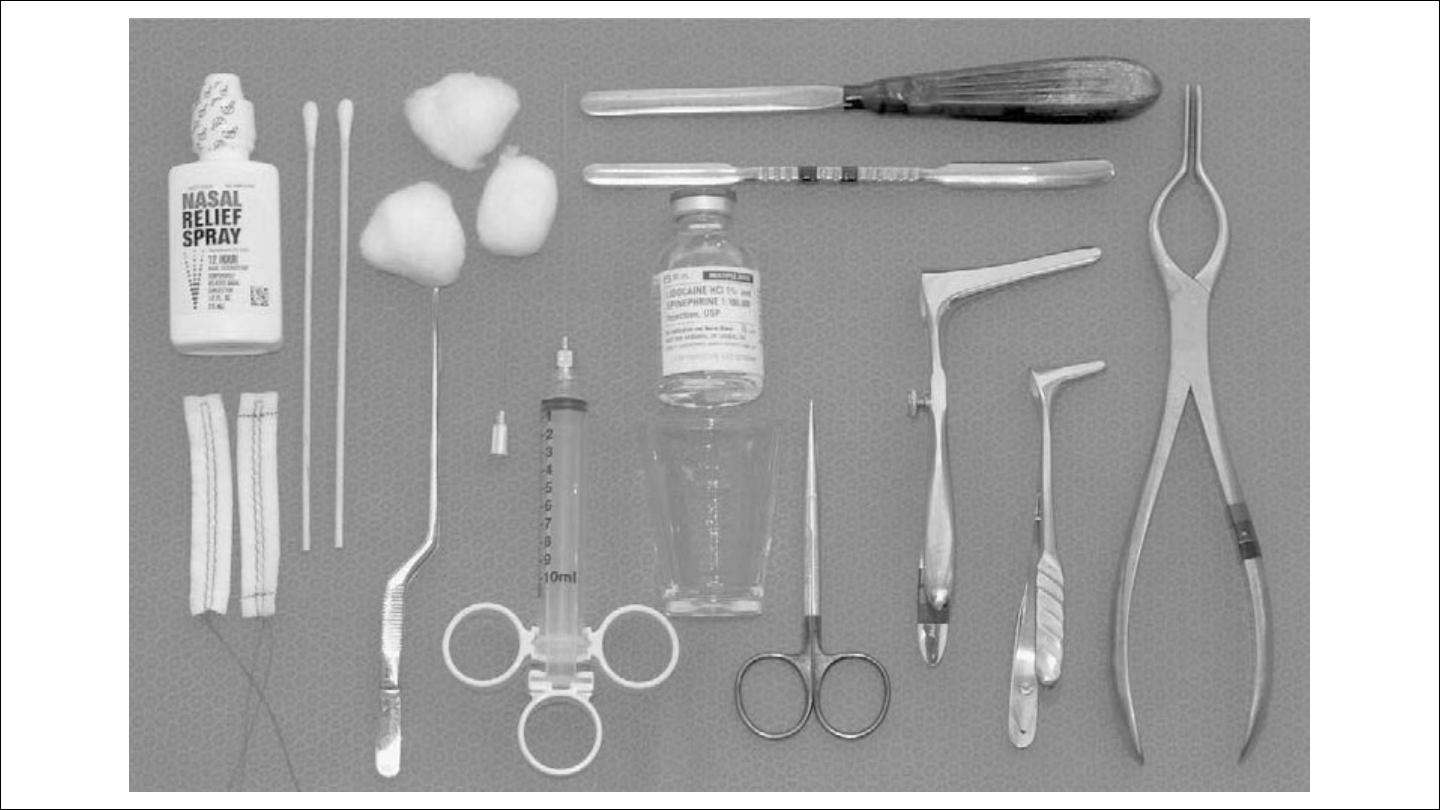
Within the nose, sprays, injections, pastes or packs coated with local anaesthetic are all
acceptable, using combinations of cocaine, lignocaine, adrenaline and phenylephrine.
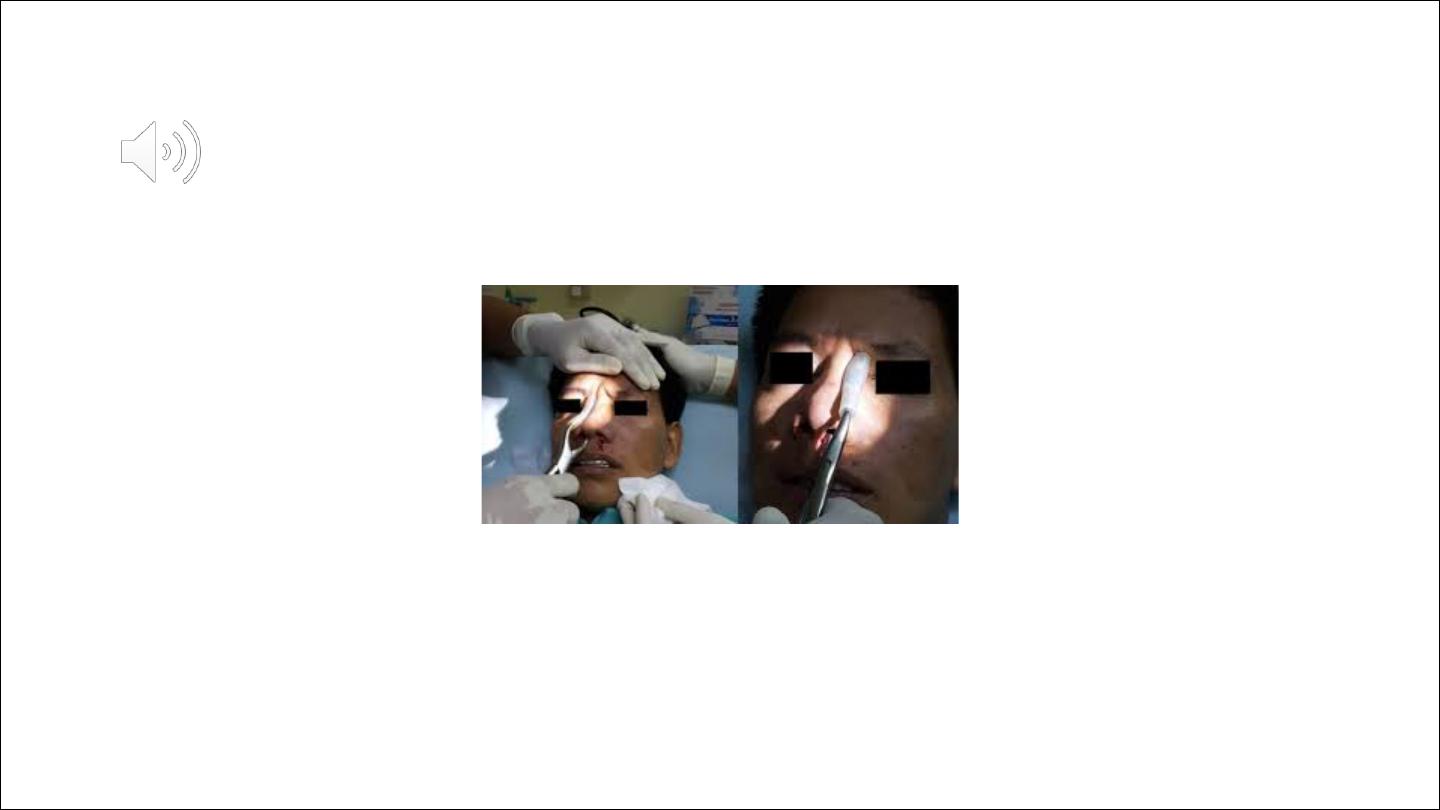
The general principle of fracture reduction is to mobilize the fragments first by
increasing and then decreasing the degree of deformity
Ashe and Walsham
forceps
Splints or packs may be necessary, depending on the stability of the reduction
and the surgeon's preference.
A splint or plaster applied to the nasal bridge maintains, to some extent, the
position of the nasal bones and prevents accidental displacement.
Splints are usually kept in place for about seven days.
It is advisable to refrain from contact sports for at least six weeks
All class 1 and most class 2 fractures can be reducedwith these techniques.

indications for open reduction
:
• bilateral fractures with dislocation of the nasal dorsum and significant
(preexistent or recent) septal deformity;
• infraction of the nasal dorsum;
• fractures of the cartilaginous pyramid, with or without dislocation of the
upper laterals
For depressed tip or flail lateral fractures that are unstable despite closed
reduction techniques, Kirschner (K) wires can be used
The external wire can be covered by dressings or plaster to protect the
wires from disruption and the patient from injury.
The wires are removed after two weeks