Thrombosis
By dr Alaa sadiq
1

Haemostasis
•Blood must be maintained in a fluid state in order to
function as a transport system, but must be able to
solidify to form a clot following vascular injury in
order to prevent excessive bleeding, a process
known as haemostasis.
•Successful haemostasis is localised to the area of
tissue damage and is followed by removal of the clot
and tissue repair.
•This is achieved by complex interactions between the
vascular endothelium, platelets, coagulation factors,
natural anticoagulants and fibrinolytic enzymes .
•Dysfunction of any of these components may result
in haemorrhage or thrombosis
2

Platelets
• Platelets are formed in the bone marrow from megakaryocytes.
• Megakaryocytic stem cells
• The formation and maturation of megakaryocytes are stimulated
by Thrombopoietin produced in the liver.
• Platelets circulate for 8–10 days before they are destroyed in the
reticulo-endothelial system.
• Some 30% of peripheral platelets are normally pooled in the
spleen and do not circulate
• Drugs which inhibit platelet function and thrombosis include
aspirin (cyclo-oxygenase inhibitor), clopidogrel (adenosine
diphosphate (ADP)-mediated activation inhibitor),dipyridamole
(phosphodiesterase inhibitor), and the
IIb/IIIa inhibitors abciximab, tirofiban and eptifibatide(which
prevent fibrinogen binding)
3

Clotting factors
•Clotting factors are synthesised by the liver, although
factor V is also produced by platelets and
endothelialcells.
•Factors II, VII, IX and X in the liver is vitamin K-
dependent. Vitamin K must be reduced to its active
form by a reductase enzyme. This reductase is
inhibited by warfarin, and this is the basis of the
anticoagulant effect of coumarins .
•Congenital (e.g.haemophilia) and acquired (e.g. liver
failure) causes of coagulation factor deficiency are
associated with bleeding
4

Investigation of coagulation
• The tissue factor (‘extrinsic’) pathway is assessed by the prothrombin
time (PT), and the ‘intrinsic’ pathway by the activated partial
thromboplastin time (APTT),
• Coagulation is delayed by deficiencies of coagulation factors and by
the presence of inhibitors of coagulation, such as heparin .
• If both the PT and APTT are prolonged, this indicates either deficiency
or inhibition of the final common pathway (which includes factors X, V,
prothrombin and fibrinogen) or global coagulation factor deficiency
involving more than one factor, as occurs in disseminated intravascular
coagulation .
• A mixing test with normal plasma allows differentiation between a
coagulation factor deficiency(the prolonged time corrects) and the
presence of an inhibitor of coagulation (the prolonged time does not
correct);
• the latter may be chemical (heparins) or an antibody (most often a
lupus anticoagulant but occasionally a specific inhibitor of one of the
coagulation factors, typically factor VIII). Willebrand disease may
present with anormal APTT
5

• Platelet function has historically been assessed by the
bleeding time, measured as the time to stop bleeding after
astandardised incision.
• However, most centres have abandoned the use of this test.
• Platelet function can be assessed in vitro by measuring
aggregation in response to various agonists,
• Coagulation screening tests are also performed in patients
with suspected DIC, when clotting factors and platelets are
consumed, resulting in thrombocytopenia
and prolonged PT and APTT.
In addition, there is evidence of active coagulation with
consumption of fibrinogen and generation of fibrin
degradation products (D-dimers).
• Note, however, that fibrinogen is an acute phase protein
which may also be elevated in inflammatory disease.
6

• The international normalised ratio (INR) is validated only to
assess the therapeutic effect of coumarin anticoagulants,
including warfarin. INR is the ratio of the patient’s PT to that
of a normal control, raised to the power of the international
sensitivity index (ISI)
• Monitoring of heparin therapy is, on the whole, only
required with unfractionated heparins.
• Therapeutic anticoagulation prolongs the APTT relative to a
control sample by a ratio of approximately 1.5–2.5
• Low molecular weight heparins have such a predictable dose
response that monitoring of the anticoagulant effect is not
required, except in patients with renal impairment
(glomerular filtration rate less than 30 mL/min). When
monitoring is indicated, an anti-Xa activity assay rather than
APTT should be used
7
Thrombotic disorders
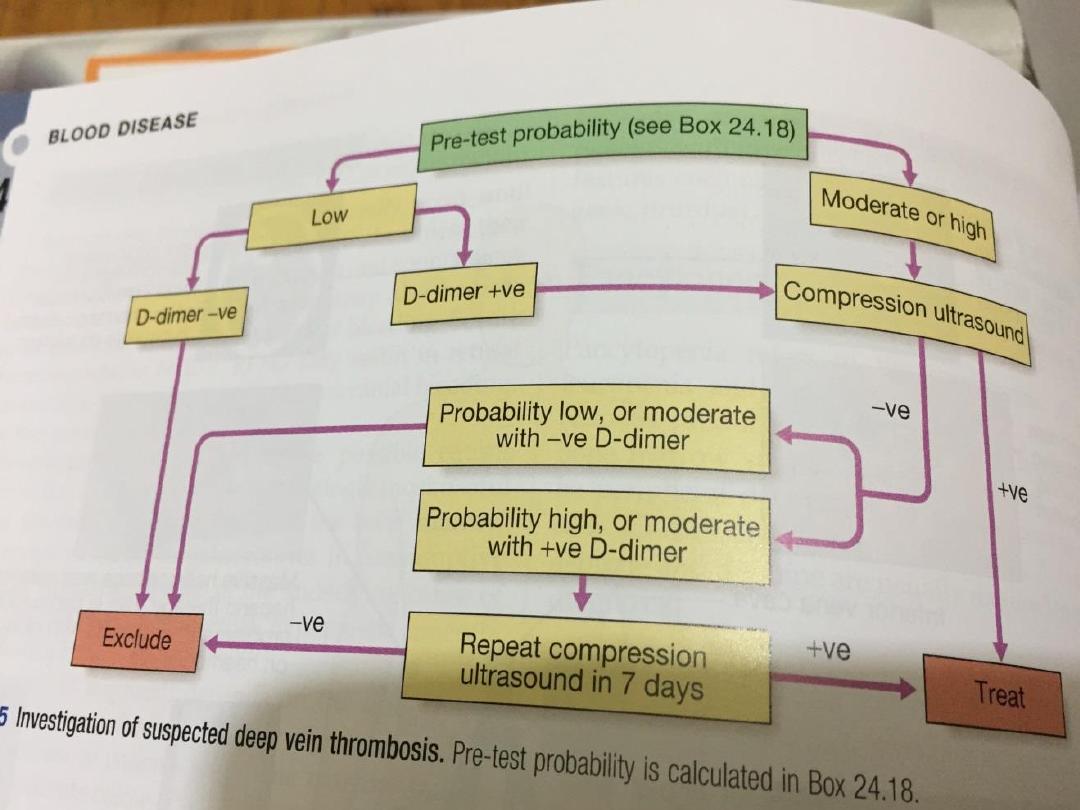
• Measurement of plasma levels of D-dimers derived from fibrin degradation is
useful in excluding the diagnosis of active venous thrombosis in some patients .
8

Venous thrombosis
• While the most common presentation of venous
thromboembolic disease (VTE) is with deep vein thrombosis
(DVT) of the leg and/or pulmonary embolism similar
principles apply to rarer manifestations such as jugular vein
thrombosis, upper limb DVT, cerebral sinus thrombosis and
intra-abdominal venous thrombosis (e.g. Budd–Chiari
syndrome;
• DVT has an annual incidence of approximately 1 : 1000 in
Western populations and the case mortality is
1–3%. It is increasingly common with ageing, and many of
the deaths are related to coexisting medical conditions,such
as active cancer.
9

Clinical assessment
• Lower limb DVT characteristically starts in the distal veins, causing
pain, swelling, an increase in temperature and dilatation of the
superficial veins. Often, however, symptoms and signs are minimal.
• It is typically unilateral but may be bilateral, and clot may extend
proximally into the inferior vena cava.
• Bilateral DVT is more commonly seen with underlying malignancy or
anomalies of the inferior vena cava.
• The differential diagnosis of unilateral leg swelling includes a
spontaneous or traumatic calf muscle tear or a ruptured Baker’s cyst,
both characterise by sudden onset and localised tenderness. Infective
cellulitis is usually distinguished by marked skin erythema and heat
localised within a well-demarcated area of the leg and may be
associated with an obvious source of entry of infection (e.g. insect bite,
leg ulcer).
• Risk factors for DVT should be considered and examination should
include assessment for malignancy.
10

• Symptoms and signs of PE should be sought particularly in those with proximal
thrombosis; asymptomatic PE is thought to be present in approximately 30% of
patients with lower limb DVT.
• Clinical criteria can be used to rank patients according to their likelihood of DVT
or PE: for example, by using scoring systems such as the Wells score
11
Management
• The management of leg DVT includes elevation and analgesia.
Thrombolysis may be considered for limbthreatening DVT, but
the mainstay of treatment is anticoagulation with low molecular
weight heparin (LMWH), followed by a coumarin anticoagulant,
such as warfarin.
• An alternative is the oral Xa inhibitor, rivaroxaban, which has a
rapid onset of action and can be used immediately from
diagnosis without the need for LMWH.
• Treatment of acute VTE with LMWH should continue for at least
5days.
• If a coumarin is being introduced, the heparin should continue
until the INR has been in the target range for 2 days.
• Patients who have had a DVT and have a strong contraindication
to anticoagulation, and those who, despite therapeutic
anticoagulation, continue to have new pulmonary emboli,should
have an inferior vena cava filter inserted to prevent life-
threatening PE.
12

•The optimal initial duration of anticoagulation is
between 6 weeks and 6 months. Patients who have
thrombosis in the presence of a temporary risk
factor, which is then removed, can usually be treated
for shorter periods (e.g. 3 months) than those who
sustain unprovoked thrombosis.
13
14

• Post-thrombotic syndrome is due to damage of venous
valves by the thrombus. It results in persistent leg swelling,
heaviness and discoloration.
• The most severe complication of this syndrome is ulceration
around the medial malleolus.
Antithrombin deficiency
• Antithrombin (AT) is a serine protease inhibitor (SERPIN)
which inactivates the activated coagulation factors IIa, IXa,
Xa and XIa. Heparins, fondaparinux and idraparinux achieve
their therapeutic effect by potentiating the activity of AT.
• Familial deficiency of AT is inherited as an autosomal
dominant; homozygosity for mutant alleles is not compatible
with life. Around 70% of affected individuals will have an
episode of VTE before the age of 60 years and the relative
risk for thrombosis compared with the background
population is 10–20.
15

• Pregnancy is a high-risk period for VTE and this requires
fairly aggressive management with doses of LMWH which
are greater than the usual prophylactic doses (≥ 100
U/kg/day). AT concentrate (either plasmaderived or
recombinant) is available; this is required for
cardiopulmonary bypass and may be used as an adjunct to
heparin in surgical prophylaxis.
• Protein C and S are vitamin K-dependent natural
anticoagulants involved in switching off coagulation factor
activation (factors Va and VIIIa) and thrombin generation .
Inherited deficiency of either protein C or S results in a
prothrombotic state with a fivefold relative risk of VTE
compared with the background population.
16

Factor V Leiden
• Factor V Leiden results from mutation which prevents the cleavage
and hence inactivation of activated factor V. This results in a relative
risk of venous thrombosis .
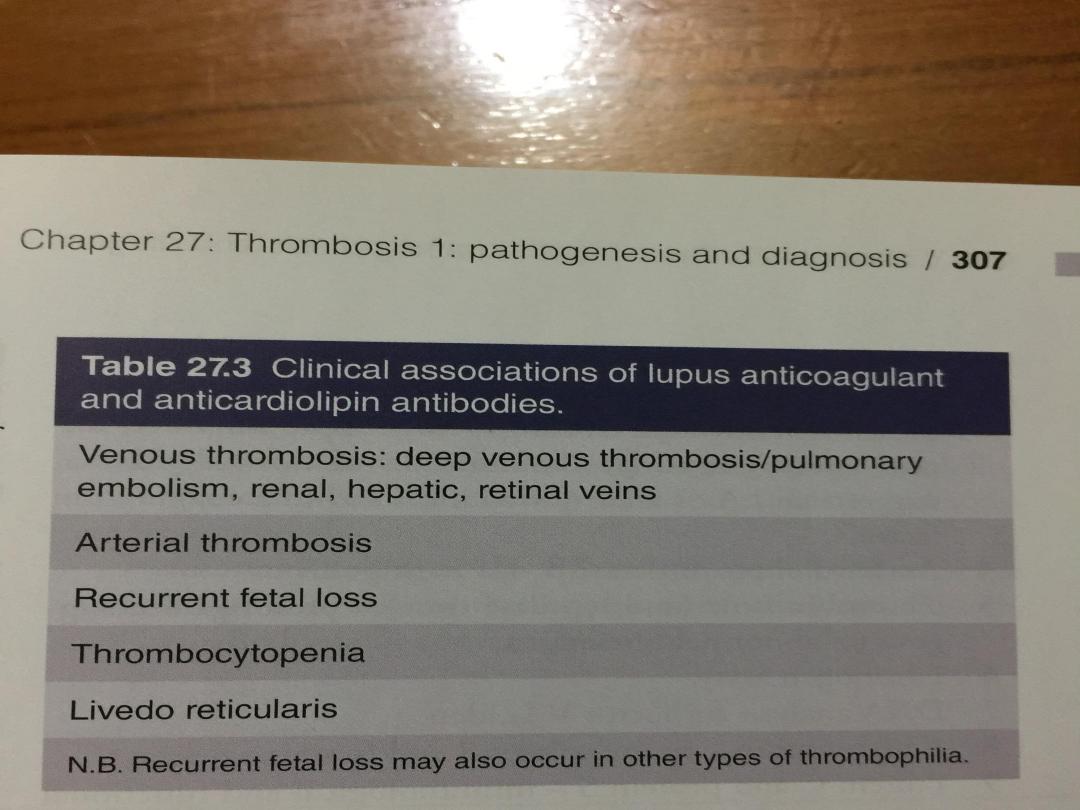
Antiphospholipid syndrome
• Antiphospholipid syndrome (APS) is a clinicopathological entity in
which a constellation of clinical conditions, alone or in combination, is
found in association with apersistently positive test for an
antiphospholipid antibody.
• The mechanisms underlying the clinical features of APS are not clear.
• In clinical practice, two types of test are used, which detect: antibodies
(called an anticardiolipin antibody test) those which interfere with
coagulation tests like the APTT or the dilute Russellviper venom time (
called a lupus anticoagulant test).
• The term antiphospholipid antibody encompasses both a lupus
anticoagulant and an anticardiolipin antibody;
• individuals may be positive for one or both of these activities.
17

• Arterial thrombosis, typically stroke, associated with APS
should be treated with warfarin, as opposed to aspirin. APS-
associated VTE is one of the situations in which the
predicted recurrence rate is high enough to indicate long-
term anticoagulation after a first event
18
19

Disseminated intravascular coagulation
• Disseminated intravascular coagulation (DIC) may
complicate a range of illnesses . It is characterised by
systemic activation of the pathways involved in coagulation
and its regulation.
• This may result in the generation of intravascular fibrin clots
causing multi organ failure, with simultaneous coagulation
factor and platelet consumption causing bleeding.
• There is consumption of platelets, coagulation factors
(notably factors V and VIII) and fibrinogen.
• The lysis of fibrin clot results in production of fibrin
degradation products (FDPs), including D-dimers.
20

investigations
• Measurement of coagulation times (APTT and PT), along with
fibrinogen,
• platelet count and FDPs, helps in the assessment of prognosis and aids
clinical decision-making with regard to both bleeding and thrombotic
complications.
Management
• Therapy is primarily aimed at the underlying cause.These patients will
often require intensive care to deal with concomitant issues, such as
acidosis dehydration, renal failure and hypoxia.
• Blood component therapy, such as fresh frozen plasma, cryoprecipitate
and platelets, should be given if the patient is bleeding or to cover
interventions with high bleeding risk, but should not be prescribed
routinely based on coagulation tests and platelet counts alone.
• Prophylactic doses of heparin should be given, unless there is a clear
contraindication.Established thrombosis should be treated cautiously
with therapeutic doses of unfractionated heparin, unless clearly
contraindicated. Patients with DIC should not, in general, be treated
with antifibrinolytic therapy, e.g. tranexamic acid.
21

Thrombotic thrombocytopenic
purpura
• Like DIC and also heparin-induced thrombocytopenia
thrombotic thrombocytopenic purpura (TTP) is a disorder in
which thrombosis is accompanied by paradoxical
thrombocytopenia.
• TTP is characterised by a pentad of findings, although few
patients have all five
Components:
1. thrombocytopenia
2. microangiopathic haemolytic anaemia
3. neurological sequelae
4. fever
5. renal impairment.
22

• It is an acute autoimmune disorder mediated by antibodies
The features are of microvascular occlusion by platelet
thrombi affecting key organs, principally brain and kidneys. It
is a rare disorder (1 in 750 00 perannum), which may occur
alone or in association with drugs (ticlopidine, ciclosporin),
HIV, shiga toxins and malignancy.
• It should be treated by emergency plasma exchange.
• Corticosteroids, aspirin and rituximab also have a role in
management.
• Untreated mortality rates are 90% in the first 10 days, and
even with appropriate therapy, the mortality rate is 20–30%
at 6 months.
23