
Contact Dermatitis
Irritant Contact Dermatitis
Irritation of the skin is the most common cause of contact dermatitis. The epidermis is a
thin cellular barrier with an outer layer composed of dead cells in a water-protein-lipid matrix.
Any process that damages any component of the barrier compromises its function, and a
nonimmunologic eczematous response may result. Repeated use of strong alkaline soap or
industrial exposure to organic solvents, extracts lipid from the skin. Acids may combine with
water in the skin and cause dehydration. When the skin is compromised, exposure to even a
weak irritant sustains the inflammation. The intensity of the inflammation is related to the
concentration of the irritant and the length of exposure. Mild irritants cause dryness, fissuring,
and erythema; a mild eczematous reaction may occur with continuous exposure. Continuous
exposure to moisture in areas such as the hand, the diaper area, or the skin around a colostomy
may eventually cause eczematous inflammation. Strong chemicals may produce an immediate
reaction. Patients vary in their ability to withstand exposure to irritants. Some people cannot
tolerate frequent hand washing whereas others may work daily with harsh cleaning solutions
without any difficulty.
Allergic Contact Dermatitis
Allergic contact dermatitis is an inflammatory reaction that follows absorption of
antigen applied to the skin and recruitment of previously sensitized, antigen-specific T
lymphocytes into the skin. It affects a limited number of individuals. The antigens are usually
low-molecular-weight substances that readily penetrate the stratum corneum. Most contact
allergens are weak and require repeated exposure before sensitization occurs. Strong antigens,
such as poison ivy, require only two exposures for sensitization.
Interaction between antigen and T lymphocytes is mediated by antigen-presenting
epidermal cells (Langerhans' cells) and is divided into two sequential phases: an initial
sensitization phase and an elicitation phase. .
Sensitization phase.
Antigen is applied to the skin surface, penetrates the epidermal barrier (stratum
corneum) and is taken up by Langerhans' cells in the epidermal basal layer. The antigen is
“processed” and displayed on the surface of the Langerhans' cell. This cell migrates to the
regional lymph nodes and presents the antigen to T lymphocytes. Cytokine-induced
proliferation and clonal expansion within the lymph nodes results in T lymphocytes bearing
receptors that recognize the specific antigen. These antigen-specific T lymphocytes enter the
bloodstream and circulate back to the epidermis. This process taken about 1-3 weeks.
Elicitation phase.
The elicitation phase occurs in sensitized patients with reexposure to the antigen.
Langerhans' cells bearing the antigen interact with antigen-specific T lymphocytes that are
circulating in the skin. This interaction results in cytokine-induced activation and proliferation
د
.
و
ﺳ
ﺎ
م
ﻋ
ﻠ
ﻲ
ﻋ
ﻮ
ض
ﻟا
ﻤ
ﺤ
ﺎ
ﺿ
ﺮ
ة
ا
ﺜﻟ
ﻧﺎ
ﯿ
ﺔ

of the antigen-specific T lymphocytes and the release of inflammatory mediators. Allergic
weeks.
Etiologic Agents:
Irritants cause more cases of contact dermatitis than do allergens, although the clinical
appearances are often similar. Allergic contact dermatitis is an example of type IV
hypersensitivity.
Irritant dermatitis:
The most important irritants are:
• Water and other fluids.
• Abrasives i.e. frictional irritancy.
• Chemicals, e.g. acids and alkalis.
• Solvents and detergents.
Allergic dermatitis:
Allergens Source
Chromate Cement, tanned leather, primer paint, anticorrosive
Cobalt Pigment, paint, ink, metal alloys
Fragrance Cosmetics, creams, soaps, detergents
Nickel Jewellery, zips, fasteners, scissors, and instruments
Paraphenylene diamine Dye (clothing, hair), shoes, colour developer
Plants Garlic, poison ivy
Preservatives Cosmetics, creams and oils
Rubber chemicals Tyres, boots, shoes, belts, condoms, gloves
Clinical presentation
Contact dermatitis may affect any part of the body, although the hands and face are
common sites. The appearance of a dermatitis at a particular site suggests contact with certain
objects. For example, eczema on the wrist of a woman with a history of reacting to cheap
earrings suggests a nickel allergic response to a watch strap buckle. Diagnosis is often not easy
as a history of irritant or allergen exposure is not always forthcoming.
Knowing the patient's occupation, hobbies, past history and use of cosmetics or
medicaments helps in listing possible causes. Delayed onset of 7-10 days in allergic dermatitis
(but with repeated exposure, can be accelerated to 12 hrs.
Skin findings:
Acute: erythema, edema, vesicles, erosions
Subacute: mild erythema, less vesiculation, some thickening
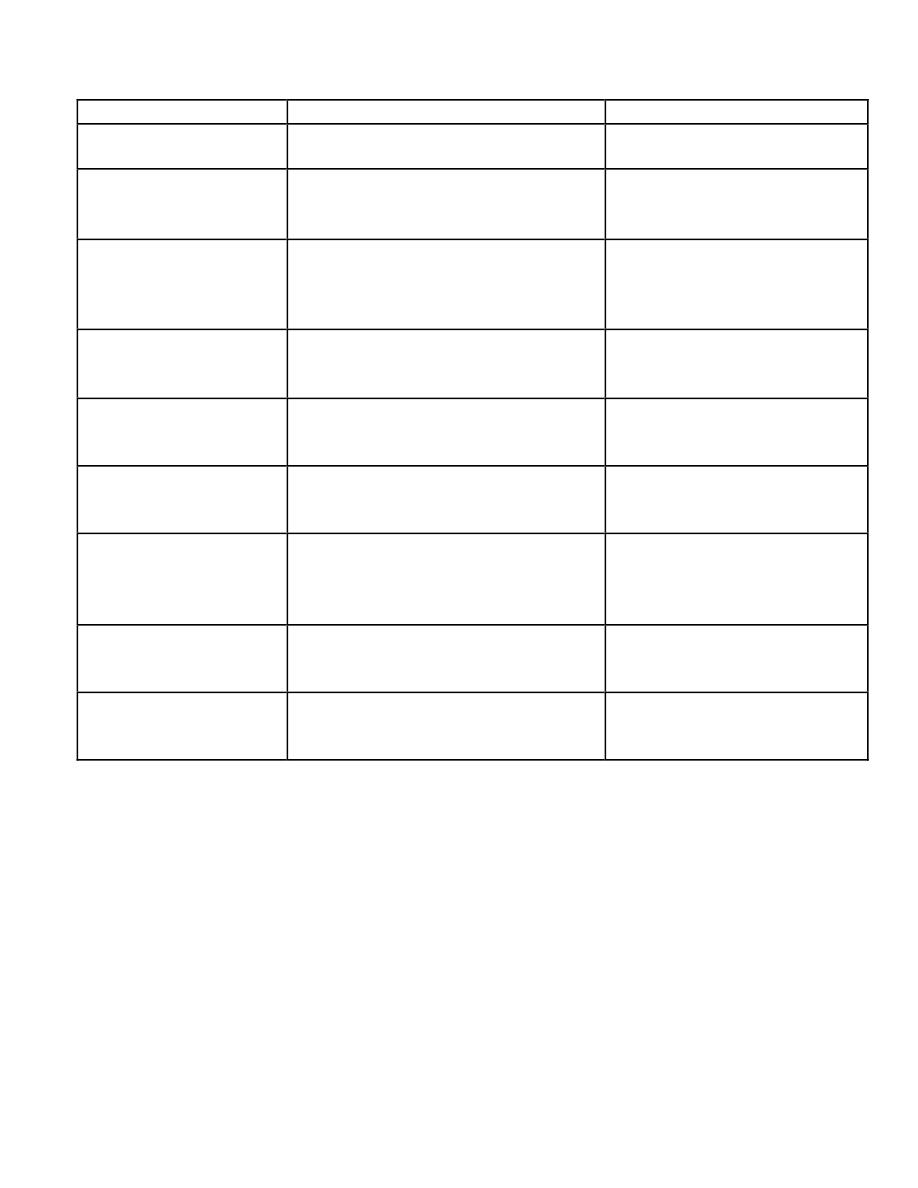
The differences between the irritant and contact dermatitis.
Parameter
Irritant
allegic
People at risk
Everyone
Genetically predisposed
Mechanism of
response
Nonimmunologic; a physical and
chemical alteration of epidermis
Delayed hypersensitivity
reaction
Number of exposures
Few to many; depends on individual's
ability to maintain an effective
epidermal barrier
One or several to cause
sensitization
Nature of substance
Organic solvent, soaps
Low molecular weight hapten
(e.g., metals, formalin, epoxy)
Concentration of
substance required
Usually high
May be very low
Mode of onset
Usually gradual as epidermal barrier
becomes compromised
Once sensitized, usually rapid;
12 to 48 hours after exposure
Distribution
Borders usually indistinct but
localized to the area of irritation
May correspond exactly to
contactant (e.g., watch band,
elastic waistband)
Investigative
procedure
Trial of avoidance
Patch test
Management
Protection and reduced incidence of
exposure
Complete avoidance
Special investigation:
Patch test: helps identify any allergens involved and is particularly useful in dermatitis
of the face, hands and feet.
Patch test.
Patch testing is indicated for cases in which inflammation persists despite avoidance of
the offending agent and appropriate topical therapy. Patch testing is not useful as a diagnostic
test for irritant contact dermatitis because irritant dermatitis is a nonimmunologically mediated
inflammatory reaction.
There are two type of patch test administration:
1- TRUE test
2- Finn test.

Type of patch test
Open patch test.
Use test.
Closed patch test.
Photopatch test.
Interpretation of patch test:
NT Not tested.
0 No reaction.
± Doubtful reaction (minimal erythema).
+ Weak reaction (erythematous and maybe papular).
+ + Strong reaction (erythematous and oedematous or vesicular)
+ + + Extreme reaction (erythematous and bullous).
IR Irritant reaction (variable, but often sharply circumscribed, with a glazed appearance
and increased skin markings).
Treatment:
Elimination and avoidance of allergens and irritants are useful although prevention is the
ideal.
Antihistamines, topical (or systemic if severe)
Drying agents in wet dermatitis (acute).
Topical anti-inflammatory (corticosteroid , tacrolimus).
System anti-inflammatory corticosteroids.
Seborrhoea dermatitis SD
Seborrheic dermatitis is a common, chronic papulosquamous dermatosis that is usually
easily recognized. It affects infants and adults and is often associated with increased sebum
production (seborrhea) of the scalp and the sebaceous follicle–rich areas of the face and trunk.
The affected skin is pink, edematous, and covered with yellow-brown scales and crusts. The
disease has a wide range from mild to severe, including psoriasiform or pityriasiform patterns
and erythroderma.
Incidence
Seborrheic dermatitis has two age peaks, one in infancy within the first 3 months of life
and the second around the fourth to the seventh decade of life. The disease in adults is believed
to be more common than psoriasis, for example, affecting at least 2 to 5 percent of the
population. Men are affected more often than women in all age groups.
Etiology and Pathogenesis
Seborrhea
The disease is associated with oily-looking skin (seborrhea), although increased sebum
production cannot always be detected in these patients.

Microbial Effects
The microbial agents involving in the etiology of seborrhoeic dermatitis include
bacteria, yeasts, or both. This hypothesis has remained unsupported.
In infancy, Candida albicans is often found in involved skin lesions and in stool
specimens. Aerobic bacteria were recovered from the scalp of patients with seborrheic
dermatitis. The lipophilic yeast Pityrosporum is abundant in affected skin.
Drugs
Several drugs have been reported to produce seborrheic dermatitis–like lesions,
including arsenic, gold, methyldopa, cimetidine, and neuroleptics.
Neurotransmitter abnormalities
Seborrheic dermatitis is often associated with a variety of neurologic abnormalities,
pointing to a possible influence of the nervous system. These neurologic conditions include
postencephalitic, parkinsonism, epilepsy, supraorbital injury, facial paralysis, poliomyelitis,
syringomyelia, and quadriplegia.
Physical factors
Seborrheic dermatitis of the face was observed in patients receiving PUVA therapy for
psoriasis and occurred within a few days to 2 weeks after the beginning of treatment .
Nutritional Disorders
Zinc deficiency in patients with acrodermatitis enteropathica and acrodermatitis
enteropathica–like conditions may be accompanied by dermatitis mimicking seborrheic
dermatitis of the face. Seborrheic dermatitis, however, is not associated with zinc deficiency
nor does it respond to supplementary zinc therapy. Biotin deficiency and abnormal metabolism
of essential fatty acids. have been proposed as possible mechanisms.
Immunological
Increased incidence in immunocompromised patients.
Clinical presentation
Common in infants (“cradle cap”) presented as thick scally scalp with or without other
manifestation of SD.
In adults, can cause dandruff (pityriasis sicca)
Scalp and facial involvement: excessive dandruff, with an itchy scaly erythematous
eruption affecting the sides of the nose, scalp margin, eyebrows and ears. Blepharitis may
occur. Most common in young adult males.
Petaloid: a dry scaly eczema over the presternal area.
Pityrosporum folliculitis: an erythematous follicular eruption with papules or pustules
over the back.
Flexural: involvement of the axillae, groins and sub-mammary areas.
Erythroderma Desquamativum (Leiner's Disease)
This complication of seborrheic
dermatitis in infants (dermatitis seborrhoides infantum) . There is usually a sudden confluence

of lesions leading to a universal scaling redness of the skin (erythroderma). The young patients
are severely ill with anemia, diarrhea, and vomiting.
Management
Therapy is suppressive rather than curative and patients should be told this.
Topical
Topical antifungal shampoo (ketoconazole), zinc pyrithione, selenium sulfide or tar.
Topical antifungal imidazole group .
Topical anti-inflammatory agents (corticosteroid cream, topical immunomodulatory agent
pimecrolimus or tacrolimus.
Rare cases can get benefit from UV light.
Topical lithium succinate cream.
Systemic
Steroid , antihistamine, antifungal, even antiandrogens.
Asteatotic Eczema
Synonyms:
Xerosis, dermatitis sicca, eczema craquelé, winter itch.
Definition:
Dermatitis secondary to superficial cracks in epidermis as a result of dryness
and reduced lipids.
Epidemiology:
Common problem, more likely in elderly and those with atopic dermatitis
or ichthyosis vulgaris.
Etiology :
Age : more with age (elderly).
Seasonal : during winter time.
Excessive washing&bathing.
Used diuretics
Sjogrens syndrome , myxedema, reflex sympathetic dystrophy.
Clinical features: Initially dry skin and pruritus. Sometimes erythematous cracks in skin
The lesions have the appearance of a cracked river bed with poorly defined borders. The
lesions is located predominantly on extensor limbs and trunk.
Diagnostic approach:
Clinical diagnosis with typical history.
Differential diagnosis:
Atopic dermatitis, various forms of ichthyosis, especially
acquired ichthyosis.
Therapy:
Avoidance of frequent baths or showers; use a synthetic detergent instead of soap;
regular lubrication of skin (lactic acid , urea containing medication), especially after bathing.
Gravitational eczema
Gravittational eczema has replaced stasis dermatitis as a more appropriate term for the
eczema that can accompany chronic venous hypertension. The disorder is rarely seen prior to
middle age. There is scaling, erythema, pigmentation, and fibrosis with other feature of venous

insufficiency (oedema, red or bluish discoloration, loss of hair, induration, haemosiderin
pigmentation and ulceration) often associated with pruritus. Venous drainage has been
compromised by a number of factors, some of which can be obesity, trauma, venous
thrombosis, or multiple pregnancies. Heredity certainly plays a role by the presence of
incompetent valves allowing back- flow of blood. The condition is common in the wheelchair-
bound patient and in all situations where the muscle pump is not able to function in
assisting blood return.
Treatment:
Local steroids should only be applied to eczematous areas and ulcers should be
avoided. Sensitisation to topical antibiotics (neomycin) and preservatives . is common in this
form of eczema. Associated peripheral oedema should be eliminated by elevation of the leg and
graded compression bandages.
Discoid (nummular) eczema
Definition:
Sharply circumscribed plaques of dermatitis; nummular means “coin shaped”.
Pathogenesis: Probably reflects atopic dermatitis, xerosis. More common in those
with poor personal hygiene and in alcoholic patients .
Clinical features:
0.5-2cm but can reach to 5 cm plaques
Types there are two type
Wet presented as erythematous papules with vesicles and crusts.
Dry presented as dull erythematous sally area .
The condition started usually as single plaque , severely itching uasully on extremeties last for
several months before disseminated to the other area of the body.
Differential diagnosis:
Atopic dermatitis, psoriasis, tinea corporis, impetigo, seborrheic
dermatitis.
Therapy:
Topical corticosteroids super potent (with occlusion), perhaps combined with
topical antibiotics or tar.
Systemic antihistamine (hydroxyzine),
Systemic steroid (oral, interalesional)
Phototoxic & Photoallergic dermatitis
Photosensitizes : chemical compound with molecular weigh less than 500 dalton which
after absorption (suitable) radiating energy result in excitation of these compounds. So after
retained these compounds to the lower energy state gives off energy through fluorescence,
phosphorescence, charge transfer, heat, or formation of free radicals(most important). Each
photosensitizer substances absorbed only specific wave length (action spectrum)
Photosensivity reaction occur when there is sufficient concentration of photosensitizer
substancesin skin exposed to the sufficient intensity and duration of light in the action spectrum
of that photosensitizer.
Phototoxic Photoallergic
More common less common
In any person can Occur only in genetically susceptible
Immediate or within 48h of exposure delayed to 1-2 weeks of exposure
High dose of photosensitizer lower dose needed
Action spectrum UVA UVA and even visible light
Histopathology as burn as contact dermatitis
Photopatch test –ve +ve
Example of
Phototoxic: tar, amiodarone, furosemide, NSAIDs (especially piroxicam, diclofenac),
psoralens, phenothiazines, tetracyclines (especially doxycycline).
Photoallergic: Benzodiazepines, nalidixic acid, NSAIDs, phenothiazines, sulfonamides,
sulfonylureas, thiazides.
Exposure to plant sap or juice plus sun exposure leads to streaking of erythrma, and
even vesicles or bolus dermatosis, which end usually with hyperpigmwentation known as
phytophotodermatitis.in children commnly found around the mouth, while in the adult on the
hands.
Berloque dermatitis is caused by using perfumes or after shave lotions containing
bergamot oil; typical picture is streaked hyperpigmented rash on side of neck where perfume is
often applied. Acute reaction often overlooked; only pigmentary changes noted.
Therapy:
Same as for allergic and toxic contact dermatitis
Topical anti-inflammatory (steroid, calcinurin inhibitors)
Antihistamine
Avoidance of sun exposure
Regular use of sun screan
Lichen simplex chronicus
Lichen simplex chronicus is a chronic dermatologic disorder felt to be precipitated by
emotional factors. It is a localized disorder characterized by intense pruritus, which leads to a
very thickened, lichenified area because of scratching. The lichenified areas are themselves
intensely pruritic, which perpetuates
)
ﯾ
ﺪ
ﯾ
ﻢ
(
the cycle. Favourite areas are the nape of the neck
in women, the legs in men, and the anogenital area in both sexes. Lesions may resolve with
treatment but tend to recur either in the same place or elsewhere.
Treatment
Breaking the cycle of scratching is the central goal of treatment
Tranquillizers are often disappointing.
Antihistamine
Topical steroid
Interalesional steroid
Pompholyx (dyshydrotic eczema)

Recurrent deep vesicles and bullae occur on the palms, palmar surface of the fingers
and soles, and are extremely itchy. This form of eczema can occur in atopic eczema and in
irritant and contact allergic dermatitis. It can be provoked by heat, stress and nickel ingestion in
a nickel-sensitive patient but is often idiopathic.
Treatment:
Aluminium acetate or potassium permanganate soaks in wet type (acute)
Topical steroid (under occlusion) usually not effective
Topical PUVA
Systemic steroid usually needed
Antihistamine for severe itching
Napkin (diaper) dermatitis
The most common type of napkin eruption is irritant in origin, and is aggravated by the
use of waterproof plastic pants. The mixture of faecal enzymes and ammonia produced by urea-
splitting bacteria, if allowed to remain in prolonged contact with the skin, leads to a severe
reaction. The overgrowth of yeasts is another aggravating factor.
Differential diagnosis
The sparing of the folds helps to separate this condition from infantile seborrhoeic
eczema and candidiasis.
Treatment
It is never easy to keep this area clean and dry, but this is the basis of all treatment.
Theoretically, the child should be allowed to be free of napkins as much as possible but this
may lead to a messy nightmare. The area should be cleaned at each nappy change with aqueous
cream and water. Protective ointments, e.g. zinc and castor oil ointment, or silicone protective
ointments, are often useful as are topical imidazole preparations that stop yeast growth. Potent
steroids should be avoided but combinations of hydrocortisone with antifungals or topical
antibiotics