Urinary system imaging
lecture (2)
5
TH
stage
By
Dr. Firas Abdullah
Thiqar college of medicine
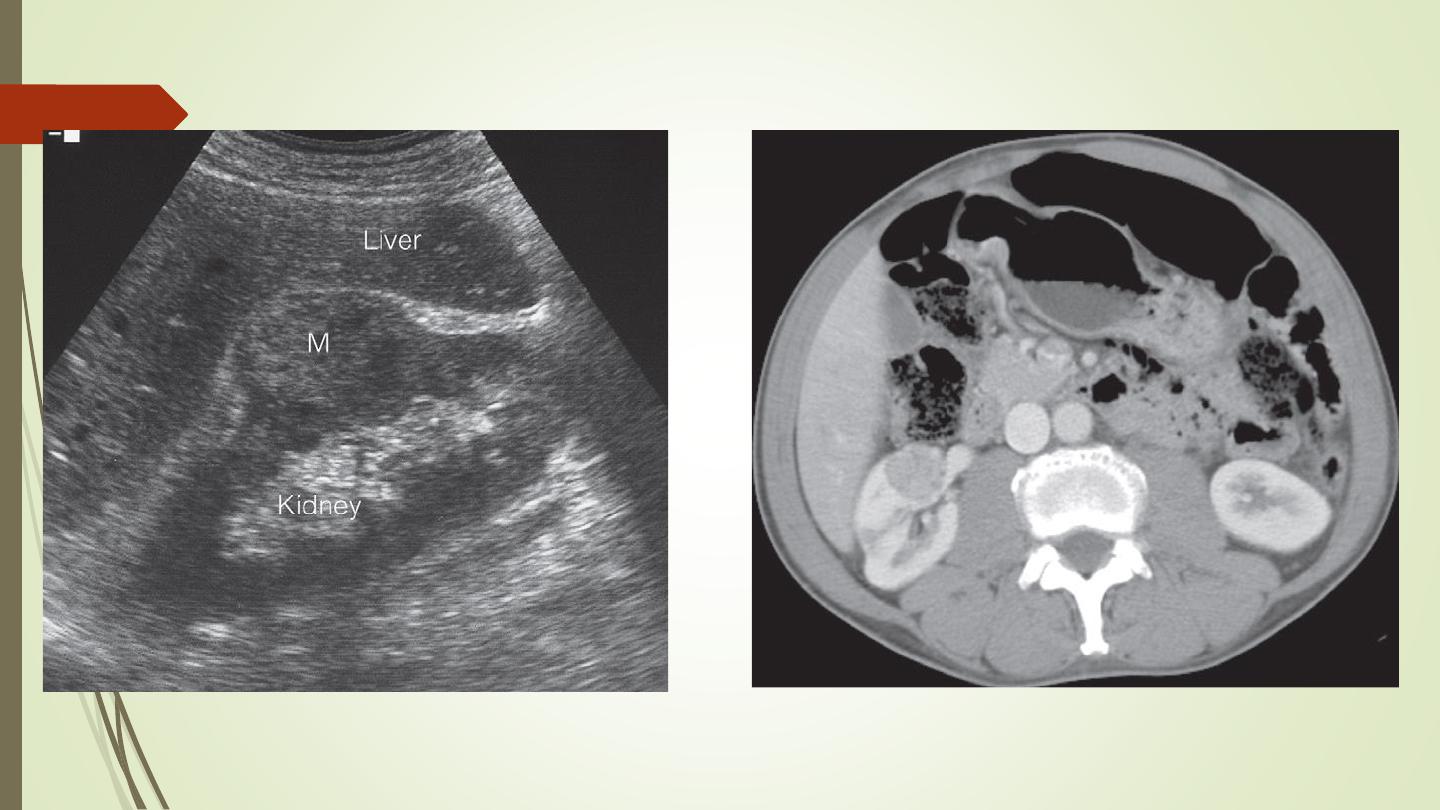
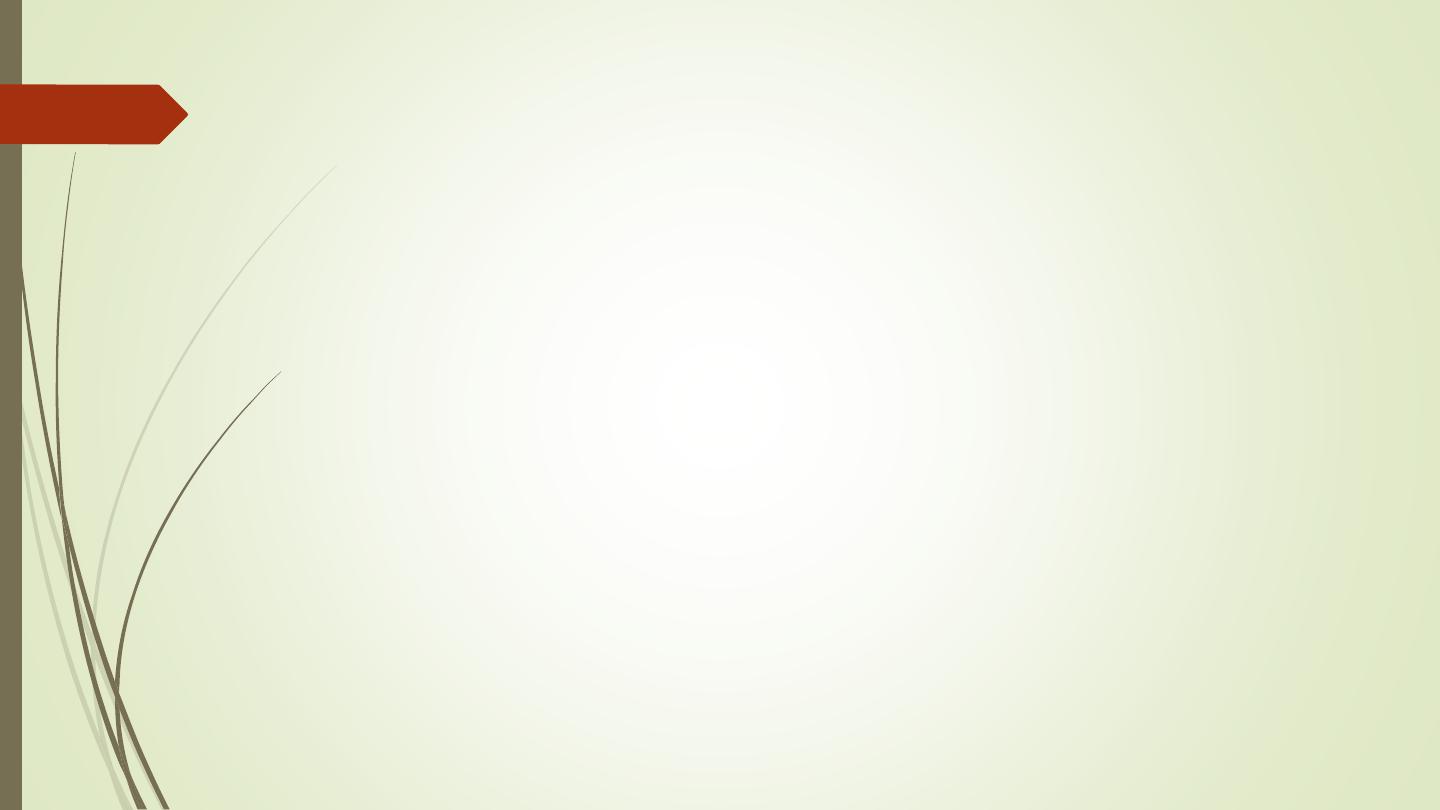
Renal cell carcinomas
Spherical and often lobulated, usually isodense to
renal parenchyma.
Focal necrotic areas may result in areas of low
density, and stippled calcification may be present
in the interior of the mass.
Renal cell carcinomas enhance, but not to the
same degree as the normal renal parenchyma.
The enhancement is inhomogeneous.
Check LN, liver, adrenal, pancreas, bone, renal
vein and IVC
Acute infections of the upper urinary tracts
Most patients with acute urinary tract infection do not
require urgent imaging investigations.
In patients presenting with signs of infection associated
with pain, particularly if the symptoms are not settling
with antibiotics, ultrasound and plain films may
diagnose underlying stones, obstruction or abscess
formation
Investigation of the renal tract is indicated in all
children with a confirmed urinary tract infection.
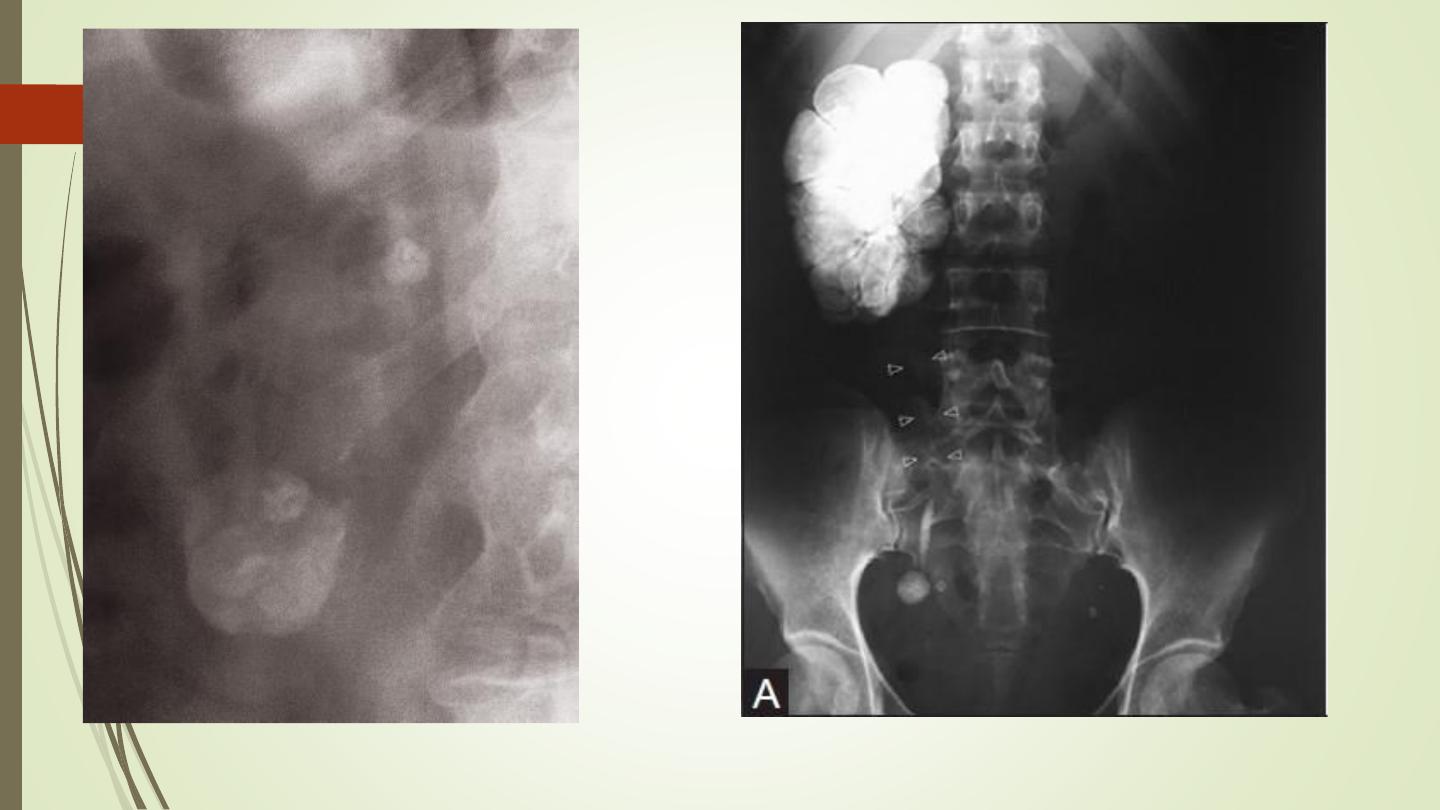
Urinary tuberculosis
Calcification is common. Usually, there are one or more foci of
irregular calcification, but in advanced cases show
(autonephrectomy). Calcification implies healing but does not
mean that the disease is inactive.
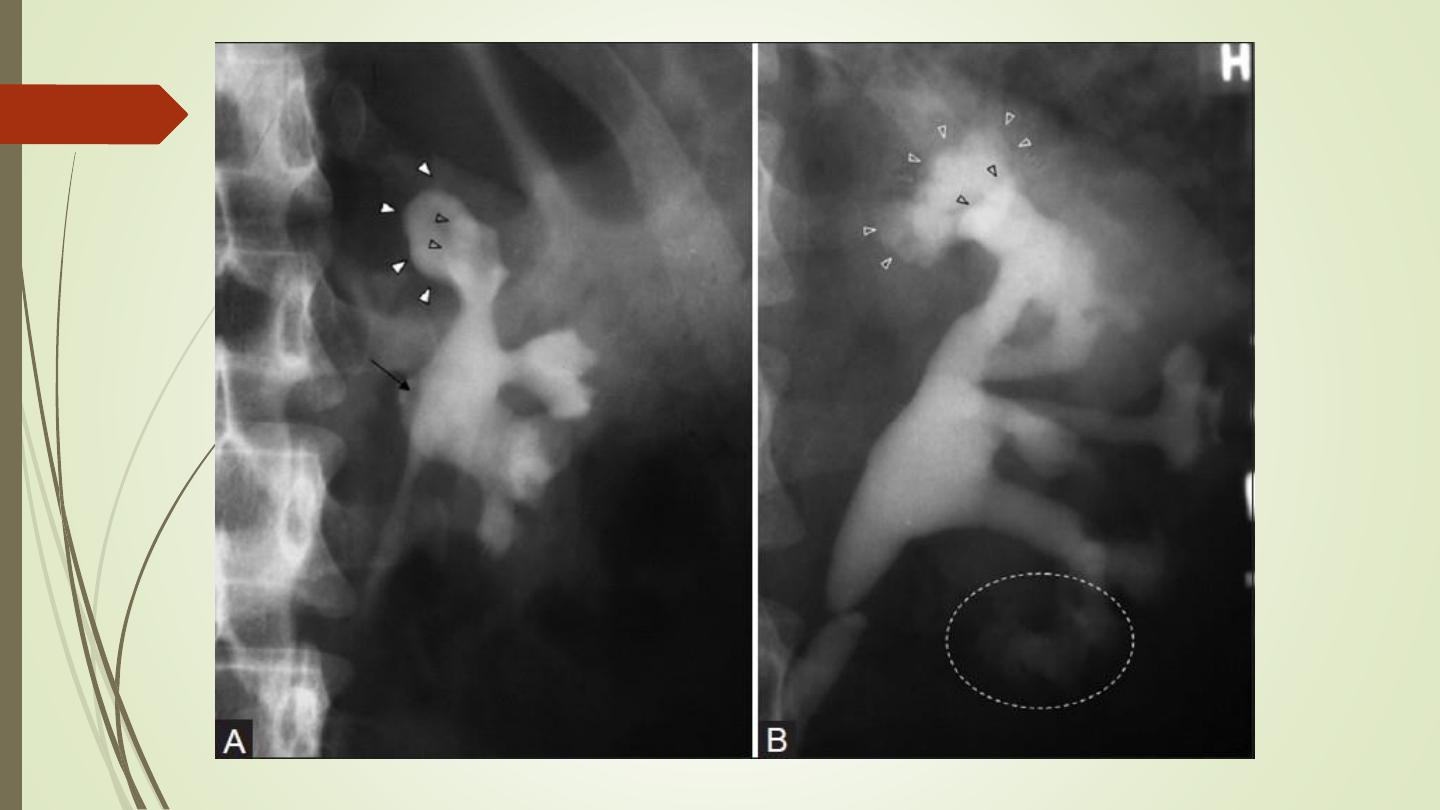
The earliest change on the post contrast films is irregularity of a
calix. Later, a definite contrast-filled cavity may be seen adjacent
to the calyx.
Strictures of any portion of the pelvicaliceal system or ureter may
occur, producing dilatation of one or more calices. The multiplicity
of strictures is an important diagnostic feature.
If the bladder is involved, the wall is irregular because of
inflammatory edema; advanced disease causes fibrosis resulting in
a thick-walled small volume bladder.
Multiple strictures may be seen in the urethra.
Chronic pyelonephritis (reflux nephropathy)
Local reduction in renal parenchymal width (scar
formation). The upper and lower calices are the most
susceptible to damage from reflux.
Dilatation of the calices in the scarred areas
Overall reduction in renal size partly from loss of renal
parenchyma.
Dilatation of the affected collecting system
Vesicoureteric reflux may be demonstrated at
micturating (voiding) cystography.

Renal trauma
Computed tomography is the preferred investigation,
which can:
➢
Demonstrate the presence or absence of perfusion to the
injured kidney.
➢
Ensure that the opposite kidney is normal.
➢
Show the extent of renal parenchymal damage.
➢
Demonstrate injuries to other organs
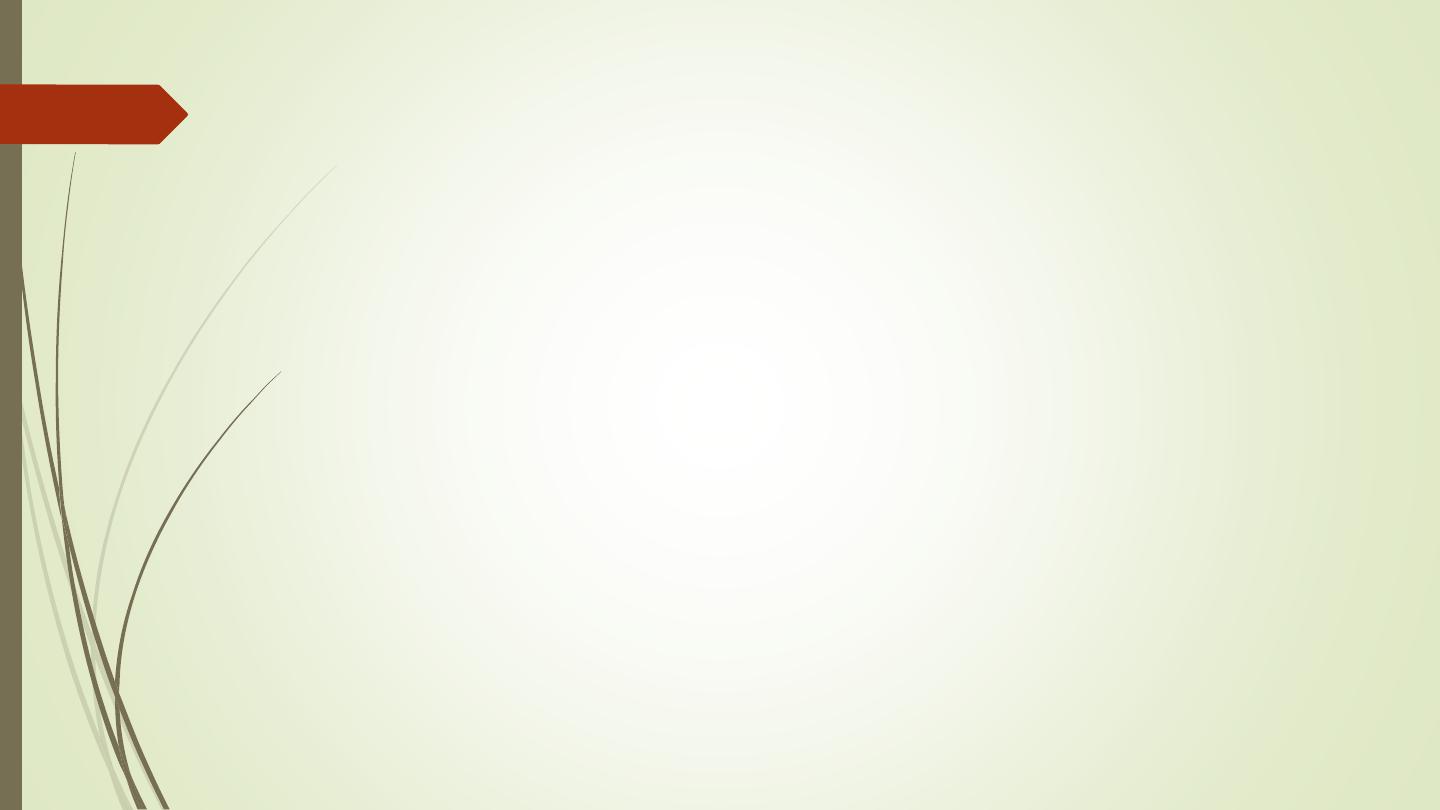
Congenital anomalies of the urinary tract
Bifid collecting systems: most frequent congenital
variation
The two ureters may join at any level between the renal
hilum and the bladder or may insert separately into the
bladder
The upper moiety ureter may drain outside the bladder,
e.g. into the vagina or urethra, producing incontinence
if the opening is beyond the urethral sphincter.
The lower moiety ureter may show reflux. And inserted
proximal to upper moiety ureter.
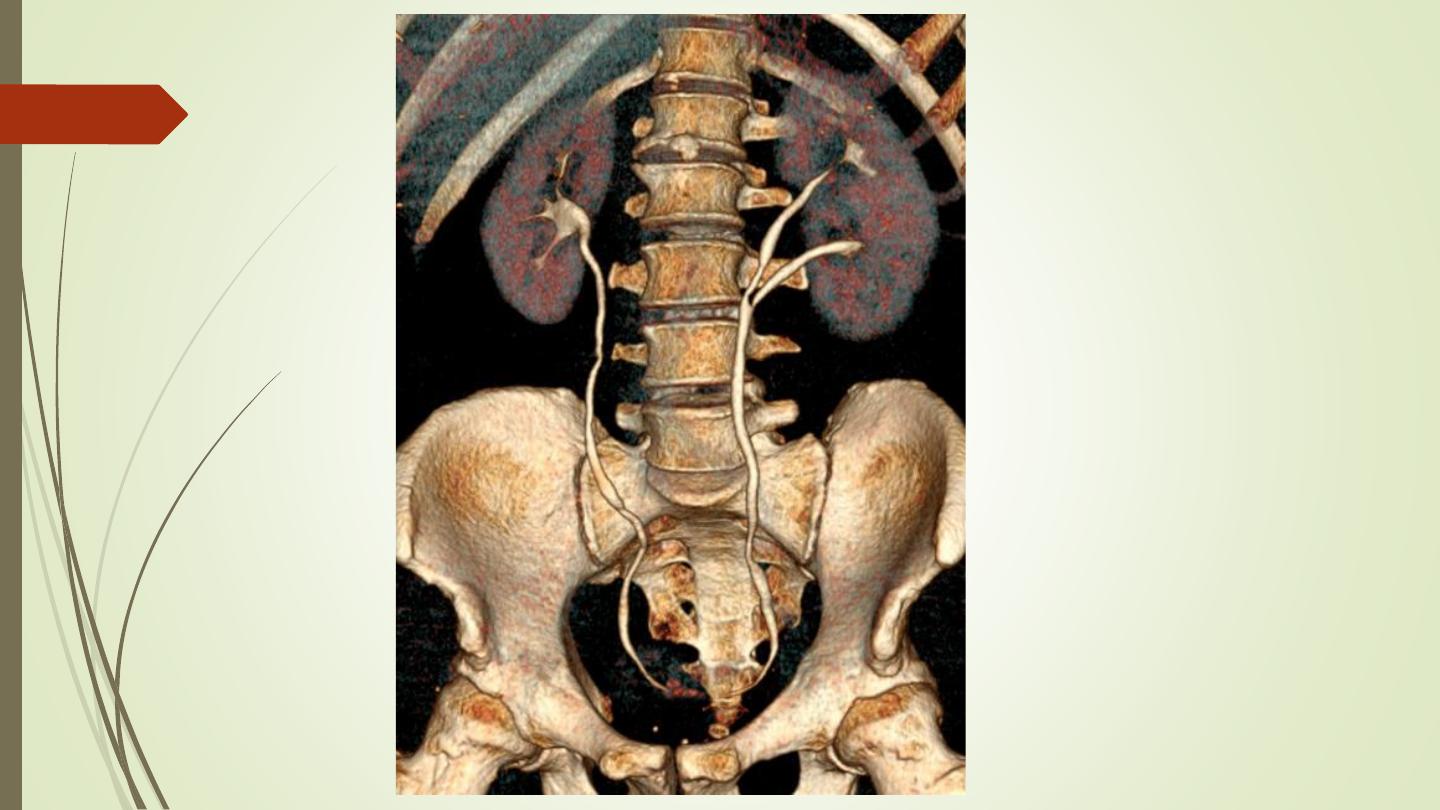
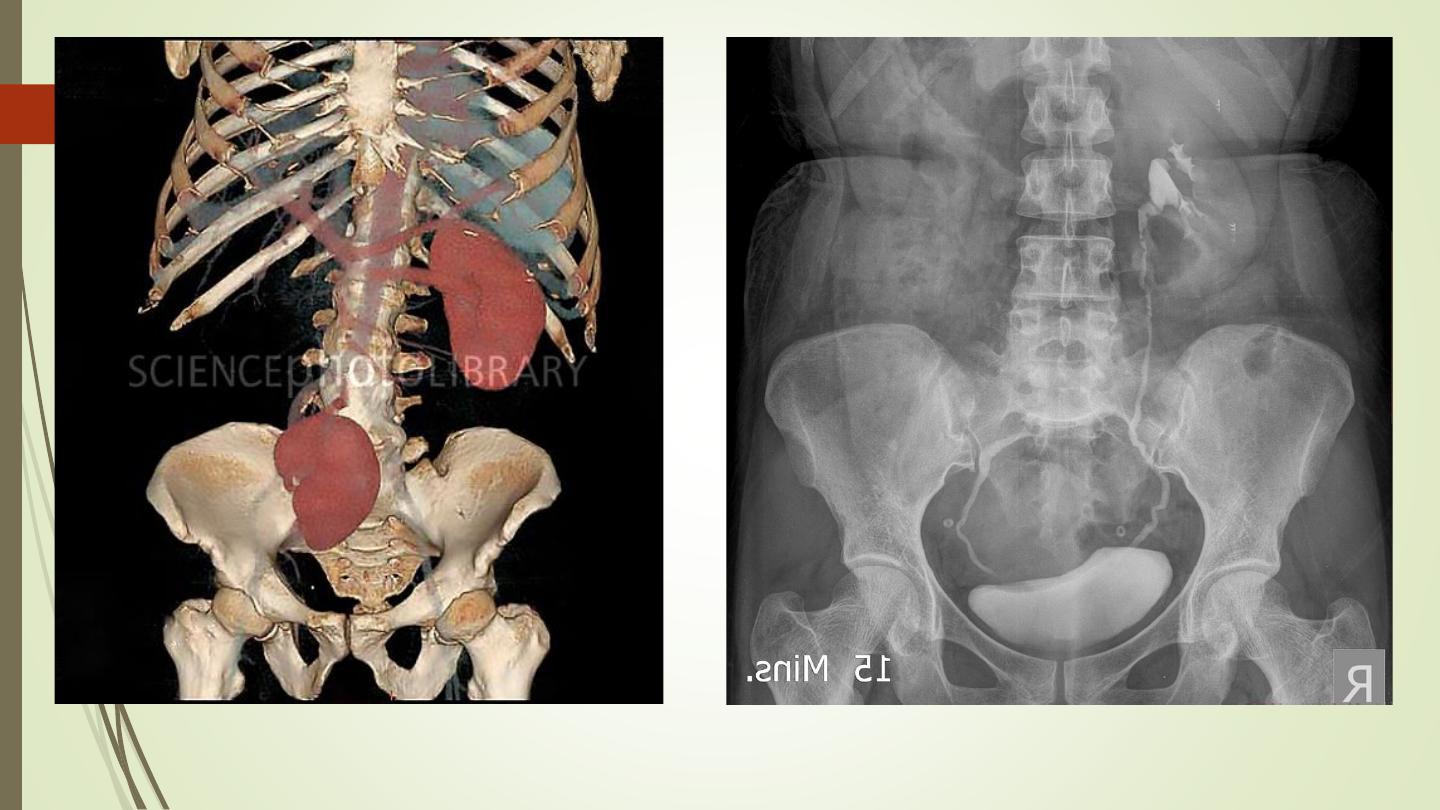
Ectopic kidney:
During fetal development the kidneys ascend within the
abdomen.
An ectopic kidney results if this ascent is halted.
They are usually in the lower abdomen and rotated so that the
pelvis of the kidney points forward.
The ureter is short and travels directly to the bladder.
Chronic pyelonephritis, hydronephrosis, and calculi are all more
common in ectopic kidneys
But usually it is an incidental finding.
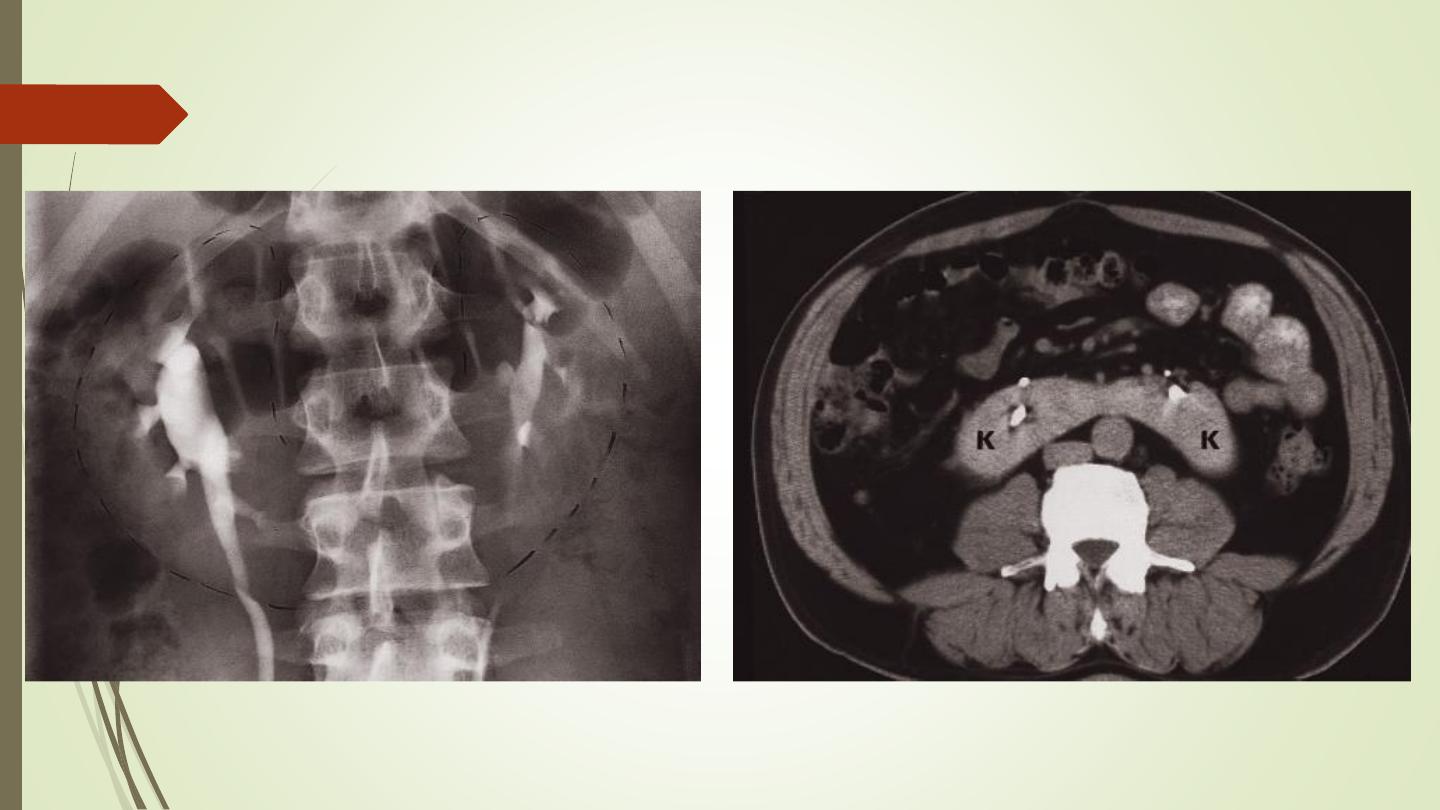
Horseshoe kidney
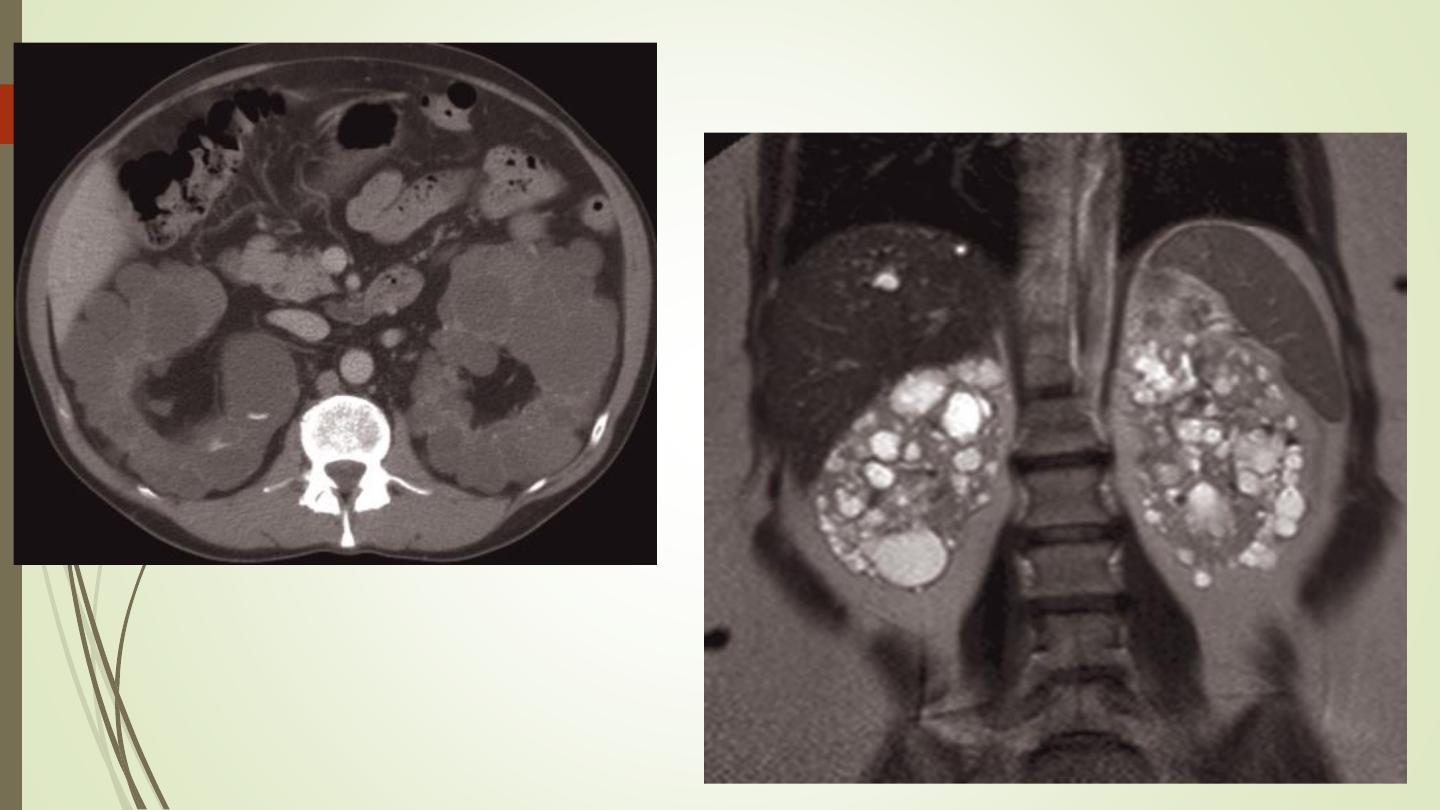
Autosomal dominant polycystic kidney disease.
This is a familial disorder which although inherited, usually
presents between the ages of 35 and 55 years with
hypertension, renal failure or hematuria
The diagnosis is readily made at ultrasound, as well as on CT
The liver and pancreas may also contain cysts and these organs
are routinely examined in such patients
Ultrasound screening is usually offered at the age of 18 to the
offspring of those with the disease
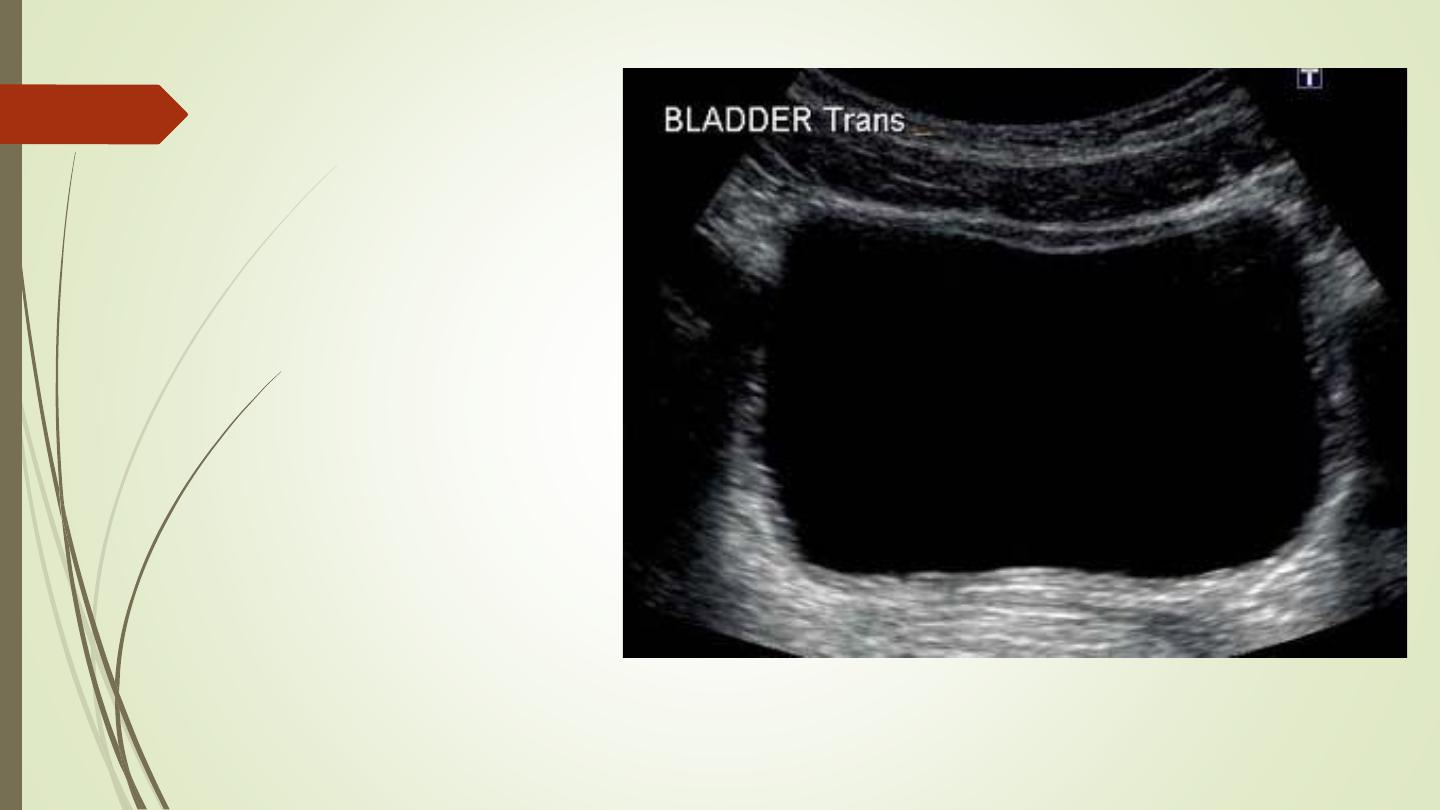
Urinary bladder
normal wall thickness when distended should
be less than 3 mm.
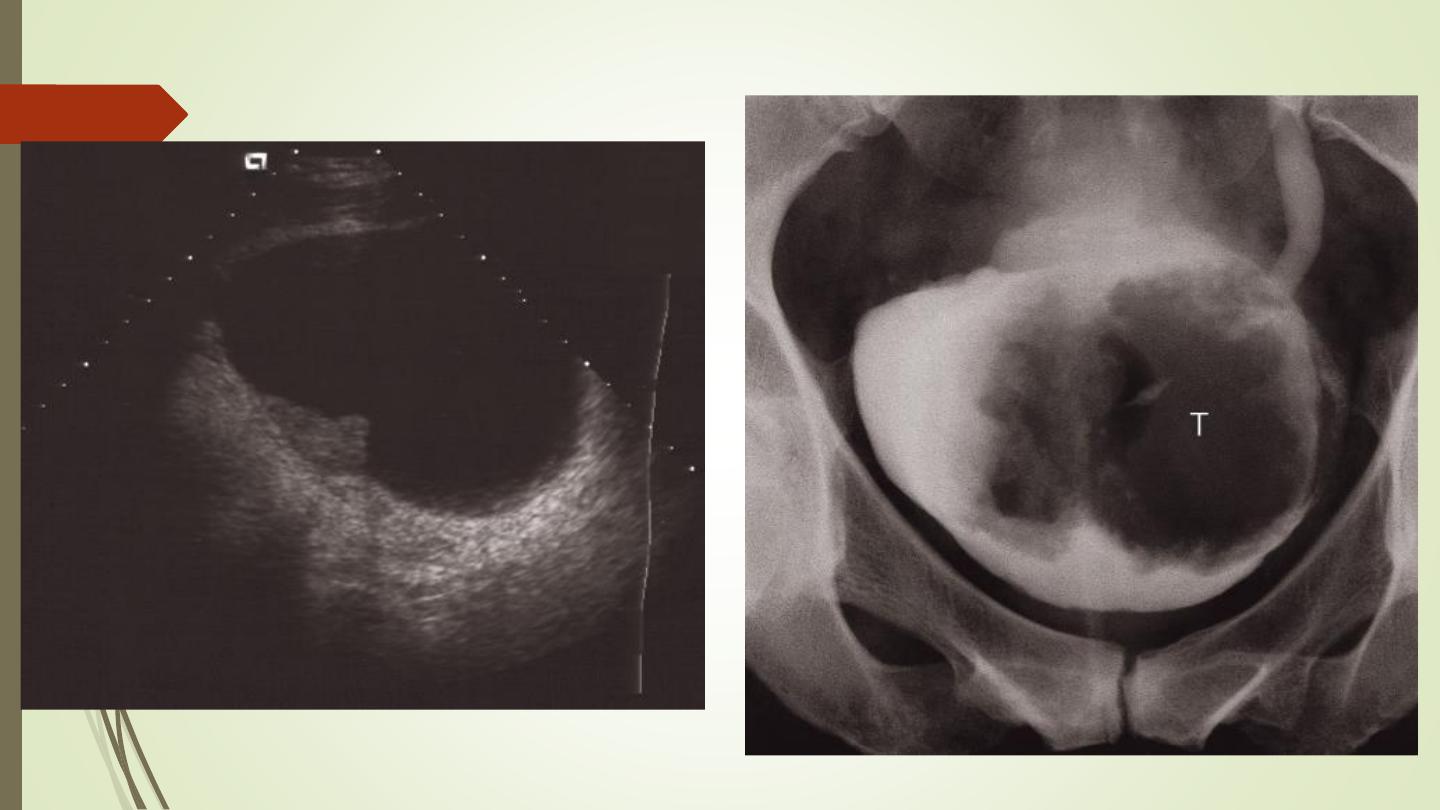
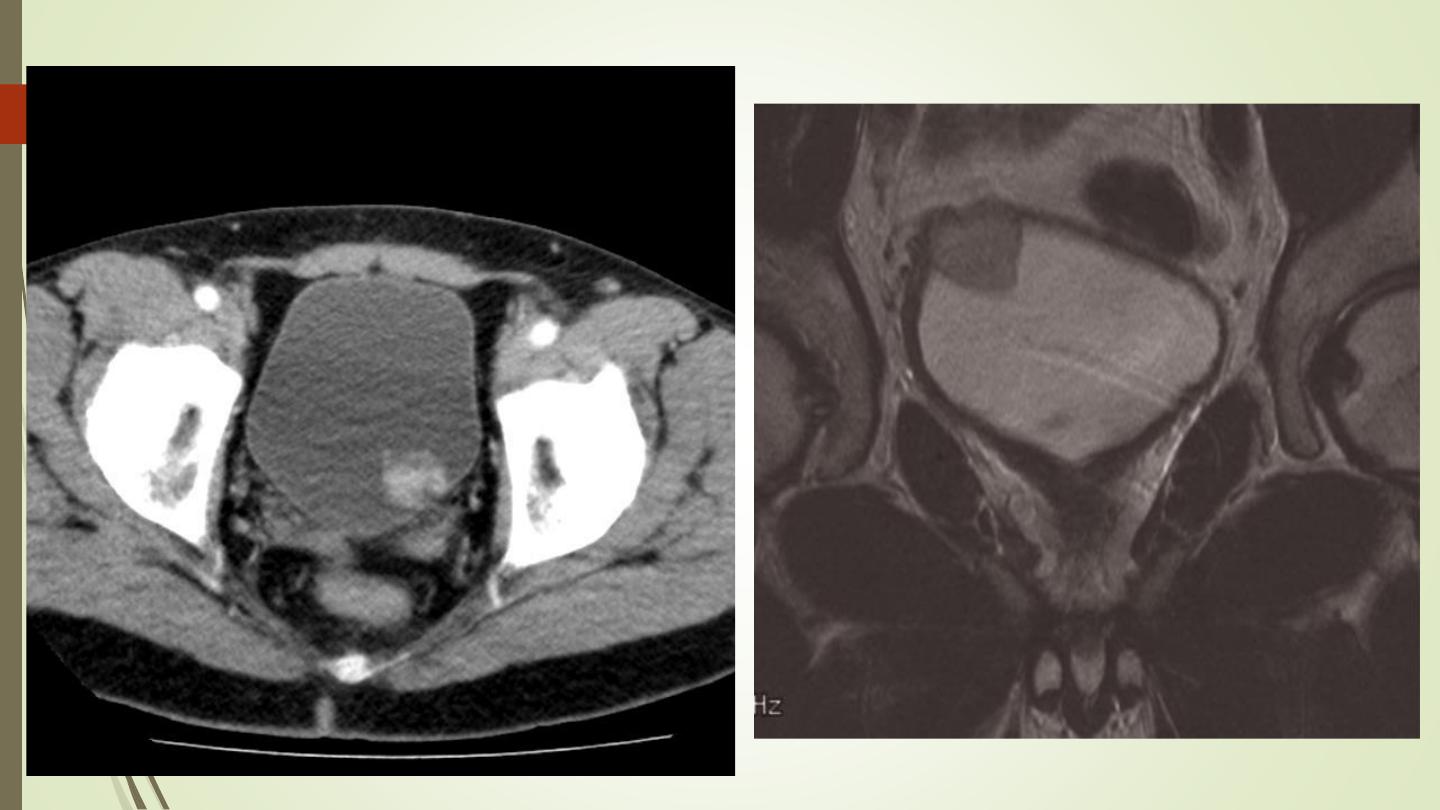
Bladder tumours
The bladder is the most frequent site for neoplasms in the
urinary tract.
Almost all are transitional cell carcinoma
US and IVU
the roles of CT and MRI are to stage the tumour, assessing
the depth of invasion within the muscle, can determine
spread of tumour beyond the bladder wall and assess
lymph node involvement
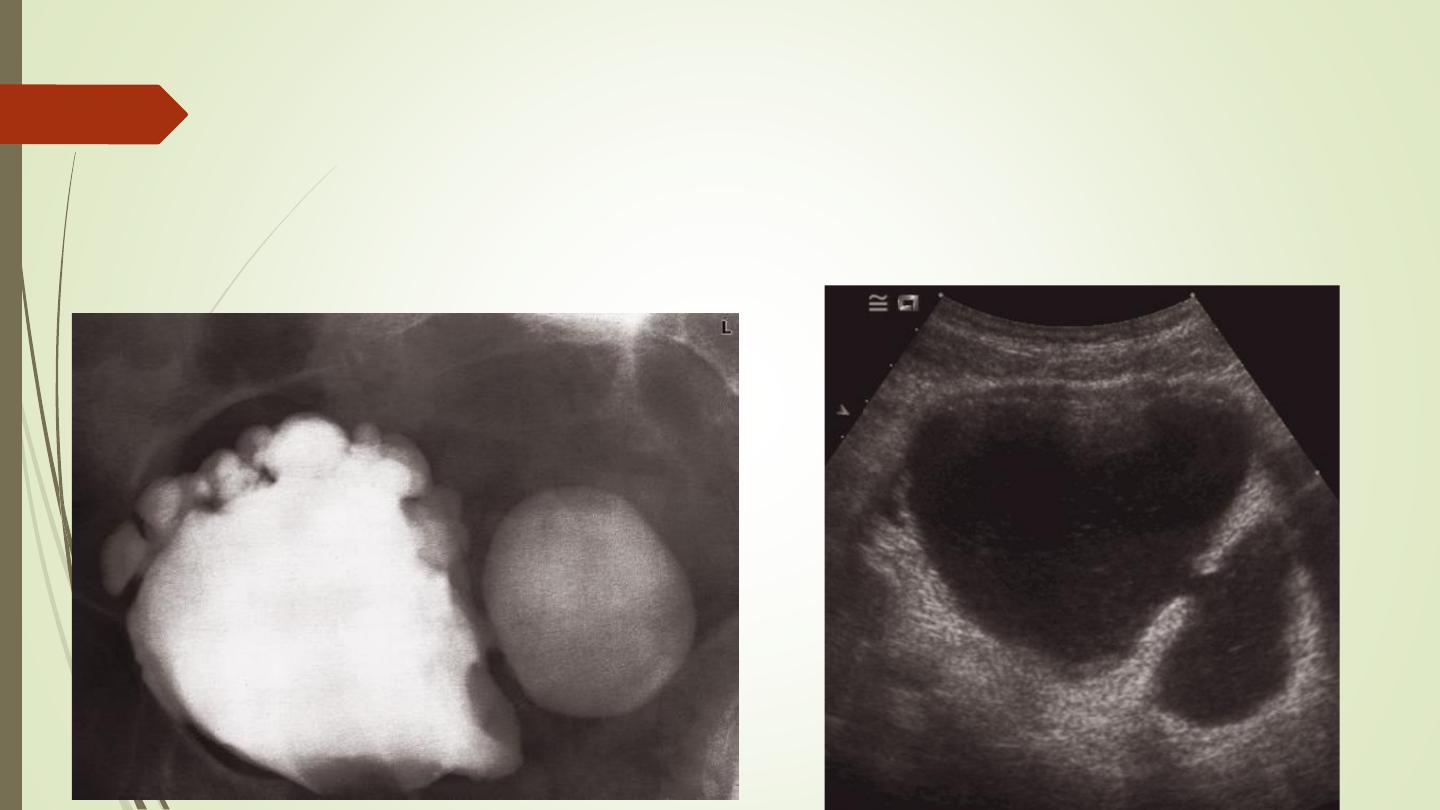
Bladder diverticula
Bladder diverticula may be congenital in origin but are
usually the consequence of chronic obstruction to
bladder
Neurogenic bladder
There are two basic types of neurogenic bladder:
❖
The large atonic smooth-walled bladder with poor or
absent contractions and a large residual volume
❖
The hypertrophic type, which can be regarded as
neurologically induced bladder outflow obstruction
(Christmas tree bladder)

Hypertrophic Neurogenic bladder
Christmas tree bladder
Prostate and urethra
:
Benign prostatic hypertrophy involves the median zone
Prostatic CA involve the peripheral zone
Bladder outflow obstruction
The most frequent cause of bladder outflow obstruction is
enlargement of the prostate. Other causes include
bladder tumours, urethral strictures and, in male infants or
boys, posterior urethral valves
➢
Increased trabeculation and thickness of the bladder wall,
often with diverticula formation.
➢
Residual urine in the bladder after micturition.
➢
Dilatation of the collecting systems.
Urethral stricture:
Post-traumatic strictures are usually in the posterior
urethra – the most vulnerable portion of the urethra to
external trauma. Such strictures are usually smooth in
outline and relatively short.
Inflammatory strictures, which are usually gonococcal in
origin, may be seen in any portion of the urethra, but are
usually found in the anterior urethra. Usually long
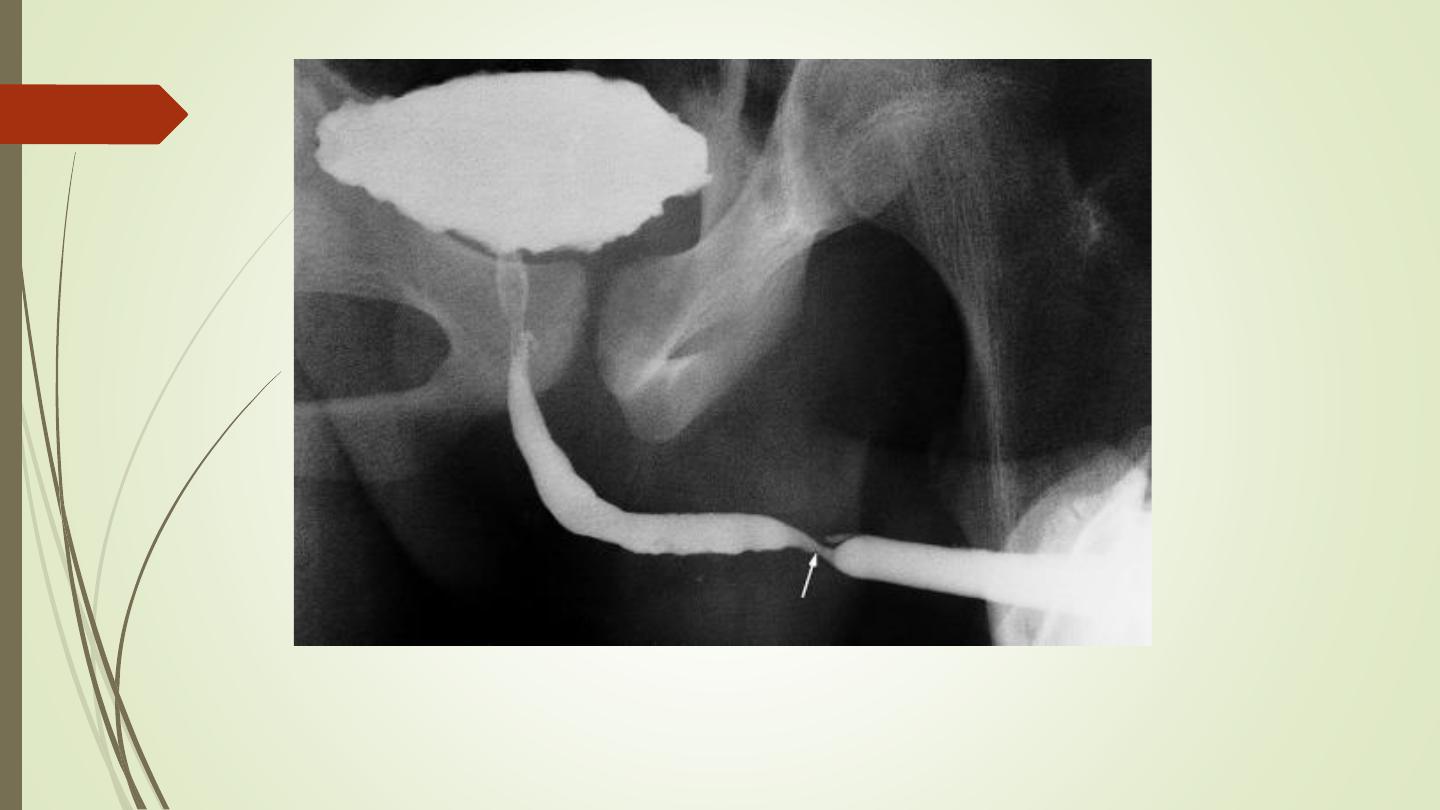
Ascending urethrogram

Best Wishes