



Disease of neuromuscular junction
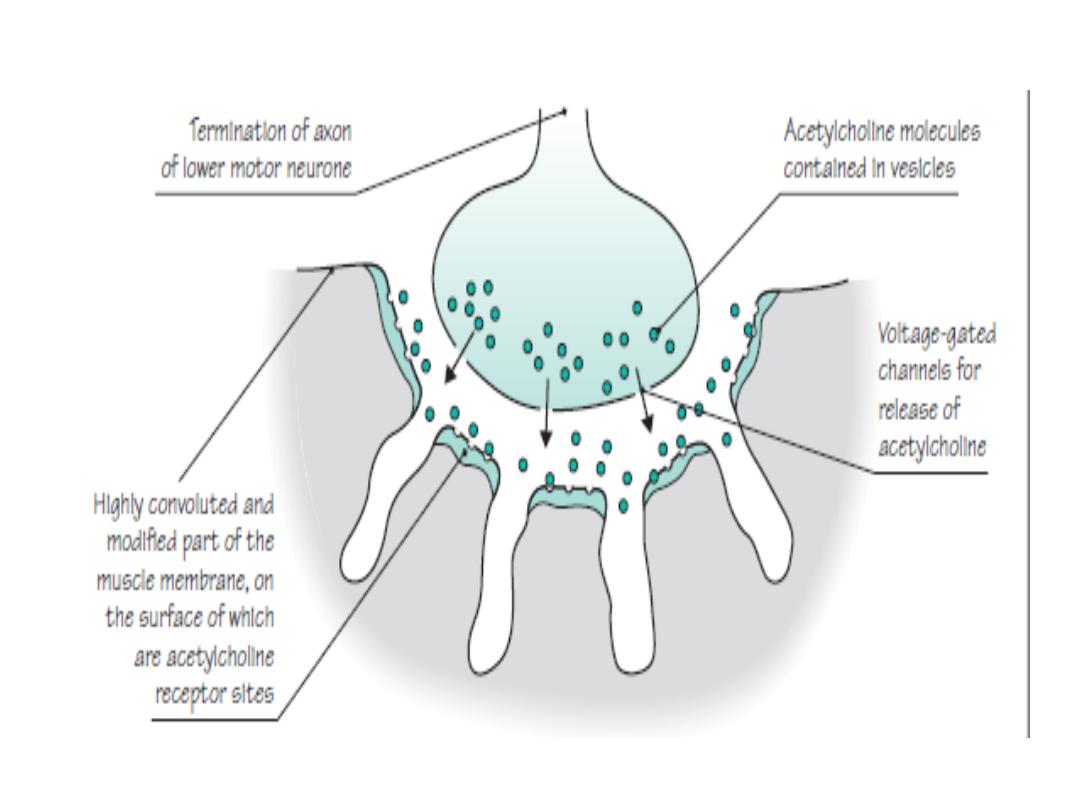
The Neuromuscular Junction is composed of :
✓ Presynaptic membrane
✓ Postsynaptic membrane
✓ Synaptic cleft
▪ Presynaptic membrane contains vesicles with Acetylcholine (ACh) which
are released into synaptic cleft in a calcium dependent manner
▪ ACh attached to ACh receptors (AChR) on postsynaptic membrane
▪ The Acetylcholine receptor (Ach R) is a sodium channel that opens when
bound by Ach :
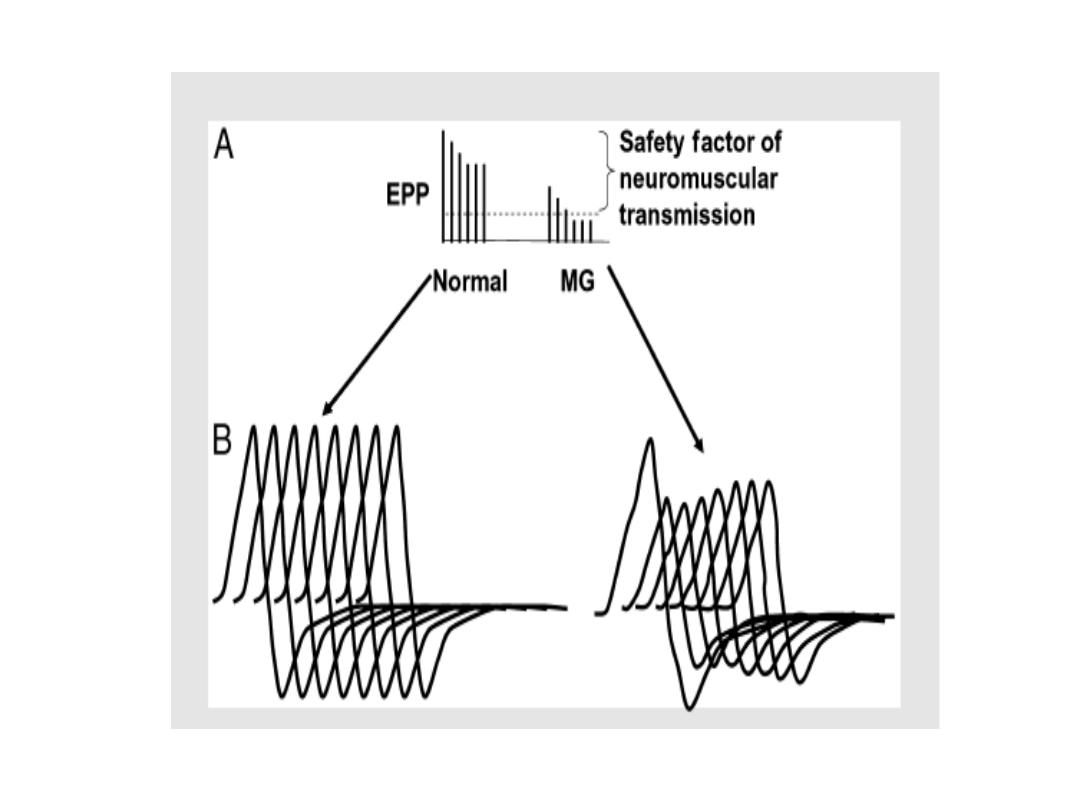
There is a partial depolarization of the postsynaptic membrane and this causes
an excitatory postsynaptic potential (EPSP)
If enough sodium channels open and a threshold potential is reached" a muscle
action potential is generated in the postsynaptic membrane
• Myasthenia gravis
• It is an acquired autoimmune disorder, clinically characterized by
weakness of skeletal muscles and
fatigability
on exertion.
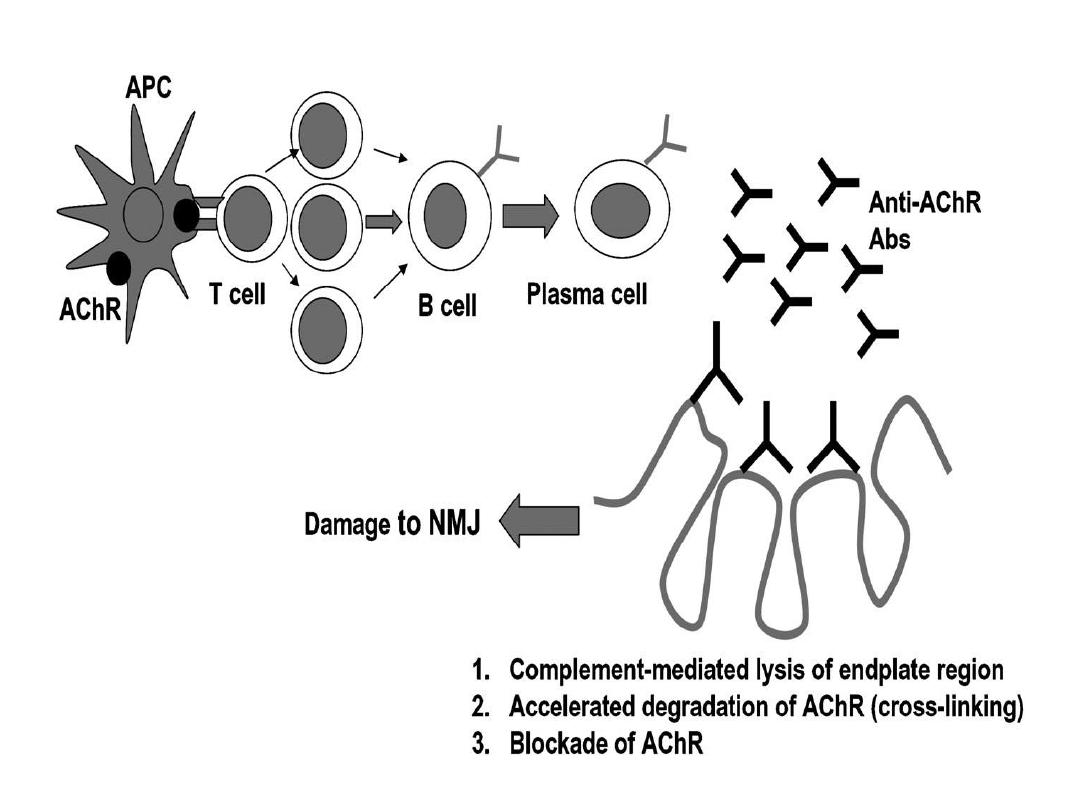
• pathophysiology
• In MG, antibodies(lgG) are directed toward the acetylcholine
Nicotinic receptors at the neuromuscular junction of skeletal
muscles resulting in;
•
Decreased number of receptors at the motor end-plate
•
Reduced postsynaptic membrane folds
• Widened synaptic cleft
• Role of thymus
• 75 % of cases of MG the thymus was abnormal
• 65% had thymus hyperplasia
• 10 % had thymoma (rarely in children)
• epidemiology
• MG has two peak onset;
• first at 20-30 years of age, mostly affect Females
• The second at 40-60 years of age, mostly affect males
•
(Overall, female are more frequently affected than male in a ratio of
approximately 3-2
• familial cases are rare.
• Clinical Presentation
(fatigable)
▪ Fluctuating weakness increased by exertion
➢ Weakness increases during the day and improves with
rest
▪ Extraocular muscle weakness
➢ Ptosis is present initially in 50% of patients.
➢ during the active course of disease in 90% of patients
▪ Head extension and flexion weakness
➢ Weakness may be worse in proximal muscles

▪ Ocular muscle weakness
➢ Asymmetric,
usually
affects
more
than
one
extraocular muscle and is not limited to muscles
Innervated by one cranial nerve
➢ Ptosis caused by eyelid weakness
➢ Diplopia is Very common

▪ Bulbar muscle weakness
Palatal muscles
➢ Nasal voice, nasal regurgitation
➢ Chewing may become difficult
➢ Severe jaw weakness may cause jaw to hang open
➢ Swallowing may be difficult and aspiration may
occur with fluids--coughing and choking while
drinking
• Progression of disease
❑Usually spreads from ocular to facial to bulbar to
truncal and limb muscles.
❑Often, symptoms may remain limited to EOM and
eyelid muscles for years
❑The disease remains ocular in 16% of patients.
• Remissions
❑Spontaneous remission rare
❑Most remissions with treatment occur within the first
three years
• Respiratory muscle weakness
▪ weakness of the intercostal muscles and the diaghram
may result in C02 retention due to hypoventilation ,
and may cause a neuromuscular emergency
▪ Weakness of pharyngeal muscles may collapse the
upper airway So Monitor vital capacity is important
• Co-existing autoimmune disease
✓ Hyperthyroidism:- Occurs in 10-15% MG patients,
exophthalmos and tachycardia point to hyperthyroidism
,weakness may not improve with treatment of MG
alone in patients with co-existing hyperthyroidism
✓ Rheumatoid arthritis
✓ Scleroderma
✓ Lupus
❖Note: in MG patients. neurological examination is
normal with only
PROXIMALWEAKNESS
• Differential diagnosis
• Amyotrophic Lateral Sclerosis
• Brain stem gliomas
• Lambert-Eaton"Myasthenic Syndrome
• Thyroid disease
• Botulism
•
Investigation
• Laboratory study
❖Anti-acetylcholine receptor antibody Positive in
74%
▪ 80% in generalized myasthenia gravis .
▪ 50% of patients with pure ocular myasthenia
❖Antistriated muscle AB
▪ Present in 84% of patients with thymoma who are
younger than 40 years
• Imaging studies
❖Chest x-ray
• Plain anteroposterior and lateral views may identify a
thymoma as an anterior mediastinal mass .
❖Chest CT scan is mandatory to identify thymoma
❖MRI of the brain and orbits may help to rule out other
causes of cranial nerve deficits but should not be used
routinely
• Electrodiagnostic studies
I.
Repetitive nerve stimulation RNS
2.
Single fiber electromyography (SFEMG)
✓ SFEMG is more sensitive than RNS in MG (but it needs
much time)
✓ Any decrement over 10% is considered abnormal
✓ Should not test clinically normal muscle
✓ Proximal muscles are better tested
• Most common employed stimulation rate is 3Hz, several
factors can affect RNS results e.g. lower temperature
increases the amplitude of the compound muscle action
potential, and many patients report clinically significant
improvement in cold temperatures
• Pharmacological testing
• Edrophonium(Tensolon test)
▪ Patients with MG have low numbers of AChR at the
NMJ
▪ Ach released from the motor nerve terminal is
metabolized by Acetylcholine esterase
▪ Edrophonium is a short acting Acetylcholine Esterase
Inhibitor that improves muscle weakness
▪ Evaluate weakness (i.e. ptosis and ophthalmoplegia)
before and after administration
• Treatment of MG
• Main line of Rx are:
❖AChE inhibitors
❖Immunomodulating therapies
❖Plasmapharesis
❖Thymectomy (Important in treatment, especially if
thymoma is present)
• AChE inhibitors
• Pyridostigmine bromide (Mestinon)
• Starts working in 30-60 minutes and lasts 3-6 hours
• Adult dose:
• 60-360mg/d PO
• 2mg IV \IM q2- 3h
• Caution
Check for cholinergic crisis
due to depolarisation block of
motor end plates, with muscle fasciculation, paralysis, pallor, sweating,
excessive salivation and small pupils
• myasthenic crisis
severe weakness due to exacerbation of myasthenia
• This may be distinguished by the clinical features and, if necessary, by the
injection of a small dose of Edrophonium
.
• Others: Neostigmine Bromide
• Propantheline( 15mg tablets)
• Given if patient develops abdominal pain/diarrhea, l5mg tds
or 15 mg taken 30 minutes before each dose of
Pyridostigmine
• Immunomodulating therapies
• prednisolone
▪ Most commonly used corticosteroid in MG
▪ Significant improvement is often seen after a decreased
antibody titer which is usually 1-4 months
▪ No single dose regimen is accepted
• Azathioprine
▪ Start on 25mg bid
▪ Increase by 25mg/day until patient is on a dose
of2.5mg/kg BW per day
▪ Assess full blood count and LFTs before starting
treatment and after a few days of initiation, then
weekly for 8weeks.
• cyclosporine
• Methotrexate
(in adults) 7.5-20 mg once weekly
• mycophenolate mofetil

• Thymectomy
▪ Done when indications for thymectomy present
▪ Patient with thymoma - the thymectomy is indicated all
.
▪ If no thymoma - the patient age, symptoms, duration,
severity, response to medication.
▪ Thymectomy is not recommended for the neonatal type
of myasthenia gravis.
▪ In juvenile form - thymectomy for patient with more
severe symptoms and lack of response to medical
therapy.
• plasma exchange and IVIG
this is given in :
✓ acute fulminant MG
✓ Preoperative (sometime)
✓ myasthenic crises
• As Five exchanges (3-4L/exchange)
• IV immunoglobulin- 400mglKg per day for 5 clays
• prognosis
▪ Untreated MG carries a mortality rate of 25-30 %
▪ Treated MG has a 4% mortality rate
▪ 40% have
ONLY
ocular symptoms
• Complications of MG
▪ Respiratory failure
▪ Dysphagia
▪ Complications secondary to drug treatment e.g. Long term steroid
use like
✓ Osteoporosis, cataracts, hyperglycemia,
✓ HTN , gastritis, peptic ulcer disease
• Lambert Eaton myasthenic syndrome
▪ It is a Presynaptic disorder of the NMJ
▪ Voltage gates calcium channel antibodies impede release of
acetylcholine
• Presented as
▪ Weakness
✓ more of Lower extremities than Upper Extremities
✓ bulbar and ocular muscles less often involved
▪ decreased reflexes - post tetanic potentiation
▪
Autonomic Nervous System involvement
▪ Associated with a cancer in the majority of patients( paraneoplastic)
▪ Underlying cancer may be previously unrecognized,
▪
Small cell lung cancer is the most common
• Treatment
:
▪ Underlying cancer
▪ Guanidine
▪ 3,4 diamino pyridine